
Abstract
Introduction:
This study introduces protocols for using hybrid fillers (mixing calcium hydroxylapatite and hyaluronic acid) in facial, jaw, neck, and hand aesthetic treatments. The goal is to establish clear, standardized procedures to enhance effectiveness and safety.
Methods:
The study outlines detailed protocols for using hybrid fillers in aesthetic treatments, covering patient selection, injection techniques, and posttreatment care for face, jaw, neck, and hands.
Results:
The detailed descriptions empower clinicians with insights to implement standardized approaches using hybrid fillers. They aim to optimize procedural accuracy and effectiveness while reducing the risk of complications.
Conclusions:
The hybrid filler protocols standardize aesthetic treatments, aiding in optimal outcomes and guiding clinicians in enhancing their practice. In addition, these protocols serve as a valuable reference, offering comprehensive guidelines for future research in the realm of hybrid filler utilization in aesthetic medicine.
Introduction
The use of the hybrid filler mixtures, which combine (premix) calcium hydroxylapatite (CaHA) and hyaluronic acid (HA) fillers, has gained popularity in the field of aesthetic medicine.1 -4 However, the lack of standardization in the application of hybrid fillers has led to variations in treatment outcomes and an increased potential for complications. Many physicians are taking advantage of the complementary mechanisms of action of HA and CaHA fillers by combining them, so that patients receive both fillers in a single injection session.
Premixing CaHA with HA serves a dual purpose. First, it capitalizes on CaHA’s high G’ and HA’s smooth texture to create a velvety, creamy-white gel that significantly elevates the tissue, while also being more flexible, adaptable, and easier to administer than CaHA alone. Second, the combination appears to reduce the temporary early loss of volume after injection of CaHA. This volume loss may be due to a relatively quick decomposition of CaHA’s carrier gel or due to a slow collagen metabolism. Hyaluronic acid decomposition takes place slowly and evenly over time. By premixing CaHA with HA, the HA filler will mitigate or prevent this noticeable loss of volume. In addition, as HA gradually decomposes, CaHA’s biostimulatory effect induces delayed collagenesis, shifting the volumizing effect from the HA filler to the CaHA filler. 3 The authors acknowledge that the combination of CaHA and HA alters the rheologic characteristics of the individual filler and that more research is needed to evaluate the rheologic and biostimulatory properties, as well as the longevity of the mixture. They also recognize that not all HA fillers are compatible with CaHA.
The use of cohesive polydensified matrix (CPM) fillers (Belotero range, Merz Pharmaceuticals GmbH, Frankfurt, Germany) has demonstrated both histological (1) and clinical (2) safety. Calcium hydroxylapatite (Radiesse, Merz Pharmaceuticals GmbH, Frankfurt, Germany) has also been shown to exhibit a good safety profile. 5 Premixing the CPM-HA with CaHA can be performed with different products from the CPM-range and using different ratios of both types of fillers. This can make it challenging for physicians wanting to apply the hybrid fillers, to choose the right CPM-HA and the optimal ratio for any given indication. Consequently, the purpose of this study is to present a comprehensive set of guidelines for the application of hybrid fillers in aesthetic treatments using the CPM-portfolio and CaHA. Specifically, we outline a distinct protocol for several treatment areas, including facial volume restoration and lifting (Facial Pro-Lifting), jaw contouring (Jaw Sharp Contouring), neck (Neck Hydro-Lift), and hand (Hand Hydro-Stimulate) enhancement of the volume and improvement of the skin quality.
Method
A systematic review of literature on the use of hybrid fillers and existing premixing protocols was conducted, but no data were found on this topic. To address this gap, a set of standardized protocols for 4 of the most common filler treatment areas was developed by combining existing literature with our clinical experience.
Based on published safety and efficacy data,1 -4 the authors’ technique protocol utilizes CaHA, Radiesse, and CPM-HAs, Belotero range (both products from Merz Pharmaceuticals GmbH, Frankfurt, Germany). The appropriate CPM-HA product is selected based on the treatment concept, with CPM-V (Belotero Volume) used for Facial pro-lifting technique, CPM-I (Belotero Intense) for Jaw sharp contouring technique, CPM-B (Belotero Balance) for Neck hydro-lift technique, and CPM-R (Belotero Revive) for hand hydro-stimulate technique. All our patients were thoroughly informed about the procedure and willingly provided their explicit consent before undergoing any treatment.
Facial Pro-Lifting
This technique is suitable for patients who desire a facial lifting effect. Inclusion criteria comprise patients with facial volume loss and soft-tissue laxity, while exclusion criteria consist of individuals with excessive facial fat or “round/square faces.” The treatment areas include the temples, cheeks, preauricular region, jawline, marionette lines, and nasolabial folds. The CaHA and CPM-V products are premixed using a Luer-lock connector in an empty 10-ml syringe, and lidocaine 2% is added at a ratio of 0.5 ml for every 1 syringe of CaHA (1.5 ml). The 2 gels are transferred between two 10-ml syringes at least 10 times to ensure homogeneity. Two rounds of “foaming” are then performed by aspirating the mixture from one syringe to the other to ensure uniform foam formation. Finally, an additional 10 passes between syringes are conducted to ensure complete homogeneity of the final mixture. The number and ratio of syringes of CaHA: CPM-V used can vary depending on the observed soft-tissue laxity and volume loss of the treated areas. For cases with minimal or little volume loss and laxity, the CaHA:CPM-V mixture can be performed with relatively smaller total volumes and a higher CaHA ratio, such as 1:1 and 1:2, or 1:3, 2:2, and 2:4 for slightly higher volumes. Conversely, when treating a more extensive volume loss and laxity, the total volume of the CaHA: CPM-V mixture can be increased with a relatively higher ratio of CPM-V, to 2:6, 2:7, or 3:8. The authors’ most commonly used mixture comprises 2 syringes of CaHA (3 ml) with 5 syringes of CPM-V (5 ml) and 1 ml of lidocaine 2% (Supplementary Video). All injections are performed using 50 mm × 25 G cannulas (TSK Laboratory, Japan) in the subcutaneous plane in a fanning technique.
Jaw Sharp Contouring
This technique is suitable for patients who desire a sharp jawline contour. Inclusion criteria comprise patients with weak jaws and retruded chin with volume loss (Angle Class II), while exclusion criteria consist of individuals with excessive jaw fat or masseteric hypertrophy. The treatment areas include the posterior jaw angle, anterior jaw depression, chin, and jawline contour (in some cases marionette lines). The CaHA and CPM-I products are mixed using a Luer-lock connector in an empty 10-ml syringe, and lidocaine 2% is added at a ratio of 0.5 ml for every 1 syringe of CaHA (1.5 ml). The mixing and foaming method follows the same technique as described previously. The number and ratio of syringes of CaHA: CPM-I used varies depending on the area needed to be treated. For smaller volume corrections, CaHA:CPM-I ratio’s of 1:1 or 1:2 are applied. For larger areas or volume corrections, CaHA: CPM-I ratios of 2:3, 2:4, and 3:6 can be applied. Similarly, to the Facial Pro Lifting technique, for larger volume corrections a relatively higher ratio of CPM-I is applied. The most commonly used mixture for jawline contour and chin comprises 2 syringes of CaHA (3 ml) with 3 syringes of CPM-I (3 ml) and 1 ml of lidocaine 2%. All injections are performed using 50 mm × 25 G cannulas (TSK Laboratory, Japan) in the subcutaneous plane, with the exception of the chin area, where the injection was directed deeply into the deep fat compartment below the submuscular plane in a fanning technique.
Neck Hydro-Lift
This technique is suitable for patients who desire an improved neck, appearing more hydrated and less “saggy.” Inclusion criteria comprise patients with volume loss and soft-tissue laxity limited to Merz Scale Grade 0-2 for neck volume, while exclusion criteria consist of individuals with excessive laxity or a fatty neck (Merz Scale Grade 3 and 4 for neck volume). The treatment areas include all the neck anterior and posterior to the sternocleidomastoid muscle (SCMM). The CaHA and CPM-B products are mixed using a Luer-lock connector in an empty 10-ml syringe, and lidocaine 2% is added at a ratio of 1.5 ml for every 1 syringe of CaHA (1.5 ml). The mixing and foaming method follows the same technique as described previously. The number and ratio of syringes of CaHA:CPM-B used varies depending on the size of the surface area that is being treated. To treat a localized, smaller area of the neck, a ratio of CaHA:CPM-B 1:1 can be used. For the full area anterior to the SCMM, a higher mixture volume is used, with a CaHA:CPM-B ratio of 2:1 or 2:2. For full neck treatment, anterior and posterior to the SCMM border, an even higher mixture volume, with a CaHA-CPM-B ratio’s of 2:3 or 3:3 may be employed. The most commonly used mixture for anterior neck comprises 2 syringes of CaHA (3ml) with 1 syringes of CPM-B (1 ml) and 3 ml of lidocaine 2%. All injections are performed using 50 mm × 25 G cannulas (TSK Laboratory, Japan) in the subcutaneous plane in a fanning technique.
Hand Hydro-Stimulate
This technique is appropriate for patients seeking to enhance the appearance of their hands by making them appear younger and more hydrated. Inclusion criteria consist of patients with a loss of fatty tissue and visible veins and tendons, while exclusion criteria include those with fatty hands. The treatment areas encompass the entire dorsum of the hands. For the purpose of stimulation and hydration, the ideal filler is CPM-R (Belotero Revive). However, other CPM ranges may be used depending on the Hand Merz Scale Grade. Given their rheological features, we consider CPM-R (Belotero Revive) is appropriate for Grade 0 and 1, CPM-S (Belotero Soft) for Grade 1, CPM-B for Grade 2 and 3, and CPM-V for Grade 4. The CaHA and CPM-HA products are blended using a Luer-lock connector in an empty 10-ml syringe. Lidocaine 2% is then added at a ratio of 1.5 ml for every 1 syringe of CaHA (1.5 ml). The mixing and foaming method follows the same technique as described previously. The ratio of syringes of CaHA:CPM used varies depending on the area requiring treatment. To treat both hands; Grade 0 and 1, CaHA:CPM 1:1 is employed; Grade 2, 3, and 4, CaHA:CPM 2:1 is employed. All injections are carried out using 50 mm × 25 G cannulas (TSK Laboratory, Japan) in the dorsal intermediate lamina in a fanning technique.
Post-Treatment Care
Generally, it is advisable to minimize exposure of the treated area to excessive sun, heat, and ultraviolet light from lamps for approximately 24 hours or until any initial swelling and erythema have resolved. To minimize tenderness, swelling, and bruising, patients can use an ice or cold pack as directed by their physician. Patients should also be advised to promptly report any adverse events (other than mild local reactions) to their physician. In the case of hybrid filler, the authors recommend frequent massage of the treated area twice a day during the first week. In addition to massaging the hands after treatment, patients are advised to sleep with a pillow beside their body with the hands placed on it.
Result
The proposed hybrid filler protocols provide a comprehensive and standardized approach for facial pro-lifting (Figure 1), jaw sharp contouring (Figure 2), neck hydro-lift (Figure 3), and hand hydro-stimulate (Figure 4). The protocols outline patient selection criteria, injection techniques, and posttreatment care, which enhance the precision and effectiveness of the procedures while minimizing the potential for complications.
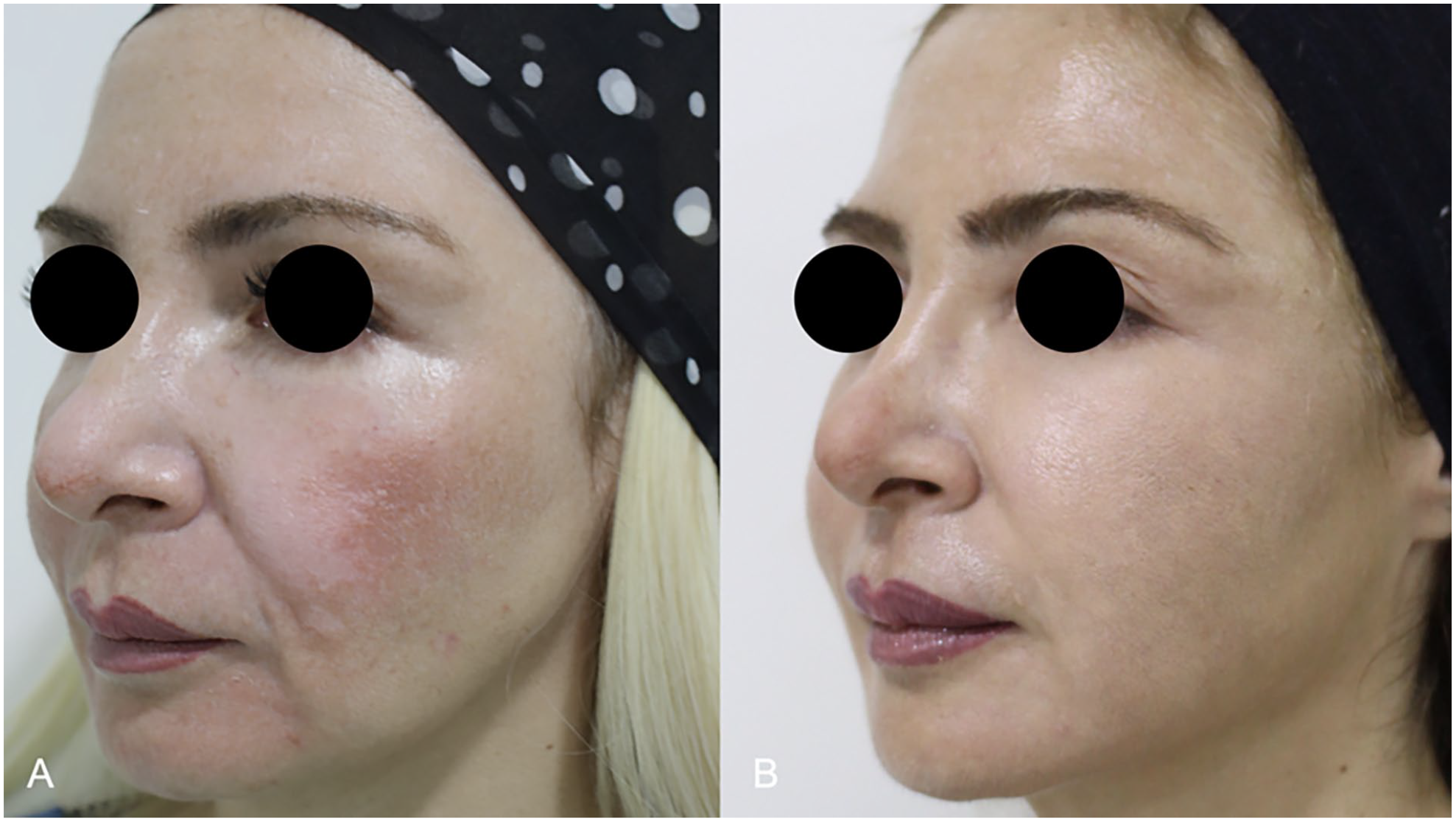
A 46-year-old female seeking complete facial rejuvenation underwent premixed hybrid filler injection (6 ml of CaHA, 7 ml of CPM-HA Volume, and 2 ml of lidocaine 2%). A. Before the treatment. B. Result at 6 months. Note: An additional 0.5 ml of CPM-HA Balance was injected into the tear trough area on each side.
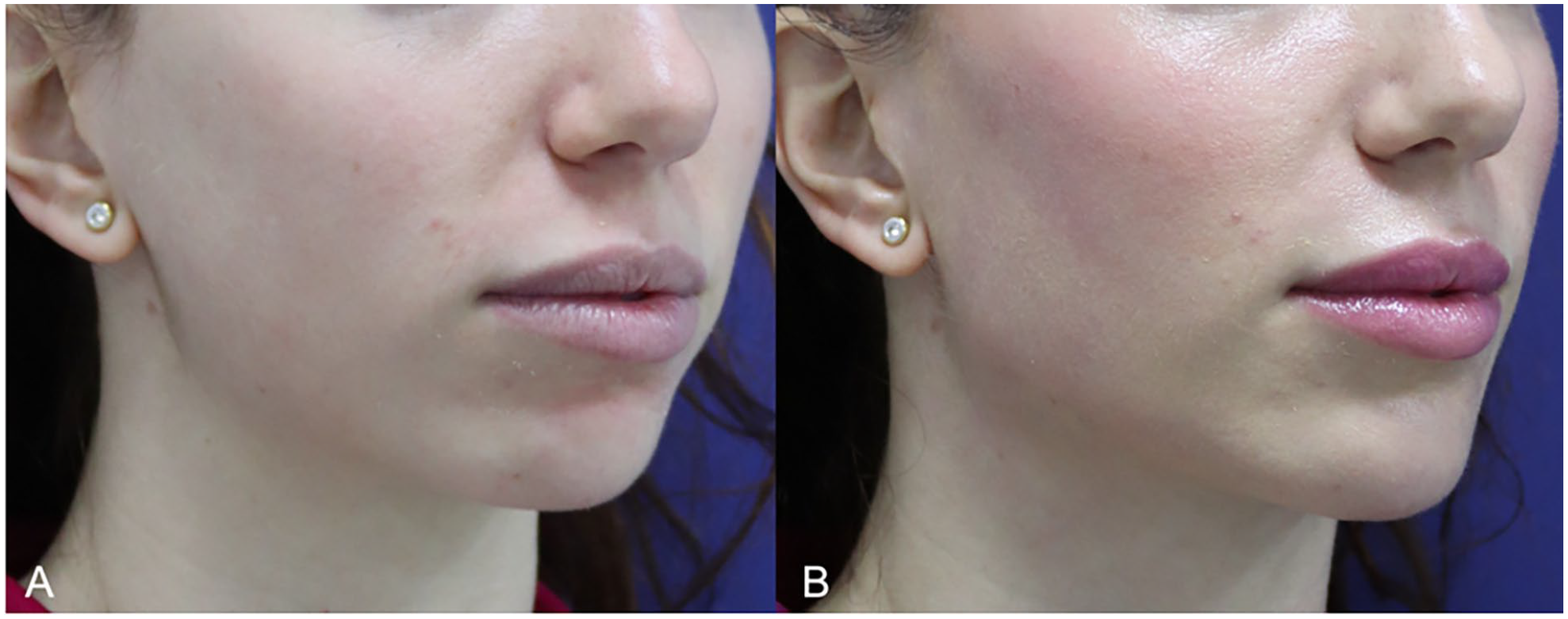
A 30-year-old female seeking jaw and chin contour underwent premixed hybrid filler injection (3 ml of CaHA, 2 ml of CPM-HA Intense, and 1 ml of lidocaine 2%). A. Before the treatment. B. Result at 3 months.
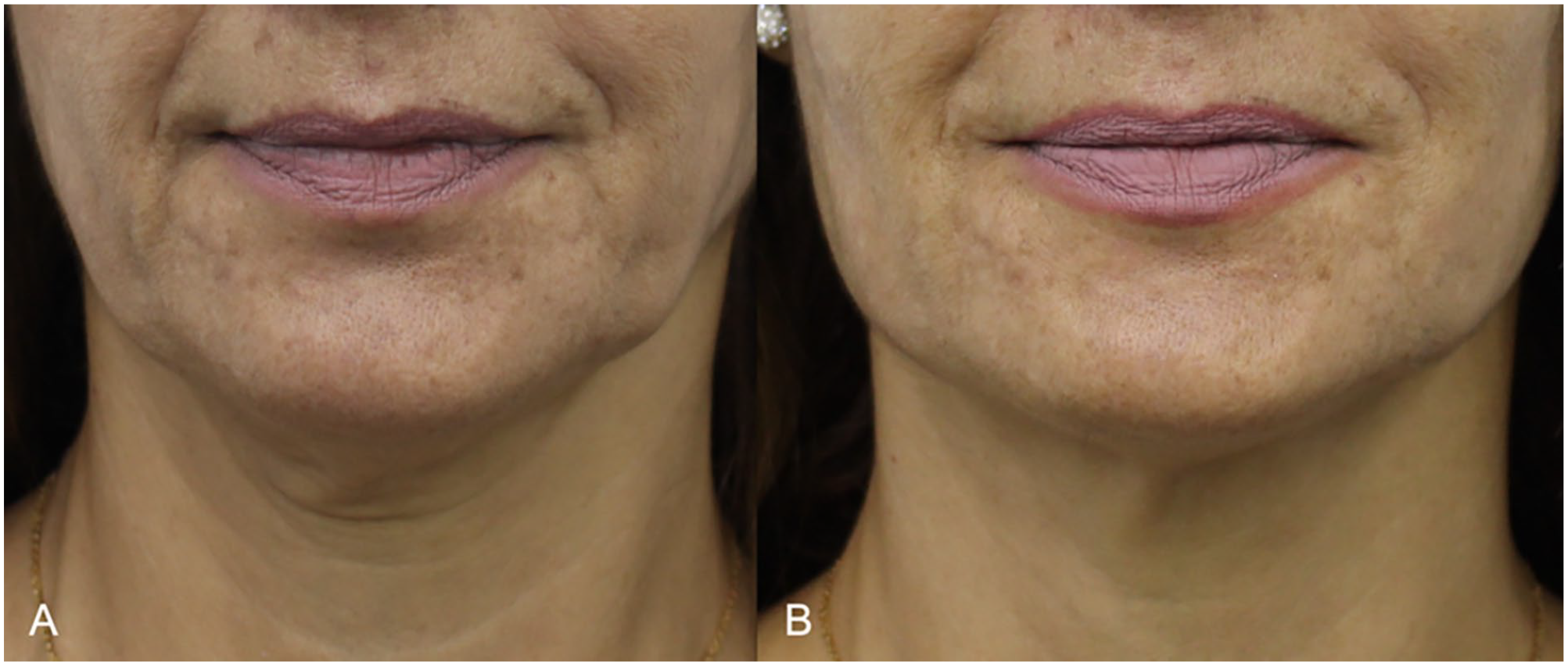
A 48-year-old female seeking neck enhancement underwent premixed hybrid filler injection (3 ml of CaHA, 1 ml of CPM-HA Balance, and 3 ml of lidocaine 2%). A. Before the treatment. B. Result at 2 months.
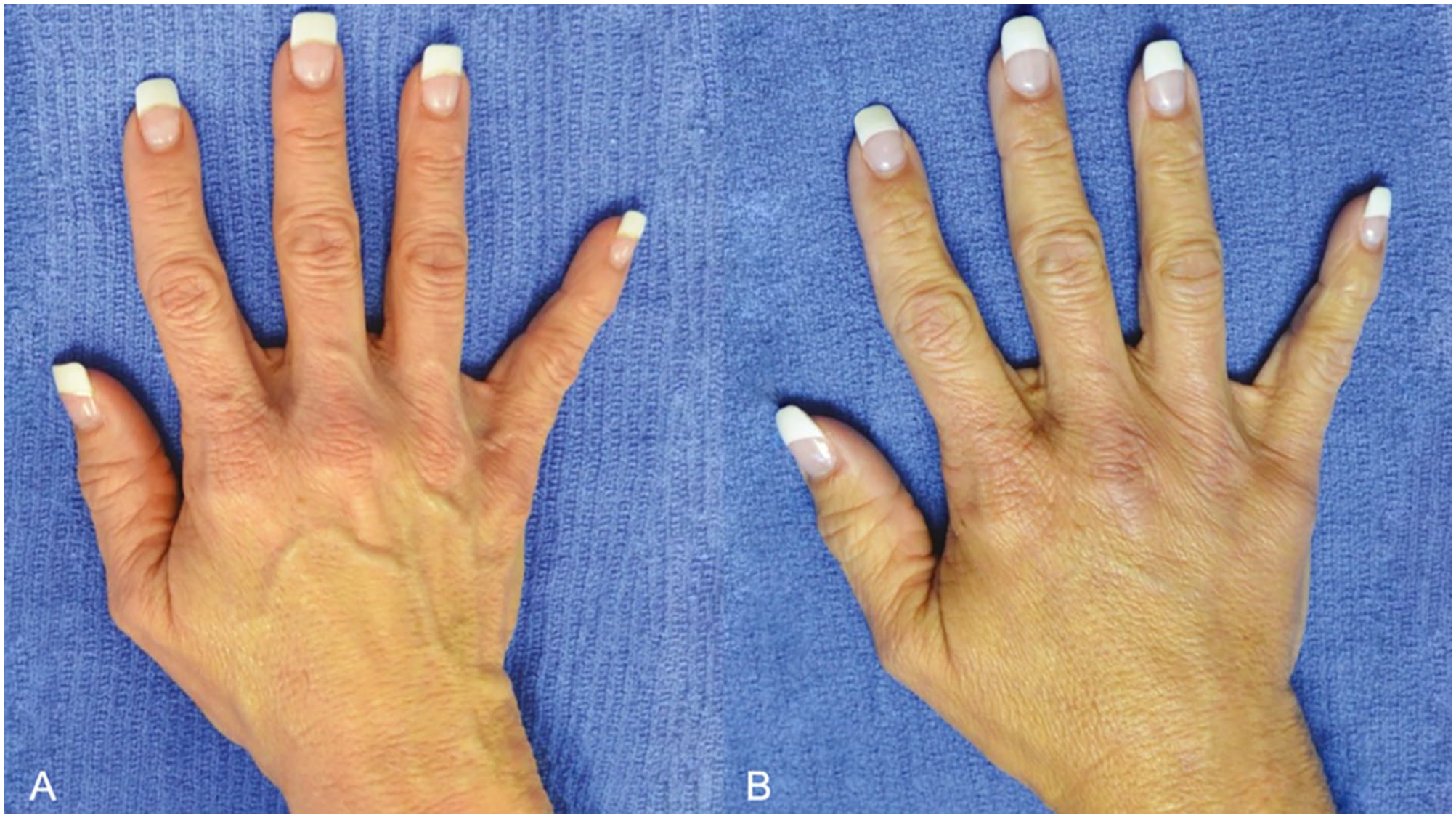
A 48-year-old female seeking hand rejuvenation underwent premixed hybrid filler injection (1.5 ml of CaHA, 1 ml of CPM-HA Revive, and 1.5 ml of lidocaine 2%). A. Before the treatment. B. Result at 3 months.
Discussion
Physicians have made significant strides in the use of CaHA and HA fillers, both separately as together in the same treatment session, and both in terms of indications and techniques. Because of this CaHA and HA fillers are well-established aesthetic treatments with a long history of clinical use and their safety profiles are well documented in the literature.5 -10
Traditionally, the products have been used together for many years, however not premixed. A layering technique was used where CaHA was injected in the deeper soft tissue compartments first to volumize and support overlying tissues, recontour problem areas and stimulate collagen production. Then HA filler was used to smooth out finer lines and wrinkles.11,12 However, some physicians (amongst the authors) have been experimenting with a new approach by premixing the fillers and injecting them from the same syringe.1 -4
The injection of premixed CaHA and CPM-HA offers a combined therapeutic effect in a single treatment. Calcium hydroxylapatite exhibits an immediate volumizing effect and stimulates collagen and elastin production over the long term, making it a desirable agent for aesthetic procedures. On the contrary, HA fillers have hygroscopic properties and can maintain their structure under compressive forces due to water absorption. Hybrid fillers are best injected in the subcutaneous layer (above the SMAS) where the CaHA microspheres can form a scaffold for fibroblast infiltration and encourage the formation of new collagen. After the premixed CaHA:CPM-HA is injected, the HA component will support the CaHA microspheres after the CaHA carrier gel has been degraded, allowing for homogeneous tissue integration. This approach has been shown to be effective in promoting neocollagenesis.13 -15 Similar to CaHA used alone, premixed products may not be suitable for injection into areas with repetitive muscle activity, such as the perioral and periorbital regions. Muscle movements may induce focal accumulation, or clumping of CaHA microspheres leading to nodule formation or noticeable/palpable product.
In the absence of sufficient literature on the use of hybrid fillers, the authors developed a set of standardized protocols for each of the 4 most common treatment areas based on their own clinical experience over a 5-year period. These protocols were refined through a series of case studies, which demonstrated their safety and effectiveness in achieving optimal aesthetic outcomes. Our mixing protocol for CaHA with CPM-HA includes the addition of lidocaine 2% to the mixture. The U.S. Food and Drug Administration (FDA)-approved mixing protocol involves adding 0.11 ml of 2% lidocaine to a 0.8 ml CaHA syringe and 0.26 ml lidocaine to a 5 ml CaHA syringe. However, we used higher concentrations of lidocaine in our protocol as they served a dual purpose. While the original CaHA:lidocaine mixing protocol was developed to reduce discomfort during the injection process, 15 our higher concentrations of lidocaine also lower the G prime and viscosity of the original CaHA formulation, making it softer and easier to inject without compromising the filler’s physiological properties. As dermal fillers are increasingly being used for new indications, physicians have adopted the practice of adding a slightly larger volume of lidocaine to the CaHA to facilitate spreading, although saline can be used as a substitute for lidocaine. To ensure consistent and accurate placement, we administered all injections of the CaHA: CPM-HA combination with a cannula, which reduces product dispersal into multiple anatomical layers.16,17
Common complications are similar among all HA fillers and may include edema, erythema, non-inflammatory, and inflammatory nodules, as well as infections. While these reactions are usually transient, there are other complications that are considered emergencies due to their potential irreversibility, such as anaphylaxis and vascular occlusions. These vascular complications have severe consequences, potentially resulting in persistent skin necrosis, ophthalmoplegia, permanent unilateral or bilateral vision loss, and even strokes.
To date, published reports on premixed therapy have not identified any adverse events or raised any significant safety concerns.1 -4 In a study involving 19 patients followed up for 9 months after receiving premixed CaHA and CPM-B, no complications were reported. 1 Similarly, a retrospective analysis of 134 patients treated with premixed CaHA and either CPM-V or CPM-B identified no adverse events except for 2 cases of overcorrection, which were quickly resolved using hyaluronidase. 2 Another retrospective chart review of 41 patients injected with a premixed combination of CaHA and CPM-V showed no adverse events. 3 These findings collectively suggest that premixed therapy with CaHA and CPM-HA is generally safe and well-tolerated.
The studies discussed demonstrate that restoring the jawline contour is an effective rejuvenation procedure achieved through various injection techniques and products. Chang et al 1 found that premixing CaHA with CPM-HA resolved the issue of early volume loss (probably due to rapid carboxymethylcellulose degradation) after CaHA injection seen in some subjects. In another study, Godin et al 11 found that combining CaHA with HA (Restylane, Galderma S.A., Lausanne, Switzerland) resulted in higher satisfaction rates than using CaHA alone. In our previous study, we mixed CaHA with CPM-HA to benefit from their complementary mechanisms of action (namely stable volumization and neocollagenesis), resulting in improved jawline contour scores at 1 year, demonstrating the volumizing and lifting capacity of the hybrid mix. 3 Patients receiving the CaHA:CPM-HA mixture reported high satisfaction with their immediate and long-term outcomes.3,4 The results suggest that premixing a CaHA with a CPM-HA results in greater satisfaction than using CaHA alone at t = 3 months, but this advantage diminishes at t = 12 months, which may correspond to the degradation of the CPM-HA component of the hybrid CaHA:CPM-HA mix. 3
Further randomized clinical studies are necessary to assess the efficacy, safety, and longevity of hybrid fillers, as well as to determine the rheology of these mixtures for the development of an optimal protocol.
Conclusions
Our proposed hybrid filler protocols offer a standardized approach for aesthetic treatments and facilitate the implementation of best practices for achieving optimal outcomes. The protocols presented in this study will serve as a valuable reference for clinicians seeking to enhance their aesthetic treatments and provide a comprehensive set of guidelines for future research on the use of hybrid fillers in aesthetic medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NF and JK are both consultants for Merz Aesthetics (Frankfurt, Germany).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was performed in line with the principles of the Declaration of Helsinki. This article does not contain any studies with human participants or animals performed by any of the authors.
Consent to Publish
All participants have provided consent for the publication of their photographs.
Data Policy
For this type of study, we don’t have data to deposit in a public repository.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.