
Abstract
Background:
Ultrasound-assisted liposuction (UAL) and power-assisted liposuction (PAL) have been independently shown to homogeneously aspirate higher amounts of fat, better protect tissue, and reduce hematoma formation when compared with standard liposuction (SL). Most liposuction surgeons use either one of these devices. In this study, we aimed to evaluate the safety of combining both methods in local anesthesia in a series of consecutive patients.
Materials and Methods:
Between March 2020 and March 2022, 956 patients underwent ultrasound UAL, followed by PAL in local anesthesia. There were 623 females and 333 males (mean age = 40.3, range = 21-67 years). Intraoperative and postoperative data were collected, and side-effects were noted.
Results:
Mean operation time was 83 minutes. There were no severe complications, and no hospitalizations were required. Minor complications included seroma (9), post-liposuction hyperemia (7), and hyperpigmentation (3). Eighteen patients required touch-up.
Conclusion:
Combining UAL and PAL in local anesthesia shows a safety profile similar to SL, provided these energy devices are used by experienced surgeons. After a learning curve, surgery time is comparable to SL.
Introduction
Liposuction ranks among the most commonly performed aesthetic procedures today. 1
Introduced by Klein in 1985, tumescent infiltration is a type of local anesthesia for cutaneous and subcutaneous surgery, where large amounts of dilute local anesthetic are subcutaneously administered, with either a blunt cannula or needles. 2 The tumescent solution containing saline, adrenaline, and lidocaine enlarges the target area, reduces pain and bleeding during and after surgery, and also has antibacterial properties. 3
Tumescent liposuction in wide-awake local anesthesia was shown to be safe, providing it is performed by an experienced surgeon and the guidelines of care for liposuction are strictly followed.4-6
Limitations of standard liposuction (SL) include excessive hematoma, surgeon fatigue, decreased effectiveness in fibrous areas (in gynecomastia and areas where liposuction was previously performed), contour irregularities, and limited aspiration volume.
Energy devices have been introduced to facilitate fat removal, allow for a more homogeneous aspiration, shorter procedure time, reduce surgeon’s fatigue, and reduce hematoma and postoperative pain.7-9 The most widely used energy devices include ultrasound-assisted liposuction (UAL) and power-assisted liposuction (PAL).
Ultrasound waves which apply internally to the fatty tissue using a titanium probe, cause repetitive expansion and passive contraction of adipocytes, preserve cell membranes and are termed cavitation. 10
The homogenization of fat is then followed by PAL, which is an intensification of SL involving a rapidly reciprocating cannula, thus creating a “jackhammer effect,” which replicates the surgeon’s back and forth movement at an amplitude of 3 mm. 11
The objective of this study was to evaluate side effects in a larger series of consecutive patients, where both energy devices were used, ie, fourth-generation ultrasound liposuction devices, followed by PAL devices.
Materials and Methods
Between March 2020 and March 2022, 956 consecutive patients underwent UAL, followed by PAL in local anesthesia. There were 623 females and 333 males (mean age = 40.3, range = 21-67 years). Intraoperative and postoperative data were collected, and side-effects were noted.
Hemoglobin levels were normal in all patients, and potential interaction with other prescription drugs was evaluated.
To increase the volume of the tumescent solution without increasing the risk of potential systemic side-effects of the anesthetics, we used a combination of lidocaine and prilocaine (Laboratorium Dr. G. Bichsel, Interlaken, Switzerland). This combination is still widely used by several liposuction surgeons, mainly in Germany.12-14 We used a combination of saline, adrenaline, lidocaine (300 mg/L), and prilocaine (250 mg/L). Potential decrease of body temperature due to the high tumescent solution volume was addressed by using preheated solution and heating blankets.
To reduce the risk of infection, antibiotic prophylaxis was performed with 200 mg of doxycycline daily for 5 days. We used an interconnected flow system with four 28-gauge needles (Vacuson 60 LP, Erlangen, Germany) to allow for more painless infiltration. Vibration amplification of sound energy at resonance (VASER) was performed in pulsed mode with 80% using 3.7-mm probes prior to liposuction (Solta Medical, Bothell, WA). This was then followed by reciprocating PAL (MicroAire, Charlottesville, VA).
Incisions were left open (open drainage technique). To limit methemoglobinemia due to the anesthetics, mainly from prilocaine, vitamin C (1000 mg) was given orally before the patients left our day clinic. Patients were wearing compression garments for 3 weeks. Lymphatic drainage was encouraged after 48 hours. Endermology was performed in most patients starting 1 month after surgery. Patients were able to reach our day clinic 24/7 using an emergency phone number. The surgeon called every patient the day following surgery. Follow-up was scheduled 2 and 6 months after surgery.
Results
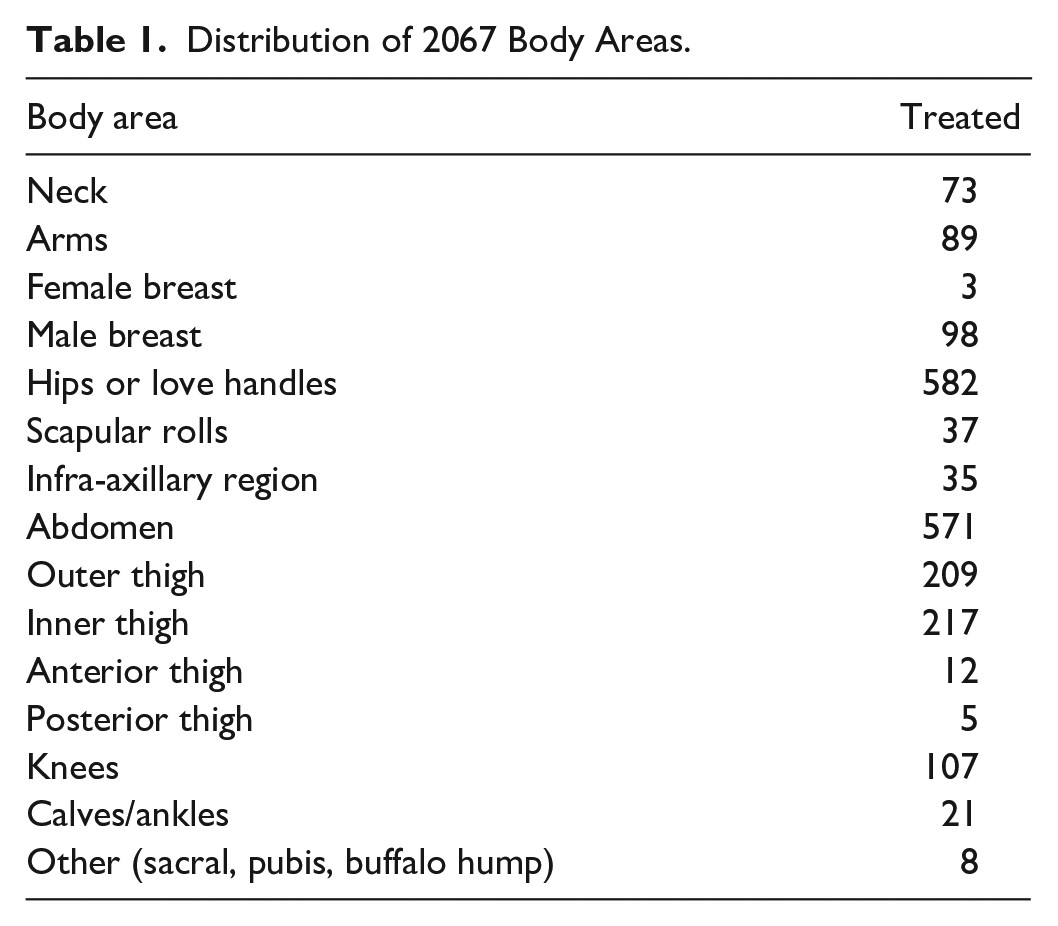
Overall, a combined number of 2067 areas were treated (Table 1). The mean infiltrated volume of tumescent solution was 6.2 L (range = 0.3-13 L), mean aspirated volume was 2.3 L (range = 0.1-5.2 L). Mean operation time was 83 minutes. After a learning curve using these energy devices, surgery time when using both UAL and PAL was comparable to previous surgery times, where only SL was used (unpublished data). There were no severe complications and no hospitalizations. Minor complications included seroma (9), post-liposuction hyperemia (7), and hyperpigmentation (3). All patients with seroma were male patients, where high-definition liposuction was performed. In total, 93 male patients underwent high definition liposuction, and the occurrence of seroma in this high-definition liposuction group was 9.6% (9 of 93). Most frequently, seromas were located on the lower part of the linea semilunaris (n = 6). Three seromas developed on the lower back. Fine-needle aspiration was performed in all cases to reduce patient’s discomfort and infection risk. Post-liposuction erythema improved in 5 out of 7 patients after 6 months. Eighteen patients required touch-up.
Distribution of 2067 Body Areas.
Discussion
In this study, we evaluated the occurrence of adverse effects in a larger series of patients undergoing UAL followed by PAL. In this series, the most frequent side-effect was seroma (n = 9).
All patients developing seroma were male patients, where high definition liposuction was performed.
Seroma develops more frequently when abdominal etching is performed, due to superficial liposuction, which enhances definition lines in between muscle groups. In a previously published series on patients undergoing high-definition liposuction, we found no statistically significant difference of the occurrence of seroma, whether PAL was used alone or in combination with UAL. 15 We therefore attribute the occurrence of seroma to the high definition technique, and not to energy devices.
Seven of 956 consecutive patients in this series developed post-liposuction hyperemia and 3 showed hyperpigmentations, a process of hyperinflammatory reaction that is associated with fibrosis and hyperpigmentation. Post-liposuction hyperemia is a localized, cutaneous condition consisting of reticulate hyperpigmentation and telangiectasias. It is caused by a partial destruction of the superficial vascular plexus that is intimately associated with the immediate undersurface of the dermis. Impairment of the superficial vascular plexus can either be mechanical due to too superficial liposuction (SL or PAL), or due to repetitive and prolonged exposure to heat (UAL), or both. In our case series, one or both factors may have contributed to this post-liposuction erythema. If there is only a slight redness, the condition will resolve by itself over several months or years in our experience. Treatment with topical tretinoin or intense pulsed light may improve the appearance. 16 Three patients developed hyperpigmentation after heat burns.
One of the major shortcomings of UAL is probe overheating and possible tissue damage, as described above. The recently developed fourth-generation US equipment was an advancement to avoid overheating injuries. It takes extensive training time, devotion and great skill to be good with ultrasound devices, as well as crucially needing to respect the body’s tissue and know how much energy to apply in which location and at what setting.
We used the so-called VASER mode in all our patients. The energy can be regulated either as a continuous wave or in pulsed mode, where the energy is delivered in short-duration bursts—around ten bursts per second—referred to as VASER mode. The advantage of VASER mode is that the energy is strong enough to burst fatty tissue while the average energy delivered over time is reduced. The amount of energy delivered to the target tissue is roughly proportional to the square of the diameter of the ultrasound probe; a reduction in diameter results in significant reductions in delivered energy.10,17 The number of grooves at the tip of the probe determines the relative partitioning of the vibratory energy. Energy delivered mainly to the front surface to the probe is ideally for fibrous tissue. Increasing the number of grooves moves more energy to the sides of the probe. A 3.7-mm probe without grooves delivers 100% of the energy to the front surface (the tip) of the probe, while a 3.7-mm probe with 3 grooves delivers 42% of the energy to the front surface, and 58% of the energy to the sides, making the process in soft tissue more efficient.10,17 To reduce potential side-effects of probe overheating using UAL, less energy is better and working deeper is safer. 18
With our current infiltration set-up using needles, the ratio of wetting solution to the total aspirate is roughly 3:1. Using UAL, the ideal ratio of wetting solution to the total aspirate, however, is 1.5:1.10,17 Therefore efficiency decreases with the excessive fluid we are using, and the risk of probe overheating is diminished.
The occurrence and frequency of adverse events in this study using both UAL and PAL appears to be comparable to previously published patients series, where only SL has been used.4,6
According to the current literature and our own observation, there are several benefits of a combined use of UAL and PAL over SL:
Vascular injury and hematoma are reduced. This has been reported separately for both UAL8,9 and PAL. 7
UAL is particularly beneficial when areas of high resistance are encountered, such as in areas with high fibrosis, like gynecomastia. Revision rates for SL in the treatment of gynecomastia were 19% in SL vs 2% in UAL. 19 UAL is also beneficial in areas where liposuction was previously performed, and we found UAL particularly useful in areas like the upper back and in chin liposuction where there is high resistance (unpublished data).
Both UAL and PAL are more efficient than SL and reduce surgery time.7,8
Diminished resistance through ultrasound waves in UAL and due to the “jackhammer” effect in PAL reduces surgeon’s fatique.7,8
Superficial UAL showed 40% more skin retraction than SL. 20
UAL and PAL are costly investments for the practitioner compared to SL. It remains to be determined whether UAL or PAL or both render better clinical results in high-definition liposuction, or better results overall. A systematic review of different surgical techniques and outcomes did not find a demonstrable benefit outside the above-mentioned listed exceptions. 11
Clinical outcomes, however, are difficult to objectify. Our observation is that these energy devices result in a generally more rigorous fat extraction, a smoother skin surface, and more marked definition lines in patients where high definition liposuction was performed.
One has to be aware, however, that there are a number of other factors that need to be considered regarding the outcome after liposuction. Among those are age, gender, other genetic factors like the individual tissue retractability, previous weight fluctuations of the patient as well as weight loss after surgery, and exercise. A major factor, in any case, is proper patient selection and, above all, the surgeon’s skill.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.