
Abstract
Introduction:
Goals of care (GoC) conversations optimally begin early in the course of cancer care, yet most happen near the end of life. We sought to describe oncologist-reported facilitators of and barriers to GoC conversations with patients who have advanced cancer.
Methods and Materials:
We conducted individual, semistructured qualitative interviews with oncologists from 4 academic, community, municipal, and rural hospitals in New York and Connecticut. Interview topics included approach to GoC conversations, facilitators, barriers, and organizational influences. We analyzed data using interpretive description. We collected demographic and practice information and surveyed oncologists on their communication skills training. We calculated descriptive statistics for quantitative data.
Results:
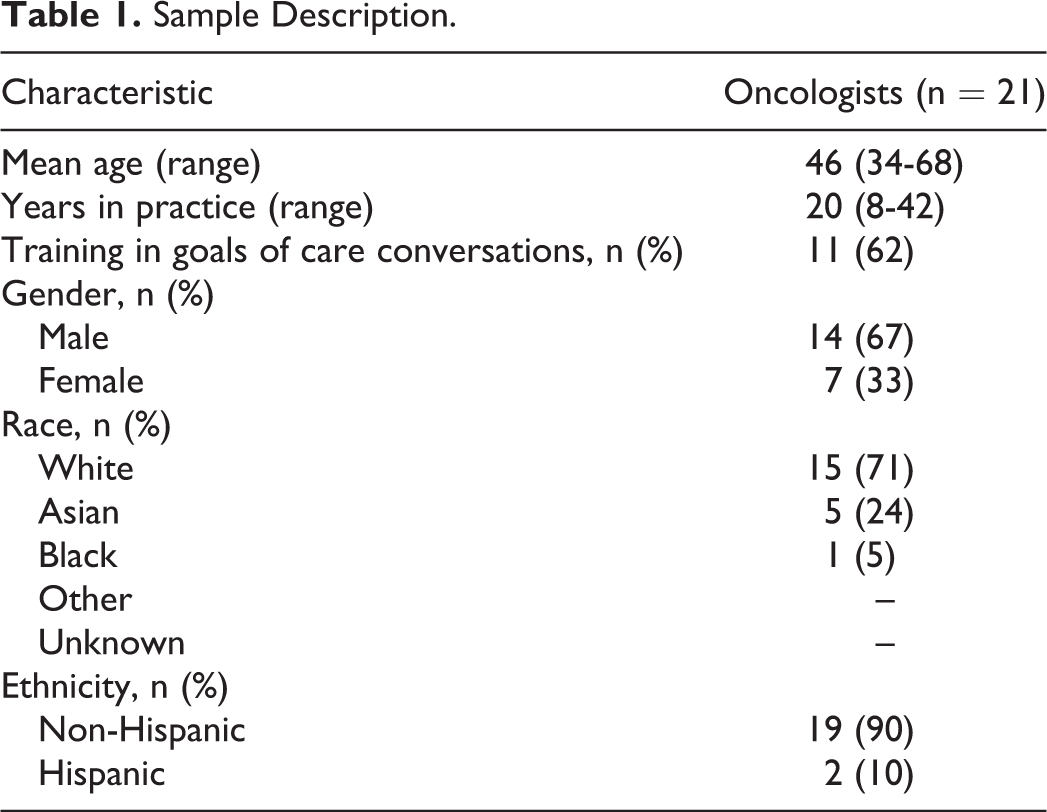
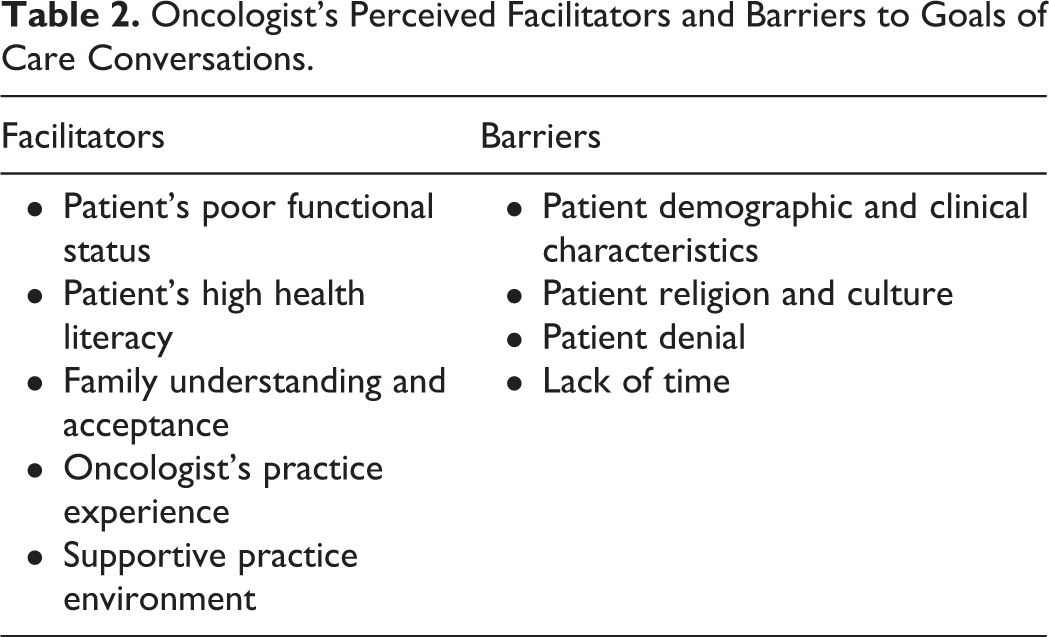
Oncologists (n = 21) had a mean age of 46 years (range: 34-68), 67% were male, 71% were White, 24% were Asian, 10% were Hispanic, and 5% were Black. They reported an average of 20 years in practice (range: 8-42), and 62% had received training on having GoC conversations. Facilitators included patient’s poor functional status, patient’s high health literacy, family understanding and acceptance, oncologist’s practice experience, and a supportive practice environment. Barriers included certain patient demographic and clinical characteristics, patient religion and culture, patient’s denial, and lack of time.
Conclusion:
GoC conversations may be facilitated by enabling oncologists to conduct these conversations despite difficult circumstances and emotional reactions by activating patients and family via increased health literacy and by advancing palliative-informed practice environments.
Introduction
The American Society of Clinical Oncology Consensus Guideline Summary on Patient-Clinician Communication offers recommendations to clinicians on how and when to conduct goals of care (GoC) conversations as well as what should be discussed. Recommendations include clarifying treatment goals so that patients can relate goals of treatment to their GoC, reassessing GoC when significant changes in the care plan are being considered, and initiating GoC conversations with involvement of family caregivers early in the course of care. 1 GoC conversations have been shown to assist patients and family members with their goals, to improve healthcare utilization, and to enhance quality of life. 2 –4 Yet, most GoC conversations happen near the very end of life, 5,6 inhibiting maximum utility. We sought to describe oncologists’ perspectives on facilitators of and barriers to GoC conversations with patients with advanced cancer.
Methods
Sample
We conducted individual, semi-structured, qualitative interviews with oncologists at 4 hospitals and community clinics in New York and Connecticut. Study sites represented academic, community, municipal, and rural settings. The institutional review boards of participating institutions approved this study. Eligible participants were solid tumor attending oncologists at the enrollment sites who saw at least 2 new patients with advanced cancer per month. We defined patients with advanced cancer as those who had a cancer associated with a life expectancy of less than 2 years. We invited all solid tumor oncologists at all sites to participate.
Procedures
Interviewers obtained oncologists’ signed consent. Interviews, which were digitally recorded and professionally transcribed, were conducted by experienced interviewers (J.J.L., S.F., C.B.S., D.S.-G.) at oncologists’ practice sites. The interview guide covered oncologists’ approach to GoC conversations, facilitators, and barriers to having these conversations and organizational influences on GoC conversations. In this article, we report on oncologists’ responses to the question, “What are some of the things that have made it harder/easier for you to have a goals of care conversation?” We report findings on other interview content elsewhere. 7,8 We continued interviewing until we achieved data saturation. We asked oncologists to complete demographic/practice information forms.
Data Analysis
In undertaking this study, we used the qualitative approach of interpretive description. 9 This approach is appropriate for studies focusing on human health and illness experiences and aiming to inform clinical reasoning and practice decisions. We used Atlas.ti qualitative software (version 5.0; Scientific Software, Berlin, Germany) to manage the data. The coding team (J.J.L., S.F., C.B.S., D.S.-G.) began with line-by-line review of transcripts and open coding of data with descriptive phrases to identify key concepts. Following review of the first 3 transcripts, coders developed an initial code key, which was then expanded and refined through independent and then joint review of subsequent transcripts. Coders compared codes until they achieved agreement on all codes, code meanings, and conceptual categories. We applied the final code key to all transcripts, produced code reports, and analyzed reports to identify facilitators and barriers to GoC conversations. Coders created memos to capture thoughts and questions about the data throughout the analytic process. Coders discussed memos and the data with the full study team, which included oncologists, patient stakeholders, and representatives of cancer advocacy organizations.
Results
Sample Description
Eighty-eight percent of invited oncologists (n = 21; Table 1) participated in interviews, which lasted an average of 34 minutes (range: 15-48). Oncologists cared for patients who were 59% female, 41% White, 38% African American, 3% Asian, 18% other/unreported, with various cancer diagnoses (ie, lung, breast, colon, pancreatic, prostate, renal cell, thymoma, appendiceal, biliary, esophageal, gastric, head/neck, tongue, and glioblastoma). 7,8
Sample Description.
Perceived Facilitators and Barriers
Oncologists reported several facilitators and barriers to GoC conversations (Table 2) in response to questions on what made it harder or easier to have a GoC conversation.
Oncologist’s Perceived Facilitators and Barriers to Goals of Care Conversations.
Facilitators
Oncologists perceived 5 facilitators of GoC conversations: patient’s poor functional status, patient’s high health literacy, family understanding and acceptance, oncologist’s practice experience, and a supportive practice environment.
Patient’s poor functional status
Functional status was reported as affecting GoC conversations where having poor functional status prompted the conversation. Oncologists reported observing patients’ functional status over time to gauge the timing of the GoC conversation. An oncologist explained, “If they still theoretically have 2 or 3 more options but they’re increasingly more debilitated, that would be a time when I bring it up…”
Having a GoC conversation was seen as easier when there was congruence between patients’ functional status and prognosis. An oncologist described: [With some] patients, there’s oftentimes a discrepancy in the burden of disease that the patient has and the way the patient feels, meaning they feel great, but they have cancer everywhere. So they say, “Wait a second. I just walked in here. I just did my bike ride. You’re telling me that we have to have a goals of care discussion?”
Patient’s high health literacy
Oncologists found it easier to engage in GoC conversations with patients who were more health literate (ie, more knowledgeable about their health condition), were active managers of their health, and were direct in their health communication. An oncologist stated, What facilitates it is having an active participant, somebody who is willing to articulate what their concerns or uncertainties are, what they want, what they’re hoping to get out of it, and also someone who’s willing to listen. Some patients have been really sick for months. Even though it’s a new diagnosis, they kind of have an idea that they’re not doing really well, and so they’re ready and willing to hear that conversation.
The ideal facilitator of a GoC conversation was described as a patient with a balance of health literacy and proactivity.
Family understanding and acceptance
Having family members with a clear understanding of the patient’s health condition facilitated GoC conversations. Oncologists described such family members as having realistic expectations, asking for more information to make treatment decisions, initiating discussions about stopping treatment, or talking about saying goodbye to the patient. Agreement among family members about GoC likewise facilitated the GoC conversation.
Another facilitator was family acceptance of the patient’s health condition and prognosis. Families were described as being readier for a GoC conversation when they saw the patient was suffering and/or declining. Oncologists described the need to discuss GoC with family members so they would feel that the patient had been well cared for. An oncologist explained, Easier is when the patient and family members want information so they can make their ultimate decisions, and once again, these are people who have accepted what their diagnosis and prognosis is.
Oncologist’s practice experience
Having more practice experience facilitated GoC conversations. Some oncologists reported that seeing palliative care specialists have GoC conversations helped them learn communication strategies. Watching poorly conducted GoC conversations was likewise a learning experience: I watched people that I respected give bad news and try to emulate them and I watched people that I didn’t respect or didn’t agree with how they gave bad news and I tried not to emulate them. Through trial and error you learn what’s a good way to say something, because you don’t want to scare patients needlessly and create undue anxiety, but you also want to make sure you say what you need to say. I think I’ve learned…when I can challenge a family with unrealistic expectations, and how to do it better without being confrontational. It’s not easy to tell a patient or a family, you know, your loved one or you have weeks to live, or yes, you qualify for hospice because your life expectancy is under 6 months. Those are not easy things to say…you have to dissociate because…people don’t want their doctors to be emotional wrecks…they look to you for guidance. Everyone is different. Some people don’t like empathetic discussions of bad news. Some patients don’t like it. They don’t want euphemisms…they like when people just say, “Sir, you are going to die. Get your house in order…everything is going to happen quickly.” Some people respect that because they are like that.
Supportive practice environment
A supportive practice environment was described as having a large and/or strong palliative care service that encouraged early discussions, supported symptom management, helped to set expectations, conducted family meetings, modeled appropriate language, supported a close-knit supportive team, and enabled a multidisciplinary approach. An oncologist stated: “Having goals of care discussions with the palliative care team involved has helped to give me a vocabulary to use in talking about difficult things.”
Some oncologists described feeling freer to conduct GoC conversations within a supportive environment where the institution did not dictate what they should discuss when: “You don’t feel like somebody’s hovering over you when you’re having a discussion or judging you…I think that’s positive.”
Oncologists who did not have a palliative care team reported relying more on other team members to help with GoC conversations. They perceived a benefit to partnering with others to support patients: “When patients start to hear from multiple people in the same way, I think it’s very, very helpful.”
Barriers
Oncologists perceived 4 barriers to GoC conversations: patient demographic and clinical characteristics, patient religion and culture, patient denial, and time.
Patient demographic and clinical characteristics
Oncologists reported several demographic and clinical characteristics that they felt made having GoC conversations more challenging. Demographic characteristics that made GoC conversations difficult included younger patient age or patients having young children, which made conversations more emotionally challenging, lower educational attainment, which made it potentially more difficult for patients to understand their health condition and treatment options, and high socioeconomic status, which could be accompanied by a sense of entitlement. Language barriers were cited due to the difficulties of arranging and speaking through a translator about complex and emotional topics.
Clinically, patients with cognitive deficits or mental illness were seen as more difficult due to their potential inability to engage in a GoC conversation. Having a newly diagnosed patient was a barrier for 2 reasons. Oncologists felt the GoC conversation would be overwhelming for the patient and lack of time to get to GoC in the first visit: “Somebody who…might have advanced disease but [is] just starting out with treatment. I don’t think that patient is ready yet.”
Patient religion and culture
A common barrier to GoC conversations was patients’ religion and/or culture. While religion was often reported as a source of patients’ comfort or acceptance of the health condition, religion was a barrier when it was used to support denial about cancer progression or to support “unlimited intervention at the end of life”: When it’s [religion] being used to support continued denial, I find that difficult. It’s hard to overcome. I try to address it and be respectful about it, but I will say it’s a source of frustration…when people are saying “My belief, what I believe in, will take care of me.”
Patient denial
A significant barrier to having GoC conversations was patients’ denial of their diagnosis or prognosis. Oncologists described denial as having unrealistic expectations, such as expecting to be cured when they had incurable disease, or having strong religious beliefs, for example, “God will save me.” A participant stated, “It’s one thing to fight, that’s okay. It’s another thing to absolutely refuse to deal with what has happened.”
Less strong than denial, oncologists also described patients not being ready for a GoC conversation. Indicators of not being ready included the patient wanting to maintain complete control of their treatment plan, having survived another cancer, and when the patient did not want to live with the knowledge that they were dying. Several oncologists expressed difficulty having the GoC conversation with patients who were in denial or not ready, describing these situations as frustrating, difficult, uncomfortable, challenging, and unhappy. A participant reported, “[you] feel a responsibility to help them get there [acceptance of prognosis], even though you can see they’re not going to get there.”
Consequences of denial or not being ready were that they impeded patients’ ability to engage in various aspects of a GoC conversation, such as weighing treatment options or accepting the absence of active treatment options, involving family or other healthcare professionals in the conversation, or being able to ask questions.
Time
Time was perhaps the greatest and most often mentioned barrier to GoC conversations, particularly in the ambulatory setting. Oncologists estimated GoC conversations to take 30 to 60 minutes on average, but as much as 90 minutes. An oncologist detailed: I think it’s almost impossible to have a conversation…with a new patient, [about] your disease, your stage, your prognosis, management, consent, and then goals of care at the same time…we have 15 minutes to see each patient, so I don’t think that’s possible.
Conclusion
Facilitators and barriers to oncologists’ engaging patients with advanced cancer in GoC conversations clustered around oncologists, patients, families, and the practice environment. Our findings are like other qualitative and quantitative studies on oncologists’ experiences of GoC conversations in which unrealistic patient or family expectations, lack of time, and composition of the palliative care team have been reported. 10 –12 Although our data, collected at 4 northeastern hospitals, may have limited generalizability, our data reflect other reports from Canada and Korea, suggesting universal themes and challenges across cultures, religions, and countries. The similarities across settings also speak to the inherent challenges of initiating GoC conversations in addition to potential system-level “fixes.” While some of our findings reflect seemingly unshakeable issues in GoC communication, our data are notable because they derive from oncologists serving diverse populations in diverse settings. Our study also elucidates the importance of recognizing differing patient cues and family values across populations and highlights the imperative of tailoring oncologists’ training to correctly identify varying cues and approaches to initiate GoC conversations among diverse populations.
The short time frame in which GoC conversations should be introduced (within 8 weeks of diagnosis) and during which they happen (within 15-minute appointments at times) make it critical to recognize facilitators and, more importantly, barriers to having these conversations. For example, the barrier of the patient “not being ready” may actually reflect oncologists’ ability or willingness to adjust to patients’ preferences and engage them in GoC conversations. The challenge is supporting oncologists in having GoC conversations wherein oncologists can identify ways to help “not ready” patients toward a better understanding of realistic GoC, or whatever being “ready” means for patients. As another example, it is worth revisiting the oft-cited barrier of time. How accurate the perception is of time demands for GoC conversations remains to be seen. This barrier may be lessened if GoC conversations begin early in the disease course and are ongoing. GoC conversations must be modified based on the changing nature of the disease. Enabling oncologists to have GoC conversations as comfortably and efficiently as possible is of high importance.
Initiatives may be implemented to support facilitators and address barriers. Oncologist-reported common elements to clear GoC communication include the belief that conversations are a process, a sense of responsibility for making recommendations, using an individualized approach, and use of experimentation, reflection, and role models. 13 Communications skills training has been shown to improve oncologists’ communication skills and self-efficacy. 14 Programs such as VitalTalk 15 offer educational and practice opportunities. Patients and family members may also benefit from educational opportunities that increase health literacy and self-efficacy by enhancing their knowledge of palliative care and their role in GoC conversations. Interventions such as ENABLE 16 and Managing Cancer Care 17 have been shown to be effective in these areas.
In addition, efforts must continue to advance palliative-informed practice environments. While 90% of large hospitals (300+ beds) in the United States offer palliative care, 18 presence of a palliative care service is not enough. There must also be culture change in the form of buy-in among oncologists and other health-care professionals who are in the position of making referrals to and/or working with palliative care specialists. GoC conversations are inherently challenging but can be made manageable by responding to oncologists’ reports of their lived experiences having them.
Footnotes
Authors’ Note
All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors, or Methodology Committee. This work was presented as a poster at the Annual Assembly of the American Academy of Hospice and Palliative Medicine, Chicago, Illinois, March 2016 (Dena Schulman-Green, Cardinale B. Smith, Jenny J. Lin, Shelli Feder, and Nina A. Bickell. What helps and hinders oncologists from conducting goals of care conversations?)
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bickell discloses work with Pfizer. Dr Schulman-Green discloses work with Genentech.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Award (#IHS-1310-06444).