
Abstract
The use of alloplastic chin implants has been associated with a risk of bone resorption. The aims of this study were to evaluate, in patients with microgenia, the association between chin implants and bone resorption and identify the associated risk factors for such resorption. The sample consisted of 51 patients with microgenia: 17 with chin implants (group A, placed over the course of a 15-year period [2002-2017]) and 34 without implants (group B). Cone-beam computed tomography was used to evaluate bone erosion in different areas of the chin. The patients were evaluated, and their medical records were reviewed to identify risk factors. A chi-square or Fisher exact test and the Mann-Whitney test were used to compare groups; resorption sites were compared with Friedman test. Linear regression models were used to evaluate associations between potential risk factors and resorption. Bone resorption was higher in group A than in group B (mean ± SD: 0.98 ± 0.63 mm vs 0.03 ± 0.12 mm; P < .0001). Symphyseal buccal cortical bone in group A was thinner (1.66 ± 0.34 mm) than it was in group B (2.07 ± 0.45 mm), P < .001. Group A showed appositional bone growth and no cortical bone perforation. The mean of the amount of bone resorption of chin implant patients compared with that of those without implants was, on average, 0.99 mm greater (95% confidence interval: 0.64-1.35; P < .001). Although statistically significant differences in bone resorption were observed between groups, these differences were not clinically significant. Thinning of symphyseal buccal cortical bone without perforation and appositional bone growth occurred in chin implant patients, suggesting bone remodeling. Our results suggest that bone that is in contact with chin implants remodels and remains stable throughout the years, instead of undergoing progressive resorption.
Introduction
Chin retrusion, or microgenia, is the most common type of chin deformity in the sagittal plane, and it can be evaluated both clinically and using cephalometric analysis. 1 One of the techniques employed to correct this condition is chin implant placement. Allograft materials, such as silicone implants, are used to camouflage chin retrusion. The use of alloplastic chin implants has been associated with a risk of bone resorption, also called bone erosion. 1 Some of the most recent studies on this issue have reported variable rates of bone erosion in patients with chin implants. However, data supporting this finding are limited.1,2
Risk factors associated with bone resorption that occurs under chin implants are not yet well studied. In 1996, Matarasso et al 3 suggested that labial incompetence should be considered a marker for severe mandibular resorption following a chin augmentation using silicone implants. However, Barnett 4 believed that the presence of a chin implant was a risk factor and that lip incompetence is a result of the bone resorption. Some studies have reported the occurrence of bone resorption under a chin implant, except when hard tissue replacement polymer chin implants stabilized with a titanium screw were used.5,6 Friedland et al 7 suggested that bone erosion is less when the implant is placed over the hard bone of the lower portion of the mandible. Despite all these findings, no protocol for the early detection of bone erosion and the follow-up of patients with alloplastic chin implant placement has yet been presented. Our literature review supports the need to conduct clinical studies to assess the status of the bone under a chin implant.
To accomplish this, our study aimed both to evaluate the association between chin implants and bone resorption in patients with chin retrusion and to identify risk factors associated with bone resorption in patients who had received a chin implant at the Oral and Maxillofacial Surgery (OMFS) clinic at the University of Puerto Rico (UPR) School of Dental Medicine over the course of a 15-year period (2002-2017).
Materials and Methods
Study Design
This was a cross-sectional study of patients seen at the OMFS clinic of the School of Dental Medicine from 2002 to 2017. A written informed consent was obtained from all the patients who participated in the study. The Institutional Review Board of the UPR approved the study on February 16, 2018 (approval #B0930217).
Study Participants
This study included individuals who had microgenia and who had received chin implants (placed within the 15 years prior to the study at the OMFS clinic at the UPR School Dental Medicine), as well as patients with microgenia (defined as the retrusion of the chin in the anteroposterior dimension) but who had not received chin implants. The inclusion criteria were (1) being 21 years old or older, (2) having a diagnosis of microgenia (ie, chin retrusion), and (3) having had their chin implants surgically placed (for those with such implants) in the 15 years prior to the study (2002-2017). Syndromic patients were excluded from the study.
A total of 102 patients with chin implants (surgically placed from 2002 to 2017) were found in our records. Thirty-two patients with chin implants were reached, and 17 of those satisfied the inclusion criteria, agreed to participate, and completed the study components (interview, cone-beam computed tomography [CBCT], and authorizing the release of medical record data). A total of 41 patients with a diagnosis of microgenia but without chin implants were identified; 38 of these patients were reached, of whom 34 completed the study as part of group B. Our total sample included 51 patients: 17 patients in group A and 34 in group B (Diagram 1).
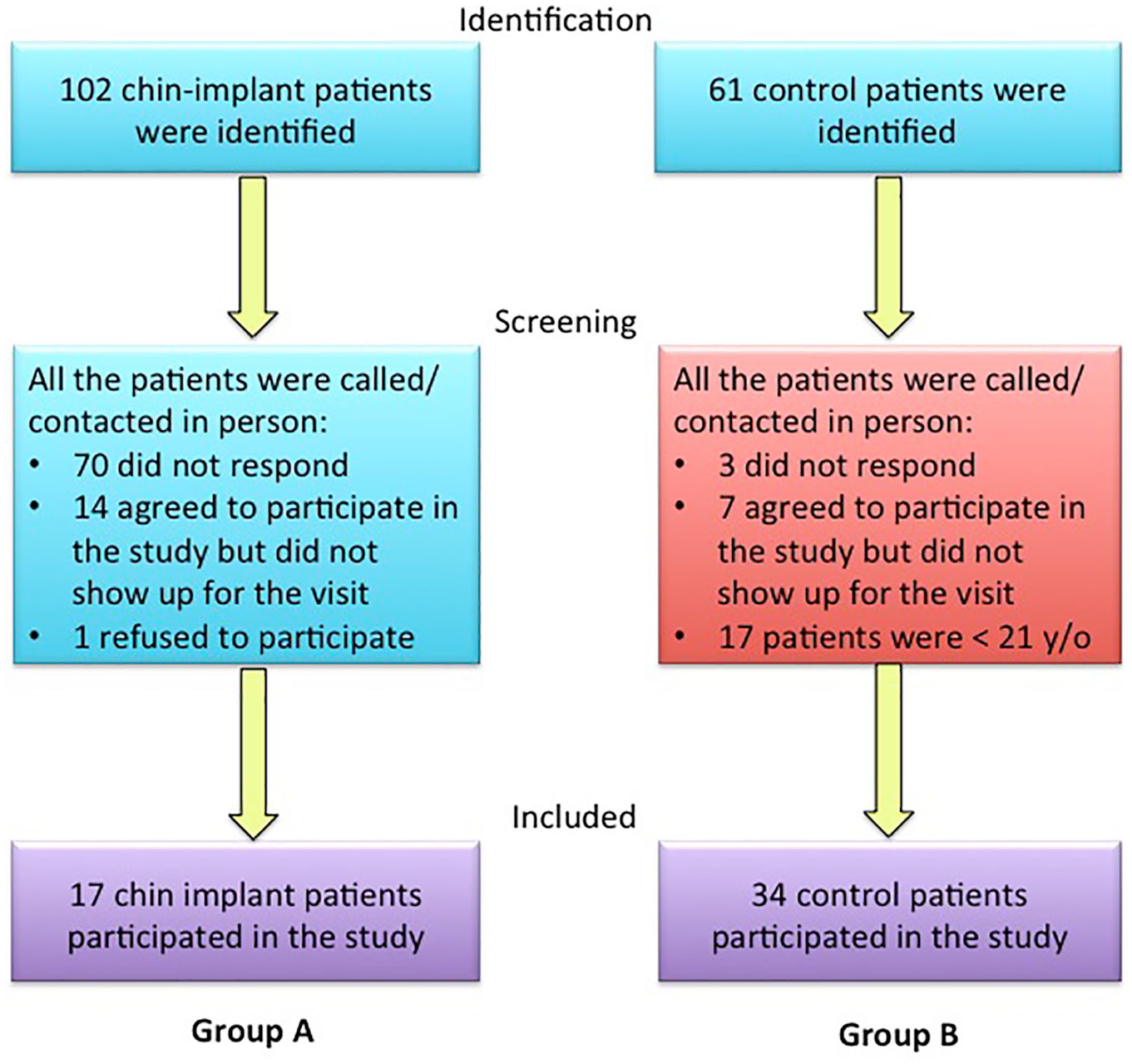
Patient selection flow chart.
Chin Implant Group (Group A)
Patients who had had chin implants placed during the relevant period were identified and contacted, via telephone or in person, to make an appointment for a chin implant evaluation; as indicated above, 17 patients showed up. During the appointment, CBCT was used to evaluate the patient’s chin implant and the underlying bone in a 3-dimensional view. The following landmarks were identified in each patient’s CBCT image (sagittal view): (1) the current position of the implant (suprapogonion, pogonion, or menton), (2) bone resorption in millimeters on the right parasymphysis, left parasymphysis, and midpoint of the implant (radiolucency between the back end of the implant and the outer bone), (3) implant displacement; in addition, if there was a screw in the implant, we evaluated whether the screw coincided with the position in the bone; if no screw was present, the most inferior-anterior position was initially considered to evaluate displacement (yes/no). Bone resorption was classified (based on the Robinson classification)8,9 as grade I if there was any degree of resorption, measuring up to a third of the implant’s anteroposterior dimension (up to 3 mm); as grade II if the resorption was from a third to half of the implant’s length (3-5 mm); or as grade III if the resorption was more than 50% of the implant’s anteroposterior length (≥5 mm).
Control Group (Group B)
Patients with a diagnosis of chin retrusion (microgenia) were identified and contacted by telephone or in person to make an appointment for an evaluation. The patients were evaluated at the clinic and a CBCT scan was done.
Data Collection in the Chin Implant Group (Group A) and Control Group (Group B)
The following information was extracted from each patient’s medical records, as collected at the initial evaluation: (1) age, (2) sex, (3) preoperative and/or postoperative labial incompetence (present [+] or absent [−]), which is the inability to passively close lips together and to achieve a relaxed, consistent, lips-together rest posture, (4) pain in the chin area (yes/no) in the presence of the chin implant: (5) postoperative complications (gingival recession, bone or root exposure, mental nerve paresthesia, infection, and toothache; yes/no), (6) postoperative period (years), (7) implant size (small, medium, large, extra-large, according to the manufacturer’s information), (8) implant material (silicone, polytetrafluoroethylene, polyethylene, hydroxyapatite), (9) titanium screw fixation (yes/no).
During the evaluation visit, a short (10 minutes) interview was conducted to collect additional information on the following: (1) mental nerve paresthesia (yes/no)—if present, this might be temporary mental nerve paresthesia (temporary numbness of the chin and lower lip) or permanent paresthesia (numbness that does not abate); (2) smoking history (from the time of the implant’s placement; yes/no); (3) history of chin trauma (yes/no); (4) sleep habits that involve pressure to the chin with the hand (yes/no)—each patient was asked whether he or she had noticed ever having engaged in this kind of behavior or, if not, whether a companion had noticed him or her ever having done so; (5) hand-to-chin support while resting (yes/no); (6) medical conditions (yes/no), including hypertension, diabetes, hypothyroidism, and/or others; (7) medication/s, (if yes, which one/s), later classified as hypertensive drugs, diabetes drugs, hypothyroidism drugs, and others. This clinical interview was created using potential risks factors that can be associated with chin implants and bone erosion, neither of which was evaluated using a CBCT scan or the medical records.
In patients with chin implants, bone resorption was defined as hypodensity and the adaptation of the outer cortex of the mandible to the contours of the implant, visible on the CBCT scan. In patients without a chin implant, bone resorption was defined as hypodensity, depression, indentation, and/or irregularity in the outer cortex of the symphysis of the mandible, visible on the CBCT scan.
Cone-beam computed tomography measurements were taken in the right parasymphysis (below the canine), symphysis, and left parasymphysis (below the canine) areas of the chin and included (1) the amount in millimeters of bone resorption, (2) anteroposterior bone resorption of the chin (dividing the millimeters of resorption by the thickness of the chin in sagittal view) in all areas, (3) buccal cortical bone thickness, (4) lingual cortical bone thickness, (5) resorption occurring predominantly in the superior bone (yes/no), (6) bone apposition or growth (yes/no), and, if positive, the area of apposition or growth (right parasymphysis, symphysis, and/or left parasymphysis basal or superior area of the chin [yes/no]), (7) dental or root involvement (yes/no). Mean bone resorption (millimeters) was calculated as the mean of the right parasymphysis, symphysis, and left parasymphysis measures; mean of anteroposterior bone resorption averaged the anteroposterior bone resorption of the chin in 3 areas.
Statistical Analysis
Descriptive statistics, such as means (±standard deviations) and medians (interquartile ranges) for continuous variables, as well as frequencies (percentages) for categorical variables, were calculated. The normality of the distribution of the continuous variables (CBCT measurements) was evaluated using the Shapiro-Wilk test and was rejected for all the variables. A chi-square or Fisher exact test and a Mann-Whitney test were used to compare patients with and without implants. Friedman test was used to compare resorption at different measurement sites, in group A and group B, separately.
To evaluate the association between the time since implant placement and resorption variables, group A was divided into 2 subgroups: patients with implants placed up to 5 years prior (2013-2017) made up subgroup 1, and patients with implants placed from 6 to 15 years prior (2003-2012) made up subgroup 2. A Mann-Whitney test was used to compare the imaging results between the 2 subgroups.
Linear regression analysis with robust (White) variances was performed to evaluate the association between mean resorption and potential risk factors, individually. In addition, the multivariate regression analysis included the risk factors that were statistically significantly associated with the outcome in univariate analysis (chin implant, sex, and having the habit of applying pressure to the chin with the hand while sleeping). Linear regression coefficients and their 95% confidence intervals (CIs) were reported. All analyses were conducted at 0.05 level of statistical significance, using SAS statistical software version 9.3 (SAS Institute, Inc, Cary, North Carolina).
Calibration
Prior to the initiation of the study, to evaluate the reliability of CBCT measurements, 2 repeated readings of cortical bone and chin width measurements were obtained (by the same examiner: C.O.-D.) for 20 patients. The readings were compared using the Wilcoxon signed rank sum test and correlated using Spearman rho and intraclass correlation coefficients (ICCs).
Results
Calibration
The average difference in 2 repeated cortical bone measurements was 0.01 mm (SD: 0.07), with the median difference of 0 (Wilcoxon signed rank sum test P value = .46). Similarly, there was no significant difference in 2 repeated chin measurements (mean ± SD: 0.02 ± 0.08 mm; median: 0.03 mm; Wilcoxon signed rank sum P value = .32). Measurements were highly correlated for both cortical bone (Spearman rho = 0.979; ICC = 0.99) and chin measurements (Spearman rho = 0.997; ICC = 0.999), demonstrating excellent intraexaminer reliability.
Patients’ Background Characteristics, Conditions, and Symptoms
The average age of the patients in our study group was 47.35 (±17.30) years (range: 21-80 years). There were 37 females and 13 males included in the study. All the members of group A were female; women comprised 58.82% and men 41.12% of group B. Of the 51 patients in the study, 10 had labial incompetence, with 4 (23.53%) being in group A and 6 (17.65%) being in group B (Fisher test P value = .7). The 4 patients in group A who had lip incompetence, preoperatively, did not have lip incompetence at the evaluation. Three patients in group A reported pain in the chin area, which resolved early in the postoperative period. Three patients presented temporary mental paresthesia that also resolved.
Table 1 summarizes the background characteristics of the patients who were evaluated in our study. Between the 2 groups, there was a statistically significant difference in the percentage of patients with the habit of applying pressure to the chin with the hand while sleeping: 3 patients in group A reported that they applied pressure to their chins with the hand while sleeping, whereas none of the individuals in group B made this report (Fisher exact test P value of .03).
Distribution a of Patient Background Characteristics, Conditions, and Symptoms Among All, and by Chin Implant Group.
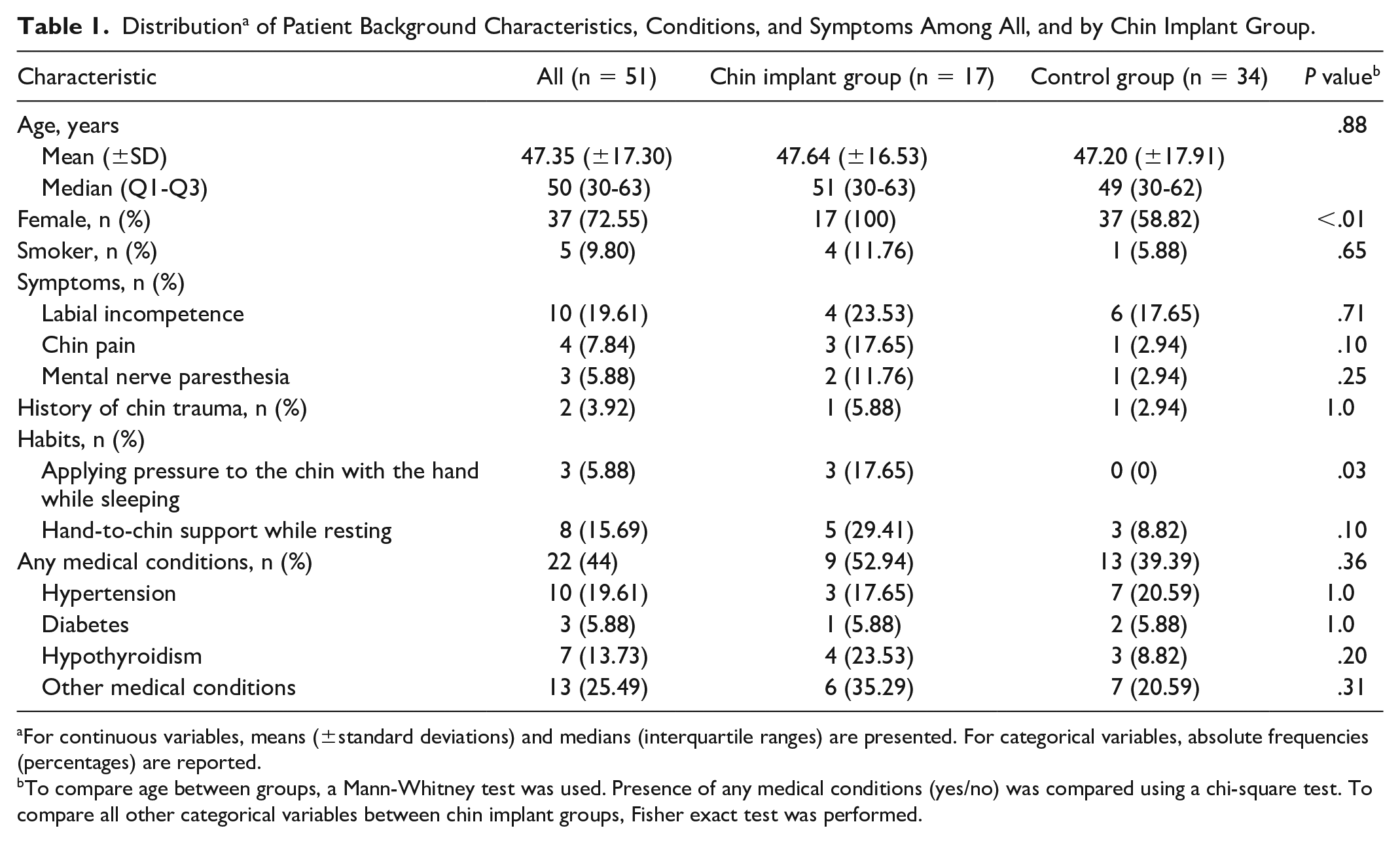
For continuous variables, means (±standard deviations) and medians (interquartile ranges) are presented. For categorical variables, absolute frequencies (percentages) are reported.
To compare age between groups, a Mann-Whitney test was used. Presence of any medical conditions (yes/no) was compared using a chi-square test. To compare all other categorical variables between chin implant groups, Fisher exact test was performed.
Clinical and Imaging Findings in the Chin Implant Group (Group A)
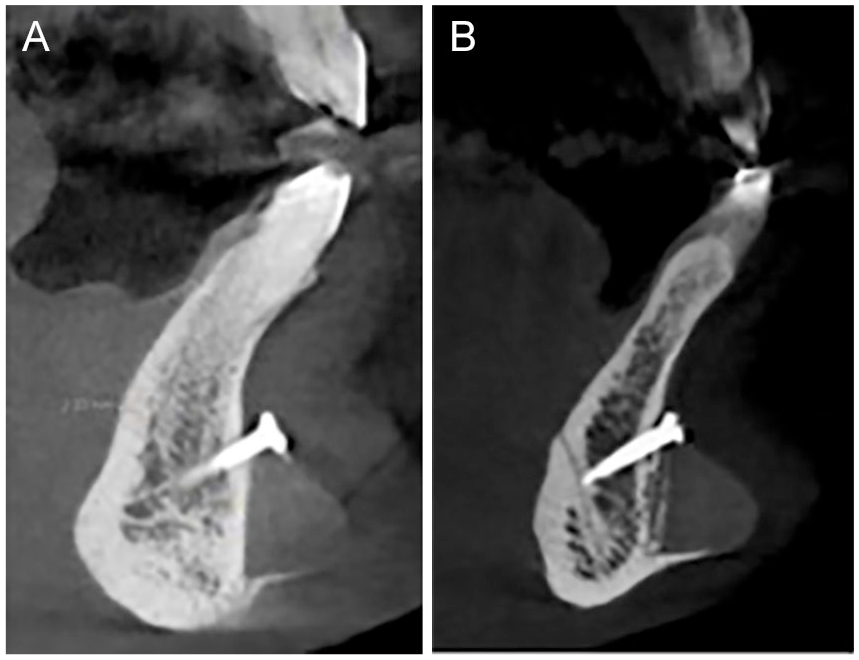
The dates of the surgeries varied, ranging from April 11, 2003, to May 8, 2017. All the chin implants were fixed with a titanium screw above the implant in the symphysis area. All the implants used were made of silicone (Anatomical Chin, Implantech, Ventura, California). Five patients presented displacement of the implant at the suprapogonion area. Three of those patients had right-side superior displacement and 2 had minimal intrusion (Figure 1). One of the patients with chin intrusion showed appositional bone growth around the implant surface (Figure 1B). In those patients, mean bone resorption varied from 0.37 to 2.20 mm. Furthermore, the cortical bone plate remained without perforations (Figure 1A).
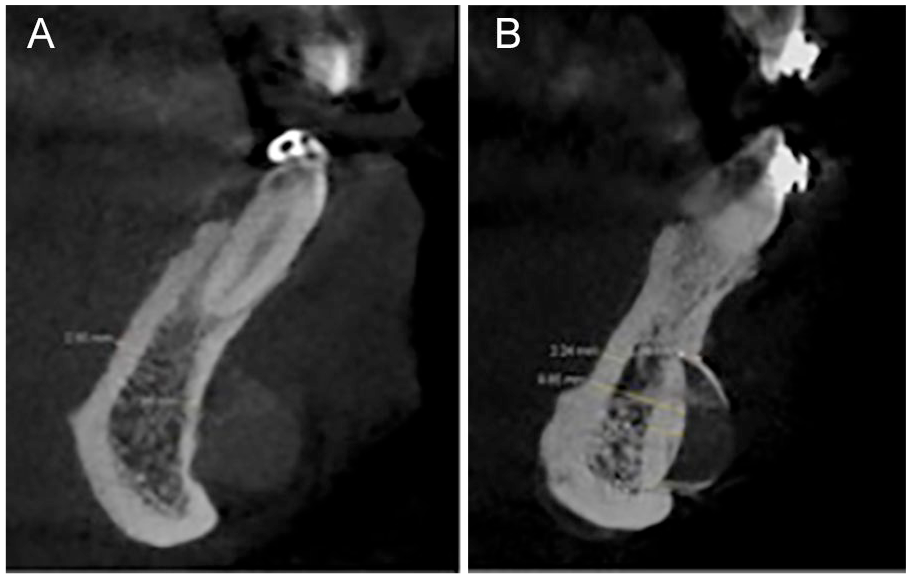
Cone-beam computed tomography showing parasymphysis of 2 patients in group A. (A) Suprapogonion chin implant (placed in 2003) displacement and (B) appositional bone growth around the chin implant that was placed in 2007.
Postoperative complications were found in 2 patients (11.76%). Both had numbness of the mental nerve, but only 1 had buccal gingival recession (associated with tooth #25). Implant sizes varied: 13 were medium, 2 were large, 1 was extra-large, and the size of 1 was not reported. There was no cortical bone perforation or root involvement found.
Table 2 summarizes the CBCT measures in both groups. In group A, the mean bone resorption underlying the implant was 0.98 mm (±0.63), ranging from 0 to 2.21 mm. Mean of anteroposterior bone resorption of the chin was 0.08 mm (±0.63), ranging from 0 to 0.21 mm. Resorption was greater on the right (mean ± SD: 1.21 mm ± 0.82) and left parasymphysis (1.21 mm ± 0.69) than it was for the symphysis (0.51 mm ± 0.92), with a Friedman test P value of .02. Similar differences were observed for the anteroposterior bone resorption of the chin (right parasymphysis, symphysis, left parasymphysis, mean ± SD: 0.10 mm ± 0.073, 0.04 mm ± 0.079, and 0.10 mm ± 0.063, respectively), with a Friedman P value of .02. The mean buccal cortical bone thickness was higher on the right (2.15 mm ± 0.70) and left parasymphysis (2.09 mm ± 0.51) than it was in the symphysis (1.66 mm ± 0.34; Friedman P value = .01). The mean lingual cortical bone thickness was 2.58 mm (±0.65) on the right parasymphysis, 2.21 mm (±0.73) in the symphysis, and 2.44 mm (±0.51) on left parasymphysis (Friedman P value = .02).
Distribution a of Cone-Beam CT Measures Among Patients in Chin Implant and Control Group.
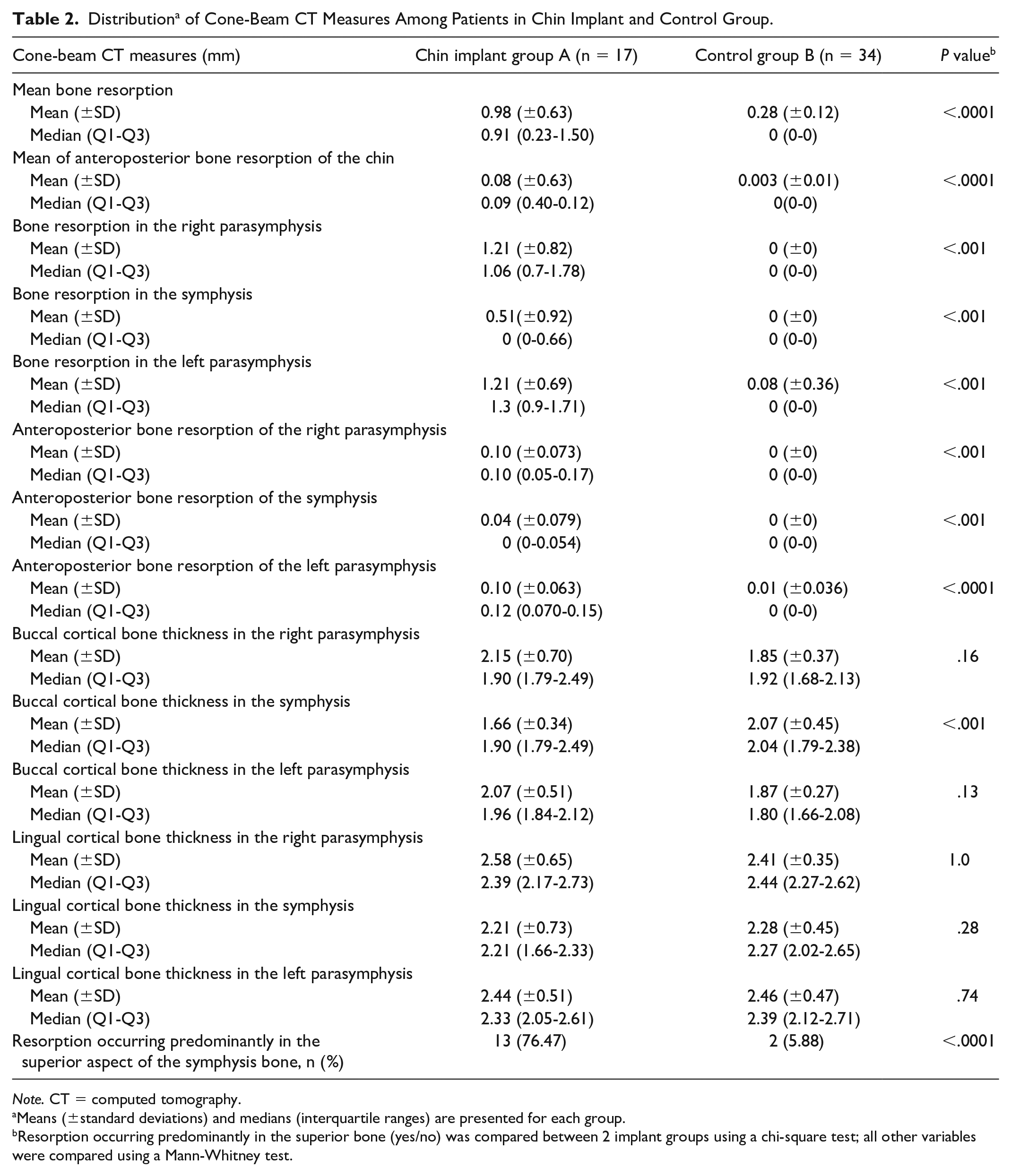
Note. CT = computed tomography.
Means (±standard deviations) and medians (interquartile ranges) are presented for each group.
Resorption occurring predominantly in the superior bone (yes/no) was compared between 2 implant groups using a chi-square test; all other variables were compared using a Mann-Whitney test.
Grade I bone resorption occurred in 16 patients; 1 patient showed no resorption. In 13 patients, bone resorption occurred predominantly in the superior bone beneath the implant. Appositional bone growth was found in 15 patients (88.24%). The apposition was evaluated in different areas of the chin. Six patients showed basal bone growth in the right parasymphysis, 12 showed basal bone growth in the symphysis, 5 showed basal bone growth in the left parasymphysis, 4 showed superior bone growth in the right parasymphysis, 3 showed superior bone growth in the symphysis, and 3 showed superior bone growth in the left parasymphysis.
CBCT Measures in Group A, According to the Age of the Implant (Time Since Placement)
Table 3 summarizes the distribution of CBCT measures in implant subgroups that are defined according to the time since placement. The mean bone resorption in subgroup 1 (implants placed up to 5 years ago) was similar (mean ± SD: 0.94 mm ± 0.63) to that in subgroup 2 (mean ± SD: 1.02 mm ± 0.68; Mann-Whitney test P value = .89). Similarly, there were no differences between groups 1 and 2 in the mean of anteroposterior bone resorption of the chin (0.081 mm ± 0.05 and 0.089 mm ± 0.063, respectively; P = .96) or in buccal cortical bone thickness in the symphysis (1.82 mm ± 0.39 in subgroup 1 vs 1.47 mm ± 0.15 in subgroup 2; P = .16).
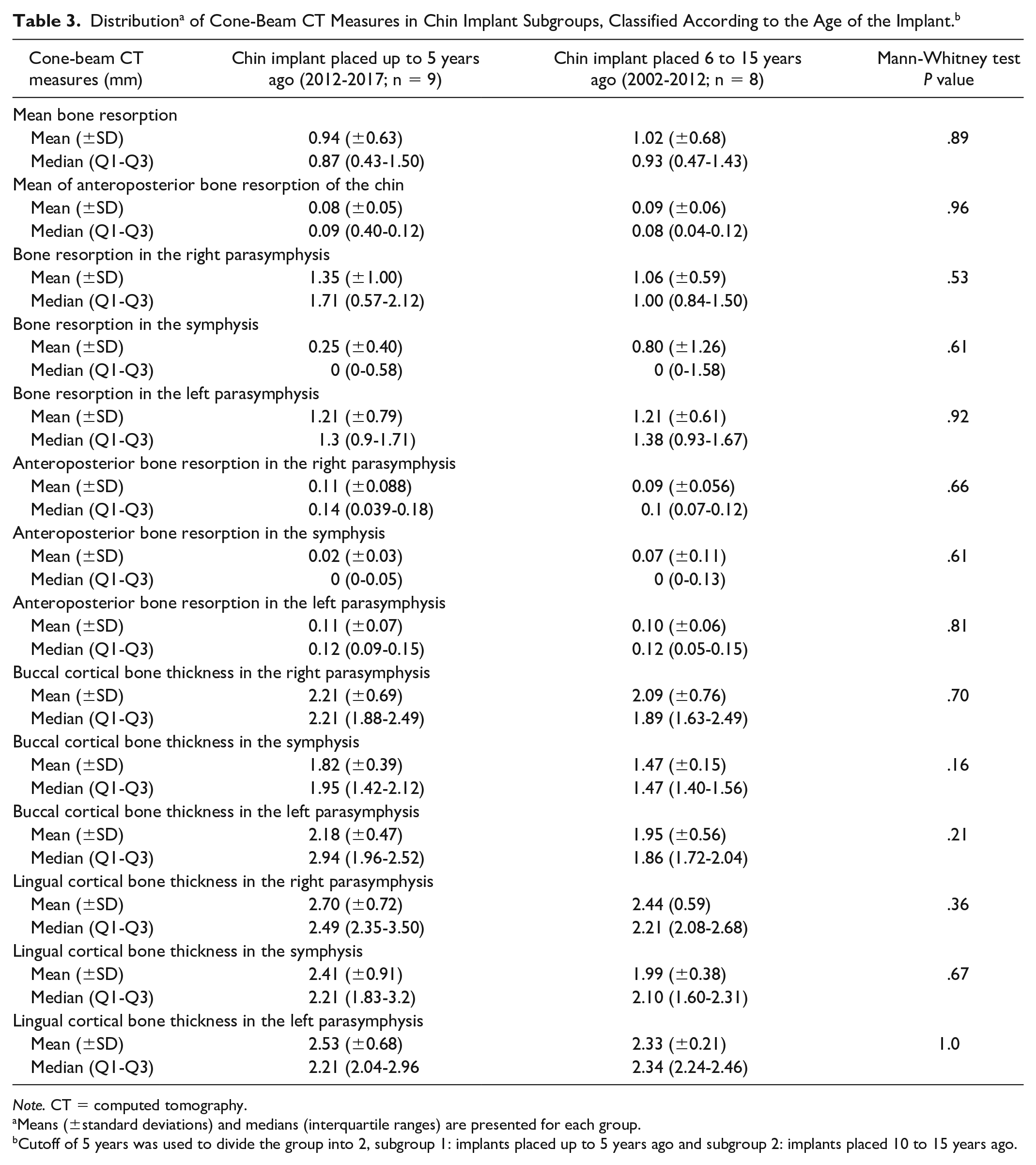
Note. CT = computed tomography.
Means (±standard deviations) and medians (interquartile ranges) are presented for each group.
Cutoff of 5 years was used to divide the group into 2, subgroup 1: implants placed up to 5 years ago and subgroup 2: implants placed 10 to 15 years ago.
Clinical and Imaging Findings in the Control Group (Group B)
Mean bone resorption was 0.028 mm (±0.12), and mean of anteroposterior bone resorption of the chin was 0.0028 mm (±0.012). The mean bone resorption on the right parasymphysis was 0.0 mm (±0) and as was that of the symphysis; a mean bone resorption of 0.084 mm (±0.36) was found on the left parasymphysis; no statistical differences were seen between the 3 areas measured (right parasymphysis, symphysis, left parasymphysis; Friedman P value = .14). In terms of mean of anteroposterior bone resorption of the chin, the means of the right parasymphysis and the symphysis were both 0.0 mm (±0), and the mean resorption of the left parasymphysis was 0.0085 mm (±0.036); no statistical differences between the 3 areas measured (right parasymphysis, symphysis, left parasymphysis) were found (Friedman P value = .14). The mean cortical bone thickness in the buccal plate was 1.85 mm (±0.37) on the right parasymphysis, 2.074 mm (±0.45) in the symphysis, and 1.87 mm (±0.27) on the left parasymphysis (Friedman P value = .01). The mean lingual cortical bone thickness did not vary significantly by the measurement site, with an average of 2.42 mm (±0.35) on the right parasymphysis, 2.28 mm (±0.445) in the symphysis, and 2.46 mm (±0.47) on left parasymphysis (Friedman P value = .31). Two patients showed resorption occurring predominantly in the superior aspect of the bone in the chin. Appositional bone growth and root involvement were not observed. Table 2 summarizes the CBCT measures.
Comparison of CBCT Findings Between Group A and Group B
The mean bone resorption in group A (0.98 mm ± 0.63) was higher than the mean resorption in group B (0.28 mm ± 0.12; P < .0001). Similarly, the mean of anteroposterior bone resorption of the chin in group A (0.08 mm ± 0.63) was higher than it was in group B (0.0028 ± 0.012; P < .0001). The means of the bone resorption at 3 sites in group A (right parasymphysis, 1.21 mm ± 0.82; symphysis, 0.51 mm ± 0.92; left parasymphysis, 1.21 mm ± 0.69) were higher than they were for the same 3 sites in group B (right parasymphysis, 0 ± 0; symphysis, 0 ± 0; left parasymphysis, 0.084 ± 0.36; P < .001, <.0007, and <.001, respectively). The means of anteroposterior bone resorption of the chin at 3 sites in group A (right parasymphysis, 0.10 mm ± 0.073; symphysis, 0.04 mm ± 0.079; left parasymphysis, 0.10 mm ± 0.063) were higher than they were in group B for the same 3 sites (right parasymphysis, 0 ± 0; symphysis, 0.04 mm ± 0.079; left parasymphysis, 0.0085 ± 0.036; P < .001, <.0003, and <.0001, respectively).
No significant differences were found in the means of buccal cortical bone thickness in right parasymphysis between group A (2.15 mm ± 0.70) and group B (1.85 ± 0.37; P = .16). Similarly, no significant differences were found in the means of buccal cortical bone thickness in left parasymphysis between group A (2.09 mm ± 0.51) and group B (1.87 ± 0.27; P = .13). However, the mean of buccal cortical thickness in the symphysis was higher in group A (1.66 mm ± 0.34) than in group B (2.074 ± 0.45); the P value was .0009. No significant differences were found in the means of lingual cortical bone thickness in group A (right parasymphysis, 2.58 mm ± 0.65; symphysis, 2.21 mm ± 0.73; left parasymphysis, 2.44 mm ± 0.51) compared with those of group B (right parasymphysis, 2.41 ± 0.35; symphysis, 2.28 ± 0.45; left parasymphysis, 2.46 ± 0.47; P = 1.0, .28, and .74, respectively). Table 2 summarizes the CBCT measures of group A and group B and includes the relevant P values.
Association of Mean Resorption With Potential Risk Factors
In multivariate regression analysis, after adjusting for sex (female vs male) and the habit of applying pressure to the chin with the hand while sleeping (2 risk factors identified as significantly associated with increased resorption in univariate analysis), patients with chin implants had an average of 0.99 mm more bone resorption (95% CI: 0.64-1.35), compared with those without such implants (P < .001; Table 4).
Association a Between Mean Bone Resorption and Potential Risk Factors.
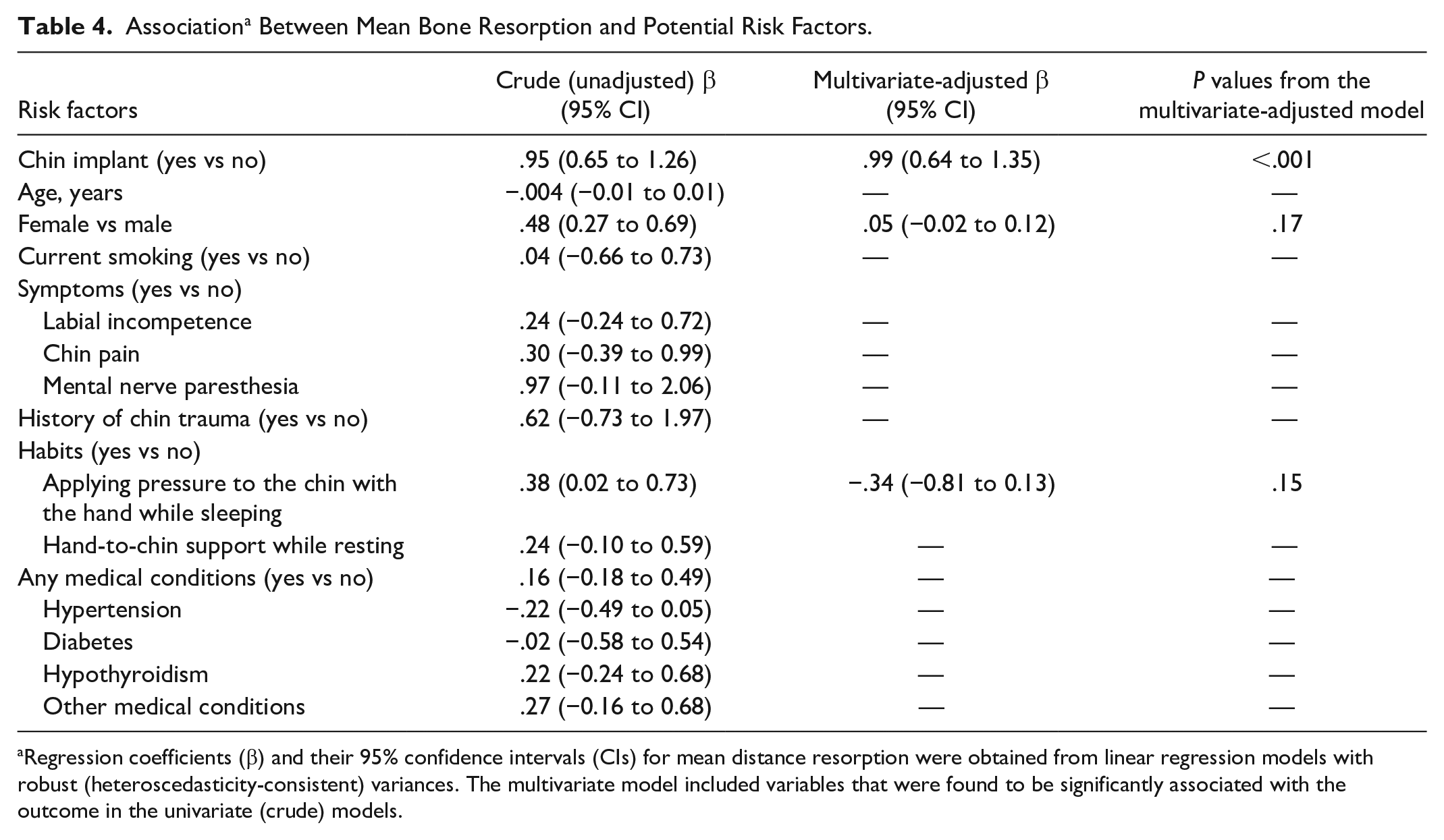
Regression coefficients (β) and their 95% confidence intervals (CIs) for mean distance resorption were obtained from linear regression models with robust (heteroscedasticity-consistent) variances. The multivariate model included variables that were found to be significantly associated with the outcome in the univariate (crude) models.
Discussion
One of the aims of this study was to evaluate the association between chin implants and bone resorption in patients with microgenia. Mean bone resorption was defined as a hypodense area between the chin implant and the cortex of the bone on right parasymphysis of, in the symphysis of, and on the left parasymphysis of the chin. The right and left parasymphysis were measured below the canine area; the symphysis, which is the central part of the chin and is where the screw is usually placed, was also measured. The mean bone resorption in group A was 0.98 mm and in group B was 0.28 mm, with a P value of less than .0001. There was a statistical difference of mean resorption in patients with chin implants and those without. The mean of anteroposterior bone resorption of the chin was defined as the millimeters of hypodense bone divided by the length, in millimeters, of the anteroposterior dimension of the chin in the sagittal plane. The number that resulted represented how much bone had been resorbed in proportion to the anteroposterior dimension of the chin. The mean resorption of the mandible in group A was 0.08 mm and was 0.0028 mm in group B, with a P value of less than .0001. There is a statistical difference between the 2 groups in terms of the mean levels of bone resorption of the chin.
When we evaluated the mean bone resorption in each of the areas of the patients in group A, we found less resorption in the symphysis (0.51 mm) than was found on the right and left parasymphysis of the chin (1.21 mm). The differences in bone resorption between the symphysis and the parasymphysis of the chin might have been caused by the presence of the screw fixing the implant in place. The reason the screw is placed above the implant is that it keeps the implant in position. This result suggests that in the parasymphysis of the chin, the movement of the implant may provoke bone resorption, which would not be the case in the area of the symphysis, where the screw prevents the displacement of the implant during muscle contraction. In mandibular retrusion, complete lip closure requires the chin muscles to work harder than normal. This tension of the mentalis muscle results in pressure that may cause bone resorption under the implant. 7 Implant fixation to bone is recommended to achieve optimal implant stabilization. 10 In previous studies, when the chin implant was stabilized to the bone with a screw, no bone resorption was found.5,6
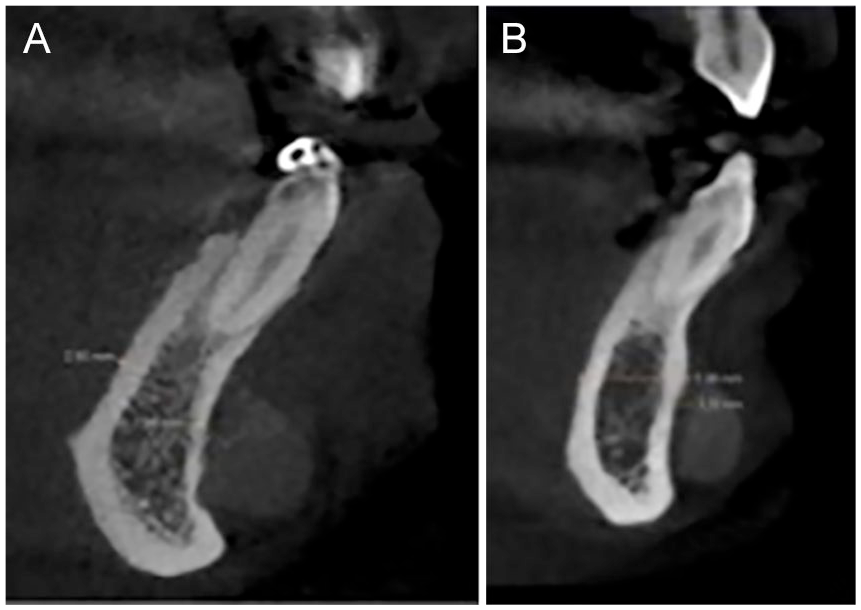
The cortical bone was evaluated in both groups. The evaluation found that the patients in group A had experienced a thinning of the buccal cortical bone of the symphysis (1.66 mm) compared with patients in group B (2.074 mm). Patients in group B showed thicker bone in the buccal cortex of symphysis (2.07 mm) than in the parasymphysis cortex of the chin (1.86 mm; Friedman P value = .01). However, group A patients showed thicker bone in the parasymphysis cortex of the chin (2.1 mm) than in the buccal cortex of the symphysis (1.66 mm; Friedman P value = .01). In addition, it was found that patients with chin implants had appositional bone growth (Figure 2) and patients without such implants did not. These results suggest that bone remodels but does not resorb in the presence of a chin implant. Compared with the region of the superior bone, most of the appositional bone growth was found in the basal bone area, and most of the bone resorption was predominantly on the superior bone (13 of 17 patients).
Cone-beam computed tomography showing appositional bone growth in the basal area below the chin implants of 2 patients in group A: (A) implant placed in 2005 and (B) implant placed in 2009.
The Robinson classification 8 was used to rate bone resorption in the chin implant group. Sixteen patients presented grade 1 (up to 3 mm), but 1 patient showed no resorption (0 mm). The 16 patients had a minimum of resorption, based on the Robinson classification. Five patients in group B had suprapogonion chin implant displacement. No cortical bone perforations were seen in those patients. The mean bone resorption varied from 0.37 to 2.20 mm in those patients. Friedland et al 7 reported that most of the patients showing bone resorption had the chin implant placed in the suprapogonion. They concluded that the resorption of bone is minimal when the implant is placed over the hard bone of the lower portion of the mandible. Although the bone resorption observed in our study was minimal, our study nevertheless supports the notion that it is important to place the chin implant at the pogonion area, which is composed of dense cortical bone and is more resistant to resorption.7,11
In our sample, the oldest chin implant had been placed in April 2003 and had a mean bone resorption of 1.89 mm, compared with the most recent chin implant, which was placed in May 2017 and in which the mean bone resorption was 1.90 mm (Figure 3). Our analysis, which evaluated bone resorption and the age of the implant, determined that there was no statistically significant difference between subgroup 1 and subgroup 2. This finding suggests that bone resorption is not progressive. Bone remodels soon after a chin implant is placed and may remain stable throughout the years. Moreover, the mean thickness of the buccal cortical bone of the symphysis was less in subgroup 2 (1.47 mm) than it was in subgroup 1 (1.82 mm); however, this difference was not statistically significant (P = .16). These results suggest that bone remodels instead of resorbing over time. In the study of Friedland et al, 7 mandibular flattening was noted beneath the implant as early as 2 months, postoperatively, and measurable resorption at 3 months. Moenning and Wolford 12 reported that within the first 12 months, postoperatively, 24 of 42 patients with Proplast (formerly from Vitek, Houston, Texas) chin implants had most of their changes appear radiographically. They explained that once the tissue reached equilibrium, osseous resorption did not seem to continue, and the implant became stable. Vuyk 13 reported no clinical side effects from minimal bone resorption in 8 of 13 patients, all of whom were studied radiographically in their study. Similarly, in our study, we did not observe any clinical changes in the patients with bone resorption.
Comparison of bone resorption underneath a chin implant (A) placed in April 2003 versus one (B) placed in May 2017.
Silicone implants were introduced in the 1950s. 13 Using lateral X-rays, Robinson and Shuken 8 were the first to report the presence of bone resorption under silicone chin implants. After this finding, some studies reported similar results in patients with silicone implants.2,3,7,11,13 None of these studies reported fixation of the implant to the bone. In our study, all the patients in group A had silicone chin implants that were fixed in place with a titanium screw. The mean bone resorption was minimal, and no clinical changes were noted.
The other aim of the study was to identify risk factors—real and potential—associated with bone resorption. Labial incompetence was observed in the initial evaluation of 4 patients with chin implants and 6 patients without. The mean bone resorption of the 4 patients with chin implants that had labial incompetence, preoperatively, was limited to 1 to 2.01 mm. There was no statistical difference between the groups. Matarasso et al 3 reported severe bone erosion in patients with labial incompetence and chin implants placed in a suprapogonion position. In our study, the preoperative labial incompetence of 4 patients with chin implants was corrected after the implant surgery and showed minimal bone erosion. Cases with persistent labial incompetence and hyperactivity of the mentalis muscle after chin implant placement may present more aggressive bone changes.3,11,14
The only statistical difference in the categorical variables was found in patients (in group A) who had the habit of exerting pressure on the chin with the hand while sleeping. The other categorical variables, such as chin pain, mental paresthesia, chin trauma, smoking, hand-to-chin support while resting, and medical conditions, evidenced no statistical differences between the 2 groups. The univariate regression analysis showed a significant association between mean bone resorption and the presence of a chin implant, being female, and having the habit of exerting pressure on the chin with the hand while sleeping. However, after including all these factors in the same model, only the presence of an implant was significantly associated with mean bone resorption. This is similar to what Barnett 4 believed, which is that the presence of a chin implant is a risk factor.
The current study had several strengths. To the best of our knowledge, this was the first study (using CBCT measures) evaluating bone resorption in the chin area of the members of a population with microgenia but without chin implants. The study examiner was calibrated prior to the study and demonstrated very high reliability in his measurements. At the same time, our study had limitations, such as the relatively small sample size and the absence of longitudinal data on resorption. Our future studies will focus on comparing patients with chin implants fixed with screws and those without such screws to evaluate bone resorption associated with fixation.
Conclusions
Our data showed a statistically significant difference in bone resorption between patients with microgenia and with and without chin implants; however, this difference could not be considered clinically significant. Our results suggest that in the parasymphysis of the chin, the movement of the chin implant may provoke bone resorption, which is not the case in the symphysis of the chin, where the fixation screw prevents the displacement of the implant by muscular contraction. Thinning of the buccal cortical bone of the symphysis and appositional bone growth occurred in chin implant patients, suggesting that bone remodels. Our analysis to evaluate bone resorption and the age of the implant showed no statistically significant difference between subgroup 1 and subgroup 2, suggesting that bone remodels over time. Sixteen patients presented a grade 1 Robinson classification of bone resorption, which is the minimum degree of resorption in the classification. No cortical bone perforation or tooth root involvement was seen. Only the presence of an implant, as a risk factor, was significantly associated with mean bone resorption. This study suggests that the bone under an implant remodels and remains stable throughout the years instead of undergoing progressive resorption.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.