
Abstract
Informal caregivers play a vital role in supporting seriously ill patients. However, informal caregiving is burdensome and can lead to negative health outcomes for the caregiver and the care recipient. The study’s aim was to evaluate relationships among caregiver burden, care recipient depressive symptomology, and race. Guided by the social exchange perspective, we examined cross-sectional dyadic data from the National Long-Term Care Survey (N = 1279). Using ordinal logistic regression, we found that higher caregiver-reported objective burden was associated with higher care recipient depressive symptoms (P < .05), an association that was stronger for blacks. Interestingly, despite significant levels of objective burden, there was an association between lower depressive symptoms in black care recipients when there was an exchange of the social good “helpful company” with a caregiver. These findings illustrate the importance of supporting reciprocal exchange as a promising component of maintaining balanced caregiver–care recipient relationships among black older adults and their informal caregivers.
Understanding the complex relationship between informal family caregivers and care recipients is a key palliative care issue because many seriously ill older adults rely on informal caregivers. In 2015, there were approximately 34.2 million informal caregivers who spent an average of 24.1 hours providing unpaid help to an older adult. 1 Most informal caregivers are married, middle-aged, white women who do not hold a college degree and have a household income of less than US$50,000 per year. 1 Nearly half of the care recipients are parents or parents-in-law; 10% are spouses or partners. 1
Informal caregiving is physically, financially, and emotionally burdensome and can lead to negative mental and physical health outcomes for the caregiver. 2,3 Equally important are the potential consequences of these negative caregiver outcomes on the care recipient. 4 -6 Caregiver burden may not only negatively affect caregivers’ mental and physical health 2,7 but likely the quality of care recipients’ physical and mental health outcomes. 8,9 In particular, caregivers and seriously ill older adult care recipients are at high risk of depression. Depression is one of the most prevalent mood disorders among palliative care patients, and it is associated with impaired social functioning, reduced quality of life, poor prognosis, and higher mortality. 10 In the United States, 1% to 5% of noninstitutionalized older adults live with some form of depression. This estimate drastically increases to 11.5% of those who live in nursing homes and 13.5% for those who receive home health-care services. 11
The relationship between caregiver–care recipient depression and caregiver burden may be influenced by a variety of sociocultural factors, such as race, that can shape how caregivers respond to feelings of burden. Generally, compared to their whites counterparts, African American caregivers have fewer financial resources and provide more care to their care recipients but often report lower levels of burden, strain, and distress. 1,12,13 It is possible that African Americans’ strong familial obligations and coping mechanisms such as prayer may cause them not to see the caregiving relationship and burden in the same way as whites. 14 -16 The social exchange perspective (SEP) provides a lens to help untangle some of these complex factors to better understand how sociocultural factors such as race might influence the relationships among caregiver burden and care recipient depressive symptomatology.
Social Exchange Perspective
The SEP posits that social relationships are a series of costs and rewards. However, the caregiver–care recipient relationship is unique; unlike other social relationships, this relationship is inherently imbalanced because the care recipient is dependent on the caregiver. 2,17 -19 This control dependency relationship imbalance may be experienced by the caregiver as both subjective and objective burden (Figure 1) and by the care recipient as negative emotional response such as depressive symptoms. 20,21 The care recipient may try to reduce the power differential by exchanging goods with the caregiver. These goods may be physical (eg, help with chores), social (eg, providing helpful company), or psychological (eg, making the caregiver feel useful). In this study, we test how caregiver subjective and objective burden is associated with care recipient depressive symptoms and whether social exchange (including physical, social, and psychological exchange goods) moderates these factors.
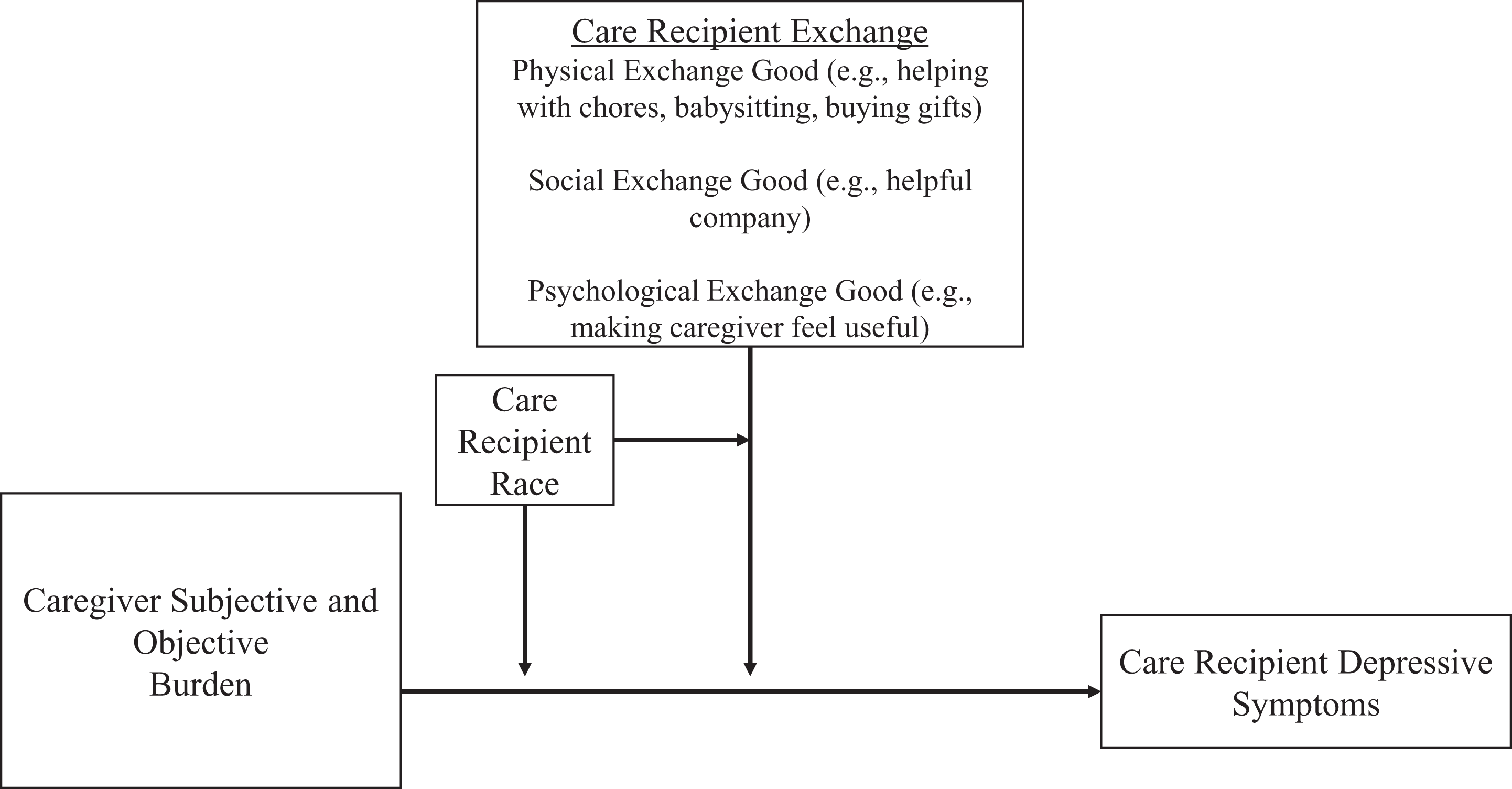
Model of associations between caregiver burden and care recipient depressive symptoms and the influence of care recipient exchange and race.
Social exchange among caregivers and care recipients may also be influenced by race. For blacks, informal caregiving is normative largely because of a historical background of oppression, racism, and limited resource availability. 14 As such, a care relationship in which resources are exchanged between caregivers and care recipients is common and can be quite beneficial. Thus, it is plausible that caregiver burden is less likely to be associated with depressive symptomology for black care recipients in the presence of exchange.
The purpose of this study was to evaluate the associations between caregiver subjective and objective burden, care recipient depressive symptomology, and exchange goods and to evaluate associations between caregiver burden, care recipient depressive symptoms, and care recipient race. We hypothesized that higher levels of caregiver subjective and objective burden would be associated with an increase in care recipient depressive symptoms (hypothesis 1). Second, we expected that any positive association between caregiver burden and care recipient depressive symptoms would be lower for black than for nonblack care recipients (hypothesis 2). Third, the exchange of physical, social, and psychological goods by the care recipient to the caregiver would be associated with a decrease in care recipient depressive symptoms (hypothesis 3). Finally, we hypothesized that any negative association between exchange goods and care recipient depressive symptoms would be greater for black than for nonblack care recipients (hypothesis 4).
Methods
Sample and Setting
We used the most recent wave of the National Long-Term Care Survey (NLTCS) to evaluate the associations between caregiver subjective and objective burden and the care recipient depressive symptoms. 22 The NLTCS is a nationally representative sample of physically disabled Medicare recipients aged 65 years or older living in the community or in formal institutions such as nursing homes and assisted living facilities. Our focus was on community-dwelling older adults. The institutional review board of University of Alabama at Birmingham approved this study (N140228001).
The NLTCS was administered through in-home and scheduled structured telephone interviews in which care recipients were asked about physical disabilities, medical conditions, recent hospitalizations, family support, activities of daily living (ADLs) and instrumental ADLs (IADLs), cognitive functioning, and the use of formal and informal caregiving. 22 Care recipients also provided information on all informal caregivers who assisted them. From the information provided by the care recipient, primary informal caregivers were identified and surveyed in a supplemental survey. An eligible caregiver was defined as one who provides unpaid help with at least 1 ADL or IADL for at least 1 hour in the week prior to participating in the National Informal Caregiver Survey (NICS). 23,24 When there was more than 1 individual who met the caregiver criteria, a primary caregiver was selected based on the individual who spent the most time providing help. 24 Caregivers were asked about the type of help that they provided for the care recipient (ie, objective burden), as well as questions on physical, emotional, and financial hardship to themselves (ie, subjective burden) caused by the caregiving relationship. 24
The initial 2004 wave of the NLTCS included a total of 20 474 respondents (note 1). For our sample, we used 4 inclusion criteria: first, the sample was restricted to care recipients who had a caregiver and whose caregivers responded to the NICS (n = 4272). Second, it included only care recipients whose caregiver received no remuneration for the care provided (n = 1837). Third, the sample was restricted to care recipients who did not have dementia or other related diseases (n = 1289). Finally, we only included care recipients who answered all 3 depression questions, resulting in an analytic sample of 1279 respondents.
Measures
Caregiver self-reported subjective and objective burden
Caregiver subjective burden and objective burden were the 2 focal independent variables. Caregiver self-reported subjective burden was measured by a modified version of the Zarit Burden Interview. 25 This study featured a 3-item scale in which respondents were asked about the emotional stress, financial strain, and physical hardship that they experience from being a caregiver. The caregiver was asked, “How emotionally stressful would you say that caring for [the care recipient] is for you? Response options were coded as not stressful at all (0), a little stressful (1), moderately stressful (2), pretty stressful (3), and very stressful (4). The caregiver was asked in the same manner about physical strain and financial hardship. Scale scores range from 0 to 12, with 0 representing no subjective burden and 12 representing high levels of subjective burden. The Cronbach α = 0.77 for this 3-item scale, suggesting acceptable internal consistency.
Caregiver self-reported objective burden was measured by a modified version of the Screen for Caregiver Burden (SCB) Index. 26 The original SCB is a 25-item scale used to evaluate the occurrence of stressful events of caregiving and the severity of distress suffered by the caregiver. 26,27 The scale in the NLTCS contains a modified 15-item version that does not include the measures of caregiver distress. In this survey, respondents were asked how many times in the past week they were tasked with dealing with behavioral issues of the care recipient. For example, caregivers were asked, “In the past week, on how many days did you personally have to deal with the following behavior of [the care recipient]? How many days did [he/she] keep you up at night?” Possible response options include no days (coded as 0), 1 to 2 days (1), 3 to 4 days (2), and 5 or more days (3). Scores range from 0 to 45. A score of 0 represents no objective burden and 45 represents high objective burden (Cronbach α = 0.81).
Care recipient depressive symptoms
Care recipient depressive symptomology, the outcome of interest, was measured by an abbreviated version of the Center for Epidemiologic Studies–Depression (CES-D) Scale provided in the NLTCS. This is a 3-item scale in which the respondents were asked questions about recent depressed mood. The older adult care recipient respondent was asked: “During the last 2 weeks, have you felt so sad, blue, or depressed that you (1) did not feel like doing things you usually do, (2) could not sleep like you usually do, and (3) lost your appetite or could not eat like you usually do?” The responses were yes (1) and no (0) on each of the 3 questions. The scores were then summed, and the scale ranged from 0 to 3, with 0 representing no depressive symptoms and 3 representing 3 depressive symptoms (Cronbach α= 0.71).
Physical, social, and psychological exchange goods
The SEP involves the exchange of physical, social, and psychological goods. These 3 types of goods were measured by proxy measures in the NICS in which caregivers were asked about resources provided to them by the care recipient. For physical exchange goods, the caregivers were asked whether the care recipient helped with household chores, babysitting, or buying them things and giving them money. If the caregiver reported receiving none of the 3, they were scored 0. If the caregiver reported receiving any 1 of the 3, they were scored 1. Social exchange goods were measured by asking the caregiver whether the care recipient ever provided “helpful company” to them. Possible response options were no (0) and yes (1). To measure psychological goods, the caregivers were asked whether the care recipient had made them feel useful and needed. Possible response options were also no (0) and yes (1).
Sociodemographic and health-related covariates
Sociodemographic covariates included the care recipient age, race, caregiver and care recipient gender, education level, and caregiver relationship to care recipient (eg, spouse, child). Health-related covariates included care recipients’ self-rated health (ordinal measure ranging from poor health = 1 to excellent health = 4), cognitive function (measured using the Short Portable Mental Status Questionnaire), 28 and functional limitations (measured with the index of independence in ADLs 29 and the IADL scale 30 ).
Statistical Analysis
All analyses were conducted using SPSS (version 23.0; SPSS Inc, Chicago, Illinois). Continuous variables were summarized using means and standard deviations (SDs). Categorical variables were described with frequencies and percentages. To analyze the relationships between caregiver burden and care recipient depressive symptoms, we used ordinal logistic regression models. The outcome variable (care recipient depressive symptoms) was regressed on each of the focal independent variables (subjective and objective burden) along with the sociodemographic and health-related covariates. Sociodemographic and health-related covariates were included in the models as potential confounders of the relationship between caregiver burden and care recipient depressive symptoms. The conditional effects of race on the relationship between caregiver burden and care recipient depressive symptoms were assessed using interaction terms of race by subjective and objective caregiver burden.
In the second analysis, we examined the extent to which physical, social, and psychological exchange goods were associated with care recipient depressive symptoms net of caregiver burden, as indicated by the SEP. Physical, social, and psychological exchange goods are distinctly different dimensions of the SEP 21,31,32 and were each analyzed separately. Again, using ordinal logistic regression models, we regressed care recipient depressive symptoms on subjective and objective caregiver burden, sociodemographic and health-related covariates, and exchange good measures. We also evaluated the extent to which any effects of physical, social, and psychological exchange goods were conditional on the race of the care recipient by including interaction terms of race by each of the social exchange goods.
Given the racial differences in the care recipients’ demographic and sociodemographic characteristics, we conducted sensitivity analyses that included interaction terms with age, sex, education, and relationship of caregiver by each of the measures of caregiver burden and social exchange. We found no statistically significant changes that altered our original conclusions.
Results
Sample Characteristics
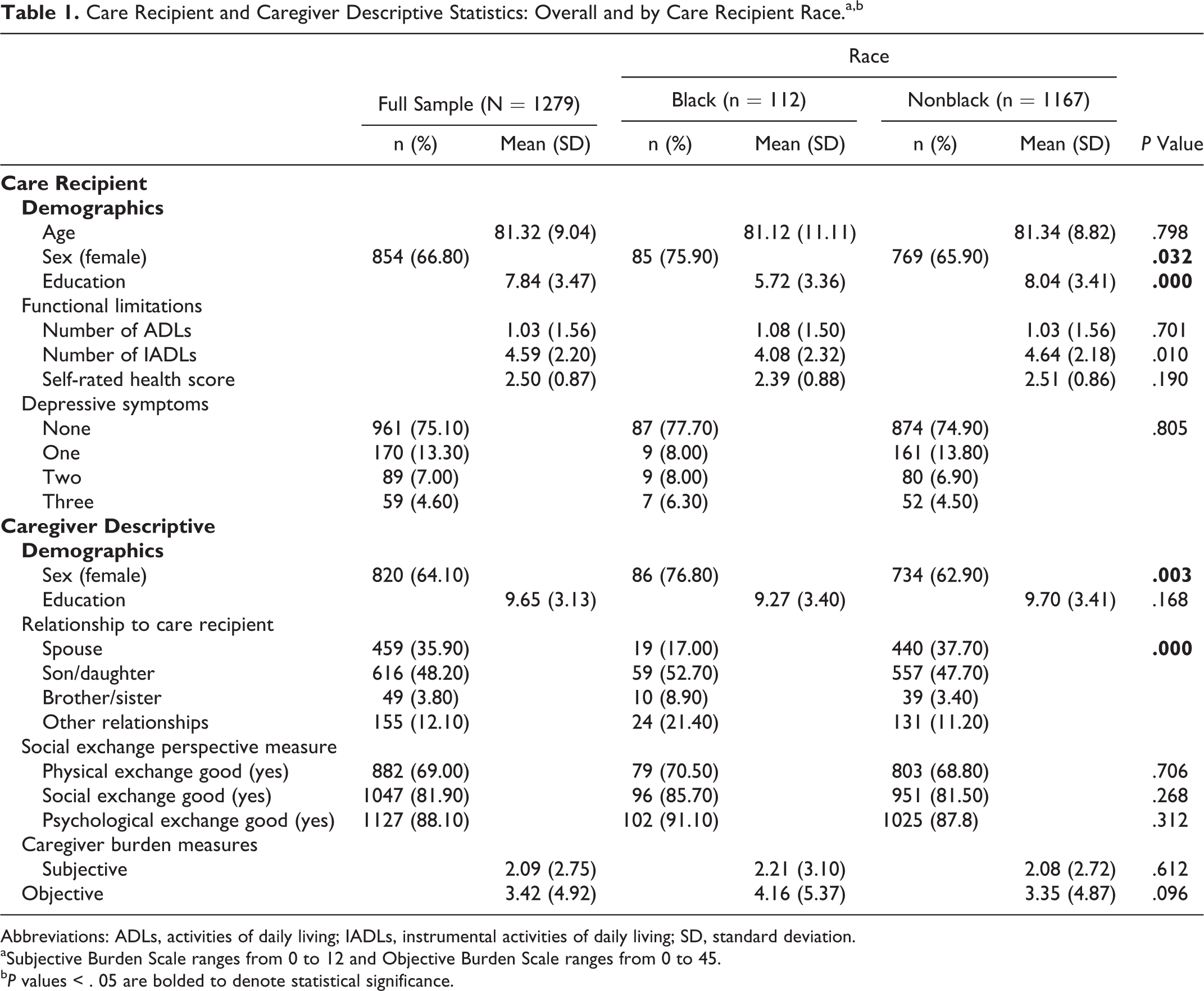
Table 1 provides care recipient and caregiver descriptive statistics overall (N = 1279) and by care recipient race (nonblack = 1167; black = 112). Overall, care recipients’ average age was 81.32 ± 9.04 years and most were female (66.8%). The average education for blacks was ninth grade (5.72 ± 3.36) and for nonblacks was high school diploma or General Equivalency Diploma (GED) (9.70 ± 3.41). Mean ADL and IADL self-rated scores were similar for the full sample and by race. Care recipients reported fewer ADLs (1.03 ± 1.56 on a 7-point scale for the full sample, 1.08 ± 1.50 for blacks, and 1.03 ± 1.56 for nonblacks) compared to IADLs (4.59 ± 2.20 on a 7-point scale for the full sample, 4.08 ± 2.32 for blacks, and 4.64 ± 2.18 for nonblacks). Care recipients also reported good to very good health (2.50 ± 0.87, full sample; 2.39 ± 0.88, blacks; 2.51 ± 0.86, nonblacks). Most (75.1%) of the care recipients reported no depressive symptoms. By race, 77.7% of blacks and 74.9% of nonblacks reported no depressive symptoms.
Care Recipient and Caregiver Descriptive Statistics: Overall and by Care Recipient Race.a,b
Abbreviations: ADLs, activities of daily living; IADLs, instrumental activities of daily living; SD, standard deviation.
aSubjective Burden Scale ranges from 0 to 12 and Objective Burden Scale ranges from 0 to 45.
b P values < . 05 are bolded to denote statistical significance.
The average subjective caregiver burden score was similar for the full sample and by race (2.09 ± 2.75 on a 12-point scale, full sample; 2.21 ± 3.10, caregivers of black care recipients; 2.08 ± 2.72, caregivers of nonblack care recipients). The average objective caregiver burden score differed by race, however. The mean objective burden score was higher for caregivers of black care recipients (4.16 ± 5.37 on a 45-point scale) than for caregivers of nonblack care recipients (3.35 ± 4.87). Most caregivers reported that they did receive physical, social, and psychological goods from the care recipient.
Associations of Caregiver Burden, Care Recipient Depression, and Race
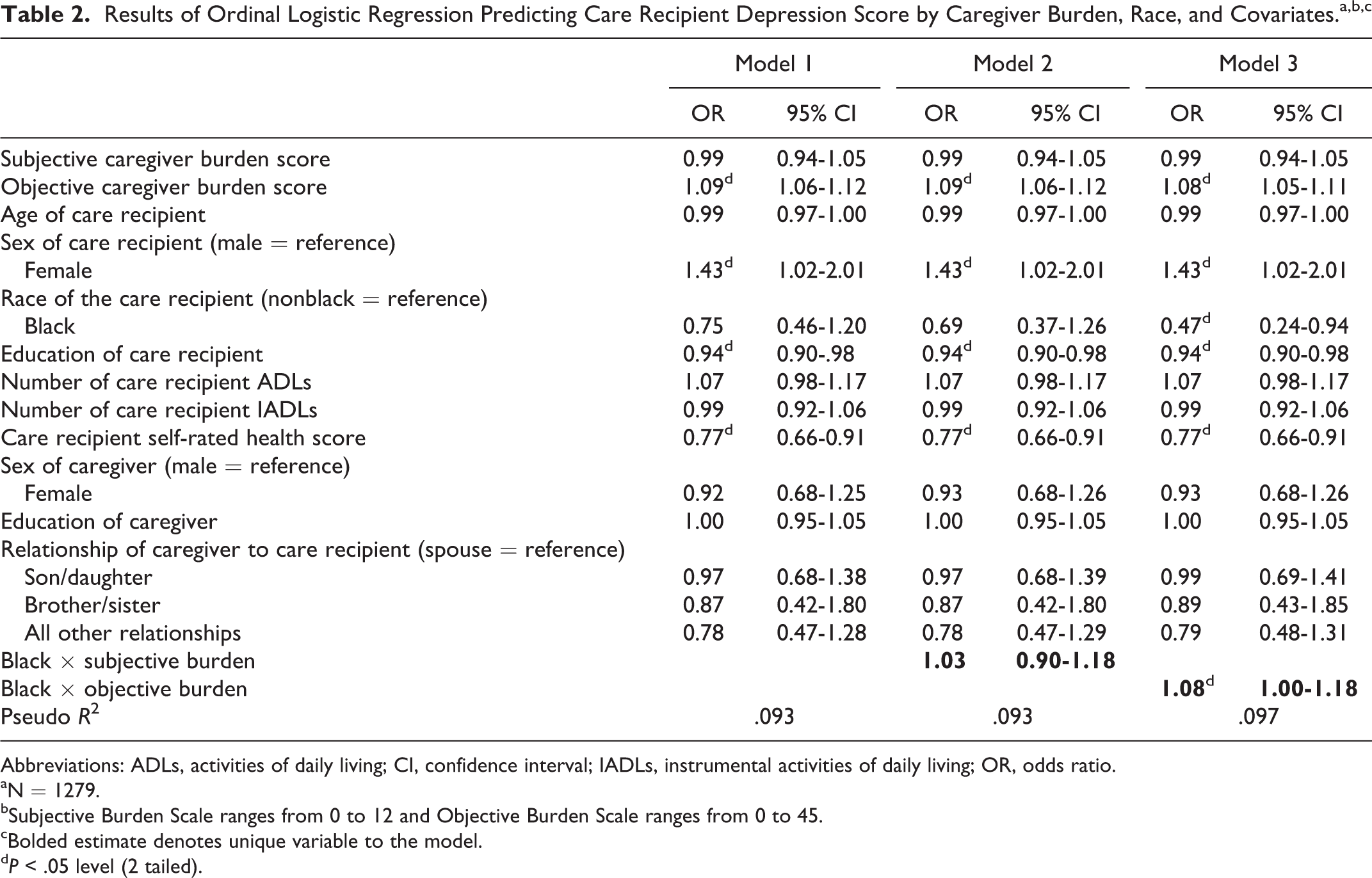
Table 2 reports odds ratios for a series of models predicting care recipient depressive symptoms. In model 1, we regressed care recipient depressive symptoms on subjective and objective care burden score and descriptive variables. Care recipient depressive symptoms were associated with objective but not subjective caregiver burden. This partially supports our first hypothesis that states that higher levels of caregiver subjective and objective burden would be associated with an increase in care recipient depressive symptoms. Care recipients who reported better health and who had higher levels of education were more likely to report fewer depressive symptoms. Female care recipients were more likely to report depressive symptoms compared to men.
Results of Ordinal Logistic Regression Predicting Care Recipient Depression Score by Caregiver Burden, Race, and Covariates.a,b,c
Abbreviations: ADLs, activities of daily living; CI, confidence interval; IADLs, instrumental activities of daily living; OR, odds ratio.
aN = 1279.
bSubjective Burden Scale ranges from 0 to 12 and Objective Burden Scale ranges from 0 to 45.
cBolded estimate denotes unique variable to the model.
d P < .05 level (2 tailed).
Model 2 introduces the interaction term of race by subjective burden, along with subjective and objective burden score and descriptive variables as in model 1. Model 3 includes the interaction term of race by objective burden, subjective and objective burden score, and descriptive variables. The significant positive interaction term for objective burden indicates that objective burden has a greater association with the odds of increasing depressive symptoms for blacks than for nonblacks. This contradicts our second hypothesis that caregiver burden would have a lower association with the odds of reporting depressive symptoms for blacks than for nonblacks.
Associations of Caregiver Burden, Care Recipient Depression, Social Exchange Measures, and Race
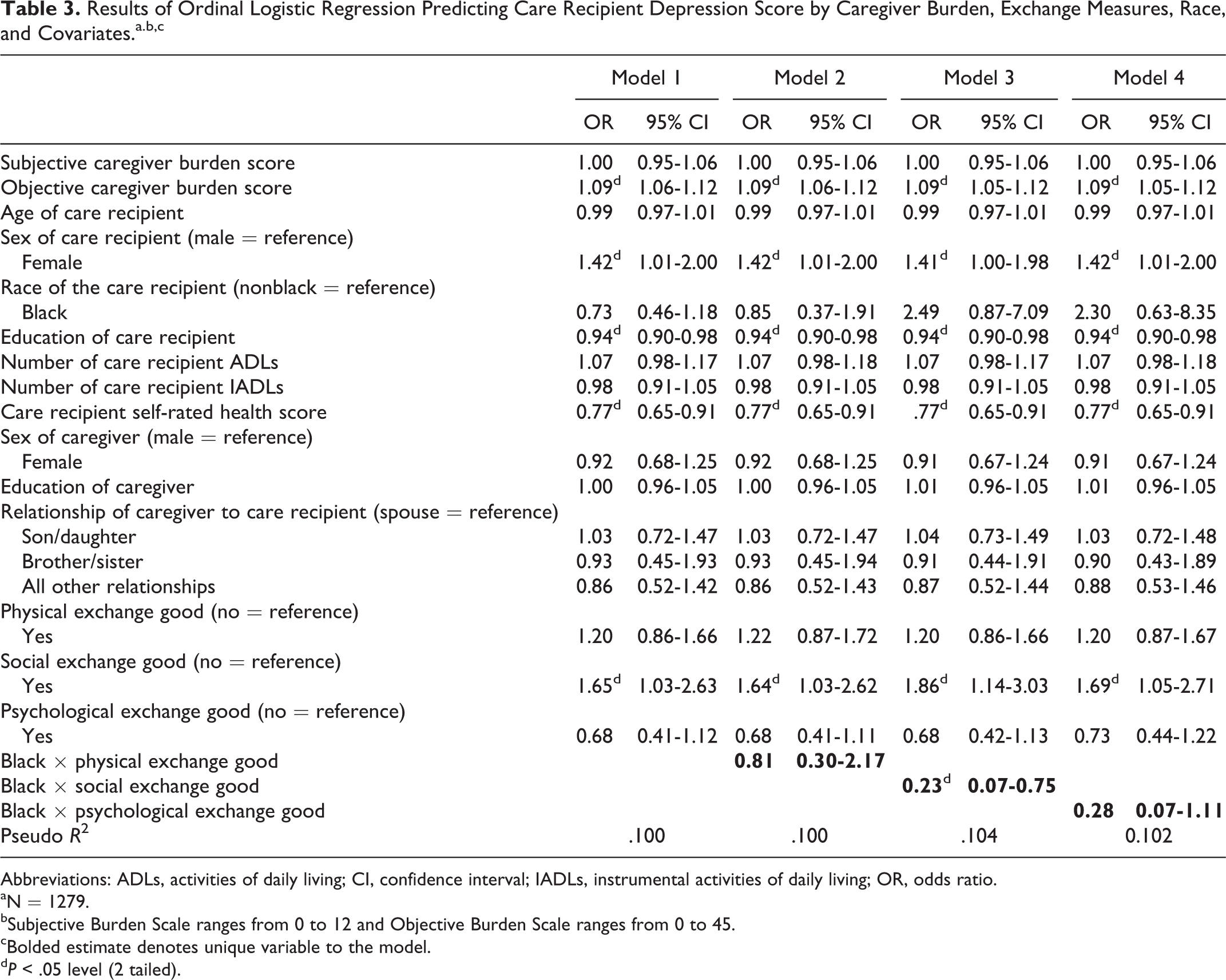
The next objective of this study was to analyze the relationships between exchange goods and care recipient depressive symptoms net of caregiver burden. Table 3 reports odds ratios for models that introduce the exchange measures into the analysis. In model 1, we regressed care recipient depressive symptoms on subjective and objective caregiver burden score, descriptive variables, and social exchange measures. We found that exchanging the social good of “helpful company” has a positive association with care recipient depressive symptoms, which partially contradicts hypothesis 3 that states that the exchange of exchange goods would be associated with a decrease in depressive symptoms. We note that including the exchange measures in the model did not alter the relationships between care recipient depressive symptoms and objective caregiver burden, care recipient health, care recipient educational attainment, sex, and race noted above.
Results of Ordinal Logistic Regression Predicting Care Recipient Depression Score by Caregiver Burden, Exchange Measures, Race, and Covariates.a.b,c
Abbreviations: ADLs, activities of daily living; CI, confidence interval; IADLs, instrumental activities of daily living; OR, odds ratio.
aN = 1279.
bSubjective Burden Scale ranges from 0 to 12 and Objective Burden Scale ranges from 0 to 45.
cBolded estimate denotes unique variable to the model.
d P < .05 level (2 tailed).
Model 2 introduces the interaction term of race by physical exchange, along with subjective and objective caregiver burden score, descriptive variables, and social exchange measures as in model 1. Model 3 includes the interaction term of race by social exchange, subjective and objective caregiver burden score, descriptive variables, and social exchange measures. Last, model 4 includes the interaction term of race by psychological exchange, subjective and objective caregiver burden score, descriptive variables, and social exchange measures. We found a statistically significant interaction for the social good of providing “helpful company” that indicates that for blacks, care recipients having exchanged the social good of “helpful company” with his/her caregiver substantially reduced the care recipients’ odds of reporting depressive symptoms. This is consistent with hypothesis 4 and suggests that exchanging the social good of “helpful company” is associated with an increased likelihood of reporting depressive symptoms for nonblacks.
Discussion
Using a nationally representative survey, this study attempted to untangle the complex relationship between caregiver burden and care recipient depression by examining factors (social exchange and race) that may have a positive or negative impact on that relationship. We found that greater caregiver objective burden levels (eg, increased time spent up at night taking care of the care recipient, dealing with a bowel or bladder accident) were associated with an increased odds of care recipients reporting more depressive symptoms. In contrast, subjective burden was not associated with care recipient depressive symptoms. We then examined whether social exchange and race impacted this relationship. We found that although the exchange of psychological and physical goods (eg, making the caregiver feel useful and needed, helping with household chores) did not vary by race, the exchange of the social good of “helpful company” substantially reduced the odds of blacks reporting more depressive symptoms. These findings suggest that black care recipients benefit by exchanging helpful company with their caregiver in efforts to bring balance to the care relationship, thus reducing “social burden.”
Because blacks have an earlier onset of chronic diseases, it is likely that black care recipients receive informal care much longer than their nonblack counterparts. 31 As a result, blacks may have a longer period over which to satisfy the norm of reciprocity and equalize the exchange by providing helpful company as a way to give back. The finding that social good exchange reduces care recipients depressive symptoms suggests that clinicians might consider reinforcing this by reminding these seriously ill black care recipients that even though they are not able to provide help with tasks such as household chores, their presence may be seen as valuable “helpful or supportive company” to their family. For example, helpful company can come in the form of providing wisdom to and company for their caregivers.
Surprisingly, exchanging helpful company did not hold true for nonblack care recipients; nonblack care recipients had an increased odds of reporting depressive symptoms in the presence of social exchange. This finding supports the potentially positive cultural impact of race on the caregiver–care recipient relationship. 32 It is possible that there is a greater acceptance of interdependency within black family life. Whereas nonblack care recipients may find exchange goods not a strong enough value to overcome dependency.
Limitations and Future Directions
Guided by the SEP, we used a nationally representative sample to examine the buffering effects of exchanging goods on the relationship between caregiver objective and subjective burden and care recipient depressive symptoms. Research in this area has primarily focused on unidirectional giving, with the caregiver providing help to the care recipient. 33 -36 Hence, this study sheds light on the effect of bidirectional exchange between caregivers and care recipients.
However, as in any secondary analysis of an existing data set, there are a number of study limitations. First, the data are over 10 years old. We should bear in mind that more recent older adult cohorts may have less illness and disability in older age, compared to their older counterparts. 37 Thus, today’s care recipients may not be as ill as those in the data set. Second, the NLTCS data do not measure depressive symptoms of caregivers and include only a limited measure of care recipient depressive symptoms (i.e., 3 items of the CES-D scale). This scale, however, has been used in previously published studies. 38 Fourth, the NLTCS does not stratify its sample by race and does not provide the race of the caregiver, and as a result, we were not able to analyze any effects that racial discordance among dyads may have had on predicting care recipient depressive symptoms.
Further, the NLTCS includes only a 3-item scale to measure subjective burden. This measure may not have been robust enough to evaluate the complex concept of subjective burden. We are mindful that measures of exchange are subjective. This may differ from the actual goods that caregivers were provided by the care recipients or care given to the care recipient by the caregiver. However, having a data set that measures exchange goods and burden among caregiver–care recipient dyads provided a unique opportunity to test the theory of social exchange. Also, the study relied on cross-sectional data and we cannot rule out the possibility of reverse causality (i.e., that care recipient depression is a source of caregiver burden). This is a challenging issue to address because of the high levels of attrition with longitudinal data among older respondents. Nonetheless, future researchers should explore alternative research designs or collect longitudinal data at more frequent intervals than the NLTCS to help address potential reverse causality.
Conclusion
Findings from this study contribute to the literature in illustrating the importance of reciprocal exchange in maintaining balanced caregiver–care recipient relationships among seriously ill African American older adults and their informal caregivers. In addition, the finding that exchange was not helpful in reducing depressive symptoms for nonblack care recipients reveals an area for further research. Given the complexity of the relationship among care recipients and their informal caregivers, longitudinal mixed methods studies would be helpful to investigate caregiver burden’s effects on the mental health of chronically ill older adult care recipients over time. Qualitative researchers should elicit care recipients’ perspective on the meaning of dependency and how it affects their relationship with their family caregivers. Future research could also further explore the concept “helpful company” since it was found to be associated with fewer depressive symptoms among African American care recipients. We also found that despite the presence of exchange, caregivers still experience objective burden associated with their caregiving roles. This highlights the need for interventions that support family members in their roles as caregivers and promotion of self-care behaviors that improve mental health outcomes among this group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Alabama at Birmingham Comprehensive Minority Faculty and Student Development Program (CMFSDP) Fellowship and the NIH/NINR (3R01NR03665-02S1).