
Abstract
Introduction:
Management of the aging brow has classically involved surgical therapy. Energy-based devices causing skin tightening, neuromodulators, or brow dermal filler volume placement can create brow lifting.
Materials & Methods:
Retrospective, consecutive patient review of Artefill (ART), now Bellafill, injection along superior brow hair to provide permanent brow lifting. The degree of brow suspension was evaluated regarding the medial, peek, and lateral brow calibrated measurements, injection site filler placement, complications, and patient satisfaction.
Results:
From 2015 through 2022, 113 patients underwent ART (Bellafill) brow lifting alone or simultaneously with upper cosmetic eyelid surgery (blepharoplasty). Using the global aesthetic improvement scale (GAIS) assessment reached 88.5% patient satisfaction with very much improved or improved responses. Brow measurements showed 80.0% having brow elevation by mean of 2.13 mm with 92% required one syringe (half of syringe per side) and injecting with a 25 G microcannula in 96%. The only side effect or complication observed was bruising (5.3%).
Conclusions:
Bellafill (ART) brow lift is a safe and effective minimally invasive procedure that uses no anesthesia (except synthetic ice) with microcannula filler administration, which reduces side effects and complications. This technically simple procedure provides long-term brow lift results comparable with surgical therapy outcomes in selected patients.
Introduction
Periorbital aesthetics is paramount to beauty. As one gazes into another’s eyes, the area around the globe is appreciated. Periorbital rejuvenation of the brow, eyelids, and midface (tear trough, malar eminence, and submalar area) provides the greatest aesthetic impact, more than any other anatomic area of the face. 1
The aging process steals our facial youthfulness by characteristically atrophying the skin, soft tissues, and bony framework.2-4 Aging of the upper third of the face is primarily a result of the loss of elastic tissue support from senile changes of both collagen and elastin fibers combined with the depressive forces of gravity. 2 However, bone loss also occurs mainly in periorbital and mid-cheek areas with bony orbit enlargement with corresponding changes in the appearance of the overlying skin and brow support structures. 5
Common aesthetic management of the aging brow and forehead centers on a variety of surgical approaches.6-9 These surgical procedures take into consideration the amount of brow elevation desired, correction of brow asymmetries; treatment of muscle activity (forehead, corrugator supercilia, and procerus) resulting in wrinkles or furrows, and avoidance of brow hair alteration. Compared to other forehead or brow lift surgical procedures, a direct brow lift (incision and skin excision along the superior brow hairline) provides the best brow suspension with the most precise brow position and contour, where the mechanical force is focused immediately along the site of suspension. 6
A problem-specific approach to contemporary management of the aging brow combined surgical options, mainly the endoscopic and direct brow lift surgical options, with botulinum toxin type A or Botox (BTX). 6
Although surgery is postulated to yield more effective brow lifting, nonsurgical or noninvasive approaches have an innate advantage associated with minimal to no downtime and lower incidence and severity of morbidity (ie, side effects and complications). There are concerns related to effectiveness or sufficient brow lifting, longevity of suspension, and predictability of nonsurgical approaches.
An early study by Frankel and Kamer 10 showed that addressing an improvement of glabellar frown lines and/or a low-positioned medial brow by injecting BTX into the corrugator supercilii and procerus muscles produced a raise in the medial brow. Objective results revealed a raise in the medial brow in 32% from the medial canthus measurement and in 48% from the midpupil with 62% of patients noting a subjective higher medial brow position. 10 Neuromodulators have achieved temporary brow lifting by altering the brow depressors (orbicularis oculi for lateral and mid-brow, procerus and corrugator supercilli for medial brow) mechanical vector forces to allow the frontalis muscle to raise the eyebrows. Botox has been routinely used for temporary medial and/or lateral brow lifting, but the amount of eyebrow lifting is difficult to predict by targeting glabellar and/or crow’s feet anatomical areas with lower than optimal success rates.9-13
Current noninvasive brow lifting options noted in the medical literature include neuromodulators, energy-based systems, and dermal fillers alone or in combination. Minimally invasive brow lifting procedures include barbed sutures, helium-based plasma radiofrequency technology (HBT) (Renuvion) with or without VASER ultrasound, and fat grafting to the brow, forehead, and/or temporal fossa.
Laser skin resurfacing highlighting fractional carbon dioxide (10 600 nm) and erbium (Er)-YAG (2940 nm) lasers as well as microneedling radiofrequency (RF) (10 or 20 MHz) treat the skin itself to cause skin tightening, which indirectly lifts the brow. 14 Combining temporal volume with energy-based devices at a single session has shown to be safe and effective rejuvenation of the temporal area and brow. 14
There are devices that penetrate deeper than the skin surface to affect subdermal tissues targeting fat and/or facial muscles while also treating (ablative) or not treating (nonablative) the surface epidermis. Energy-based devices incorporating focus-imaged ultrasonography or Ultherapy (Ulthera, Inc., Mesa, Arizona). 14 Focused ultrasound, laser, and both unipolar and bipolar RF devices delivering sufficient thermal injury (65-70°C) to contract and reorganize collagen fibers have been observed to result in the onset of perceived tissue lifting by 3 months post-treatment with a 1-year duration of clinical lifting responses. 15 Sasaki concluded that focus-imaged ultrasound cutaneous energy delivery in vertical treatment lines and higher energy deposition increased the percentage of tissue lifting with 51.4% to 71% were graded as showing a degree of response. 16 In addition, Weschler concluded that treatment with micro-focused ultrasound with visualization with vertical vectoring demonstrated appreciable lifting and tightening of facial and neck tissue resulting in improved alone or simultaneously with upper cosmetic eyelid surgery (blepharoplasty). Using the global aesthetic improvement scale (GAIS) scores and a high degree of patient satisfaction for up to 1 year. 17 Unfortunately, authors note a wide variation in consistency and predictability of results (40%-80% response) at 1 year after noninvasive treatments.18-21 Nonenergy-based skin treatments such as chemical peels, used mainly for skin resurfacing, may produce some skin tightening that can result in a degree of brow position changes.
There are also innovative methods that combine surgical modalities with an energy-based device that causes subdermal collagen fiber retraction (65% fiber retraction when temperature reaches 85°C for 0.08- to 0.44-second duration) with or without fat removal that results in skin retraction. 22 Regarding the forehead area, a more generalized brow lift or complete forehead lift may be achieved. Sterodimas et al 23 revealed the effectiveness (100% patient satisfaction) of HBT or Renuvion (Apyx Medical, Clearwater, Florida) in reducing visible forehead lines and elevating the eyebrows to provide a more youthful appearance by addressing laxity and ptosis in the brow, forehead, and upper eyelids. Other authors have shown this innovative technique of HBT subperiosteal brow lifting is safe, effective, and long-lasting (over 3 years). 24
Volume replacement by silastic implants, fat grafting, and/or filler placement into the temporal hairline, into the temporal fossa, and/or along the superior aspect of the brow hair are alternative options to provide a brow lift. Othman et al 25 performed a literature search systematic review in 2020 and noted 4 articles using implants: 2 using methyl methacrylate26,27 and 2 implanting expanded polytetrafluoroethylene or Gore-Tex.28,29 Facial implants made of silastic offer the optimal implantable substance since there is no tissue ingrowth, which makes revision surgery rapid and uncomplicated, negligible to no tissue reaction, easily modifiable, and permanency.
Silastic implants (Implantech Associates, Inc., Ventura, California) designed for the temporal fossa can augment part of the fossa, the entire fossa, or with patient-specific or custom designed implants enhance part or the entire temporal and/or forehead anatomic areas. 30 The temporal fossa anatomy reveals that implants or fat grafting can be placed in different anatomical planes to include above or below the deep temporalis fascia or in the subperiosteal plane.31,32
Autologous fat grafting on the upper face with the greatest volume correction into the temporal fossa rejuvenates the aging face and may produce a lateral brow lift. 33 There is permanent yet varied and inconsistent volume replacement outcomes because of the non-standardized and differing techniques in fat harvesting, processing, enrichment, and administration.31-35
There are numerous temporary dermal fillers to include hyaluronic acid (HLA), calcium hydroxyapatite (CaHA), and poly-
The aging process results in the temporal fossa becoming more concave, which emphasizes the lateral orbital rim prominence and pulls the tail of the lateral brow inferiorly and posteriorly. Temporal fossa augmentation not only improves a deflated temple but also contours the upper face with secondarily lengthening and lifting the lateral brow. 38
The retro-orbicularis oculi fat (ROOF) or brow fat pad is the thin fibrofatty layer of tissue between the orbicularis oculi and frontalis muscles. Fillers can contour the brow and add volume to this area, which is generally injected into subcutaneous, sub-ROOF, or supraperiosteal planes. 38 The filler has the advantages over BTX by achieving support of these periorbital soft tissues. Higher HLA filler elastic modulus or stiffness known as G′ contributes to efficacy of overlying skin and soft tissue lifting. 36 The increased HLA viscosity assists in resisting spread to adjacent areas, which can diminish the aesthetic appearance and tissue vectoring, while increasing the complication rate.
In an attempt to provide the same effectiveness and precision of suspension as surgical therapy, especially comparing the surgical direct brow lift, placing a dermal filler along the superior half of the hair of the eyebrow was hypothesized to create an effective nonsurgical brow lift. 38 Since the preferred result is a long-term or permanent outcome, the filler chosen to be administered was the only long-term or permanent filler approved by the FDA. This dermal filler is composed of bovine collagen gel suspended polymethylmethacrylate (PMMA) microspheres, known as Artefill (ART). The US manufacturer changed the name to Bellafill (Tiger Aesthetics Medical, LLC, Franklin, Wisconsin).
This third generation of PMMA spheres have a greater uniformity of size and shape, a smoother surface, a lower rate of clumping with the improved suspension medium (bovine collagen), and less granuloma or nodule formation. 39 The proposed mechanism of action of the PMMA microspheres is that they create a matrix that supports endogenous human collagen synthesis and long-term residence in soft tissues. 40 A study revealed anywhere between 50%, but closer to 100% of the bovine collagen gel is replaced by endogenous human host collagen. 41 Histologic studies have shown that PMMA microspheres cannot be broken down by enzymes, since a methyl group in the alpha-position stabilizes the molecule. 40
Patients were educated about the indications for skin testing prior to treatment with Bellafill. A European clinical trial of 1280 patients revealed only one patient with a systemic allergic reaction reported to the manufacturer of the same collagen used in Artecoll and Bellafill. 42 Lemperle et al observed only 2 acute allergic reactions among more than 3000 patients after Artecoll implantation. Interestingly, both patients had negative skin testing prior to treatment. 42
Material and Methods
The investigation followed rules of the Declaration of Helsinki of 1975 and 2013, and was approved through Touro University Nevada Institutional Review Board TUNIRB00178. GenAI was not used in the preparation of the article.
Patient Selection
Patients presented for different reasons or complaints: (1) evaluation of upper eyelid dermatochalasis, (2) facial volume replacement, (3) general aesthetic facial evaluation, and (4) specifically for brow ptosis. All patients treated with ART to the brow were noted to have brow ptosis by physical examination. Those estimated to have less than 3 mm of brow ptosis (mild severity) were given the option of treatment using a long-term dermal filler instead of surgical therapy.
Those with more significant brow ptosis or significant asymmetry were recommended to undergo surgical therapy with most choosing a type of temporal brow lift or endoscopic approach. Those concerned about wrinkles or furrows caused by animation of frontalis, corrugator supercilia, and/or procerus muscle action were recommended to combine a neuromodulator to the planned treatment.
Pre-Treatment ART Assessment
Patients presenting for facial rejuvenation completed a detailed medical and surgical history, including inquiring about allergies to both lidocaine and red meat. Those with no history of allergic response did not undergo allergic skin testing. 43 The use of aspirin, non-steroidal anti-inflammatory drugs, fish oil, or other anti-coagulants were questioned. Previous facial treatments including surgery and use of dermal fillers were queried regarding the adverse reactions, complications, type, amount, and anatomical sites of filler injection.
Brow Physical Examination
The aesthetic examination concentrated on the upper third of the face and the upper eyelids. The comprehensive brow examination shapes therapeutic options and their likelihood of success (Table 1).
Pertinent Brow Physical Findings.
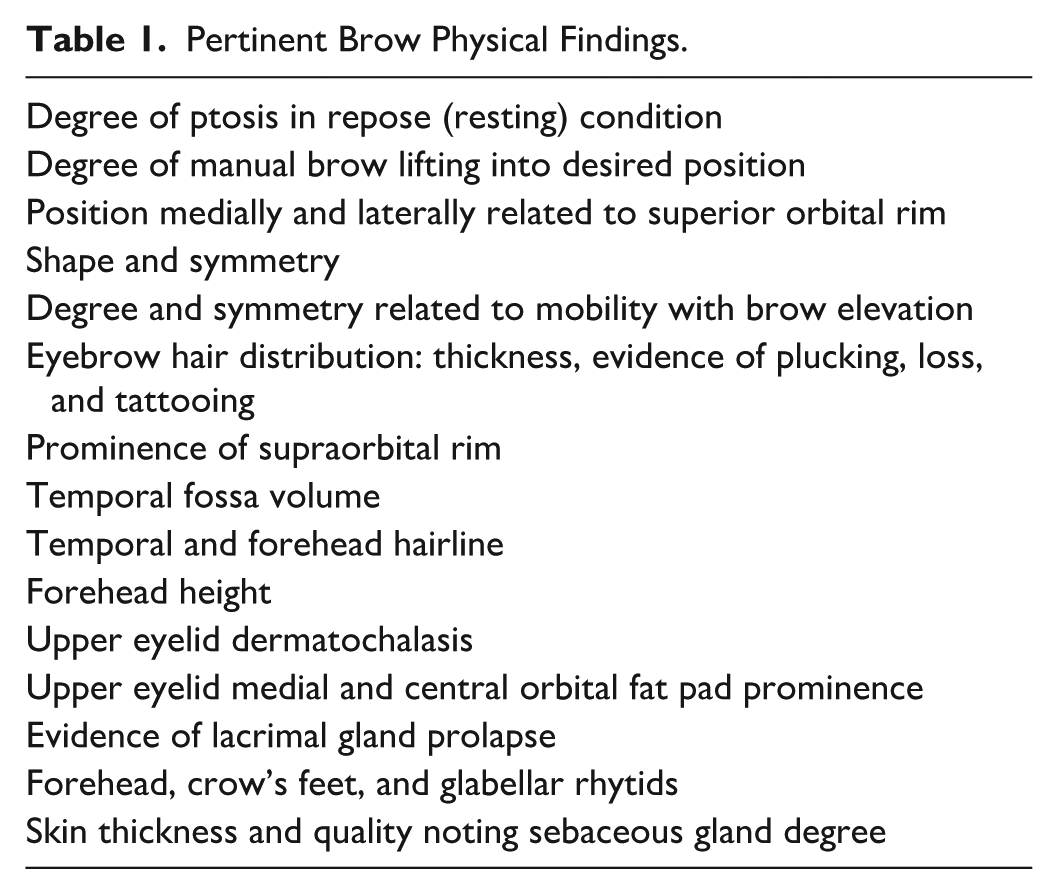
The goal is to yield a suspension of the brow, while achieving the ideal eyebrow shape and position. An ideal men’s brow is horizontal at about the level of the supraorbital ridge. The ideal woman’s brow has a much more complex appearance (Figure 1).
Female ideal eyebrow spatial relationships landmarks for brow position are related to the underlying bony anatomy. The ideal female eyebrow begins medially at or just inferior to the supraorbital rim (B) with its greatest width there. Its medial extent at a vertical line connecting the medial canthus (G) to the nasal lateral ala (A). The eyebrow hair proceeds laterally along an inclined line above the supraorbital rim, peeking (E) between the lateral limbus (D) and the lateral canthus (F). The lateral extent of the eyebrow hair (C), which thins or is tapered, is at the diagonal line connecting the lateral ala (A) to the lateral canthus (F).
It was best to demonstrate true brow ptosis in front of a mirror after encouraging the patient to relax the frontalis muscle. Thereafter, the brow was digitally repositioned to illustrate the degree of elevation necessary to acquire the desired cosmetic effect.
ART Dermal Filler Material
Artefill contains atellocollagen (bovine) 3.5%, phosphate buffer 2.7%, sodium chloride 0.9%, lidocaine hydrochloride 0.3%, and water 92.6% with a pH between 6.9 and 7.0. 44 The manufacturer combines 6 ml (23%) of PMMA with 20 ml (77%) of bovine collagen gel together and fills syringes to about 0.85 ml. The FDA-approved indications for use of ART were for the correction of nasolabial folds (NLFs) and correction of moderate to severe, atrophic, distensible facial acne scar on the cheeks. 44
Artefill is an excellent filler material to achieve lasting improvement of facial wrinkles and furrows, acne scars, other soft tissue contour deficiencies and pan-facial volume deficiencies.39,41,43 Artefill can be safely injected with excellent aesthetic outcomes in all areas of the face (most off-label indications), excluding the bulk of the upper and lower lips.
ART Skin Testing Determination
A “Bellafill” Informed Consent form reviewing the risks and possible complications was reviewed with the patient. Patients were given the option of a skin test prior to treatment. However, if the patient did not have an allergy to either red meat (bovine collagen) or local anesthetics (lidocaine), the patient was informed that a skin test was not required. 43
Dermal Filler Injection Technique
The desired location for suspension and shape of eyebrow was reviewed. The specific anatomical site (medial, lateral or both) for ART placement to address the exact region of ptosis. Artefill placement along the superior brow hair was designed to create the ideal brow shape and position as confirmed with the patient prior to treatment (see Bellafill brow lift technique video). A customized small artificial ice pack was applied to the brow for at least 10 seconds or until the patient could not tolerate it topically any longer, which was used for both anesthetic and hemostatic effects. Alcohol swabs cleaned the treatment area.
The tissue plane of filler placement was into the immediate subdermal plane at the superior aspect of the eyebrow hair. If the brows were symmetric, half of the treatment syringe was injected per side (approximately 0.4-0.45 cc). If a patient had brow ptosis asymmetry, more of the filler was administered to the more ptotic side. Most patients were injected with a microcannula. Needle injection was used for fine tuning, if necessary. An entry port was produced with a 23 G needle at the lateral most aspect of the brow injection prior to cannulation with the 25 G 1½-inch-long microcannula.
The choice of microcannulas was either the DermaSculpt (Cosmofrance, Inc., Miami, Florida) or Steriglide (TSK Laboratories, Inc., Oisterwijk, The Netherlands) using a 25 G 1½-inch microcannula. The needle used was that accompany the ART syringe of 26 G, 5/8-inch needle supplied by the manufacturer.
After the injection was complete, mild manual compression for at least 2 minutes to the entry site was performed to minimize bruising. Thereafter, the exact area of brow placement was gently massaged between 2 fingers to ensure a smooth contour and brow shape optimized. The treated area was not compressed downward to avoid flattening the filler appearance. Arnica Montana as a lubricant and anti-bruising gel.
Combining Aesthetic Treatments
If the patient is contemplating a skin resurfacing or tightening procedure(s) as well as considering brow lifting, the patient was counseled to initially perform the energy-based device (carbon dioxide laser or microneedling RF). Swelling from these procedures mostly resolves by 2 weeks and it takes at least 2 to 3 months to achieve the initial skin tightening from these energy-based devices. If performed associated with an upper blepharoplasty, the brow lift is always performed first. When using a Bellafill brow lift, it is best to perform it at least 1 week in advance to assess efficacy. However, often patients requested it to be performed on the day of blepharoplasty surgery.
Aesthetic Follow-Up Visits
Standard follow-up after all dermal filler injections, including ART brow lifting, was at 1 to 2 weeks, 4 to 6 weeks, 3 months, 6 months, and each year thereafter if possible. History and physical examination assessment of the presence of any complications, satisfactory aesthetic brow position and shape, need for additional brow treatments, and interest in any adjuvant aesthetic therapy was carried out. The potential additional treatments considered were neuromodulators for periorbital wrinkles and furrows, eyelid surgery for dermatochalasis, skin resurfacing to smooth skin texture, skin tightening technologies, and facial volume replacement treatment options. If patients desired additional brow lifting, the patient and physician made a realistic determination if additional filler placement had a good chance of suspending the brow further without creating excess and unnatural suprabrow fullness.
Patient objective measurements were acquired from 3 to 6 months after the Bellafill brow lift. Long-term (12 months to 8 years) follow-up was assessed in most patients with high persistent patient satisfaction, but these were not tabulated.
Determining ART Brow Lift Treatment Success
Patient satisfaction input was acquired related to no change or minimal improvement with persistent ptosis versus improvement to satisfactory brow position. The other inquiry was if any brow asymmetry existed, if it was bothersome to the patient, and if the patient requested some form of additional treatment. The GAIS was the overall patient-reported outcome measure used to determine patient satisfaction. If insufficient brow lifting was observed, the patient was educated on 3 options: (1) no further treatment, (2) an additional ART brow injection, or (3) consideration for surgical brow lift options.
The treatment goal was to give an overall brow position perception of being raised, understanding the variability of medial, lateral, and more impactful aesthetically, peak brow anatomic sites. Artefill was injected into either the medial, lateral, or the entire extent of the brow after site of ptosis was visually confirmed.
Clinical Study Photographic Analysis and Measurement Methodology
Before and after 35 mm or iPhone photography were obtained. Brow position measurements were performed using Adobe Photoshop CS6 with the Ruler Tool. A standardized digital measurements protocol to ensure consistency and accuracy across subjects. Patients did not have a neuromodulator injection within 3 months of taking after photographs for measurements. Some patients did undergo upper eyelid cosmetic surgery (blepharoplasty) around the time of ART brow placement.
Step-by-step process are as follows:
1. Image preparation. Both before and after photographs in repose (relaxed state) were imported into Adobe Photoshop CS6 and displayed side by side for simultaneous comparison.
2. Magnification and iris calibration. Each image was digitally sealed to match an iris diameter of approximately 12 mm, which reflects the human physiological range (11-13 mm). This provided a consistent reference size for all subjects regardless of camera distance or zoom level.
3. Scale adjustment. Using the “Ruler Tool” from the Photoshop toolbar, the measurement scale was calibrated, so that 112 pixels = 10 mm. Calibration was verified by overlaying the Photoshop ruler against an actual metric ruler.
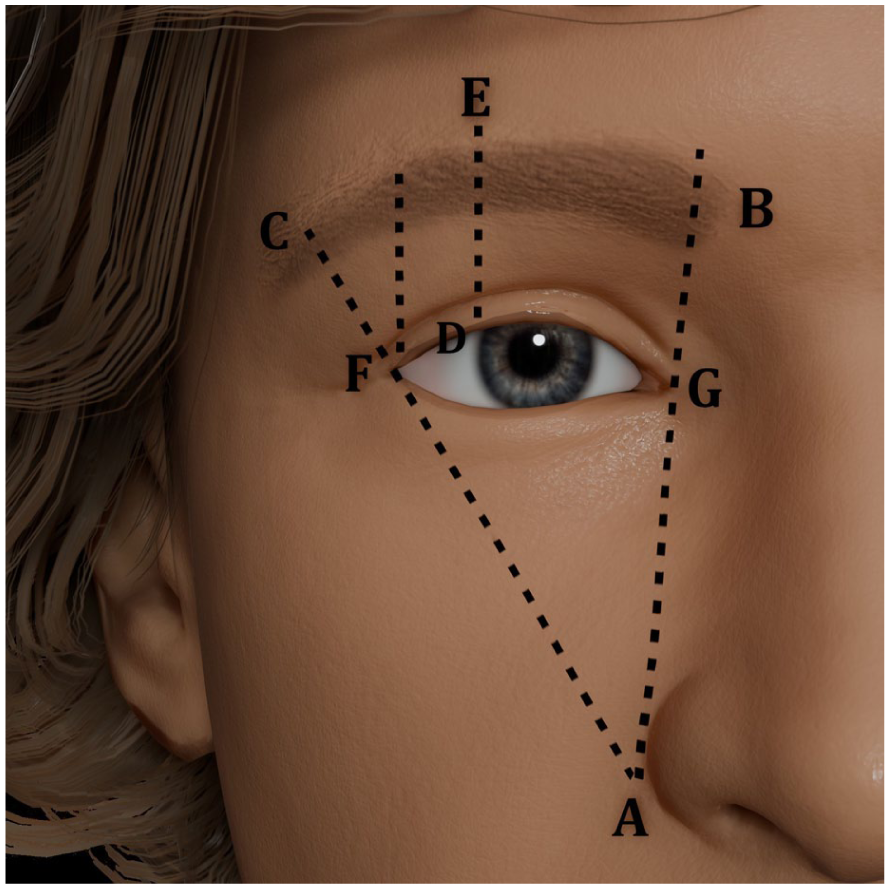
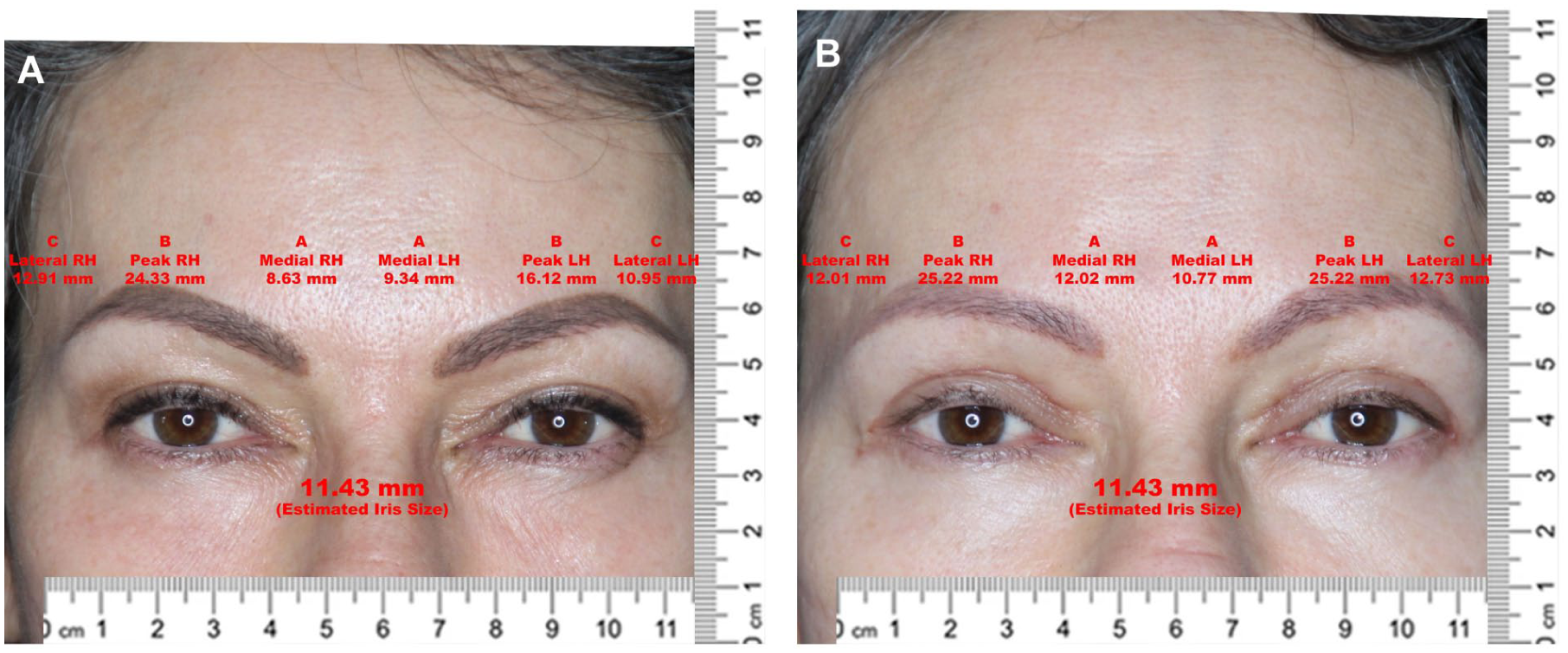
4. Measurement points defined (Figure 2). On each brow, 3 anatomical landmarks were identified and measured relative to the fixed ocular reference points (ie, canthi):
(a) Medial. Distance from the medial canthus to the medial brow border (b) Peak. Distance from the pupil centerline/brow peak to the superior brow margin below the peak (c) Lateral. Distance from the lateral canthus to the lateral brow border
5. Data collection. Measurements were obtained bilaterally both before and after. With 12 measurements per patient.
6. Change calculation. The difference between before and after values was computed for each brow segment (medial, peak, and lateral) on both sides to quantify vector displacement in millimeters.
7. Verification and data entry. All numeric values were verified on 2 different occasions for accuracy and entered into a spreadsheet for statistical analysis.
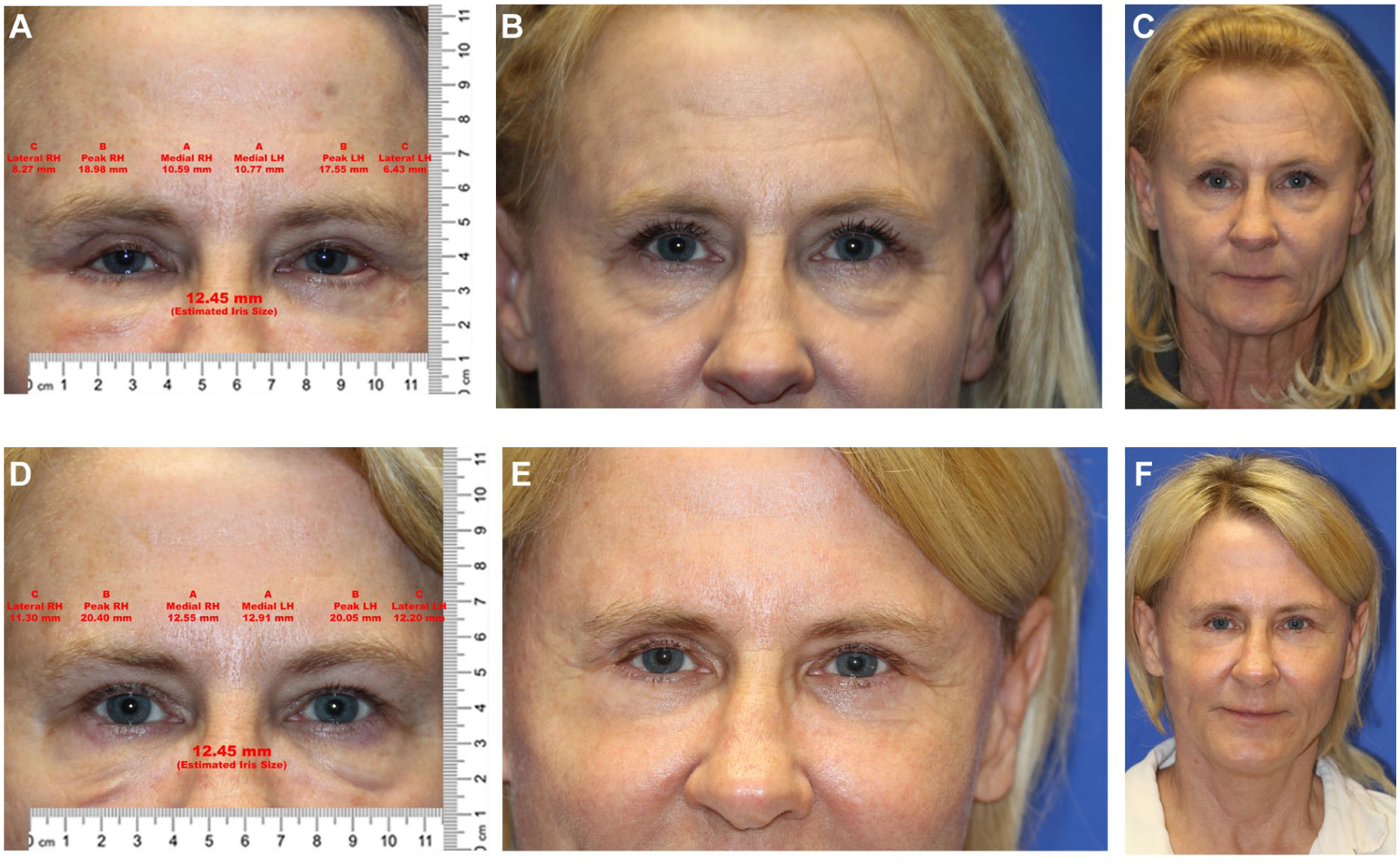
Brow measurement points defined. The medial, peak, and lateral brow positions (before and after ART injection) were measured relative to the fixed medial and lateral canthi using Adobe Photoshop CS6 software. Fifty-nine-year-old woman who underwent Bellafill brow lift with ART injection into full brow length and, upper blepharoplasty with 8 mm of skin excision. She also had facial rejuvenation by lower blepharoplasty, midface lift with small combined submalar implant, and deep-plane facelift. Before (A), measurements (B), close-up eyes (C), full-face, and after (D), measurements (E), close-up eyes (F), and full-face.
Results
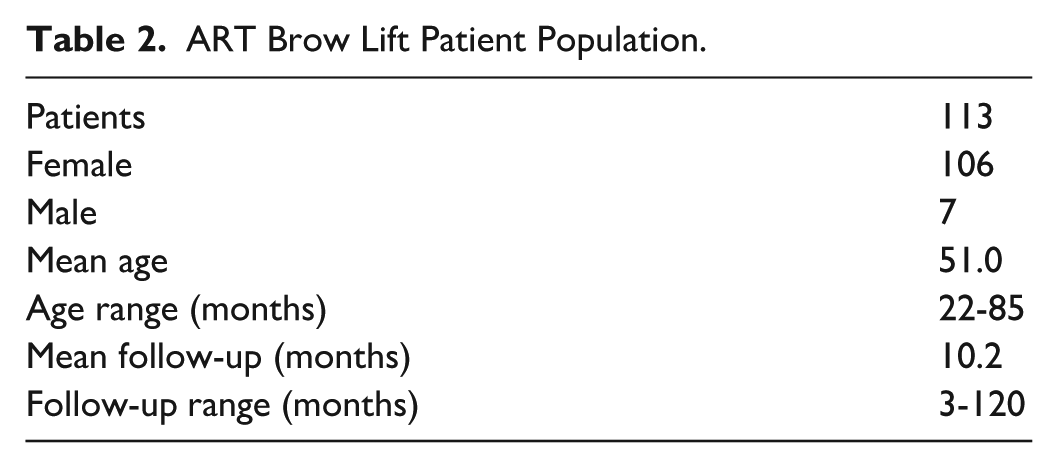
From 2015 through 2022, the above inclusive patient population (n = 113, Table 2) underwent a Bellafill brow lift. The majority of patients were injected with a 25 G 1½-inch microcannula (95.6%, n = 108) compared with the accompanying filler 26 G 1½-inch needle. Ninety-two percent used only one syringe, while 8.0% (n = 9) underwent 2 syringes separated by at least 2 months.
ART Brow Lift Patient Population.
Patient overall satisfaction rate was 88.5% (n = 100) using the GAIS with very much improved or improved responses. Brow measurements were tabulated with 80.0% having elevation at site of ART injection by 1.0 to 3.5 mm (Figure 3). Both those without blepharoplasty (Figures 4 and 5) and those who underwent upper blepharoplasty (20.4%, n = 23, Figures 6 and 7) were analyzed.
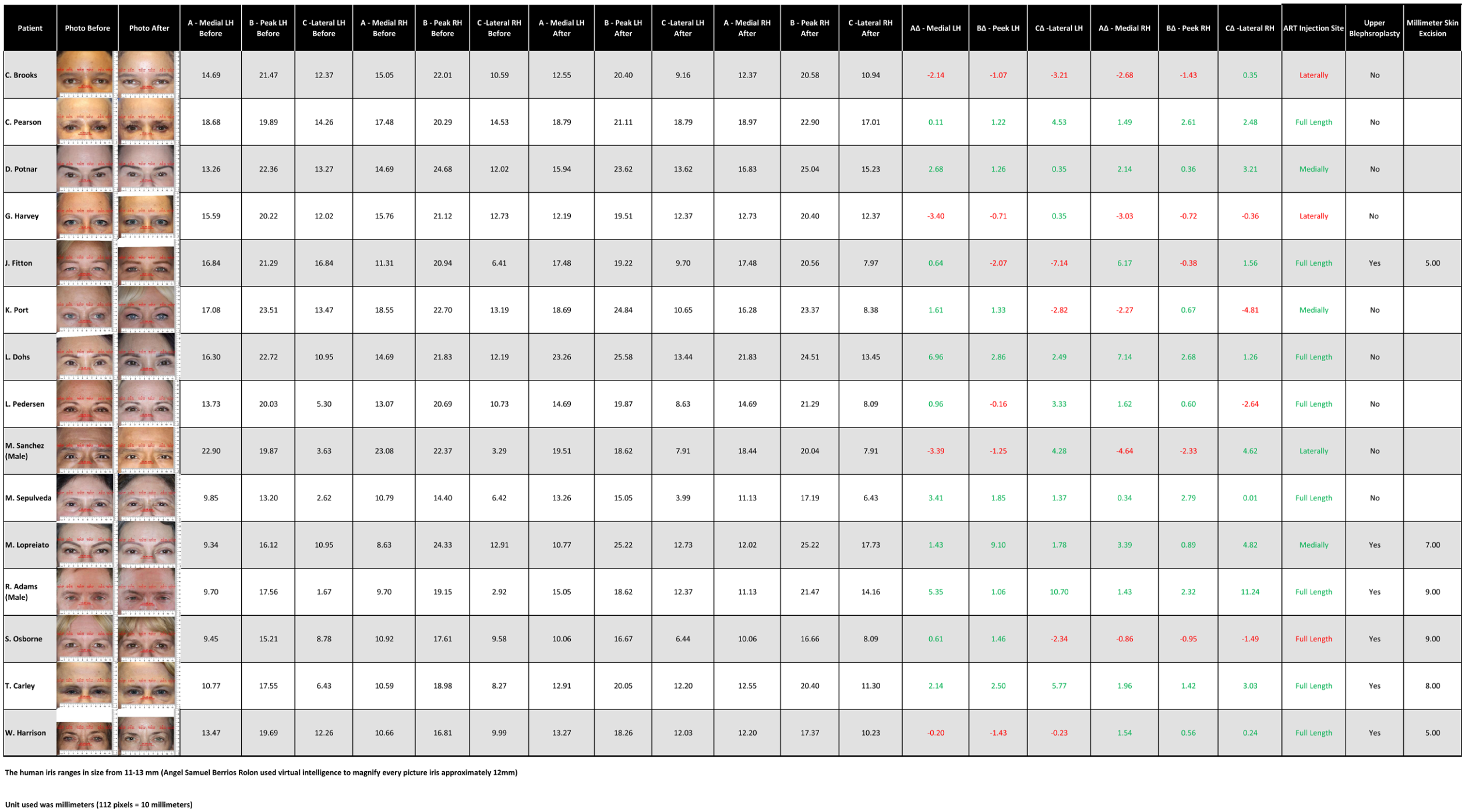
Brow Measurements Tabulated. The before and after ART injection brow measurements were tabulated noting changes to the medial, lateral and peek brow anatomic sites with mean follow-up of 10.2 months. Green colored numbers represent elevation in brow position, where red note a reduction.
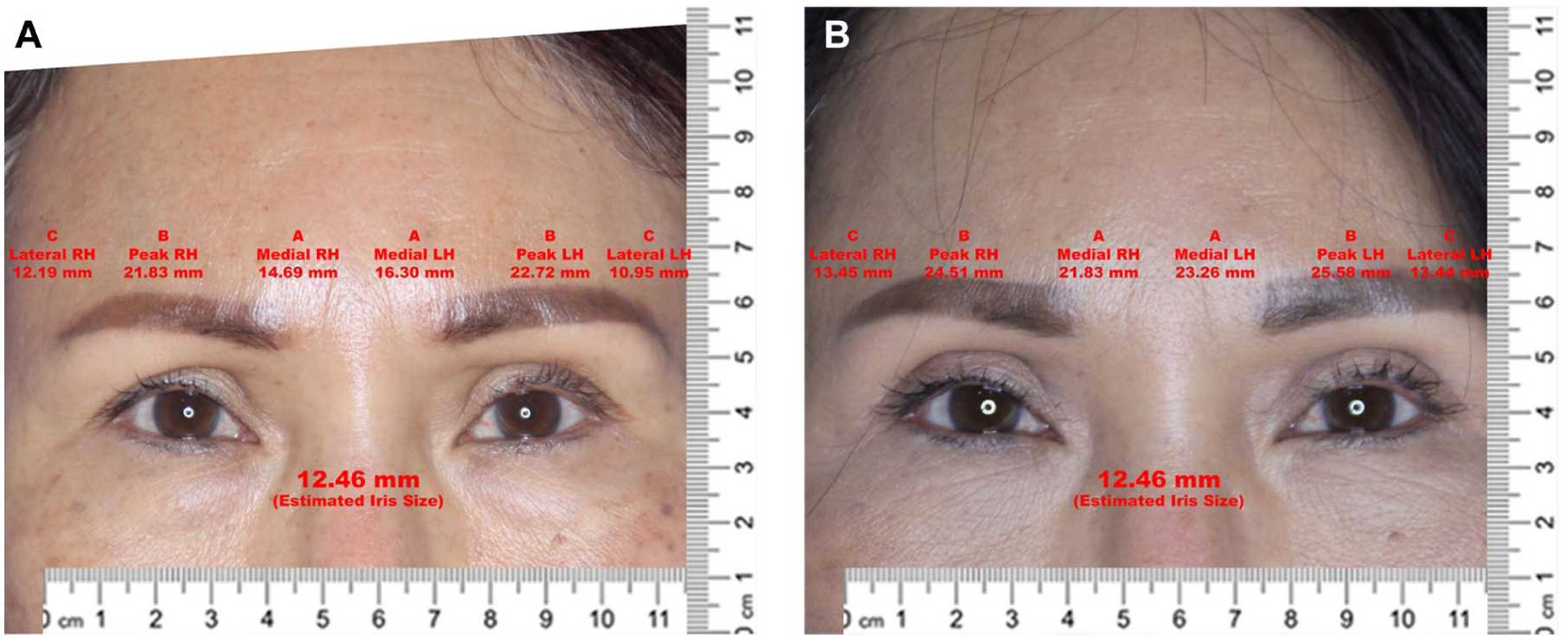
Bellafill brow lift without upper blepharoplasty. Sixty-two-year-old woman with one ART syringe injection along full brow length who did not undergo eyelid surgery. (A) Before and (B) after (14 months).
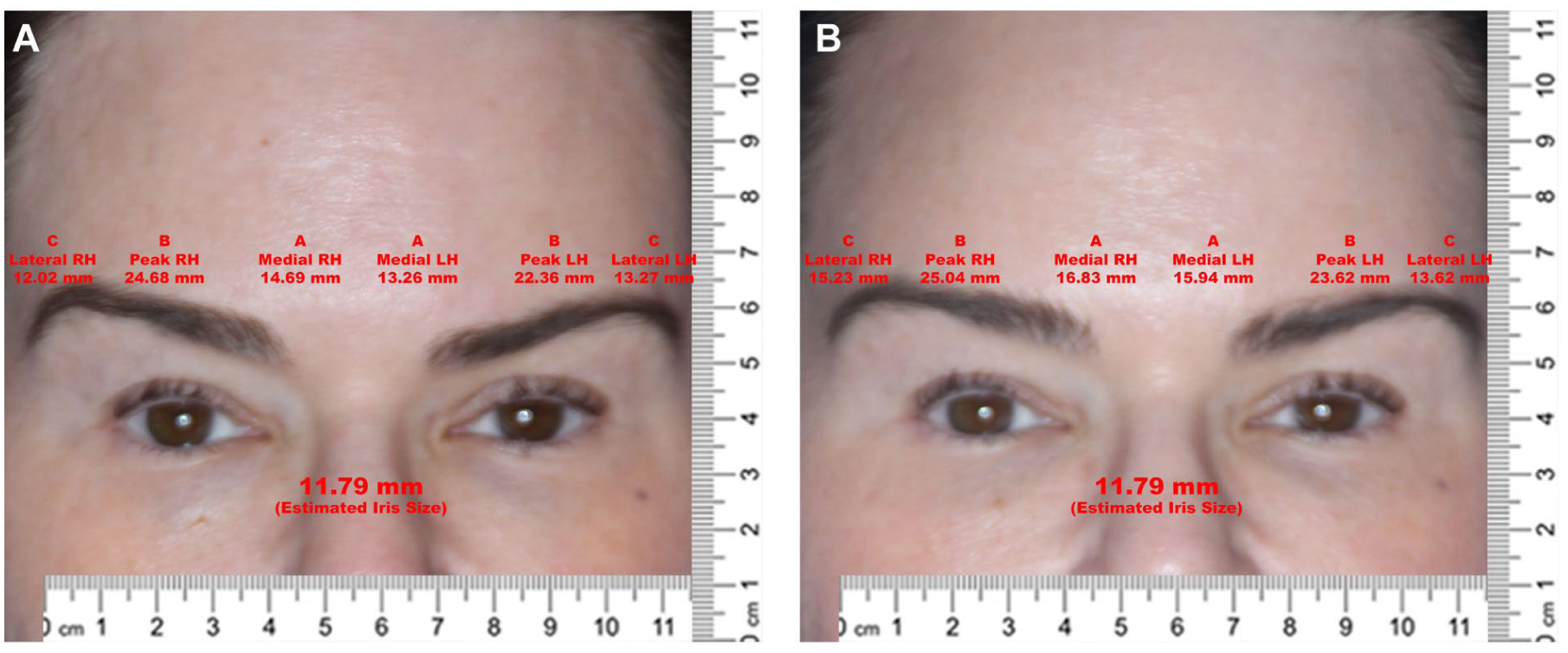
Bellafill brow lift without upper blepharoplasty. Fifty-year-old woman with one ART syringe injection at medial brow site who did not undergo eyelid surgery. (A) Before and (B) after (6 months).
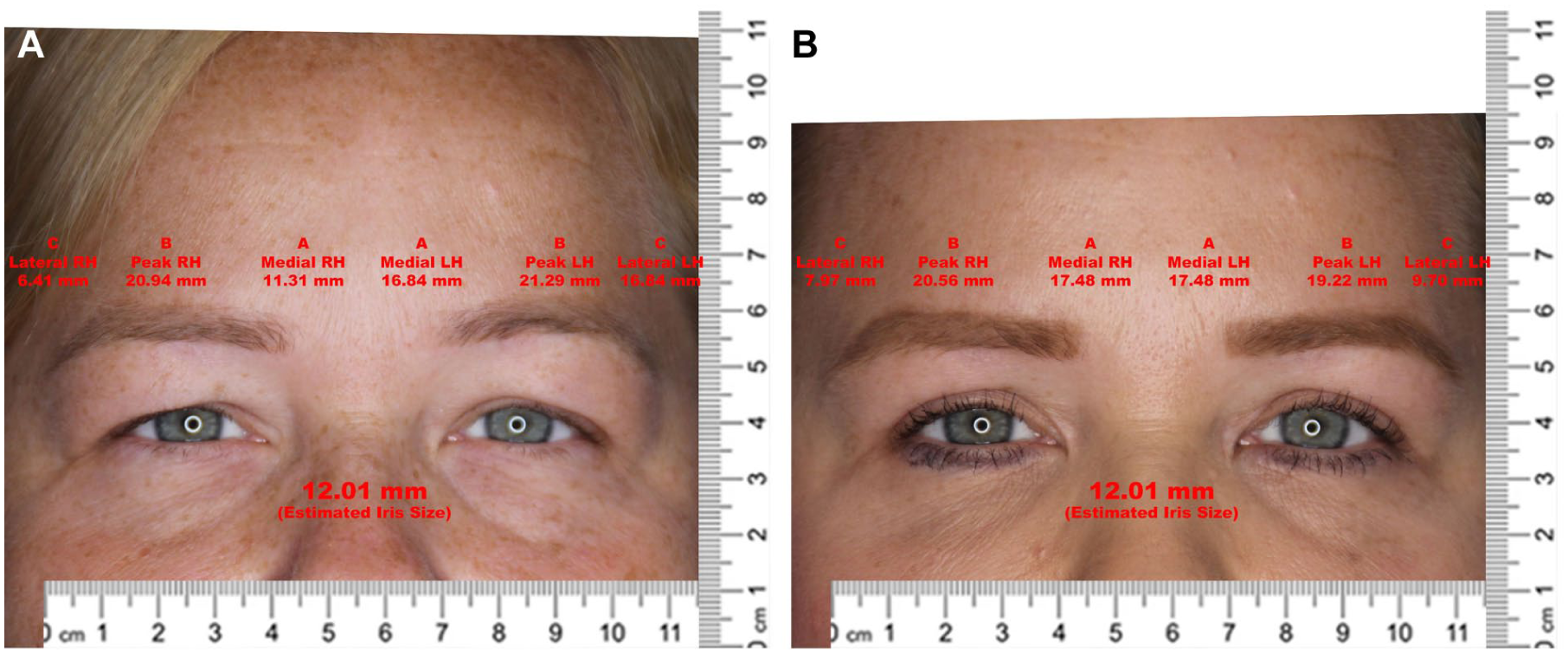
Bellafill Browlift With Upper Blepharoplasty. Forty-five-year-old woman underwent treatment with one ART syringe injection along full brow length who underwent upper blepharoplasty with 5 mm of skin excision at same setting. (A) Before (B) After (8 months).
Bellafill brow lift with upper blepharoplasty. Fifty-six-year-old woman with one ART syringe injected at medial brow site who underwent upper blepharoplasty with 7 mm of skin excision. (A) Before and (B) after (8 months).
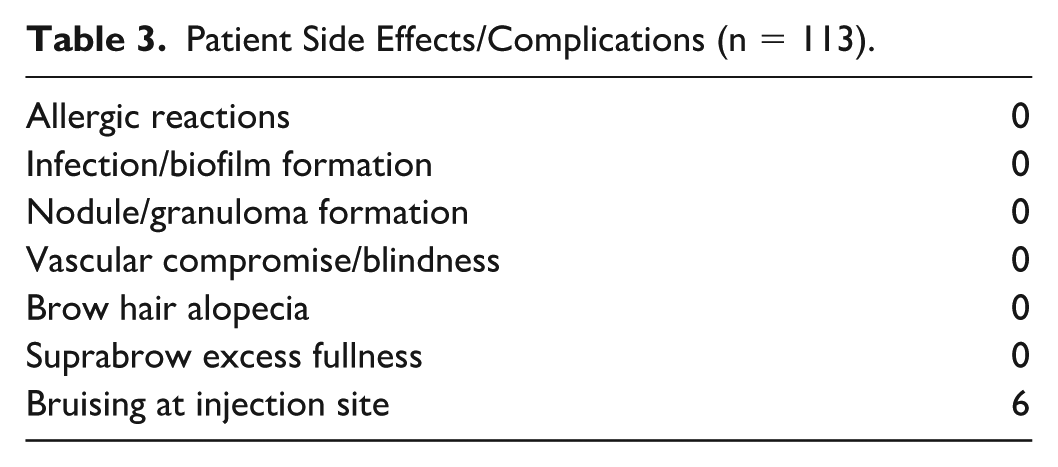
The only side effect or complication observed was bruising (5.3%, Table 3). From the authors’ observation, nearly every patient queried at the 1- to 2-week follow-up stated that about 80% of the initial volume augmented persisted.
Patient Side Effects/Complications (n = 113).
There was no change in the degree of brow suspension perceived by patients comparing immediate response within 1 to 2 weeks post-injection and 6 to 12 months after the procedure. Objective measurements of brow position changes from pre- to post-injection were acquired from 3 to 6 months after the Bellafill brow lift procedure. Long-term (12 months-10 years) follow-up was assessed in most patients with high persistent patient satisfaction, but these were not tabulated.
There was no observed nodule (granuloma) formation, hematoma, alopecia, pilot hole skin scarring, irregularities, infection, allergic reactions, excess filler placement, or vascular compromise in any patient.
Statistical Analysis
The injection site of the brow was noted as being full (entire brow hair length), medial, or lateral aspect related to the observed site of brow ptosis. Only brow anatomic regions corresponding to specific filler injection sites were analyzed. The non-injected brow regions were excluded from the measurement analysis.
The measurement of the new brow height after ART injection showed positive (brow elevation) or negative (brow descent) values (Table 4). There was a sum of positive ranks of 93 and sum of negative ranks of 27. A composite injected site brow elevation score was calculated for each patient and compared to baseline using the Wilcoxon signed-rank test analyzed the data. The Wilcoxon test statistic (W) was 19 of the sample size of 15 evaluated. The composite change in brow position using ART brow lift revealed a statistically significant increase in brow height at the injected site compared with baseline (W = 19, P = .018). Positive values for brow lifting showed a range of 0.34 to 5.4 mm elevation with a mean of 2.13 mm at 10 months.
ART Brow Lift Statistical Analysis.
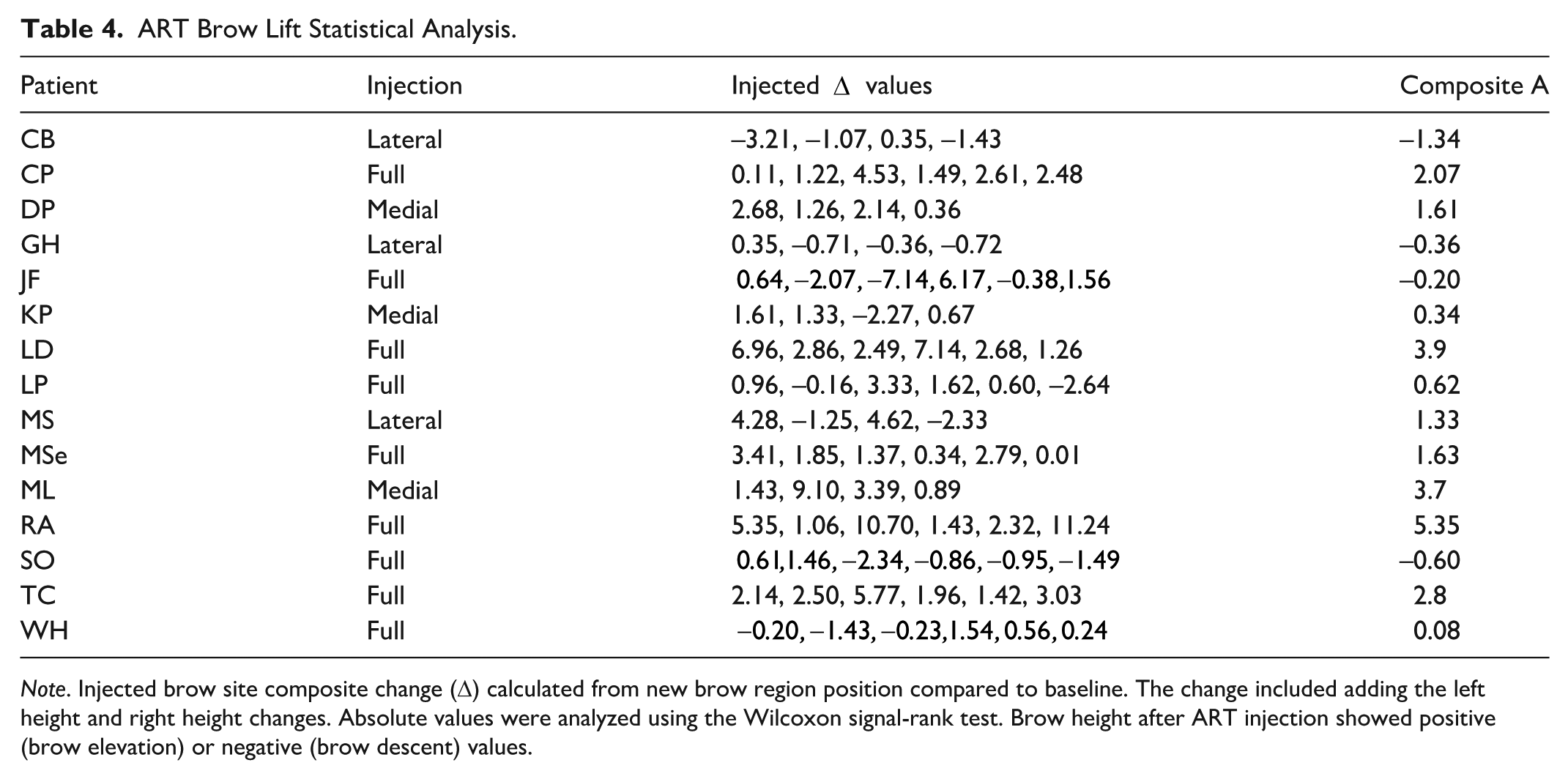
Note. Injected brow site composite change (Δ) calculated from new brow region position compared to baseline. The change included adding the left height and right height changes. Absolute values were analyzed using the Wilcoxon signal-rank test. Brow height after ART injection showed positive (brow elevation) or negative (brow descent) values.
Discussion
Brow lifts may provide a significant reduction in perceived age. In a study comparing upper blepharoplasty alone, brow lifting alone, and combining these procedures, they concluded that when planning periorbital rejuvenation, a thorough preoperative evaluation should be performed, and consideration should be given to brow lifting procedures. 45
The ideal candidate to attempt an ART brow lift is a patient with an isolated area of brow ptosis of mild severity. Isolated medial brow ptosis is difficult to address surgically, and this study illustrates brow suspension using ART is safe, simple, rapid, effective aesthetic procedure with no downtime. Most patients due to the aging process acquire some degree of temporal fossa volume loss. When lateral brow ptosis concomitantly exists with this volume loss, volume replacement in the temporal fossa, and/or lateral brow area may achieve a satisfactory brow suspension.
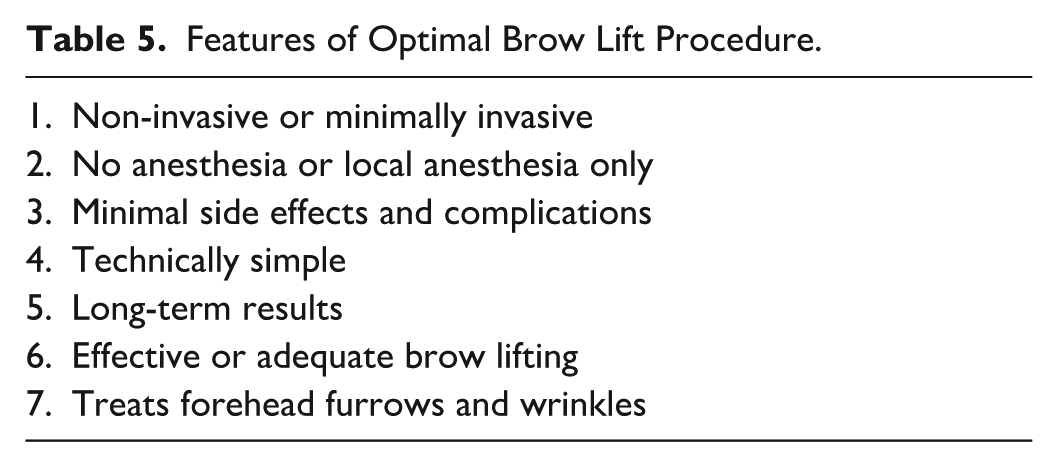
An optimal brow lifting procedure would offer numerous benefits with minimal risks (Table 5). Artefill brow lifting achieves all the optimal procedure features, except for treating forehead furrows and wrinkles. These can be effectively treated, albeit temporary, by the addition of a neuromodulator to provide a complete minimally invasive rejuvenation treatment.
Features of Optimal Brow Lift Procedure.
To achieve patient satisfaction, one should develop a comprehensive yet individualized periorbital aesthetic rejuvenation treatment plan.1,6 This plan strives to optimize the cosmetic result, while anticipating post-operative outcomes and identifying predisposing factors to complications. One should identify jointly with the patient the anatomical aesthetic issues of concern and then review all alternative treatment options.
Most patients prefer to avoid surgical therapy if the likelihood of achieving their aesthetic goals can be realistic attained with either noninvasive or minimally invasive treatments.
Bellafill (ART) brow lift in patients presenting with mild brow ptosis revealed this approach as a validated highly successful alternative to surgical therapy (88.5% patient satisfaction rate). The high patient satisfaction rate combined with the easily mastered, minimally invasive injection technique attracts patients and medical aesthetic professionals alike. Proper patient selection with mild brow ptosis with or without asymmetry can be treated successfully without surgery using ART.
Previous clinical studies have shown the benefits of blunt microcannulas for filler placement.13,44 A consensus recommendation of the use of microcannulas for filler placement found improved safety, decreased risk of ecchymoses, faster return to normal daily activities, and in some patients, an improved comfort during the injection. 44 The panel stated the safety and efficacy of filler injections ultimately depends on the knowledge and skill of the injecting physician. 44 Our study confirmed the literature findings that microcannulas minimize the risk of injecting fillers too superficially as well as lowering adverse effects to include discomfort, ecchymoses, and vascular injury or embolization.
Longevity data revealed no change in the degree of brow suspension perceived by patients comparing immediate response within 1 to 2 weeks post-injection and 6 to 12 months after the procedure. The measurements of brow position changes from pre- to post-injection revealed objective persistence of suspension for at least the timing of the measurements at 3 to 6 months after the Bellafill brow lift procedure. Long-term (12 months-10 years) follow-up was assessed in most patients with high persistent patient satisfaction, but these were not tabulated.
The observations of this study confirmed the observations by Lemperle, that the volume of the injected ART collagen (80%) remained stable in the implant over the years. 40 The PMMA microspheres act as a scaffold and stimulus for constant collagen production, thus the bovine collagen is completely replaced by the body’s own connective tissue. 40 A significant benefit of the Bellafill brow lift is that additional filler can be injected with a 3-minute duration procedure to create more suspension of the brow caused by additional ptosis from the aging process. Patients can return to their routine life activities immediately.
Our data showed a statistically significant (P = .018) brow lift at the site or region of the brow where the ART filler was injected. The success rate was higher when the site of ptosis was isolated either medially or laterally compared to the entire length of the brow. Our results showed a range of 0.34 to 5.4 mm elevation with a mean of 2.13 mm at 10 months. There was no difference in elevation if an upper blepharoplasty was completed.
Evaluating and achieving the amount of brow lifting has been examined using different quantitative methodology. Kimbrell using helium plasma RF for subperiosteal brow lifting (n = 26) showed a mean change in forehead height decreased between 4.1 and 4.9 mm, and the mean brow height increased between 1.5 and 2.1 mm at a mean of 1-year post-treatment with 87% of patients satisfied or very satisfied with outcome. 24 Ahn et al 11 using BTX measured a mean elevation of 1.0 mm at the central brow and 4.8 mm at the lateral brow, which was unfortunately temporary for about a 3-month duration.
One of the main reasons some physicians do not implement ART into their facial volume treatment armamentarium is the risk of nodule or granuloma formation, fortunately, there were none observed in this study. Clinical data confirm that the incidence of nodules from ART46-51 is rare with a similar occurrence rate as HLA fillers 52 (0.1%-1.2% vs 0.02%-1.0%). Artefill-induced nodules are mostly self-limited with a high treatment resolution rate.46,47 A specific site of fullness can be either from excess collagen stimulation (nodule) or a result of a chronic inflammatory reaction (granuloma). Histologic analysis is required to differentiate this diagnosis, although the treatment of each is identical. The initial 4 ART studies used for FDA approval revealed a cumulative granuloma rate of 1.2%.48-51
Data from a 12-year post-market surveillance (2007-2019), injecting 75 229 syringes reported 839 product-related adverse events (0.11%), some of those being nodule formation. 53 One study revealed 5 patients of 1645 injected with ART resulted in a nodule. Four of five of these nodules were completely resolved and one partially absorbed treating with combination 5-flurouracil and triamcinolone injection(s). 46
The study limitations were the retrospective design; however, patients were consecutive. Subjective patient reported outcome measures were used for patient satisfaction, but there were also objective brow elevation measurements. There was some error having patients remain in repose for photographs, since a degree of facial muscle contraction can alter the measured brow position. Also, camera straight view positioning may not be identical in before and after views.
Conclusion
Bellafill (ART) brow lift is a safe and effective minimally invasive procedure that uses no anesthesia (except synthetic ice) with microcannula filler administration reducing complications and side effects. The ideal candidate to attempt an ART brow lift is a patient with an isolated site of brow ptosis of mild severity. This technically simple procedure offers long-term brow lift results comparable to surgical therapy outcomes in selected patients.
Footnotes
Acknowledgements
The authors would like to acknowledge the practice team comprising Amy Stanley, Samantha Bustamante, and Yesenia Torres for their assistance in patient care, compiling data, and chart review. They would also like to acknowledge the librarians at Touro University Nevada for their assistance with interlibrary loans in the preparation of the manuscript and references.
Authors’ Note
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.