
Abstract
Introduction:
Third-generation ultrasound-assisted liposuction (UAL) or vibration amplification of sound energy at resonance (VASER) combined with helium-based plasma technology (HPT) or Renuvion creates a sculpted aesthetic outcome, while optimizing skin tightening in body contouring.
Material & Methods:
A multicenter retrospective chart review assessed safety and efficacy combining UAL with HPT in body contouring of 160 consecutive adult patients presenting from 2018 to 2022 in 2 clinical cosmetic practices. A prospective study evaluated a subset of patients regarding the overall energy delivery measured with the device joule counter using the manufacturers recommended treatment parameters for different anatomical areas.
Results:
Patient satisfaction rate was 95% (152 of 160 patients) using the Global Aesthetic Improvement Scale with no patients noting no change or worse result. No patient experienced a serious adverse effect. The most common complication (14/160 or 8.8%) was a seroma with 9 (5.6%) experiencing minor contour irregularities. Five requested additional liposuction to treated areas. All areas of revision removed less than 10% of the volume removed during the initial liposuction. The overall surgical revision rate was 4.4% (7/160). Radiofrequency (RF) energy delivery for abdomen, flanks, and lower back was 13.8, 15.6, and 3.2 (kJ/cm2), respectively. Keeping treatment planes between 1.3 and 2.3 cm apart achieved 3D RF energy delivery of abdomen, flanks, and lower back of 31.7, 32.8, and 3.9 (kJ/cm3), respectively.
Conclusions:
Third-generation ultrasound-assisted body liposuction combined with internal RF helium-based plasma yields superior patient satisfaction and aesthetic results with no serious adverse effects. Manufacturer energy delivery guidelines appear both safe and effective. Surgeon subjective assessment revealed improved skin retraction over UAL alone by the addition of helium-based plasma.
Introduction
Since its inception, body contouring through fat removal has seen incremental key advancements in technique and technology designed to either heighten the aesthetic outcome or improve safety. Implementing awake, conscious sedation versus general anesthesia, tumescent versus superwet wetting solution infiltration, ultrasound-assisted liposuction (UAL), high-definition sculpting, skin tightening technologies, and the addition of both fat grafting and silastic body implants have resulted in superior, reproducible sexually dimorphic, athletic cosmetic body contouring outcomes.
Manipulating fat to create highlights and shadows, while keeping a smooth body contour, is one main surgical aesthetic goal. The parameter with the most variability is changes to the skin from a combination of the aging process, post-weight loss, or after fat removal.
The clinical indications in body contouring for skin tightening has expanded significantly. Besides optimizing liposuction aesthetic outcomes augmenting skin retraction, an association with open excisional procedures has blossomed. Technologies to provide superior skin retraction has allowed patients with moderate skin laxity to avoid an excisional procedure (lipoabdominoplasty, brachioplasty, and thighplasty) altogether or reduce the length of incisions for these procedures. For instance, brachioplasty and thighplasty may avoid the longitudinal incision on the extremity and limit the incisions to the creases of the axilla or inguinal area, which avoids visible scars with little sacrifice of the cosmetic result. Weight loss using glucagon-like peptide-1 (GLP-1) agonist weekly injections has resulted in fat reduction and resultant skin laxity in both the face and body.
Suction-assisted liposuction (SAL) alone provides some retraction due to simple deflation of the skin envelope. In addition, mechanical stimulation resulting from liposuction blunt cannula trauma and suction induced non-thermal inflammation of the fibro-collagenous matrix, promotes neovascularization, neo-collagenesis, and scar tissue formation. 1 Skin surface area retraction or tightening with SAL measures about 10% at 6 to 8 weeks and finalizes at 8% at 1 year. 1 Superficial fat is often under resected due to the fear with post-aspiration skin laxity or, more commonly, over resection of fat may result in contour irregularities.
Since the degree of skin tightening and soft tissue retraction with SAL alone is often insufficient, adjuvant modalities during the liposuction have been added to enhance the amount of skin retraction. Superficial liposuction (SupL), laser-assisted liposuction (LAL), UAL, and radiofrequency-assisted liposuction (RFAL) have been studied.
Aggressive manual liposuction of the superficial areolar subcutaneous layer can result in more skin retraction than standard liposuction techniques that spares this layer. Although this SupL method may increase skin retraction, it significantly increases the risk of contour irregularities and even more ominous, vascular compromise.2-4 The authors have seen this technique used with full thickness skin loss in several patients by other practitioners. Selected lines of SupL in high-definition liposuction (ie, vertical linea alba and linea semilunaris, and horizontal rectus muscle insertions) is safe, while creating a superior slender, muscle sculpted aesthetic outcome.
Alternatively, energy-based systems create a thermal effect by some form of electromagnetic energy. Thermal induced contraction of collagen occurs when heated to a specific temperature and duration, causing protein denaturation and coagulation. Heat-induced denaturation of structural proteins, mainly collagen, is a time-dependent irreversible transformation of the native helical structure to a random, coiled result. 5 Chen et al examined this heat-induced shrinkage and denaturation of collagenous tissue (bovine chordae tendineae) absent of any mechanical load regarding the temperature level, duration of heating, and speed of heating. The hotter the temperature, the shorter the amount of treatment time needed for maximum collagen contraction. Chen et al 5 have shown that a temperature of 85°C required only 0.044-second duration for collagen denaturing. The thermal tissue injury creates a reduction of tissue volume by contraction or shrinkage of the fibroseptal network (FSN) with resultant retraction of the skin surface area.
Laser-assisted liposuction using a 3-laser wavelength device (1064, 1320, and 1440 nm) referred to as “Smart Lipo” (Cynosure, Westford, MA), has revealed 13 to 17% skin surface area reduction at 3 to 6 months. This retraction compares to under 10% skin contraction with suction-assisted alone in a randomized, blinded study using ultraviolet tattooing. 6 Due to the prolonged treatment time (25-45 minutes per area) after liposuction to perform the laser-induced tightening, the potential complication of skin burns and irregularities, and the better amount of skin retraction using RFAL and UAL, this technology has seen a dramatic drop in clinical use.
Bipolar radiofrequency (RF) with indwelling liposuction capability, known as BodyTite (InMode Ltd, Yokne’am Illit, Israel), was introduced in 2008. Unipolar RF ThermiTight (Thermi, Austin, Texas) was developed in 2012. Both products were approved by the Food and Drug Administration (FDA) for RF energy delivery in body contouring. The bipolar RFAL device results in a target temperature of 40°C for 1 to 2 minutes using 100 J/cm2. Duncan1,7 in a randomized, blinded study treating the arms, revealed that RFAL caused a 36% soft tissue contraction compared with 8.1% with SAL alone at 12 months. Hurwitz and Smith 8 studied 17 women (mean body mass index [BMI] 29.5) with an average aspirated volume of 1759 ml in the arms, abdomen, or thighs treated with BodyTite RFAL. The maximum vertical contraction was 15.7% for the abdomen, 7.4% for the thighs, and 3.3% for the arms with mean follow-up of 13.3 months. 8 These RF technologies targeted the skin directly via bulk heating for retraction.
One study (n = 10) using fluorescent tattoo marking to objectively assess skin tightening treated one arm with aggressive SupL followed by standard SAL, while the other arm was treated with RFAL plus standard SAL. 9 Chia et al revealed measured surface area reductions on the anterior arms averaged 15.0% for RFAL compared with 10.9% for SupL at 1 year. Posteriorly, RFAL showed a 13.1% reduction compared with SupL 8.1% reduction. Linear reduction for RFAL averaged 22.6%, while 17.8% for SupL postoperatively at 1 year, despite the reduced FSN and relative paucity of fat of the anterior arm. 9 This revealed that RFAL resulted in superior skin tightening over SupL.
The first addition of energy-based systems to liposuction began in 1992 with the first-generation ultrasound energy delivery device in an attempt to improve the aesthetic results. 10 A third-generation ultrasound device perfected UAL by delivering appropriate ultrasound frequency (36 000 Hz) into the tumescent solution prior to suctioning to separate the fat by a process known as “cavitation.” Cavitation results from the compression and rarefaction of the ultrasound energy wave, which allows dissolved air bubbles of 5 to 10 µ to migrate between adipocyte cells. The bubbles would coalesce when reaching the resonant size of 180 µ, the bubble then collapses or ruptures, thereby separating adipocytes from there matrix. 11 Minor cellular trauma occurred without affecting blood vessels, nerves, or the FSN. After all the ultrasound energy was delivered, then liposuction was completed.12-14
Vibration amplification of sound energy at resonance (VASER) (Bausch Health Companies, Inc., Laval, QC, Canada) became the preferred ultrasound delivery method due to its enhanced aesthetic result and reduced complication rate. Except for changing to digital from analog, the technology has not changed since its market entrance in 1999. Ultrasound-assisted liposuction in the form of the VASER device is used in high-definition body sculpting, because of the clinical data proving maximum skin tightening, sparing of neurovascular perforators, and minimizing blood loss.12,13
Nagy and Vanek 14 compared liposuction alone on one side of the body with the addition of internal ultrasound to the opposite side regarding skin retraction (n = 20). Skin retraction was analyzed by measuring length changes of a 50-mm triangle ultraviolet light tattoo. The addition of ultrasound revealed a statistically significant improvement in skin retraction of 53% relative to the SAL side. A nonthermal ultrasound wave stimulates tissue myofibroblasts, which results in 3-dimensional tissue tightening. Dr Vanek believes that there is a final quantitative skin retraction of more than 20% optimized at 6 months (personal communication with Dr Vanek in March 2025). Vibration amplification of sound energy at resonance has been an intricate component in achieving high-definition body contouring aesthetic outcomes due to a large part from this heightened skin tightening.12-14
Another novel thermal device was introduced in 2012 delivering internal monopolar RF helium-based plasma technology (HPT) for cutting, coagulation, and ablation of soft tissues. It was introduced in liposuction patients by Dr Jack Zamora in 2016 (personal communication in 2018). One author (RJT) began using and teaching HPT at continuing medical education courses for body contouring in 2018 along with VASER high-definition liposuction to augment skin retraction.
The systems generator delivers RF energy to the 15 cm (cervical and face) or 27 cm (body areas) handpiece electrode. When helium gas is passed over the energized electrode, a helium plasma is generated. Helium is ionized at very low energy levels produced by the low-current generator. The plasma allows heat to be applied to tissue in 2 distinct ways. 15 First, heat is generated by the actual production of the plasma beam itself through the ionization and rapid neutralization of the helium atoms. Second, since plasmas are excellent electrical conductors, a portion of the RF energy passes from the electrode to the patient through the plasma. 15
Renuvion energy instantly heats the tissue by passing current through the resistance of the tissue, a process known as “joule heating.”15,16 This is compared with the “bulk heating” of Thermi and BodyTite that requires exposure of the targeted tissue for more than 120 seconds at 65°C in order for maximum contraction to occur, which increases the risk of surface skin thermal injury (Figure 1). 17
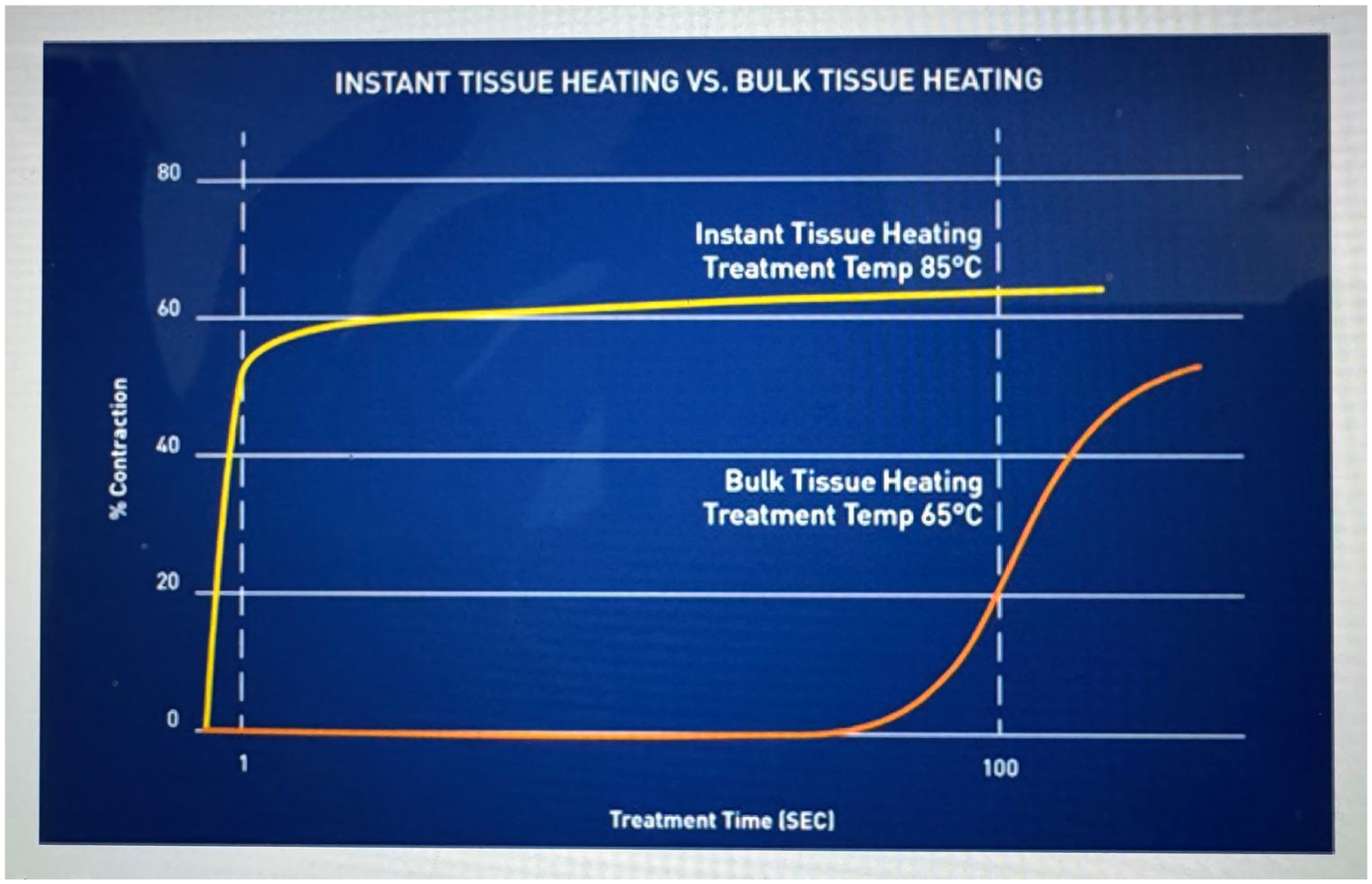
Instant tissue (joule heating) vs bulk tissue heating.
Duncan and Roman performed HPT on the abdomen of a live pig after wetting solution delivery and liposuction. Simultaneous internal and external temperatures were measured using a forward-looking infrared camera at various power and helium gas flow settings. Helium flow rates above 1 L/min were required. Maximum internal tissue temperature using 60% and 80% power exceeded 85°C for about 0.08 seconds at probe speeds of 1 cm/s undergoing 6 passes (Figure 2). 17 This temperature is needed to produce soft tissue coagulation and protein contraction more rapidly. Fortunately, external skin temperatures remained in a safe range with less than a 2°C increase with HPT. 17
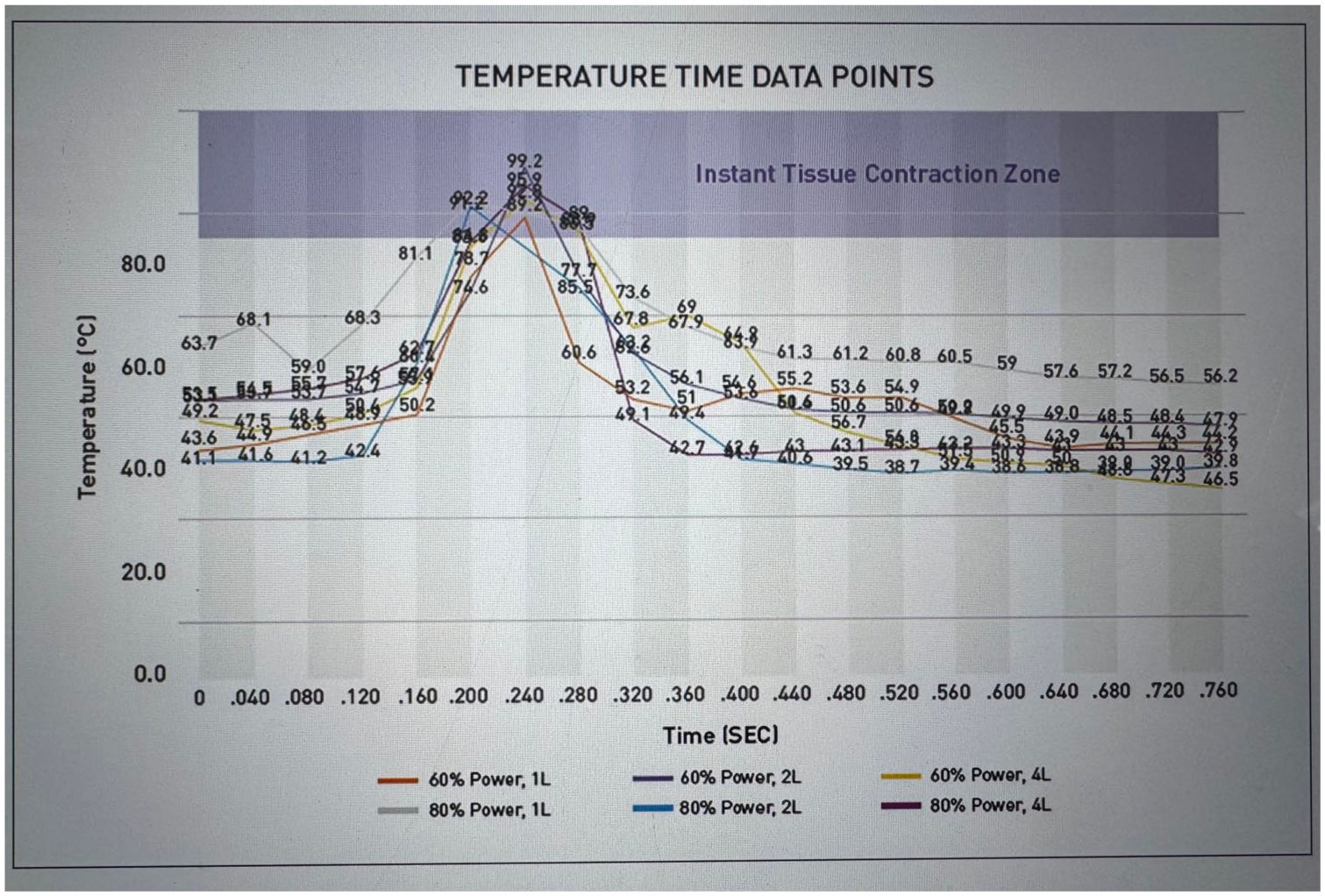
Renuvion energy delivery: temperature versus time.
Ruff et al 18 completed a safety study using HPT alone without liposuction to the neck using 4 to 6 passes at 70% power, 1.5 L/min helium flow, probe speed of 1 to 3 cm/s with strikes separated by 2 to 3 cm after 150 to 250 ml of wetting solution was administered. Improvement in skin laxity was observed in 82.5% of those treated with no serious adverse effects and adverse effects were within the range for minimally invasive subdermal treatments. 18 The outcome from this study resulted in HPT being approved by the FDA for improvement of lax skin in the neck and submental region (July 2022).
A multicenter retrospective chart review (n = 192) examined adverse events of soft tissue coagulation using HPT alone and in combination with UAL. 19 The lower face, neck, upper body, lower body, and upper and lower extremities were treated with a mean follow-up of 3 months. There were no serious adverse events and 24% of patients experienced minor adverse events, which were mainly caused by ancillary surgical procedures such as blepharoplasty and breast implant surgery. They did observe delayed healing, epidermal lysis, skin blister, fibrosis, fullness, nodule, contour irregularities, and wound dehiscence. Expected side effects included swelling, erythema, and drainage. Seroma was the most frequency adverse event, occurring in 6.8% of patients, but observed only in those treated with combination UAL and HPT. 19 Due to a large part of the results of this study, HPT was subsequently FDA approved to be used following liposuction for aesthetic body contouring (April 2023).
Methods
Study Design
A retrospective study was performed on consecutive body contouring patients electing combined VASER liposuction followed by HPT from April 2018 to December 2022. In addition, patients (n = 20) from 2023 to 2024 had the Renuvion device joule counter measure the amount of energy delivered during 360° liposuction. The investigation was carried out following the rules of the Declaration of Helsinki of 1975, revised in 2013. This study was approved through the investigational review board of Touro University Nevada (TUNIRB000228).
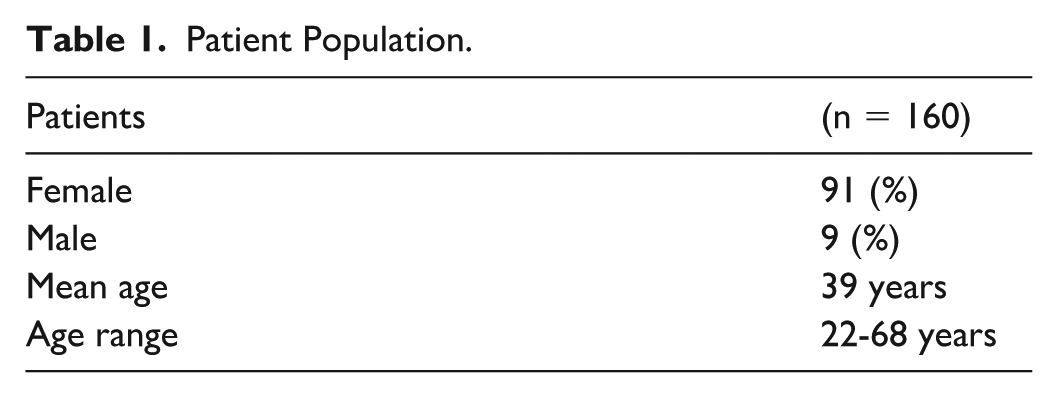
Participants
Adult healthy patients (22-68 years of age) presented requesting body contouring to 2 surgeon’s private practices (Table 1). They consented to VASER liposuction with HPT. Benefits of improved body contour (reduction of excess fat and skin tightening), limitations of persistent excess skin, possible side effects, and complications were described in the consent process. Any observed complication would be treated with the current standard of care. Patients identified with a seroma were treated by needle aspiration as needed.
Patient Population.
Clinical Indications
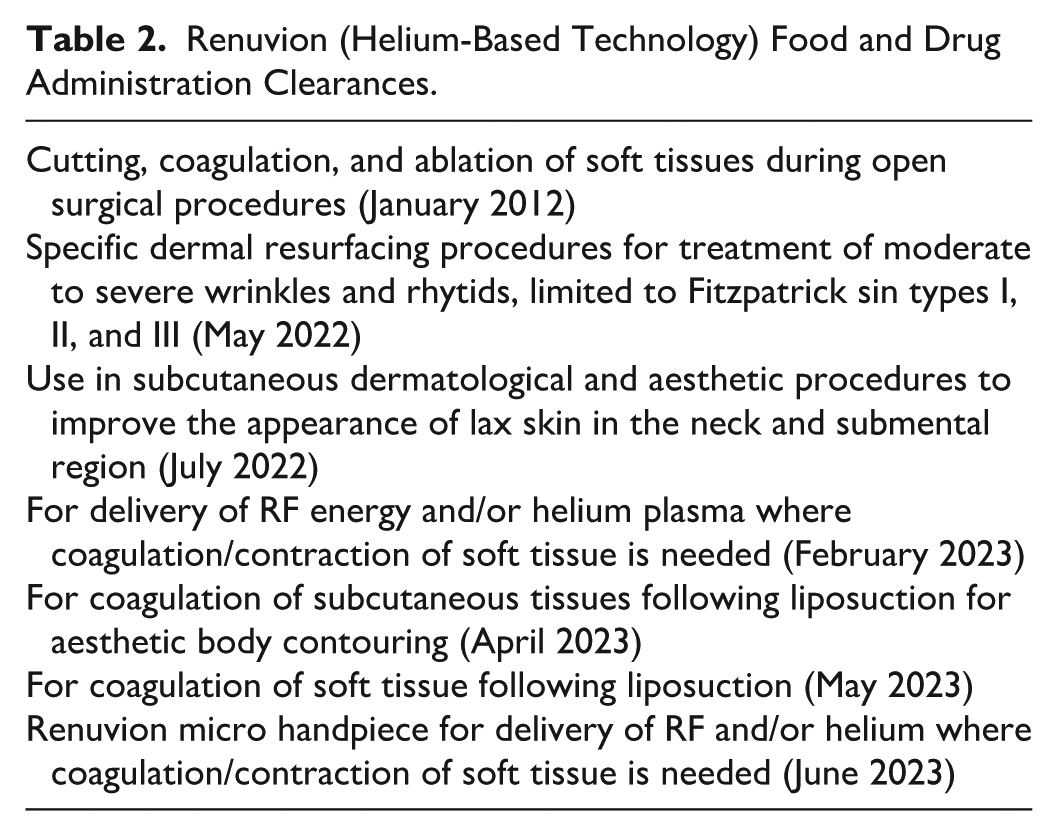
Helium-based plasma technology has received numerous clinical clearances from the FDA (Table 2) including following liposuction for aesthetic body contouring. The device previously sold as J-Plasma in the hospital surgical market. It is now sold as Renuvion in both hospital surgical and cosmetic surgery markets (Apxy Medical Corporation, Clearwater, Florida).
Renuvion (Helium-Based Technology) Food and Drug Administration Clearances.
Patients were instructed that VASER liposuction combined with HPT is an invasive procedure that will provide fat debulking and skin retraction.
Preparation
All patients underwent a comprehensive history and physical, complete blood count, and stopped any aspirin or fish oil 2 weeks prior to the procedure. Other testing was ordered as clinically warranted. Photography documentation was performed before and serially postoperatively.
Marking
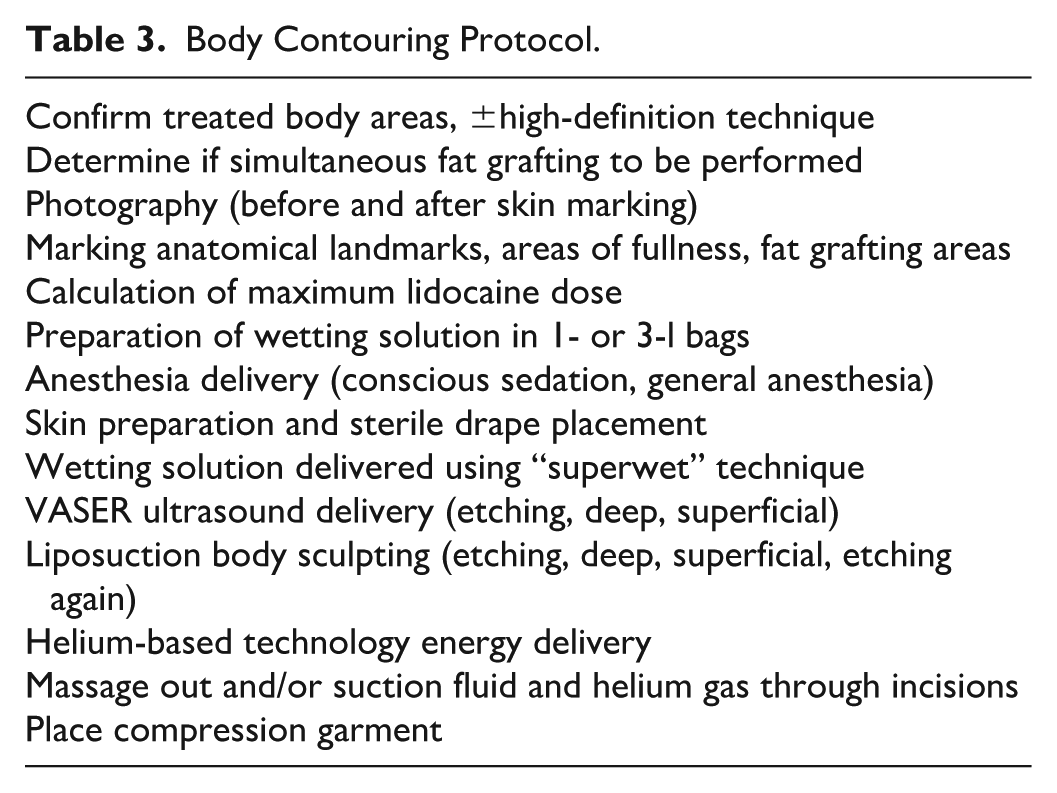
Patients followed a standardized surgical liposuction protocol (Table 3). Body markings for standard (mainly SH) and high-definition (mainly RJT) liposuction were carried out. The linea alba and bilateral linea semilunaris as well as the anterior inferior rib cage were denoted with a Sharpe. The point of maximum indentation of the flanks was noted laterally. Incisions in the mons pubis area along the linea semilunaris and at the 12 o’clock position of the umbilicus and the superior aspect of the intergluteal crease for 360° liposuction were noted with a different color. Areas of fat removal were noted in a topographical map technique. If fat grafting was to be performed, the areas for fat placement were noted with a different color Sharpe in a topographical map method.
Body Contouring Protocol.
Anesthesia
Patients either had intravenous conscious sedation (RJT) or general anesthesia (SJ, minority with RJT) for the body contouring procedure. With conscious sedation patients took oral lorazepam (2 mg), and hydrocodone (10 mg) at least 30 minutes prior to commencing surgery. Patients also were given cephalexin 1000 mg (RJT) or amoxicillin/clavulanate (Augmentin) 875 mg (SH) (clindamycin 600 mg with penicillin allergy), and ondansetron (4-8 mg). General anesthesia was performed by a nurse anesthetist or anesthesiologist with endotracheal intubation.
The skin of the body was prepped with chlorhexidine. Local anesthesia of lidocaine with epinephrine was injected into the proposed incisions. The maximum dose of lidocaine at 50 mg/kg was not exceeded. A wetting solution of diluted lidocaine, epinephrine, and bicarbonate (Klein solution) was prepared. Using blunt infiltration cannulas, the wetting solution was delivered to the surgical sites using “superwet technique.” Under conscious sedation, between 800 and 1000 mg of lidocaine per liter were prepared, while 200 to 250 mg per liter under general anesthesia.
Postoperative anesthesia included either acetaminophen 325 mg every 3 hours or hydrocodone 5 mg with acetaminophen 325 mg (RJT) or oxycodone (Percocet) 5 to 10 mg (SH). Patients requesting high-definition body sculpting were given the option of adding gabapentin (Neurontin) 300 mg three times a day and celecoxib (Celebrex) 200 mg twice a day for 10 days. The goal of these medications was to minimize the need for narcotic analgesia.
Liposuction Procedure and Ultrasound Energy Delivery
Skin guards protected the skin as the VASER generator delivered ultrasound energy. Ultrasound energy was delivered using 80% continuous mode to the torso and 60% to 80% pulsed mode to the extremities by one surgeon (RJT) and 70% to 80% continuous mode to all areas by the other (SJ). If fat grafting was planned, one surgeon (RJT) decreased the energy to 60% pulsed mode with the minimum duration of ultrasound delivery to produce a desired body contouring result. The body received energy to both the superficial and deep fat layers and in the abdomen etching the linea alba and semilunaris. The 5-groove ultrasound probe (3.7 mm diameter) was passed until little tissue resistance subjectively persisted.
Liposuction was performed mainly using 3.0, 3.7, and 4.7 mm vented liposuction cannulas (Bausch Health Companies, Inc., Laval, QC, Canada), cautious to avoid excess use of larger cannulas in the immediate subcutaneous layer to prevent creating contour irregularities. The smaller 3.0 mm cannula was used for high-definition etching and more superficial fine-tune sculpting.
HPT Energy Delivery
Once the liposuction was completed, the significant reduction of adipocyte density in the treatment space uncovered the architecture of the FSN (Figure 3). This network is the target of the HPT, which is addressed by the RF 27 cm length handpiece energy delivery. One practitioner (RJT) always used 80% power setting with 1.5 L/min. The other surgeon (SJ) used 60% to 80% power setting with helium flow rates between 1.5 and 2.5 L/min based on the patient’s fat thickness.

Endoscopic view of the subcutaneous space after VASER ultrasound liposuction illustrating the fibroseptal network (FSN) and minimal residual adipocytes. This FSN is the target of the Helium-Based technology created plasma. The collagen of the FSN shrinks by 65% after an exposure of only 0.44 to 0.08 seconds at 85°C. The initial tissue contraction from skin envelope shrinkage, swelling resolution, and scar tissue formation combines with delayed skin retraction with maximum FSN contraction at 6 to 9 months post-treatment.
Another important variable affecting energy delivery is the speed of movement of the handpiece. Both surgeons were observant to move the handpiece no more than 3 cm/s. It is easy to move the handpiece too rapidly (>3 cm/s), which lowers the energy delivery below recommended levels. One surgeon (RJT) performed 6 passes per treated area, while the other (SJ) performed 6 to 8 passes. A pass was defined as either an antegrade or retrograde movement of the probe throughout a horizontal plane of treatment, thus a simultaneous antegrade and retrograde movement in the same treated linear area was considered 2 passes.
Since the ultrasound solid probe and liposuction cannulas pre-tunnel the subcutaneous space, it made it easier for the RF handpiece to be advanced through the tissue. If there is inadequate tunneling, there may be helium gas occlusion by 20% from obstruction of the tip of the handpiece, creating an automatic shutoff of gas flow (F13 default). Upon completion of RF energy delivery, external hand pressure was placed on the treated area to evacuate any helium gas to prevent subcutaneous emphysema migration and fluid retention.
HPT Handpiece Design Changes
The initial handpiece had the energy delivered at the open tip at the end of the 5 mm diameter electrode. This is the reason initial teaching was to only use retrograde linear activation to prevent burns by advancing the electrode against skin caught by fibrous tissue immediately in front of the electrode. The new smaller 3 mm diameter handpieces have a rounded tip with the opening allowing side emitting energy and helium flow. This design allows for activation with both an antegrade and retrograde linear movement of the handpiece. The newest handpiece design (2024) with side delivering energy decreases the shutoff frequency if one keeps the flow during both the antegrade and retrograde movement of the handpiece because there is less opportunity for the lumen to be obstructed by helium gas flow. The most recent tip design has a computer regulation of helium gas flow that prevents any shut offs.
Determination of Radiofrequency Energy Delivery
There are 2 methods to determine the amount of energy delivered: (1) total energy delivered to a target area (joule energy counter on device) or (2) number of strokes or passes per target area (following manufacturers’ guidelines). Subsequently, in a subgroup of patients (n = 20), one surgeon (RJT) correlated the measured energy delivery from the device counter to the recommended guideline technique regarding probe movement, power settings, and helium flow rate.
Understanding energy delivery begins with a review of basic energy metrics. Watt is the Système International (SI) of units of power, whereas Joule is the SI for units of energy. One watt of energy equals 1 joule of energy per 1-second duration. Alternatively, 1 watt-second (watts multiplied by seconds) equals 1 joule.
Power = energy/time Watts = joules/s joules = watts multiplied by seconds
1000 joules (1 kJ) = 1 watt for 1000 seconds or 40 watts for 25 seconds
Helium-based plasma technology RF generator power setting range from 0% to 100%, where 40 watts is 100% energy. At 40 watts or 100% power setting it would take 25 seconds to deliver 1000 joules (1kJ) of energy (1000 J/25 seconds = 40 J/s or 40 watts). At 80% power setting, moving the electrode 1 cm/s creates 32 joules of energy to that one centimeter of tissue, while 60% power setting at the same linear speed (1 cm/s) creates 24 joules of energy.
The surface area for a treated anatomical site is measured with the X (height) and Y (length) axes (in centimeters). However, the Z-axis (depth) is a difficult value to measure, thus is estimated. Previous laboratory bench tissue studies determined that the plasma created by HPT extends through a path of least resistance from the probe tip (currently 3 mm in diameter) a distance between 5 and 10 mm. 17 Given these data, each pass related to the 3-dimentional elliptical footprint of energy emission should be separated by 1.3 to 2.3 cm at the distal aspect of the triangular shaped treatment area starting from an incision.
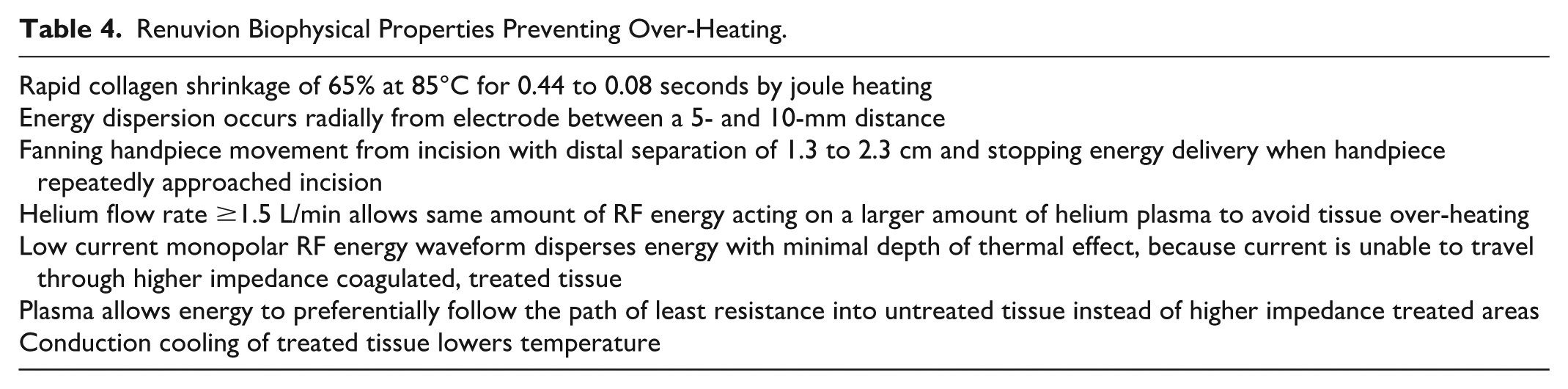
The amount of RF energy delivered to the treated tissue is directly related to the power setting (in percent), speed of moving the handpiece, number of passes (maximum 6-8), and ensuring all the 3-dimentional tissue volume is treated. There are a number of biophysical properties that reduce the risk of over-treating tissue (Table 4). To avoid over-treatment closer to the incision, the handpiece is turned off when adequate energy delivery is estimated by the surgeon being delivered in concentric circles (Figure 4).
Renuvion Biophysical Properties Preventing Over-Heating.
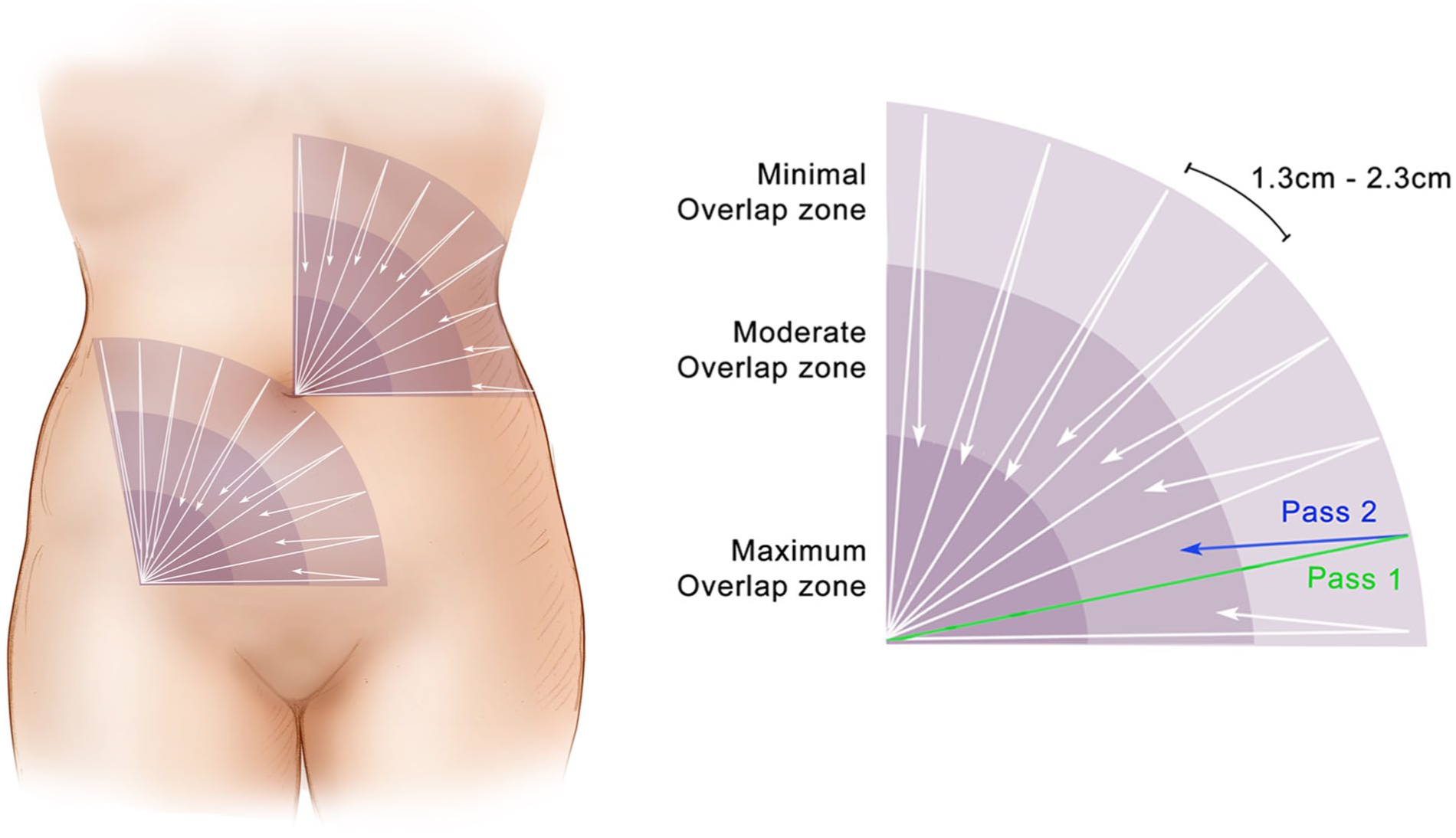
Renuvion treatment method: fanning from incision.
Since the complication rate from HPT is negligible due to the properties of both RF and plasma, if there is some overlap of a previous pass, there is little increased risk of excess temperature creation. The initial plane of treatment is deep, 0.5 to 1.0 cm above muscle fascia. Treatment proceeds superficially, estimating depths of plane of delivery of HPT energy treatment of 1.3 to 2.3 cm between planes, and keeping about 1.0 cm from the skin surface (Figure 5). This means that there is 1.3 to 2.3 cm between each stroke of the probe or 3D plane of treatment. This technique of movement of the probe ensures all tissue 3-dimentionally receives adequate energy delivery, while protecting the skin from excess thermal temperatures.
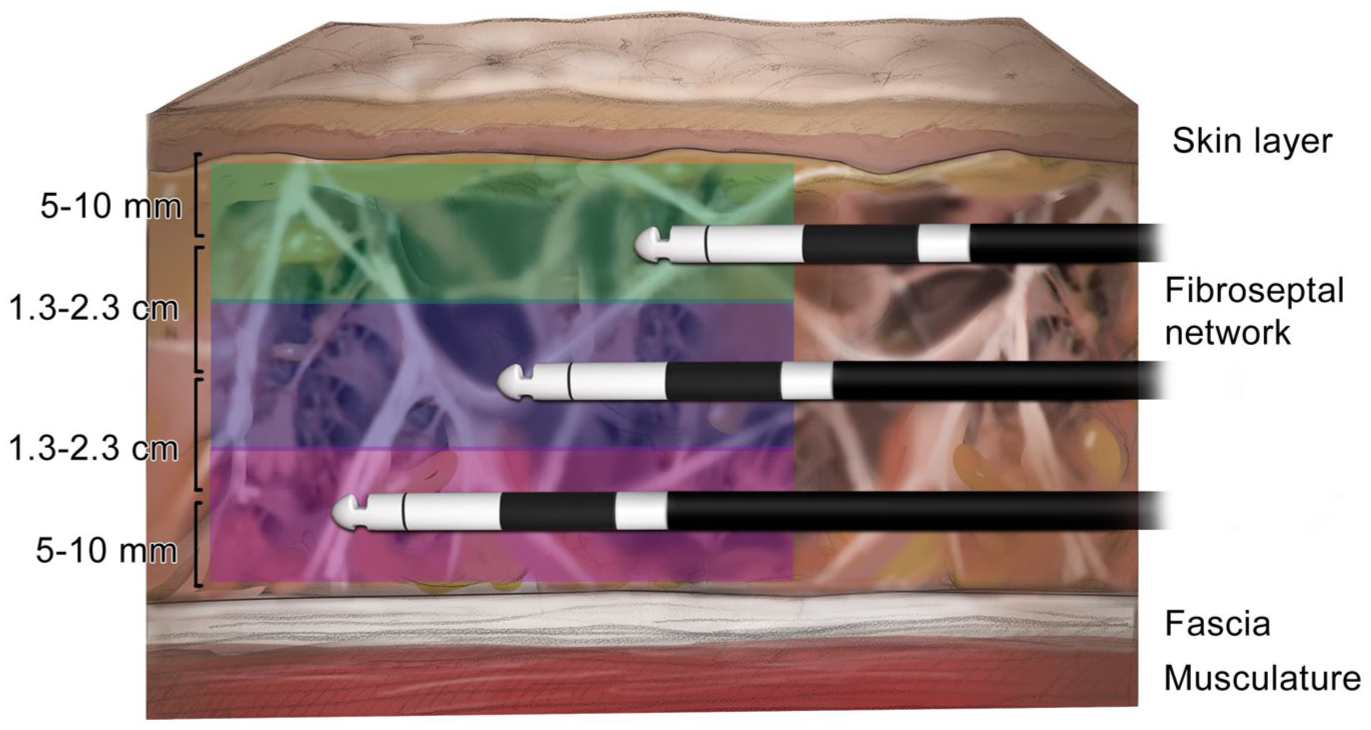
Renuvion treatment method: handpiece depth.
Dressing
A standard compression garment was used continuously by one surgeon (RJT) for 1 month followed by 1 week at night, while the other (SJ) uses the garment for 6 to 8 weeks continuously. Both recommend beginning manual massage 4 times a day beginning 5 to 7 days after surgery for 2 months postoperatively. In addition, patients were encouraged to undergo lymphatic massage once or twice a week for 2 to 4 weeks postoperatively.
Follow-Up
Patients were instructed to follow-up at 1 day, 1 and 2 weeks, 1, 2, 3, and 6 months, and every year thereafter. The Global Aesthetic Improvement Scale (GAIS) assessment. This 5-point scale (0 to 5) is from worse, no change, improved, much improved, and very much improved (last 2 tabulated together). Patients were weighed regularly postoperatively and counseled on weight loss if experienced a weight gain with dietary changes, exercise, and bioidentical hormone testing and supplementation. Patients were recommended not to return to exercise for at least 3 to 4 weeks after surgery.
Results
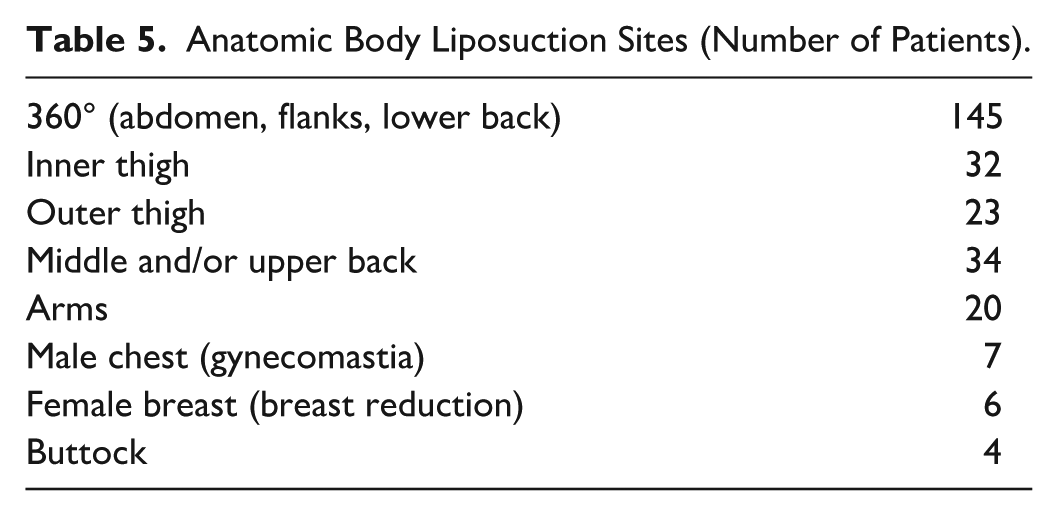
There were 561 anatomic liposuction areas in 160 patients with an average of 3.5 sites per patient (Table 5). The majority of patients (90.6%) had 360° (abdomen, flanks, and lower back) liposuction. The overall patient satisfaction rate was 95% (152 of 160 patients) using the GAIS definition of either very much improved or much improved (Figures 6 and 7). Eight patients noted improvement or improved only. The reasons for only improvement were recurrent seroma formation (1 patient), liposuction indentation requiring fat grafting to restore (2 patients), and those requesting additional liposuction (5 patients). No patients admitted no change or a worse result.
Anatomic Body Liposuction Sites (Number of Patients).
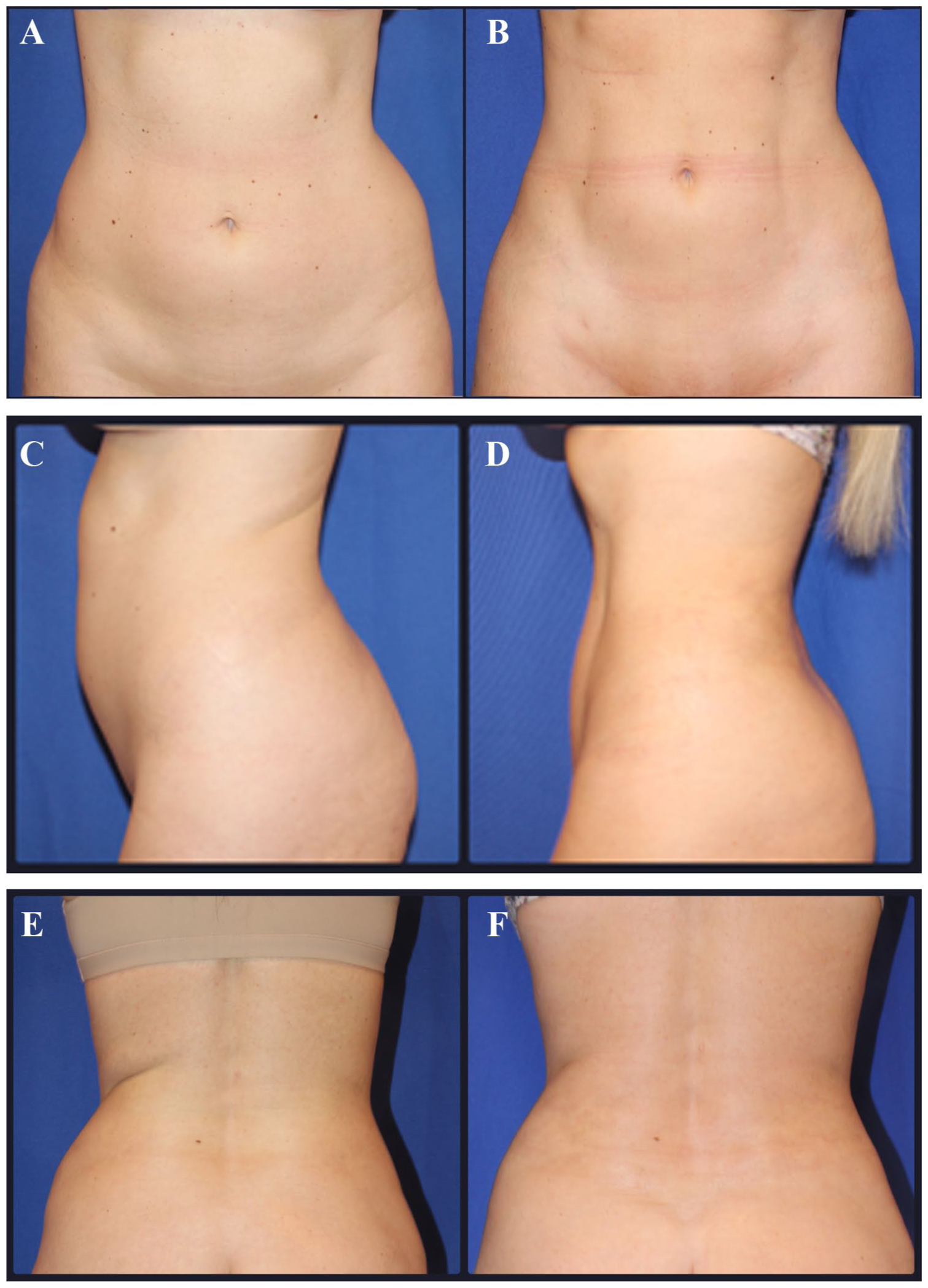
Forty-one-year-old gravida 0, female (5′9″, 155 pounds, 1200 cc supernatant fat removal) who underwent ultrasound-assisted liposuction with helium-based plasma technology on abdomen, flanks, and lower back. Before and 12 months after (A, B) front view, (C, D) left lateral view, (E, F) posterior view. Adverse effects were not observed.
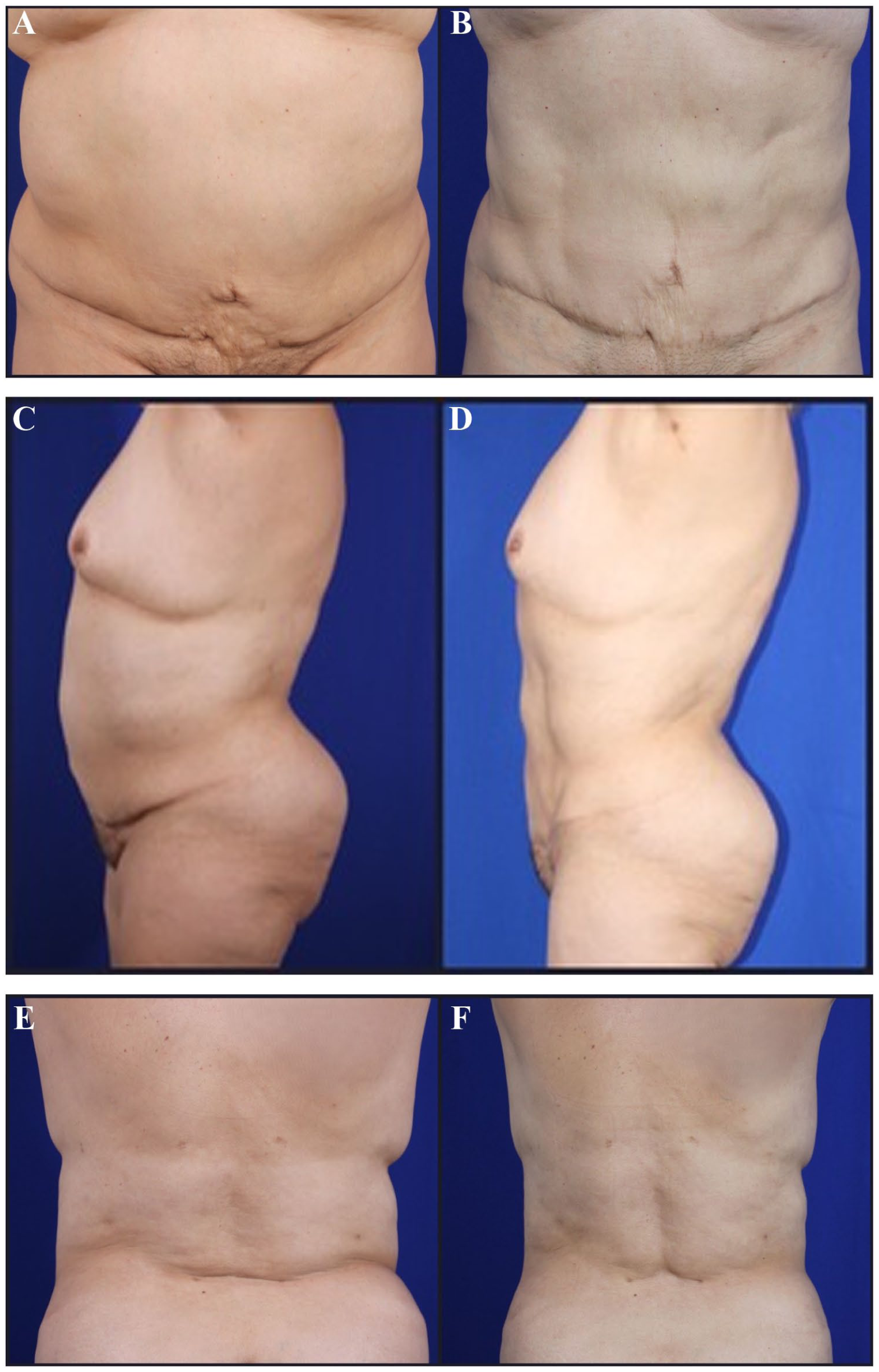
Sixty-eight-year-old gravida 3 female (5′3″, 185 pounds, abdominoplasty in past, 2950 cc supernatant fat removal) who underwent ultrasound-assisted liposuction with helium-based plasma technology on abdomen, flanks, lower back, and upper back. Before and 8 months after (A, B) front view, (C, D) left lateral view, (E, F) posterior view. Adverse effects were not observed.
No patient experienced a serious adverse effect (Table 6). The most common complication (14/160 or 8.8%) was a seroma formation that was observed between 1 and 3 weeks postoperatively. All seromas resolved with one or more needle aspirations and continued compression garment use.
Complications (n = 27).
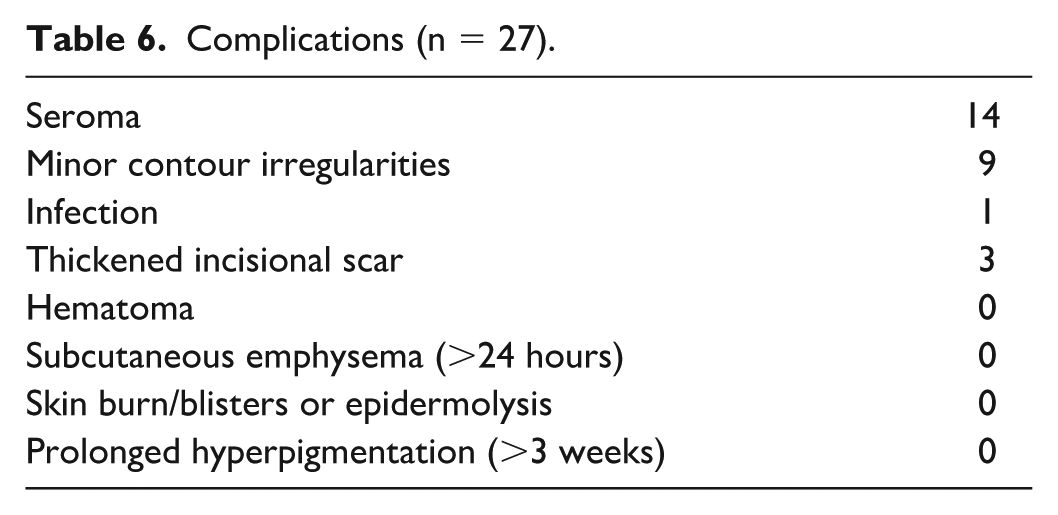
Nine (5.6%) patients experienced minor contour irregularities. Five resolved with the patient performing manual massage several times each day for 1 to 3 months. Two resolved with external ultrasound (VASERShape) treatments (2 and 3 sessions). Two patients with persistent minor depressions of the inner thigh required fat grafting (20 and 30 cc) to resolve the indentation. Five patients (3 of the 5 were obese or morbidly obese) requested additional liposuction to remove additional excess fat from areas of previous liposuction. All areas of revision removed less than 10% of the volume removed during the initial liposuction procedure. The overall surgical revision rate was 4.4% (7/160).
Three patients requested additional external skin tightening postoperatively and were given the option of either RF (Venus Legacy) or ultrasound (VASERShape). All were satisfied with the further skin contraction, although surgeon physical examination noted minor excess skin remained.
No patients experienced anesthetic complications, other than nausea. Expected clinical side effects included mild to moderate discomfort, edema, ecchymosis, and itching. No patients required narcotics past 7 days postoperatively.
Subjective surgeon assessment of skin retraction by both surgeons compared with their experience with ultrasound alone revealed better skin tightening with the addition of HPT. Some visible improvement is noted at the 24-hour postoperative visit and continued to improve over the first 6 months.
The measured energy delivery using the machines joule counter (n = 20) for abdomen, flanks, and lower back following the manufacturer’s guidelines of treatment (80%, 1.5 L/min, 3 cm/s, 6 passes) revealed optimal 3-dimentional energy delivery for 360° liposuction anatomic areas (Table 7).
Renuvion Energy Delivery by Anatomic Area (n = 20).
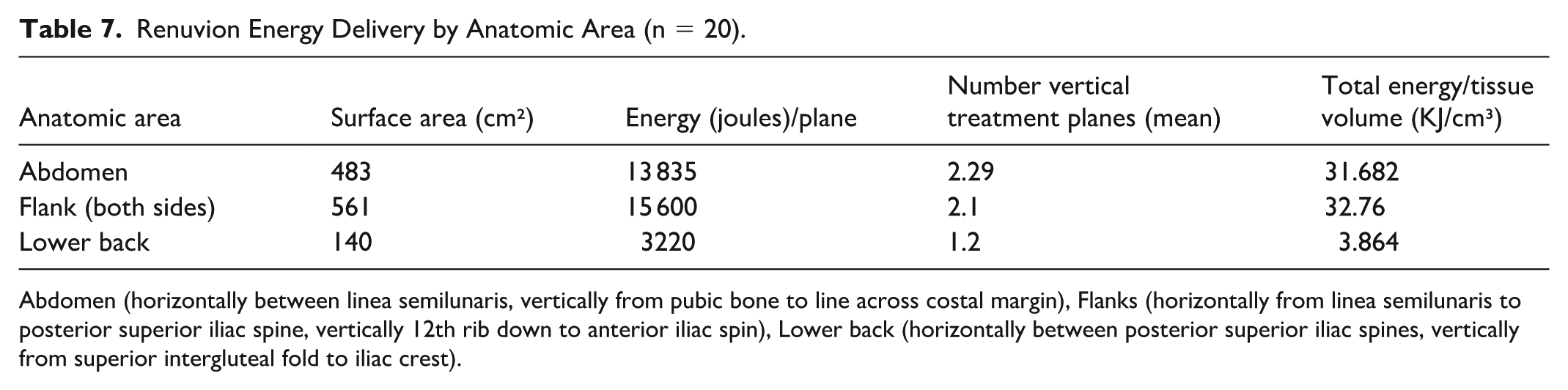
Abdomen (horizontally between linea semilunaris, vertically from pubic bone to line across costal margin), Flanks (horizontally from linea semilunaris to posterior superior iliac spine, vertically 12th rib down to anterior iliac spin), Lower back (horizontally between posterior superior iliac spines, vertically from superior intergluteal fold to iliac crest).
Discussion
The results reveal that combination of UAL with HPT can be safely performed without any serious adverse effects or skin burns in body contouring. The data are in alignment with Ruff et al, 19 who also did not observe any serious adverse effects. Most of the complications were seroma formation (8.8%) and minor contour irregularities (5.6%) with an acceptable revision surgical rate of 4.4%.
Techniques to lower the incidence of seroma formation include: (1) use of pulsed instead of continuous ultrasound energy delivery, (2) reduced amount of ultrasound energy delivered for a shorter period of time (however, the less energy levels can result in less skin tightening or fat separation), (3) placement of passive or active drains when high-definition sculpting is performed for several day duration (rarely used in our patient population), (4) leaving liposuction incisions open to drain postoperatively, (5) diligent compression garment, foam, and abdominal binder use, and (6) lymphatic draining postoperatively using patient manual massage, medical professional lymphatic massage techniques, and VASERShape external therapeutic ultrasound.
A challenge of percutaneous energy delivery regarding thermal-induced tissue contraction is the balance between maintaining safe external skin temperatures, while achieving target temperatures of the internal tissues. Two RF body contouring devices (Thermi and BodyTite) use a mechanism of action of “bulk heating.”1,8,20 This method takes significantly more time, and the skin heat conduction increases the risk of full thickness skin injury.8,20
The helium plasma device focuses energy on the target tissue of the FSN, resulting in immediate soft tissue contraction without heating the dermal full thickness.5,16 The external temperature does not increase more than 2°C from baseline over the course of the typical clinical treatment of 6 passes, which keeps the skin safe from burns and vascular compromise.
The peak energy created by the helium-based plasma may extend up to 4 cm in front of the handpieces electrode with a 1.3- to 2.3-cm diameter cone of energy with dispersion axially from the tip of 5 to 10 mm. 16 The electrode can be placed safely 5 to 10 mm below the superficial skin and 1.3 to 2.3 cm distance apart from each plane of treatment to affect all depths of the treatment area.
The low current monopolar RF energy waveform disperses the energy with minimal depth of thermal effect and prevents over-treating with multiple passes, because the current is unable to travel through the higher impedance of coagulated, treated tissue. This allows the energy to preferentially follow the path of least resistance or impedance of the untreated tissue. The adjacent surrounding tissue at lower temperatures from the treated area allows for rapid cooling through conductive heat transfer. 21
The FSN contracts immediately, but it will take weeks to months for the overlying epidermis and dermis to settle over the contraction foundation below. The initial skin will have some excess and this redundancy takes time to tighten. If one desires more rapid or additional skin transformation, one can perform external carbon dioxide or erbium-YAG laser, microneedling RF skin resurfacing, therapeutic ultrasound (ex. VASERShape), or RF (eg. Venus Legacy) treatments.
The suspected optimal treatment of a 10 × 15 cm surface treatment area is for a 5-minute duration using 70% power setting yielding 5 kJ of energy delivery to the tissue.16,17
However, this estimation does not include the depth component of the tissue volume. Immediate contraction of the FSN occurs without heating the full thickness of the dermis. In HPT, the tissue surrounding the treatment area remains much cooler allowing for rapid cooling of the treated area through conductive heat transfer. 17 The skin follows the substructure of FSN that supports the skin. Since the FSN is the treatment target, there is no focus on heating the overlying skin. The FSN contraction will ultimately result in skin retraction and tightening. Triple helical collagen fibers when denatured shrink from 290 to 10.5 nm, a contraction of over 65%.5,17
Understanding HPT energy delivery is paramount to optimizing the efficacy of skin contraction and minimizing complications. If one moves the handpiece too rapidly (>3 cm/s) the rate of tissue treated at 80% power setting drops by 30%, resulting in less FSN collagen contraction. 17 One concern was that moving the handpiece too slow (<1 cm/s) would result in skin burns. However, the handpiece can be static for 20 seconds before resulting in a skin burn (personal communication with first Apyx Medical sales representative, Christian Winkle October 2024).
By measuring the surface area and estimating the depth of tissue to be treated (cm2), one can either directly measure with the energy counter on the device or calculate the total energy delivered accurately. The tissue depth component is the variable which is most difficult to determine and the variable least discussed when calculating sufficient energy delivery to achieve the desired skin retraction.
Set of experienced users have clinically estimated that the optimal total amount of energy to deliver to body areas, such as the abdomen is about 15 to 20 joules/cm2 (Apyx Medical compiled data, personal communication with first sales representative, Christian Winkle October 2024). Since there are minor tissue variables and energy influences affecting the precise energy delivered, Apyx Medical has accurately tested the exact energy amount depending on power settings. At 80% power setting, it takes 51.9 seconds to deliver 1000 joules (1 kJ) of energy corresponding to 19.25 joules/s of power delivered to the tissue. At 70% power setting it takes 60.3 seconds to deliver one kJ and at 60% power setting it takes 71.9 seconds to deliver 1 kJ of energy (Renuvion Tech Memo, March 2022).
Apyx Medical Corporation has improved Renuvion safety by implementing the following actions: (1) better handpiece/electrode design, (2) helium flow rate lowered to 1.5 L/min, (3) better training for new practitioners, and (4) the understanding that the patients innate perfusion of blood through the adjacent and deep tissues cools by alleviating heat, known as “conduction cooling.”
The flow rate of helium gas does not affect energy delivery as long as it is greater than 1 L/min; however, it may affect safety. In a live pig model, if the flow rate is <1.5 L/min, the same amount of RF energy affects a smaller amount of helium plasma and gets hotter. 17 This finding can result in increased risk of skin burns with this very low helium flow rate. Higher helium flow rates (> 1.5 L/min) do not change the speed or amount of skin tightening. High helium flow rates can lead to significant subcutaneous emphysema to even mediastinal air that can result in decreased cardiac output or airway compromise.
Skin tightening efficacy is related to the anatomical site, skin thickness, and quality of the overlying skin. The anatomical areas with the most significant observed skin tightening are the cervical area,18,21,22 abdomen, 19 and arms. 23 Increased skin thickness and, like most technologies, stretch marks result in less observed improvement of skin laxity or stria.
Ultrasound-assisted liposuction using VASER creates tightening by myofibroblast stimulation and the healing response in contrast to heat alone, 14 while HPT uses heat-based collagen fiber contraction.5,7,15,17 Our data show that 6 passes with the 60% to 80% RF power settings can be performed safely, while subjective clinical observation of achieving superior skin contraction.
The combined manual suction liposuction creating 8% to 10% skin retraction, 1 the ultrasound energy delivery with an estimated 20% skin tightening, 14 coupled with the HPT with an estimated up to 30% more,7,15,17-19 maximizes the skin retraction outcome.
Other variables affecting both overall cosmetic outcome and degree of skin retraction is the amount of ultrasound energy delivery (both power settings, probe diameter, number of solid probe rings, and duration of delivery), the amount of fat removal resulting in deflation of the skin envelope, and the amount of fat remaining after moderate or aggressive liposuction, which can inhibit further tissue retraction. Patients age, previous liposuction procedures, BMI, variables affecting healing (eg, smoking, nutrition, and diabetes), and elasticity of the skin and tissues will also certainly affect aesthetic outcome and degree of skin tightening.
Conclusions
Combination UAL with HPT for body contouring can be performed safely with no serious adverse effects and provide overall body contouring aesthetic results with superior skin retraction. Measuring the surface area and estimating the depth of tissue to be treated and following the manufacturers treatment parameters of 80% power setting, 1.5 L/min helium gas flow, moving the probe no faster than 3 cm/s, delivering 6 passes (3 antegrade and 3 retrograde movements) in a 2-dimensional plane, and keeping the planes of treatment from deep to superficial estimated between 1.3 and 2.3 cm apart will achieve the suspected optimal energy delivery: 15 to 20 joules/cm2 and about 30 kJ/cm3. This provides the optimal degree of skin retraction and tightening, while lowering the already low adverse effect incidence.
Footnotes
Acknowledgements
The authors acknowledge their office staffs for their assistance in surgery, in the manuscript photographic compilation, and patient data acquisition. They commend the librarians at Touro University Nevada for their assistance with the references.
Author Note
AI was not used in compiling this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received no financial support for the publication of this manuscript outside of support for the medical illustrations and open access fee from Apyx Medical.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.