
Abstract
Large-volume fat transfer to the buttocks and breast has rapidly become popular. Lipofilling using syringes is tedious, time-consuming, and carries the risk of contamination. Most often, systemic anesthesia is being used. This study aims to evaluate the efficacy of large-volume lipofilling in local anesthesia. Local anesthesia was performed with 2 anesthetics: lidocaine and prilocaine. We performed vibration amplification of sound energy at resonance (VASER) and reciprocating power-assisted liposuction (PAL) for fat collection in a closed-loop system using a peristaltic pump. In a reverse pump setting, fat was then used for expansion vibration lipofilling. Pre- and postoperative data were collected. There were no major complications. Liposuction volumes up to 3.100 mL were extracted, and injection volumes ranged from 200 to 1600 mL. Mean operation time was 96 minutes. Satisfaction rate was high. Anesthesia was sufficient in all patients. Using a closed-loop system for fat extraction–purification and transfer is not only time- and cost-effective but also ideal for large-volume fat grafting. Recovery time is 1 to 2 days and satisfaction rate is high.
Keywords
Introduction
In autologous fat grafting, an individual’s own fat is harvested and injected into the soft tissues to augment or correct contours. Autologous fat grafts have several beneficial characteristics, including lack of immunogenicity, low cost, and easy accessibility. Combined with high-definition liposuction, lipofilling is an important unmitigated technique for advanced body contouring.
In a 2019 global statistics survey conducted by the American Society of Aesthetic Plastic surgery, there were 346 432 cases of buttock augmentation with either implants or fat transfer. 1 Breast augmentation using implants and fat grafting remains the number one aesthetic procedure, 1 but there is currently no statistics available regarding fat transfer only. Fat grafting in aesthetic breast surgery may be performed as a form of primary autologous breast augmentation or as an adjunct to implant-based breast augmentation to disguise implant edges.
Large-volume lipofilling is usually performed in systemic sedation. However tumescent local anesthesia (TLA) has been shown to be the safest method of liposuction.2,3 The limiting factor of TLA, however, is the toxic threshold of the anesthetic. The maximal safe dose for lidocaine is 45 mg/kg. 4 The maximal safe dose for prilocaine, another anesthetic used for TLA, is 35 mg/kg.5,6
In a previously published study, we have already demonstrated the efficacy of a combined tumescent solution containing lidocaine and prilocaine. 7 In this study, we aimed to evaluate the efficacy of large-volume lipofilling in TLA. To reduce costs and operation time, and to decrease the risk of contamination, a closed-loop system was used. Pre- and postoperative data were collected.
Materials and Methods
Between September 2019 and February 2020, 32 consecutive female patients visited our 2 centers in Zurich and Geneva for fat transfer to the buttocks (n = 23) or breast (n = 9). The study was conducted in accordance with guidelines set forth in the Declaration of Helsinki. Written consent was obtained from all patients prior to surgery. The mean age in patients who underwent gluteal augmentation was 40.7 years (range 26-56 years). The goal of gluteal augmentation was to create slightly rounder buttocks with a more caudal projection, and/or to correct trochanteric depression.
Patients who had breast augmentation with autologous fat were generally younger, with a mean age of 30.4 years (range 19-41 years). All patients were opposed to the idea of implants and wished for only a slight enlargement of their breasts, up to 1 cup size. All patients were nonsmokers. A mammogram was performed in all breast augmentation patients prior to surgery.
The donor and recipient sites were marked in a standing position at all times. Tumescent solution contained 2 anesthetics: lidocaine (300 mg/L) and prilocaine (250 mg/L) (Laboratorium Dr. Bichsel, Interlaken, Switzerland). Tumescent solution was either injected with a single-blunt infiltration cannula or with an interconnected flow system using four 18 gauge needles using a roller pump (Dispenser DP30, Nouvag, Goldach, Switzerland). The recipient area was infiltrated with tumescent solution using a cannula. In these areas, the lowest amount possible was infiltrated, as a large amount of tumescent solution will lower the amount of fat that can be successfully transferred. Higher and more superficially injected amounts of tumescent solution were only used in areas within the buttocks, where grade 3 cellulite was present. In these areas, a V-shaped dissection cannula was later used for release of superficial connective tissue bands.
In the donor site, third-generation vibration amplification of sound energy at resonance (VASER) was performed in pulsed mode with 80% using 3.7-mm probes prior to liposuction (Solta Medical, Bothell, WA, USA).
Large bore tubing (Black & Black Surgical, Inc., Tucker, GA, USA) was connected in sterile conditions to a previously used tumescent solution bag, and to a 4-mm flared Mercedes cannula (Microaire, Charlottesville, VA, USA). Negative pressure was created with the very same peristaltic pump used for infiltration, but in a reverse setting. This closed-loop system prevented fat cells from being exposed to air, as the tumescent solution bag expands with the fat graft.
SAFE liposuction 8 was performed using reciprocating power-assisted liposuction (PAL). The collected fat was cooled with cool pads attached to the bag. While centrifugation can increase the operating time dramatically 9 and also increase the risk of contamination, this process has the benefits of preventing compaction of the adipose tissue and preserving its capacity to diffuse into the recipient site. 10 Excess liquid at the bottom of the bag was discarded. We added clindamycin to the collected fat (600 mg/L).
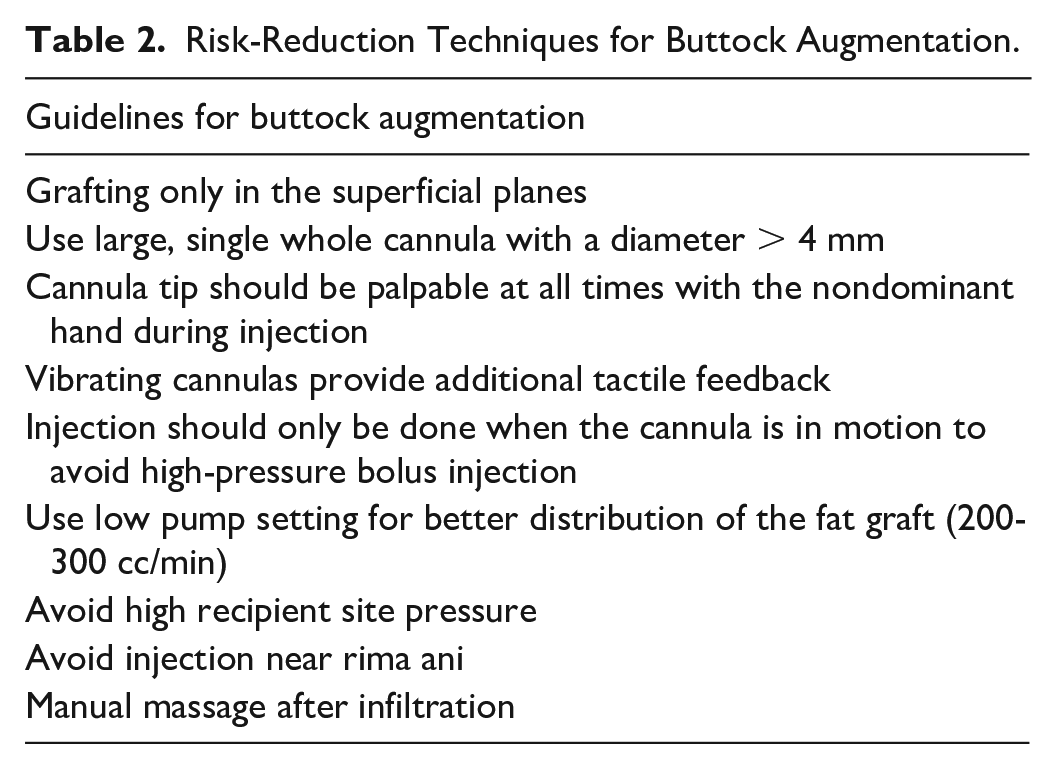
For expansion vibration lipofilling we used 4-mm flared Mercedes cannulas. A large bore tubing to propel fat out the tip of the vibrating cannula at a speed of 200 to 300 cc/min, as previously described. 11 Fat was only injected subcutaneously, and the tip of the cannula was always felt by the surgeon’s hand through the skin, when buttock augmentation was performed, according to published guidelines and set forth by the World Association of Gluteal Surgeons (Table 2). 12 When fat is seen continuously leaving exiting the incision during vibration expansion lipofilling, this is a sign of extremely high recipient site pressure and should be avoided. 12 To avoid high recipient site pressure, we injected serially and in steps of not more than 100 mL (buttock) and 50 mL (breast).
For the transfer of fat to the breasts, we used only one 3-mm stealth slit incision in the inframammary fold, and for the gluteal augmentation, 2 slit incisions inferolateral sacral over the natal cleft.
For all injection sites, we applied the 140% rule, meaning that 140 mL of fat must be injected for a desired final volume of 100 mL. 13
In most cases, nitrous oxide was used during expansion vibration lipofilling. Nitrous oxide was always limited to 30 minutes. An intensive manual massage was performed to further distribute the injected fat and decrease the occurrence of fat necrosis and cysts. To hasten resorption, we asked patients to gently massage their harvesting areas with a circular motion in the first 3 days (breasts). Patients wore compression garments for 3 weeks, specifically designed for gluteal and breast augmentation. We instructed all patients not to apply pressure on the recipient site for 1 week and to preferably sleep in a supine position (breast augmentation) or in a prone position (buttock augmentation) during that time. All patients received an emergency phone number and the surgeon (RB/PvW) could be reached 24/7. All patients received pain killers (mefenamic acid of 500 mg) and were instructed to take up to 3 tablets a day in case of pain. Pre- and postoperative data were collected. Satisfaction rate was evaluated 6 months postoperative on a scale of 1 to 6, with 6 being very satisfied.
Results
There were no major complications. One patient developed a small nodule after fat grafting to the breast, which spontaneously disappeared within a week. Liposuction volumes up to 3.100 mL were extracted from a variety of sites, including arms, waistline, thighs, and calves.
Mean operation time was 96 minutes (range 72-115 minutes). Fat transfer resulted in rounder, slightly elevated buttocks (Figures 1 and 2) and in enlarged breasts (Figures 3 and 4). The injected volume ranged from 200 to 1600 mL for buttock augmentation, and from 100 to 200 mL for breast augmentation.
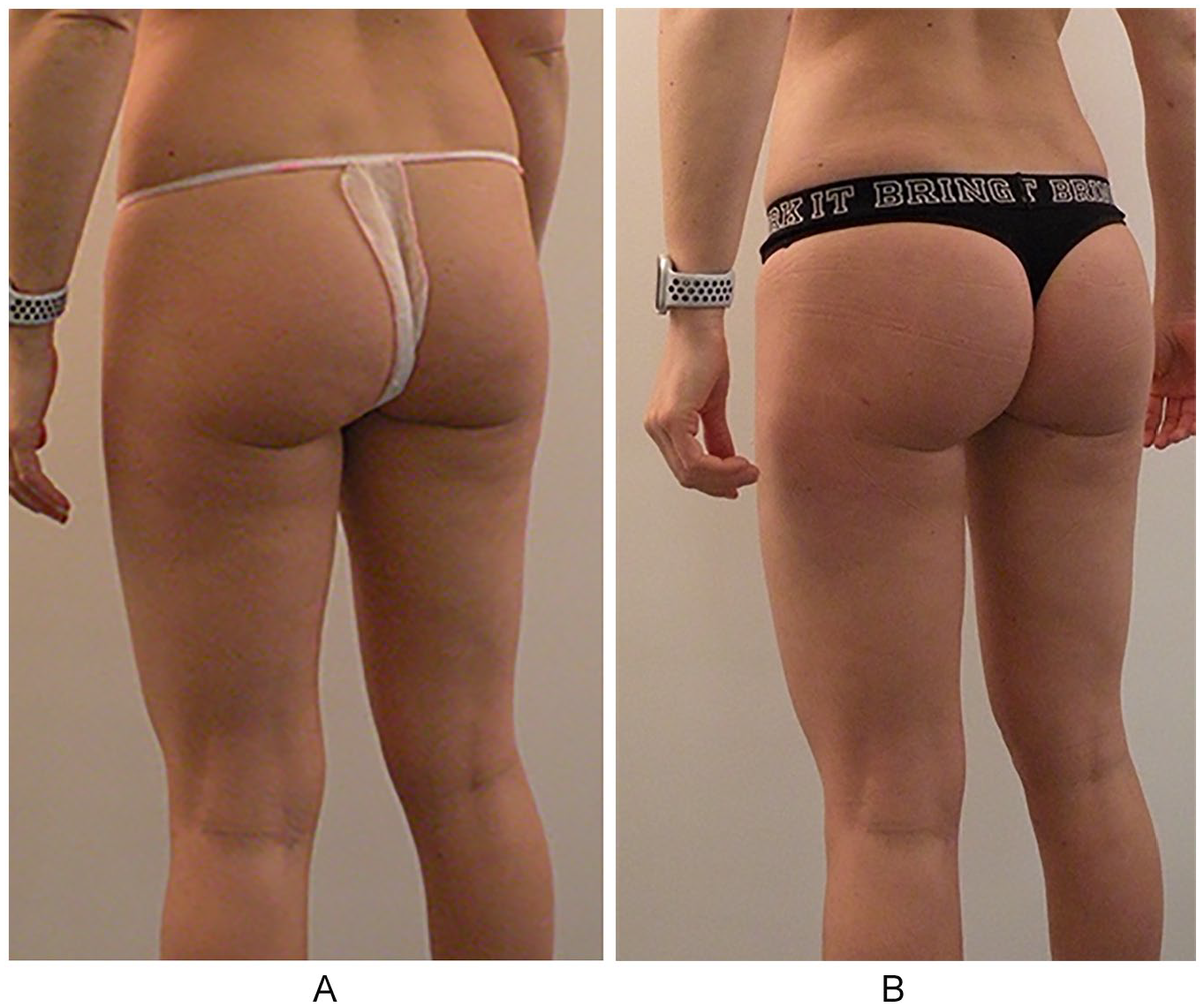
Lipofilling to the buttocks in a 30-year-old female patient: before (A) and 6 months post-op (B).

Lipofilling to the buttocks in a 25-year-old female patient: before (left) and 6 months post-op (right).
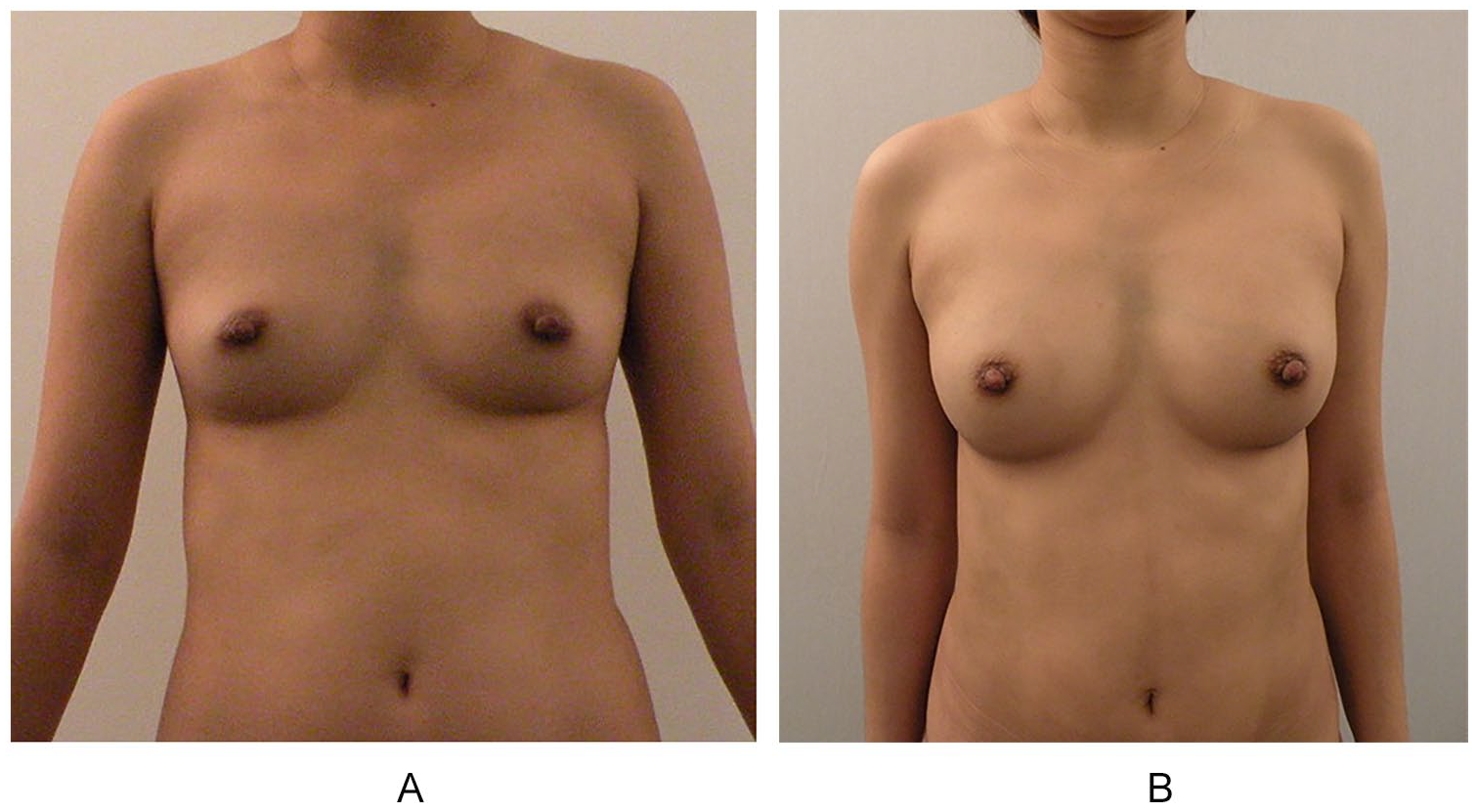
Lipofilling to the breasts in a 34-year-old female patient: before (A) and 6 months post-op (B).
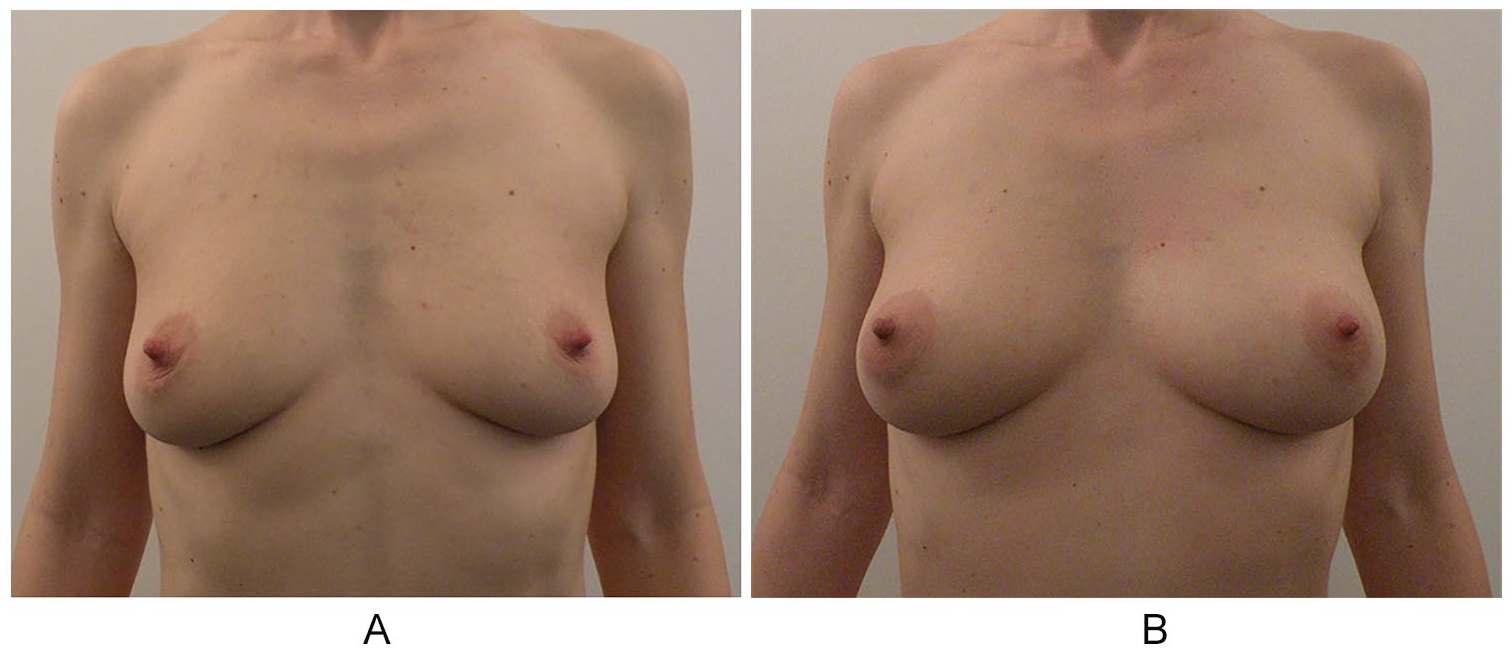
Lipofilling to the breasts in a 39-year-old female patient: before (A) and 6 months post-op (B).
Recovery time was 1 to 2 days in all patients. Mean satisfaction rate was 5.1 on follow-up 6 months after surgery.
Discussion
In this study, we demonstrated the efficacy of large-volume lipofilling in TLA. Prior to SAFE liposuction, 8 VASER was used. The use of ultrasound in TLA allows for efficient harvesting of the mesenchymal stromal cellular fraction of adipose tissue. 14 In a lipolysis assay, a mean correlative viability of 85.1% of harvested adipocytes was demonstrated. 15
SAFE liposuction is a multistep approach to body contouring consisting of fat separation, aspiration, and fat equalization, thus minimizing injury to surrounding structures. 8
The advantage of VASER in conjunction with PAL is a much more homogenous fat graft, where the tubing does not get clogged up. It also allows for a regular flow and better redistribution of autologous fat grafts during expansion vibration lipofilling. The closed system used in this study reduces the risk of contamination and allows for cost- and time-efficient liposuction and large-volume lipofilling.
Fat grafts are composed of adipocytes, stromal vascular fraction cells (adipose stem cells, preadipocytes, fibroblasts, vascular endothelial cells), and immune cells. 16 Stromal vascular fraction cells and adipose stem cells might improve fat graft survival, largely through their angiogenic properties. 17 Blood accelerates the degradation of the transplanted fat and needs to be disgarded. 18
It was previously shown that exposure to tumescent solution enhanced the adipocyte viability in adipose tissue compared with cells isolated by means of dry technique. 19 Analysis of different anesthesia drugs demonstrated greater adipose stem cell viability within adipose tissue treated with lidocaine, bupivacaine, mepivacaine, and ropivacaine compared with combined treatment with articaine and epinephrine. 20 No negative effect of lidocaine plus epinephrine or prilocaine on microangiogenesis and the survival of fat grafts was found. 21
We used large size 4-mm flared Mercedes cannulas for both fat harvesting and expansion vibration lipofilling. Studies investigating differences in liposuction cannula and cannula size have shown that the use of a larger diameter cannula enhances cell viability. 22 The use of large diameter cannula during expansion vibration lipofilling also reduces the risk of fat emboli. 23 It may be that larger diameter cannulae deposit larger parcels of fat that are less likely to enter the blood circulation. 23
Fat was harvested from a variety of different sites, and we did not observe a difference in the viability of fat grafts. This is supported by the literature, where no significant viability in adipose tissue was found regarding donor site. 24
Our fat grafts were cooled with cold pads attached to the bags. Held at 4°C, biological properties of adipose-derived stem cells do not change for up to 3 days. 25 At room temperature, however, adipocyte starts to degenerate and rupture over preservation time. Adipose-derived stem cell yield at room temperature is significantly lower and is maintained only up to 4 hours. 25
Comparative studies investigating the effects of fat processing with centrifugation, washing, and filtration have shown no significant difference in fat retention. 26
Each fat graft processing method has its own merits and shortcomings; however, due to a lack of well-defined prospective studies, there is no evidence to support one processing method as superior to another. 27
We did not have complications in this study, but the low number of patients does not merit conclusions. Fat embolus is of particular concern in buttock augmentation where mostly intramuscular injection of grafted fat has resulted in pulmonary fat embolus and death. 23 The cause of fat embolism during gluteal augmentation is the inadvertent entry of fat into the low pressure superior or inferior gluteal veins. 28
Several task forces have since proposed recommendations regarding injections techniques (Tables 1 and 2):12,29,30 (1) Fat should only be grafted into the superficial planes, (2) the cannula tip has to be palpable with the surgeon’s nondominant hand at all times during injection, (3) vibrating cannulas may provide additional tactile feedback, (4) injection should only be done when the cannula is in motion to avoid high-pressure bolus injection, and (5) the superior and inferior gluteal vessels, as well as superficial branches are found relatively superficial near the rima ani. 12 Therefore, fat transfer to this area needs to be avoided.
Complications of Buttocks Augmentation With Autologous Fat.
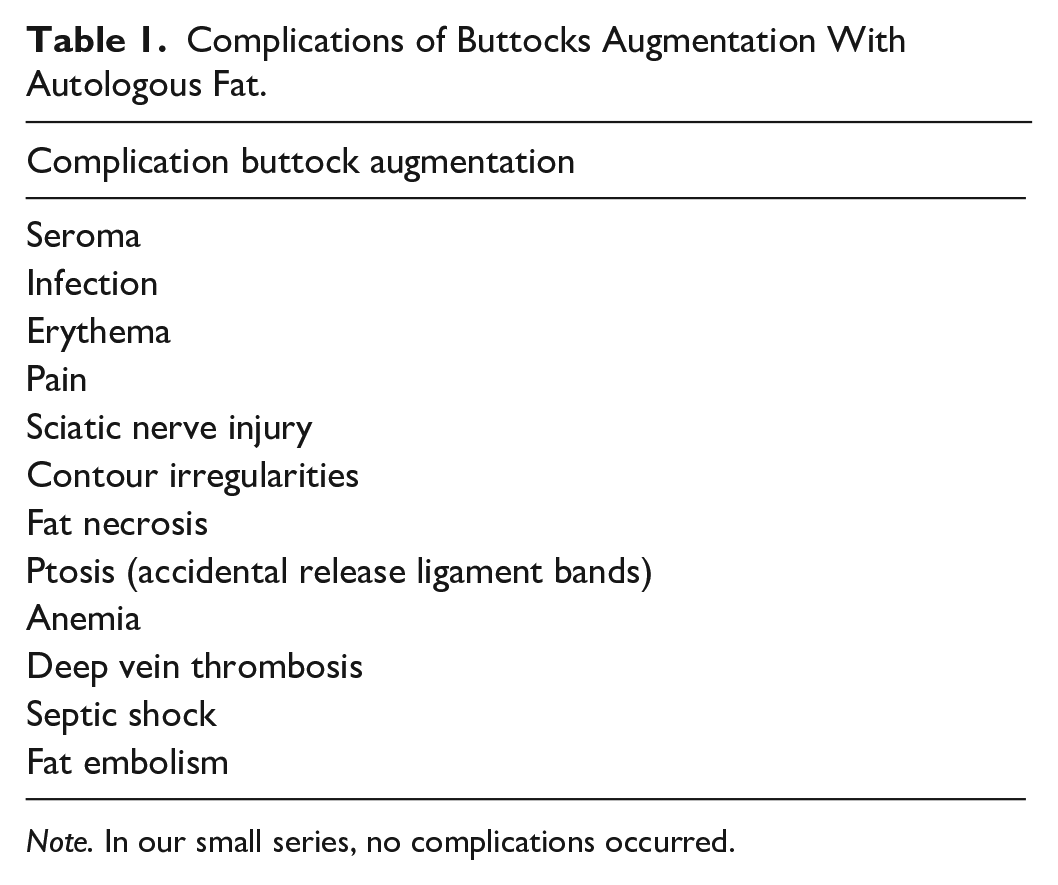
Note. In our small series, no complications occurred.
Risk-Reduction Techniques for Buttock Augmentation.
Other risk include the accidental percutaneous release of ligamentous bands caused by too aggressive tissue damage by the cannula that may result in severe buttock ptosis. 11
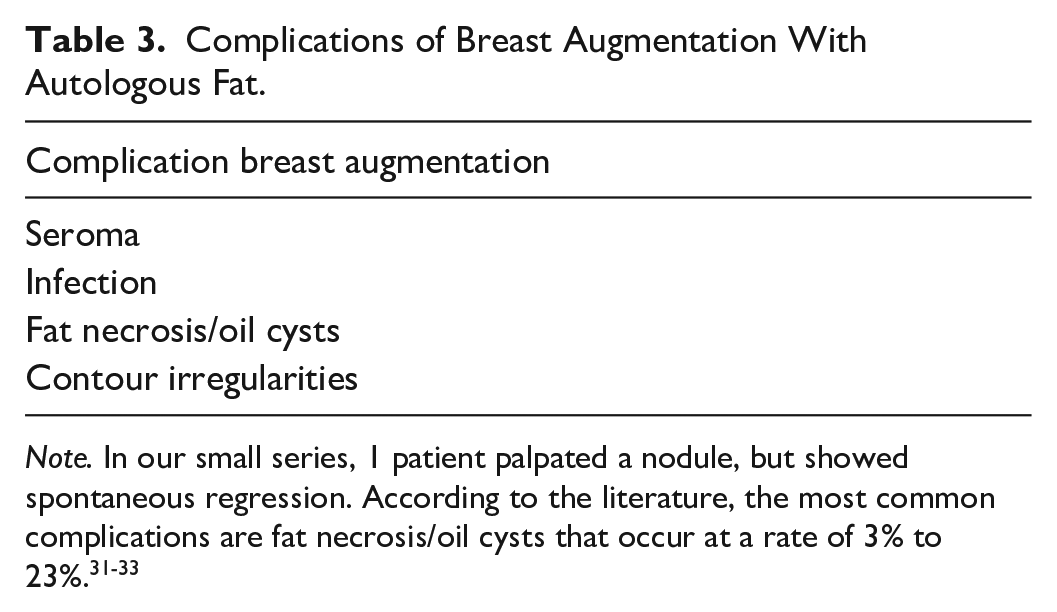
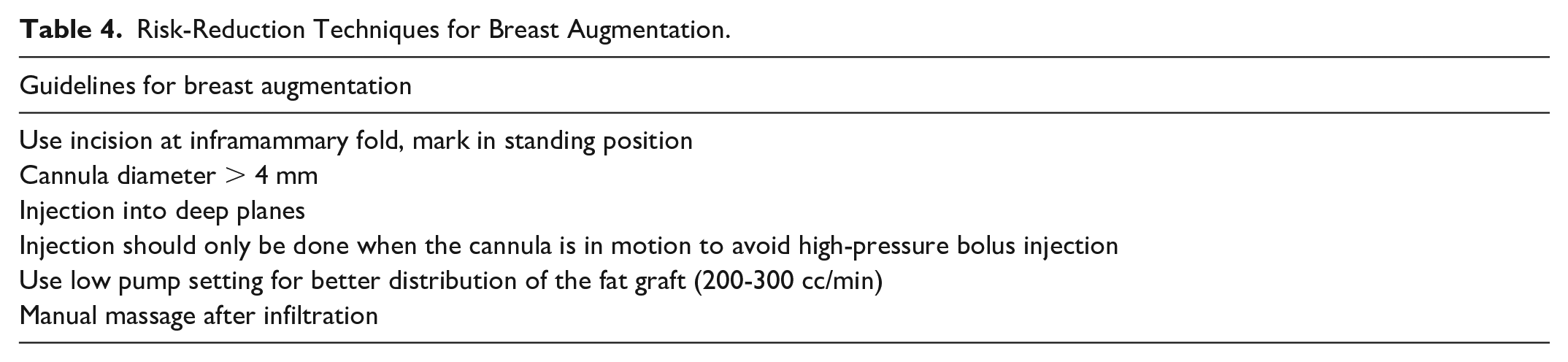
Expansion vibration lipofilling using a slow flow, and with less active axial motion, reduces the risks associated with buttock augmentation. Manual massage may help to better distribute fat grafts, decrease the risk of tissue irregularities, and to reduce the risk of seroma. In breast augmentation, fat necrosis and oil cysts can be reduced with the proper technique (Tables 3-5). Although we had only 1 palpable fat necrosis/oil cysts in our small series, they are described to occur at a rate of 3% to 23%.31-33 Often, fat necrosis disappear spontaneously, as with our patient. Superficial fat necrosis without spontaneous regression may be addressed with lipofragmentation using a disrupter cannula. 33
Complications of Breast Augmentation With Autologous Fat.
Risk-Reduction Techniques for Breast Augmentation.
Benefits and Disadvantages of VASER.
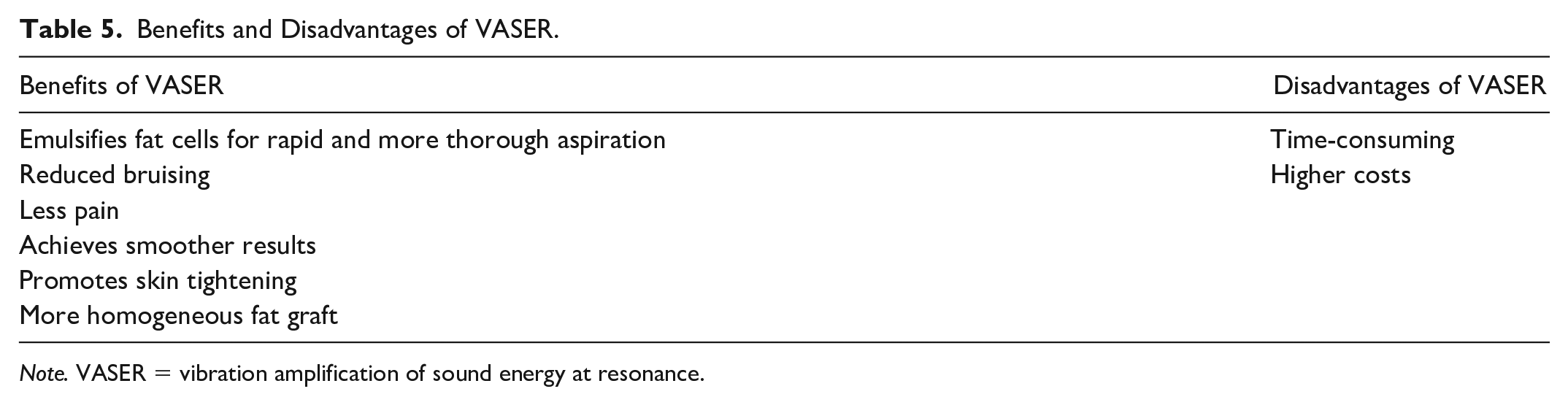
Note. VASER = vibration amplification of sound energy at resonance.
When fat transfer to the breast is performed, mammography prior to surgery is advisable, because fat transfer will result in the formation of microcalcification and may interfere with later breast cancer screenings. 34 There is no indication of an increased cancer risk in the literature, nor a higher frequency of recurrence of breast cancer. 35
Satisfaction rate was 5.1 on follow-up 6 months after surgery, and similar ratings were described in other studies. 11 To conclude, VASER, PAL, and consecutive expansion vibration lipofilling in a closed-loop system is a time- and cost-effective method for large-volume fat grafting. Recovery time is short, with only 1 to 2 days, and there is a high rate of patient satisfaction. Strict adherence to guidelines for lipofilling needs to be followed to minimize complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.