
Abstract
During the COVID-19 crisis, the American Society of Ophthalmic Plastic and Reconstructive Surgeons (ASOPRS) recommended cessation of all nonurgent oculofacial services, imparting unprecedented challenges in patient care and practice management. An anonymous survey was performed to assess surgeons’ surgical, clinical, and financial experiences during the COVID-19 restrictions. Results were collected from April 20 to May 1, 2020 and analyzed. A total 112 ASOPRS members participated. A significant majority (81.52%) performed surgeries during the COVID-19 restrictions. Fourteen percent did not allow trainee participation. While operating, 34.41% always wore an N-95 mask. Preoperative patient COVID-19 testing was mandated in 37.21% of practices. Fewer than half of surgeons were required to leave the operating room during intubation. A large majority (88.76%) of ASOPRS members used telemedicine, with most finding the virtual platform to function moderately well (62.92%) for oculofacial evaluations. Senior ASOPRS members were less interested in continuing virtual patient encounters in the future (P = .0130). Nearly all private practice surgeons (95.38%) had applied for federal funding and 83.51% expressed concern about the long-term financial well-being of their practice. ASOPRS surgeons have provided emergency oculofacial patient care during COVID-19, though often without proper safety precautions. New virtual patient evaluation platforms and financial practice hardships have posed additional challenges.
Introduction
On March 19, 2020, the American Society of Ophthalmic Plastic and Reconstructive Surgeons (ASOPRS) leadership echoed the American Academy of Ophthalmology (AAO) and American College of Surgeons recommendations to cease all nonurgent oculofacial clinical encounters and surgeries.1-3 With the number of COVID-19 cases on the rise in the United States, Surgeon General Dr. Jerome Adams urged health care systems to halt elective procedures to reduce the risk of viral transmission and conserve medical supplies, including personal protective equipment (PPE). Although general guidelines were released by specialty organizations, allowance for physician discretion was granted.1,2 Oculofacial surgeons were faced with unprecedented decisions on how to safely and appropriately provide oculofacial patient care, educate medical trainees, and financially manage their medical practices.
Materials and Methods
An anonymous electronic survey of ASOPRS members was performed from April 20, 2020 to May 1, 2020 to assess their surgical, clinical, and financial experiences during the COVID-19 restrictions. The survey was created via the SurveyHero site and posted on private ASOPRS social media and organizational websites. Results were analyzed using χ2 comparison of 2 proportions, with P values <.05 considered to be significant.
Results
A total of 112 ASOPRS members completed the survey, including surgeons in various stages of practice from all regions of the country (Figures 1 and 2). Respondents included those in solo private practice (17.14%, n = 18), private oculoplastic surgery practice (24.76%, n = 26), private multispecialty practice (35.24%, n = 37), and hospital or university settings (22.86%, n = 24). A significant majority (81.52%) of ASOPRS members continued to perform surgeries during the COVID-19 crisis, using university hospital (69.74%), outpatient surgical center (40.79%), and procedure room (50.00%) settings (Figure 3). Each surgeon’s decision to operate was influenced by national (69.57%), state medical board (34.78%), AAO (80.43%), ASOPRS (77.17%), and local practice-specific (58.70%) guidelines, as well as personal judgment (57.61%). Most commonly performed surgical procedures included periorbital laceration repair (46.74%), eyelid lesion biopsy (45.65%), and orbitotomy for lesion biopsy (43.48%) or abscess drainage (34.78%). Of those surgeons who normally educate ASOPRS fellows, 14.29% (n = 4) did not allow fellow participation in surgical cases, whereas others allowed participation as assistant surgeon (14.29%, n = 4), primary surgeon (50.00%, n = 14), or a combination (21.43%, n = 6).
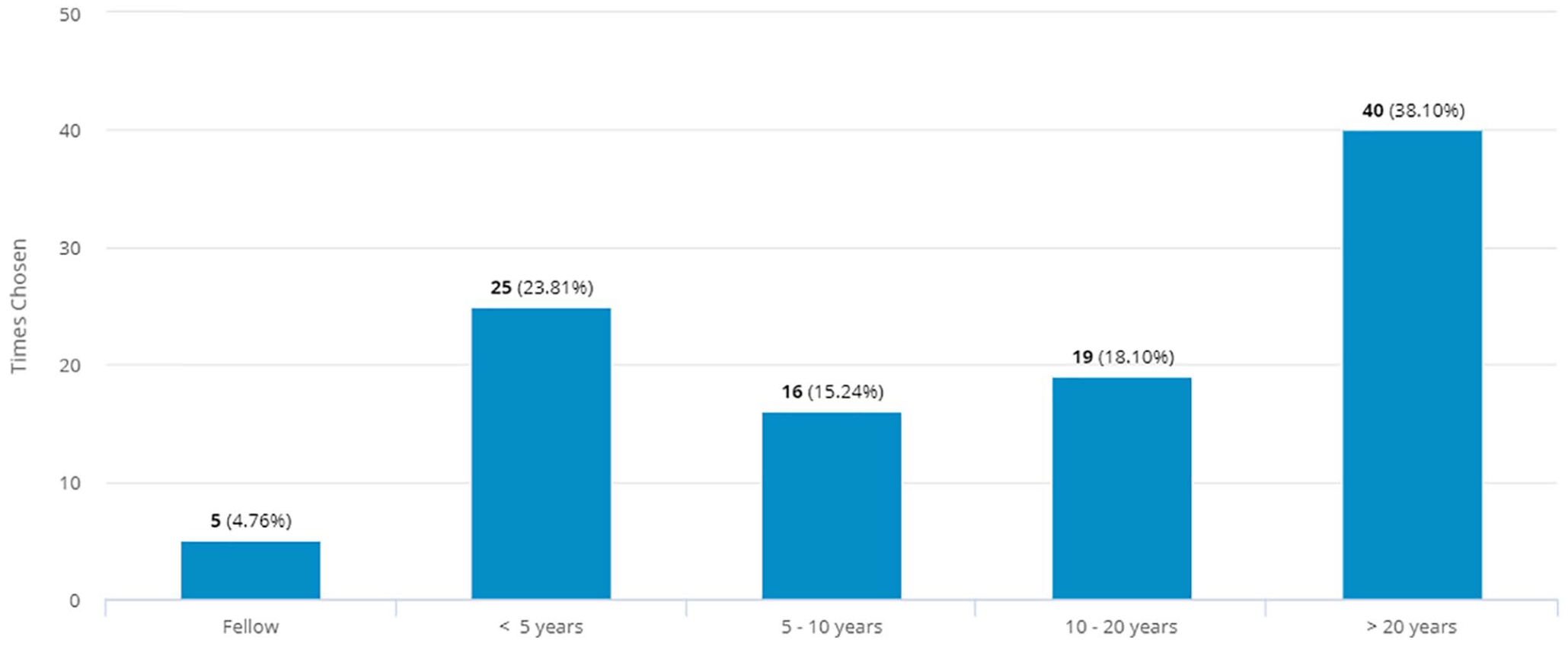
Duration of time in clinical practice.
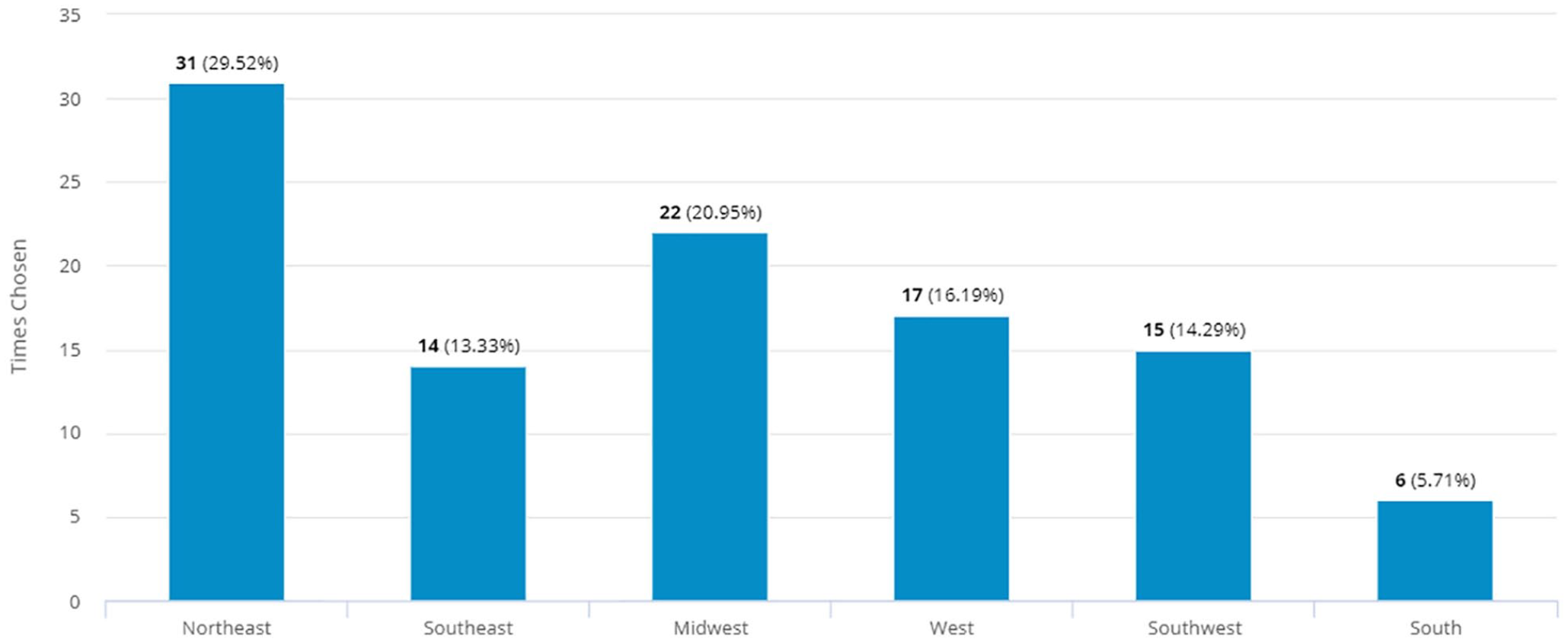
Region of practice.
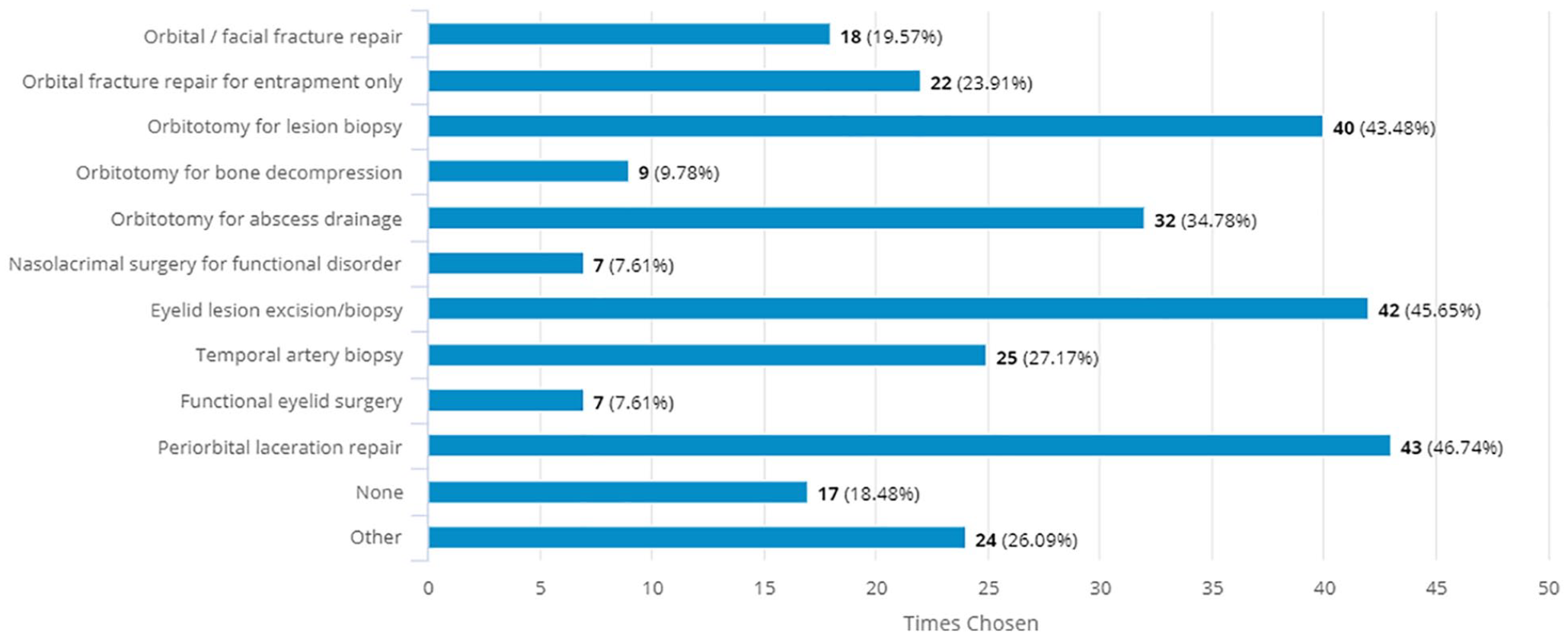
Surgical procedures performed by American Society of Ophthalmic Plastic and Reconstructive Surgeons members during the COVID-19 crisis.
During surgical procedures, 34.41% wore an N-95 mask for all cases, whereas others wore respirator masks only in cases of sinus mucosa exposure (9.68%) or if preoperative COVID-19 test was not obtained (4.30%). Many (24.73%) wore a standard surgical mask only. Preoperative COVID-19 testing of patients was reported by 37.21% of surgeons. While 19.77% (n = 17) of surgeons obtained preoperative viral testing in all surgical patients, 7 (8.17%) did so only in patients with high-risk symptoms or exposures, and 8 (9.30%) for surgeries with planned sinus mucosa exposure. More than half (52.70%, n = 39) of surgeons were not required to leave the operating room at the time of intubation.
ASOPRS members have continued to perform in-person clinic visits for a variety of conditions, including orbital/periorbital infection (63.74%), orbital lesion (57.14%), thyroid disease (50.55%), orbital fracture (47.25%), or eyelid lesion (47.25%) (Figure 4). During these visits, ASOPRS members have worn a surgical mask (68.67%), N-95 mask (44.58%), gloves (67.47%), eye protection (55.42%), and/or gown (6.02%), and many have also mandated that patients wear a surgical mask (76.74%), N-95 mask (3.49%), and gloves (8.14%).
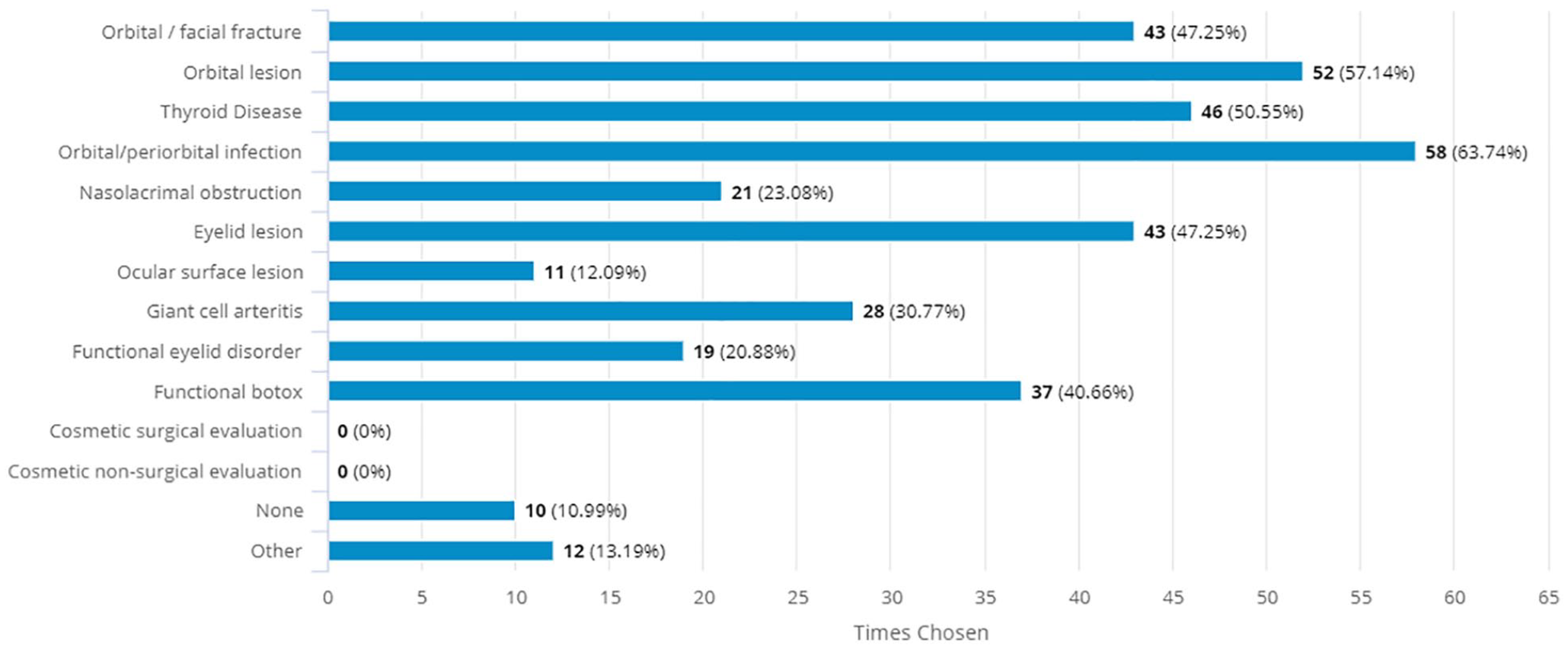
Medical conditions for which American Society of Ophthalmic Plastic and Reconstructive Surgeons members evaluated patients in-person during the COVID-19 crisis.
Many ASOPRS members (88.76%) have transitioned clinical encounters to virtual telemedicine visits (Figure 5), using Zoom (11.25%), FaceTime (11.25%), phone call (15.00%), or other virtual platforms (62.5%), including Doxy.me and WhatsApp. Telemedicine was used by surgeons for new functional (56.41%), new cosmetic (21.79%), urgent consultation (58.97%), postoperative (85.90%), preoperative (7.69%), and follow-up (8.97%) encounter types. Only 4% of surgeons felt comfortable proceeding to surgery based on a telemedicine consultation alone. Most respondents felt that telemedicine functions moderately well (62.92%) or very well (2.25%) for oculoplastic clinical evaluations, whereas 23.60% found it to not work well. When asked about likelihood of incorporation of telemedicine into their post-COVID-19 practice, 36.14% were very likely, 38.64% were moderately likely, and 35.23% were not likely to continue virtual encounters. Those surgeons in practice for fewer than 20 years were significantly more likely to consider continuation of telemedicine than those in practice for more than 20 years (75.9% vs 50.0%, P = .0130).
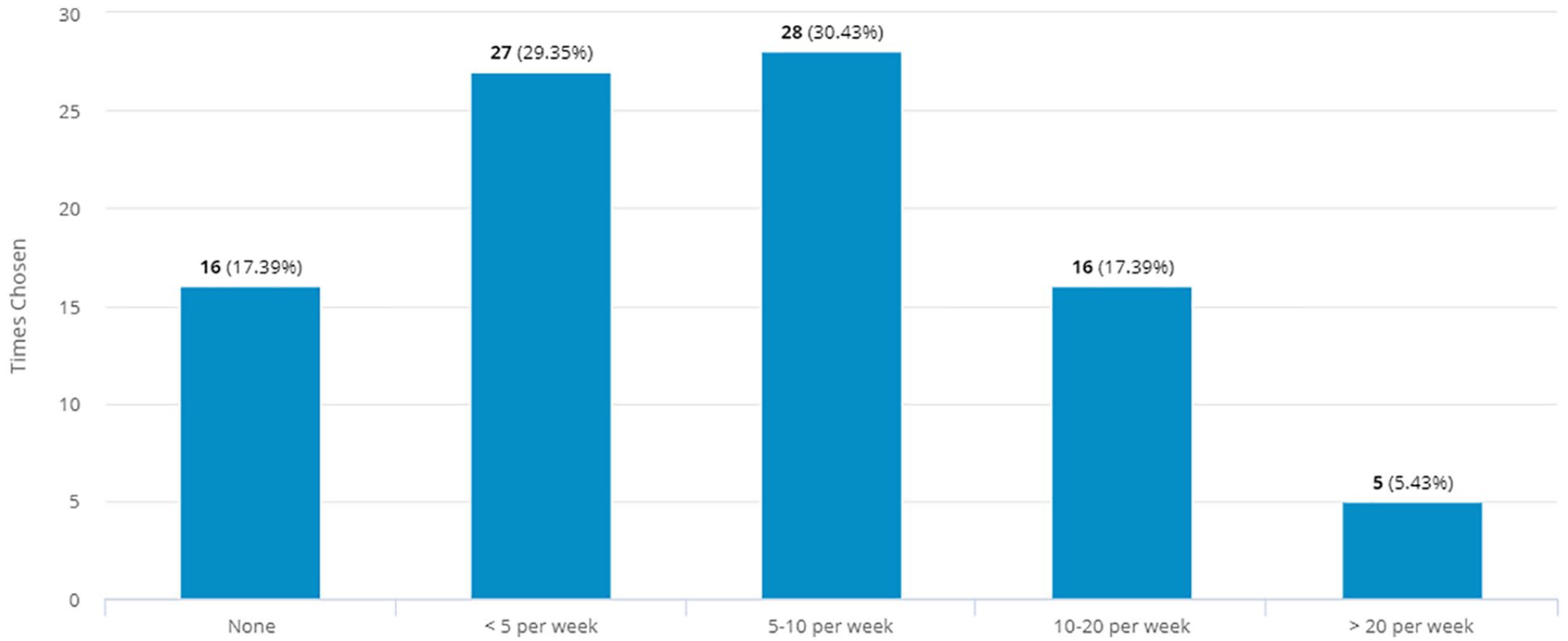
Frequency of telemedicine encounters performed by American Society of Ophthalmic Plastic and Reconstructive Surgeons members.
The financial impact of the COVID-19 restrictions on ASOPRS members was also assessed. Of those eligible for the small business stimulus package, 95.38% applied, but only 58.33% had successfully received funding at the time of the survey. Many ASOPRS members were very (35.16%), moderately (30.77%), or slightly (17.58%) worried about the long-term financial well-being of their practice (Figure 6). All of those (100%) in solo or oculoplastic-only private practice expressed some degree of concern. The vast majority in multispecialty private practice and academic settings were also apprehensive about their financial futures (92.86% and 92.86%, respectively).
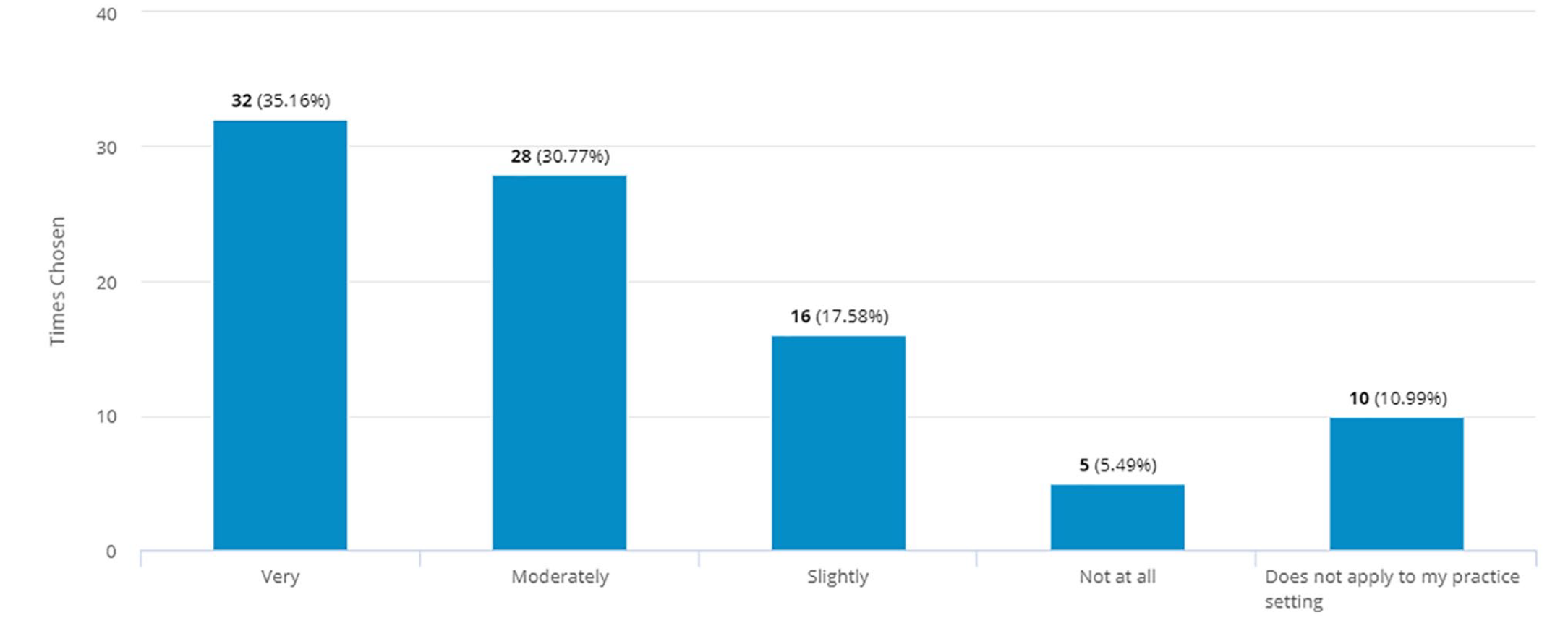
Degree of concern felt by American Society of Ophthalmic Plastic and Reconstructive Surgeons members for the long-term financial well-being of their medical practice.
Discussion
Clinical and surgical restrictions during the COVID-19 crisis have imparted novel challenges for the ASOPRS community. Facial plastic surgeons, including otolaryngologists and ophthalmologists, have been found to be at particularly elevated risks for disease exposure given high viral loads within the upper respiratory system of infected patients. 4 A report of all operating room staff contracting the virus following an endoscopic pituitary adenoma excision demonstrates the severity of this risk. 5 ASOPRS members used a combination of national, regional, and subspecialty guidelines to determine surgical necessity and urgency during this unprecedented time. Eighty-one percent deemed it appropriate to perform one or more surgical procedures, including traumatic laceration repairs, and orbital or eyelid biopsies. Many performed surgeries with potential risk for sinus mucosal exposure, including orbital abscess drainage (34.78%), orbital fracture repair (19.57%), orbital bony decompression (9.78%), and nasolacrimal surgery (7.61%). The minority (14.29%) who train fellows did not allow for the trainee to participate in the surgical case.
Medical organizations have issued recommendations for proper PPE for necessary surgical procedures during the COVID-19 crisis. The American College of Surgeons and European Society of Ophthalmic Plastic and Reconstructive Surgeons (ESOPRS) specifically recommended intraoperative use of N-95 masks, eye protection, gown, and gloves, when possible, in the operative room setting.6,7 Only one-third of ASOPRS surgeons reported use of an N-95 mask for all surgical cases. Surprisingly, a higher proportion (44.58%) reported use of an N-95 mask during in-patient clinic visits, with relatively lower risk of viral transmission. These reports of infrequent proper PPE use likely indicate limitations to full equipment access to ASOPRS surgeons.
Health care systems have instated their own site-specific policies for preoperative COVID-19 testing, varying based on patient risk factors, surgical details, and testing availability. The American Society of Anesthesiologists issued a recommendation for perioperative symptom screening, without formal viral testing, for all surgical patients. 8 Conversely, select high-risk subspecialties have issued their own mandate for preoperative laboratory testing. 9 Only 37.21% of ASOPRS surgeons reported COVID-19 testing of some patients prior to surgery. Universal agreement on perioperative recommendations may be limited by testing availability and surgical setting.
Endotracheal intubation has been found to carry particularly high risk for viral aerosol-generation, prompting recommendations for only essential personnel to be present during intubation. 10 Many hospitals have since advised that only anesthesia providers be present in the operating room during and for 10 minutes following intubation. Despite these recommendations, more than half (52.70%) of ASOPRS surgeons were not required to leave the operating room at the time of intubation and may have incurred unnecessary exposure. Standardization of intubation guidelines may help to further reduce risk of viral transmission to ASOPRS members in the operating room setting.
In response to the social distancing recommendations during the COVID-19 crisis, the Centers for Medicare & Medicaid Services (CMS) and numerous commercial health care plans have amended policies, including waived co-pays, to encourage utilization of telemedicine services. 11 The Office for Civil Rights (OCR) additionally announced that they would “not impose penalties for noncompliance with HIPPA” in connection with “the good faith provision of telehealth during the COVID-19 national emergency”. 12 Accordingly, 88.76% of ASOPRS members have used telemedicine for new functional, cosmetic, postoperative, and follow-up patient visits. While some advocate oculoplastic surgery to be uniquely well-suited for telemedicine visits, 13 23.60% of ASOPRS members found this platform to be ineffective for remote patient evaluations. Meanwhile, almost all (96%) of ASOPRS surgeons felt that an in-person preoperative visit would still be required prior to proceeding with surgery. It is yet to be determined to what degree telemedicine will continue for oculofacial surgical care in the post-COVID-19 era, with only 38.64% of participating ASOPRS members reporting interest in continuing use of this platform, most of whom entered into practice within the past 20 years.
Many ASOPRS members found their medical practices to face new economic challenges from the COVID-19 restrictions, illustrated by the majority (95.28%) in private practice seeking government assistance. At the time of the survey completion, only 58.33% of those members who applied for a payroll protection loan through the small business stimulus package had successfully received funding. It is likely that additional members were subsequently granted aid. The significant majority of ASOPRS members expressed concern about the financial well-being of their practices, including those in multispecialty private practice and academic settings. This sentiment has been widely shared across medical specialties, with telehealth reimbursement only partially offsetting the financial devastation, and many medical groups being forced to decrease wages and furlough or lay off staff. 14 Many also warn that the outpatient health care system will not regain full capacity for the foreseeable future, due to continued risk for viral resurgence. Imminent resumption of usual medical services will hopefully reinstate financial security while maintaining patient and provider safety.
This study is limited by its imperfect response rate that captures only a portion of the total ASOPRS membership. However, the respondents encompassed surgeons in all stages of practice, from all country regions and practice settings, and thus is likely a representative sample of the ASOPRS population. The survey responses during a fluid pandemic crisis capture only the surgeon experience at the time of the study. Future follow-up surveys may be of benefit.
Conclusions
The COVID-19 crisis has posed unique clinical and management challenges for ASOPRS members. Despite personal risk, ASOPRS surgeons have continued to provide emergency oculofacial patient care, though often without the optimal recommended PPE or peri-anesthetic precautions. Clinical evaluations have largely transitioned to a telemedicine setting, albeit with mixed reviews, particularly by senior members. Nearly all ASOPRS members additionally face mounting concern for the future financial well-being of their practices. As care restrictions begin to be lifted, the ASOPRS community should ban together to find solutions to optimize practice fortitude, practitioner safety, and patient health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Method of Literature Search
Given the fluid and often non-peer review nature of articles pertaining to the ongoing COVID-19 crisis, the search was performed in the following ways:
Google search—“COVID-19” and “surgical training” or “oculoplastics” or “ASOPRS” or “fellowship” or “PPE” or “telemedicine” or “financial impact.” All encountered articles were in English. All articles available at time of article preparation (April 1-June 1, 2020) were included. Articles cited in reference lists of other articles were included.
NCBI search—“COVID-19” and “surgical training” or “oculoplastics” or “ASOPRS” or “fellowship” or “PPE” or “telemedicine” or “financial impact.” All encountered articles were in English. All articles available at time of article preparation (April 1-June 1, 2020) were included. Articles cited in reference lists of other articles were included.