
Abstract
Purpose:
The objective of this pilot study is to evaluate the (1) applicability of a 15-hour attending-taught psychoeducational intervention in a retrospective cohort and (2) feasibility of a trainee-taught intervention in a prospective cohort of patients with gynecologic cancer to help manage cancer-related cognitive impairment (CRCI).
Methods:
Adults with any stage gynecologic cancer who completed chemotherapy and reported cognitive complaints were eligible. Additionally, the screening criteria of Functional Assessment of Cancer Therapy–Cognition (FACT-Cog) perceived cognitive impairment (PCI) subscale score <59 was used in the prospective cohort. Validated patient-reported outcomes including FACT-Cog and Patient-Reported Outcomes Measurement Information System (PROMIS) Applied Cognition Abilities and General Concerns were measured before and after the intervention.
Results:
Twelve patients underwent an attending-taught intervention between 2011 and 2014. Significant improvements in mean FACT-Cog PCI (+6.1, P < .048), quality of life (+2.4, P = .04), and total score (+9.8, P = .03) were demonstrated, while there was no significant change in mean FACT-Cog perceived cognitive abilities. Ten patients underwent a trainee-taught intervention in 2017. No significant changes in mean FACT-Cog subscale or total scores were seen. Significant improvements in PROMIS Applied Cognition Abilities (+8.2, P = .01) and PROMIS Applied Cognition General Concerns were demonstrated (−8.0, P < .01).
Conclusions:
Our psychoeducational intervention demonstrates applicability to patients with gynecologic cancer reporting CRCI and supports the feasibility of more widespread training based on improvements in validated patient-reported outcomes related to cognition.
Keywords
Introduction
Cancer-related cognitive impairment (CRCI) is common and may affect up to 75% of patients with gynecologic cancer undergoing chemotherapy. 1,2 In addition, up to one-third of cancer survivors may continue to report symptoms of cognitive dysfunction that persist for months or years (even 5 or more years) after treatment, suggesting that CRCI does not always improve with time alone. 3,4 These cognitive complaints, such as difficulty with short-term memory, concentration, and multitasking, can have a significant impact on cancer survivors’ quality of life (QOL) and ability to carry out their daily activities. 3
Neuropsychological testing has been used to evaluate CRCI; however, these tests are more time and resource intensive compared to patient-reported outcomes, which can limit their widespread clinical utility. 1,5 In addition, while neuropsychological tests can measure more specifically defined cognitive abilities, they may not be as sensitive as patient-reported outcomes to some of the more subtle cognitive changes associated with chemotherapy or those that most noticeably affect day-to-day function. As a result, patient-reported outcomes have been recognized as a relevant outcome measure for studying CRCI. 5 The Functional Assessment of Cancer Therapy–Cognition (FACT-Cog) and Patient-Reported Outcomes Measurement Information System (PROMIS) Applied Cognition are examples of validated patient-reported outcomes related to cognition that can be utilized in a clinical setting. 6,7
Cognitive rehabilitation has the potential to provide patients with behavioral strategies and skills to help manage CRCI. Emerging from the Haze is a 15-hour psychoeducational intervention that is offered as a clinical program at our institution. The program has been taught by the cancer rehabilitation physician and neuropsychologist (referred to as “attendings”) who developed the curriculum. The current pilot study is divided into 2 parts. The objective of the first part of the study is to evaluate the clinical applicability of the intervention in a retrospective cohort of patients with gynecologic cancer by comparing patient-reported outcomes before and after the attending-taught intervention. The objective of the second part of the study is to evaluate the feasibility of conducting the intervention with newly trained instructors (referred to as “trainees”) by comparing patient-reported outcomes before and after the trainee-taught intervention in a prospective cohort of patients with gynecologic cancer.
Methods
The current study was approved by the institutional review board of Cedars-Sinai Medical Center (IRB #Pro00046105). A waiver of informed consent was obtained for the retrospective part of the study. Written informed consent was obtained from all participants in the prospective part of the study. Emerging from the Haze is a 15-hour psychoeducational intervention conducted over 6 weeks. The curriculum emphasizes the multifactorial etiology of CRCI, including the potential role of cytokines, direct effects from cancer and its treatment, genetic vulnerability, hormonal changes, other medical comorbidities, pain, medication side effects, poor sleep, depression and anxiety, chronic stress and loneliness, poor nutrition, and physical inactivity. The materials are divided into 2 broad categories: neuropsychology and cancer rehabilitation topics. The neuropsychology material includes education on neuroplasticity and behavioral and compensatory strategies for stress management, guided relaxation, mindfulness meditation, negative thinking, attention, memory, problem solving, and coping difficulties. The cancer rehabilitation material includes information on behavioral changes to promote healthy exercise, sleep hygiene, and nutritional habits as well as the impact of social isolation on CRCI. An educational binder with printed didactic slides and supplementary homework is provided to all participants to reinforce key concepts and skills.
The first part of the study is a retrospective review of patients with gynecologic cancer who were consecutively enrolled in a clinical (nonresearch) attending-taught intervention between February 2011 and November 2014. The classes included participation by patients with any cancer types. Adult females ≥18 years of age with a diagnosis of any stage gynecologic cancer who were treated with chemotherapy alone or in combination with surgery, radiation, and/or hormonal therapy were included. Patients were referred to the program based on subjective cognitive complaints. Patient characteristics were collected, including patient age, cancer type, months since last active treatment, and year of intervention. Perceived cognitive impairment (PCI), QOL, and perceived cognitive abilities (PCA) subscales of the FACT-Cog version 3 were used as patient-reported outcomes. 6 Assessments were performed preintervention (first day of class) and postintervention (last day of class).
The second part of the study is a prospective cohort of patients with gynecologic cancer who were enrolled in a research study involving a trainee-taught intervention from February to May 2017. The trainees included an MD in gynecologic oncology fellowship and a PsyD in neuropsychology postdoctoral fellowship. The training for delivering the intervention included observing the class series at least once and leading the class series independently at least once prior to the start of this current study. The classes only involved participation by patients with gynecologic malignancies. Adult females ≥18 years of age with a diagnosis of any stage gynecologic cancer treatment who were treated with chemotherapy alone or in combination with surgery, radiation, and/or hormonal therapy were included. Participants must have completed active cancer treatment at least 2 months and no more than 60 months prior to enrollment. Continued active treatment with hormonal therapy alone, however, was allowed. Additionally, baseline screening score of <59 on the FACT-Cog PCI subscale was required prior to enrollment. 8 Patients were excluded from the intervention if there was documentation of significant personality disorder or unstable psychiatric disorder, history of brain metastases or radiation to the brain, history of stroke or other severe neurological condition, active treatment for another cancer, or significant uncontrolled intercurrent illness that would limit compliance with the class schedule. Patient characteristics were collected, including age, race, highest educational attainment, menopausal status, cancer type, months since initial diagnosis, months since last active treatment, and number of classes attended out of 6 total classes. Several patient-reported outcomes were utilized: FACT-Cog version 3 PCI, PCA, and QOL subscales; PROMIS scales including PROMIS version 1.0 Applied Cognition Abilities Short Form 8a, PROMIS version 1.0 Applied Cognition General Concerns Short Form 8a, and PROMIS-29 version 2.0; and the University of California Los Angeles (UCLA) Loneliness Scale version 3 (Table 1). Assessments were performed preintervention (first day of class) and postintervention (last day of class).
Patient-Reported Outcome Instruments Measuring Cognition and Quality of Life Domains.
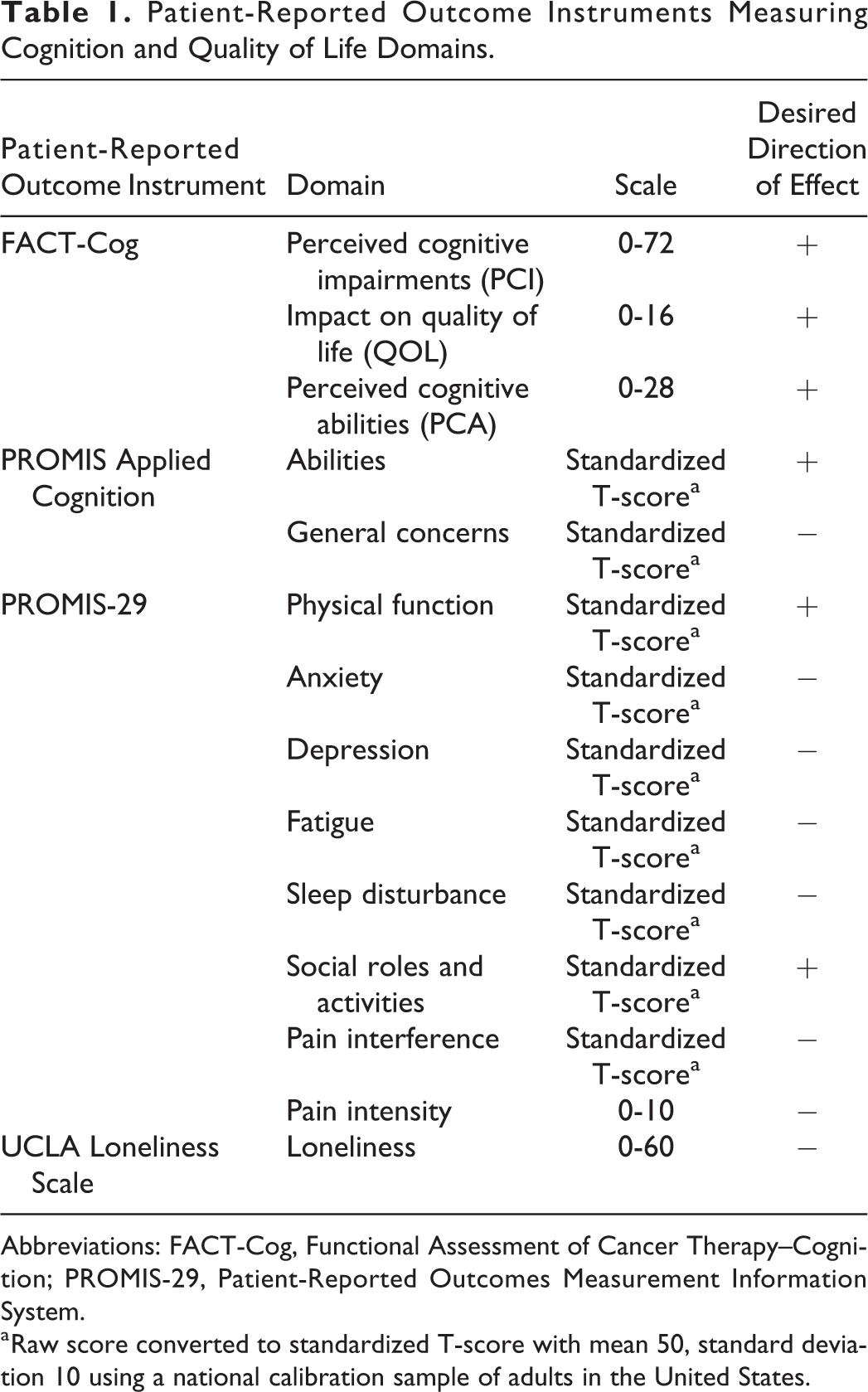
Abbreviations: FACT-Cog, Functional Assessment of Cancer Therapy–Cognition; PROMIS-29, Patient-Reported Outcomes Measurement Information System.
a Raw score converted to standardized T-score with mean 50, standard deviation 10 using a national calibration sample of adults in the United States.
Descriptive statistics were performed for patient characteristics, including mean, range, and frequency/percentage. The FACT-Cog subscale and total scores were calculated, with higher scores indicating better cognition or QOL. 6 The mean change in FACT-Cog subscales (PCI subscale from 0 to 72, QOL subscale from 0 to 16, PCA subscale from 0 to 28) and total score (total score scale from 0 to 116) were calculated from preintervention to postintervention, and paired t tests were performed. The percentage of patients who met or exceeded the suggested minimal clinically important difference (MCID) of at least a +4.7% to +7.2% increase in FACT-Cog subscale or total score were calculated based upon a published validation study in patients with breast cancer. 6,9 We chose to use the percentage increase thresholds rather than raw score increase thresholds proposed in this study since the authors used slightly different scoring procedures. For the PROMIS Applied Cognition Abilities and General Concerns questionnaires, the raw score was converted to a standardized T-score with a mean of 50 and standard deviation of 10 based on published scoring guidelines using a national calibration sample of adults in the United States. 10,11 For the PROMIS Applied Cognition Abilities, the desired direction of effect is a higher score indicating better self-reported cognitive abilities, whereas, for the PROMIS Applied Cognition General Concerns, the desired direction of effect is a lower score indicating fewer self-reported concerns about cognition. The PROMIS-29 includes questions related to 7 domains (physical function, anxiety, depression, fatigue, sleep disturbance, social roles and Activities, and pain interference). In addition, there is a question related to pain intensity. For the PROMIS-29, the raw score for each of the 7 domains is converted to a standardized T-score similarly based on published scoring guidelines. 10 The desired direction of effect is a higher score for Physical Function and Social Roles and Activities. The desired direction of effect is a lower score for anxiety, depression, fatigue, sleep disturbance, and pain interference. Pain intensity is on a scale from 0 to 10, with higher scores indicating higher levels of pain. The mean change in standardized T-score or pain intensity raw score from preintervention to postintervention was calculated, and paired t tests were performed. The UCLA Loneliness Scale was scored based on published scoring guidelines from 0 to 60, with higher scores indicating more loneliness. 12 The mean change in loneliness score was calculated from preintervention to postintervention, and a paired t test was performed.
Results
For the retrospective part of the study, there were 12 total patients with gynecologic cancer included who attended the clinical (nonresearch) attending-taught intervention. The mean number of classes attended was 5.8 (range: 5-6), with 100% attending at least 4 of 6 classes. The mean age was 46 years old (range: 34-79). Eight (67%) patients were diagnosed with ovarian cancer, 2 (17%) with endometrial cancer, 1 (8%) with cervical cancer, and 1 (8%) with choriocarcinoma. Ten (83%) participants were menopausal and 2 were actively taking hormone replacement therapy during the intervention period. The mean number of months since last active treatment was 14.1 (range: 0-57.6). Three (25%) participated in the clinical course in 2011, 1 (8%) in 2013, and 8 (67%) in 2014. There was a statistically significant increase in mean FACT-Cog PCI (+6.1, P = .048), QOL (+2.4, P = .04), and total score (+9.8, P = .03) from preintervention to postintervention. There was no significant difference in FACT-Cog PCA (+1.3, P = .10) between these time periods. The percentage of participants who met the MCID threshold of at least +4.7% to +7.2% increase from preintervention to postintervention was 50% to 58% for FACT-Cog PCI, 42% for FACT-Cog QOL, 33% to 42% for FACT-Cog PCA, and 42% to 58% for FACT-Cog total score. The FACT-Cog scores for the retrospective cohort are summarized in Table 2.
Significant Improvements Were Demonstrated on the FACT-Cog PCI and QOL Subscales and Total Score Between Preintervention (First Day of Class) and Postintervention (Last Day of Class) for a Retrospective Cohort of Patients With Gynecologic Cancer Undergoing an Attending-Taught Psychoeducational Intervention, Emerging From the Haze.a
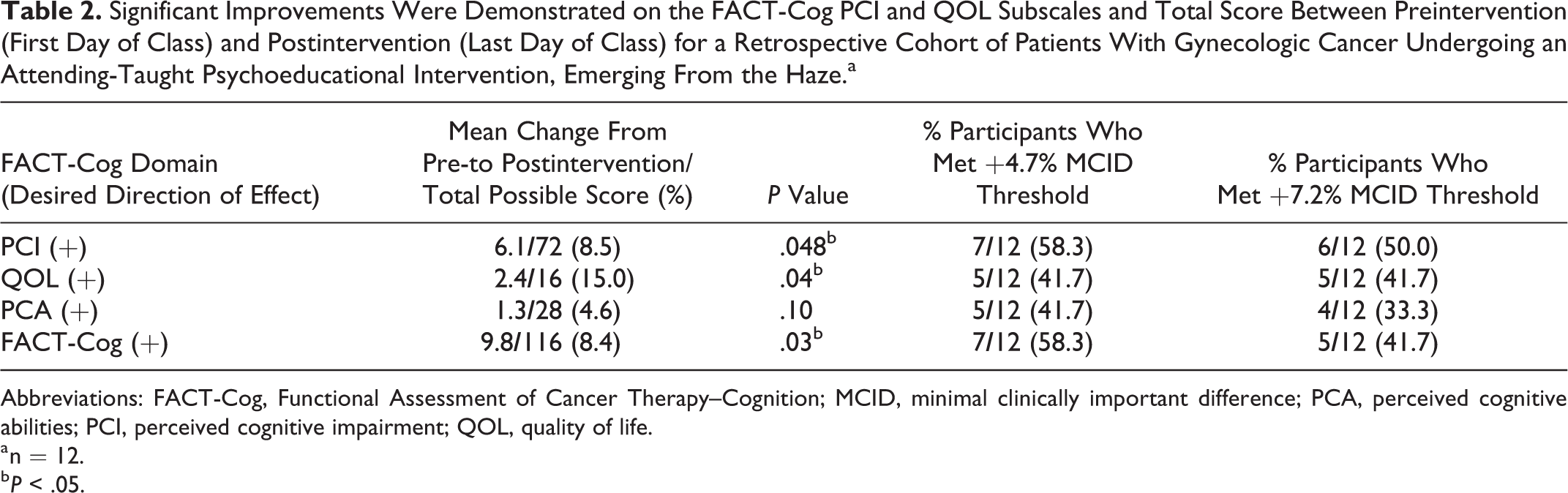
Abbreviations: FACT-Cog, Functional Assessment of Cancer Therapy–Cognition; MCID, minimal clinically important difference; PCA, perceived cognitive abilities; PCI, perceived cognitive impairment; QOL, quality of life.
a n = 12.
b P < .05.
For the prospective part of the study, there were 10 total patients with gynecologic cancer who attended at least 2 of 6 research trainee-taught intervention classes. One participant who only attended 1 of 6 classes and did not complete the postintervention survey was excluded from the analysis. The mean number of classes attended was 4.2 (range: 2-6), with 70% attending at least 4 of 6 classes. The mean age was 56 years old (range: 35-75). There were 5 participants in each of 2 series. Seven (70%) participants identified as white and 1 participant identified as black/African American, Asian, and 2 or more races each. For highest level of educational attainment, 1 participant had completed high school (10%), 4 (40%) had completed college, and 5 (50%) had completed graduate school. Nine (90%) participants were menopausal, and none were on hormone replacement therapy. Eight (80%) patients were diagnosed with ovarian cancer and 2 (20%) with endometrial cancer. The mean number of months since initial diagnosis was 79.9 (range: 6.2-465.8), and the mean number of months since last active treatment was 24.2 (1.4-59). There was no significant difference in FACT-Cog PCI (+8.3, P = .10), FACT-Cog QOL (+2.7, P = .05), FACT-Cog PCA (+3.5, P = .05), or FACT-Cog total score (+14.5, P = .07). The percentage of participants who met the MCID threshold of at least +4.7% to +7.2% increases from preintervention to postintervention were 60% to 70% for FACT-Cog PCI, 60% for FACT-Cog QOL, 40% to 50% for FACT-Cog PCA, and 60% to 70% for FACT-Cog total score. Functional Assessment of Cancer Therapy–Cognition scores for the prospective cohort are summarized in Table 3. There was a statistically significant improvement in mean standardized T-score from preintervention to postintervention for PROMIS Applied Cognition Abilities (+8.3, P = .01) and PROMIS Applied Cognition General Concerns (−8.0, P < .01). There was a statistically significant improvement in standardized T-score for physical function (+7.6, P = .02), anxiety (−11.3, P = .04), depression (−9.9, P = .02), fatigue, (−7.3, P = .04), and pain interference (−4.9, P = .03) on the PROMIS-29. There was no statistically significant change in mean standardized T-score for sleep disturbance (+1.8, P = 0.06) or raw score for pain intensity (−0.3, P = .03) from preintervention to postintervention. There was a statistically significant decline in social roles and activities (−5.8, P = .02), which was in the opposite direction of the desired effect. Patient-Reported Outcomes Measurement Information System scores for the prospective cohort are summarized in Table 4. There was no statistically significant difference in UCLA Loneliness Score (+1.3, P = .28).
No Significant Change Was Seen in FACT-cog PCI, QOL, or PCA Subscales or Total Score Between Preintervention (First Day of Class) and Postintervention (Last Day of Class) for a Prospective Cohort of Patients With Gynecologic Cancer Undergoing a Trainee-Taught Psychoeducational Intervention, Emerging From the Haze.a
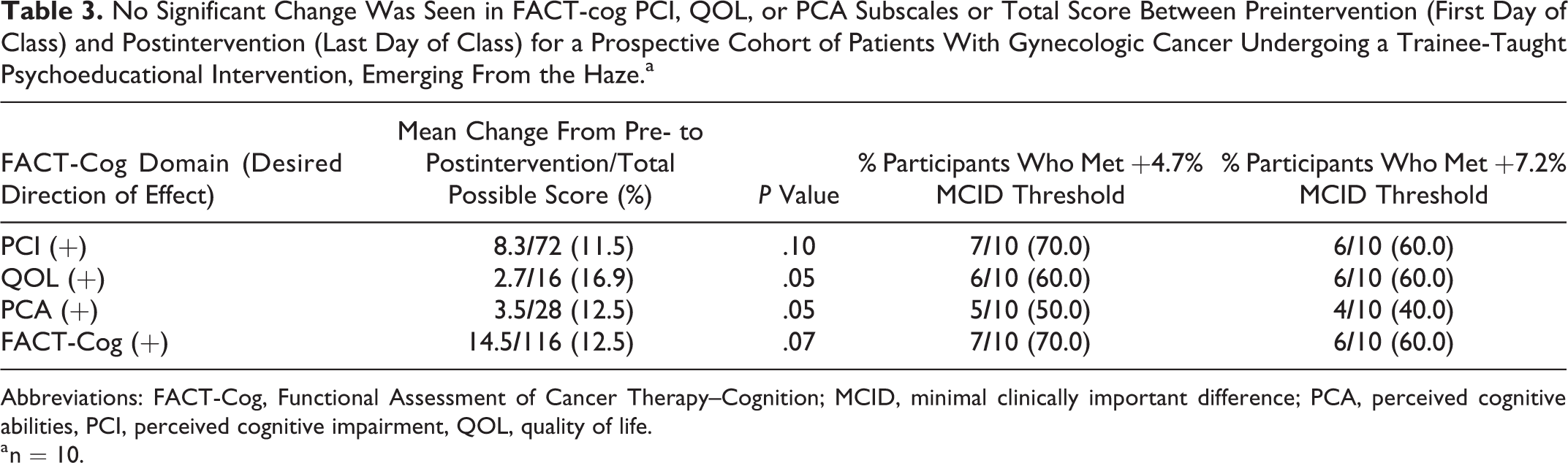
Abbreviations: FACT-Cog, Functional Assessment of Cancer Therapy–Cognition; MCID, minimal clinically important difference; PCA, perceived cognitive abilities, PCI, perceived cognitive impairment, QOL, quality of life.
a n = 10.
Significant Changes in Certain PROMIS Applied Cognition and PROMIS-29 Domains Were Demonstrated Between Preintervention (First Day of Class) and Postintervention (Last Day of Class) for a Cohort of Prospective Patients With Gynecologic Cancer Undergoing a Trainee-Taught Psychoeducational Intervention, Emerging From the Haze.a
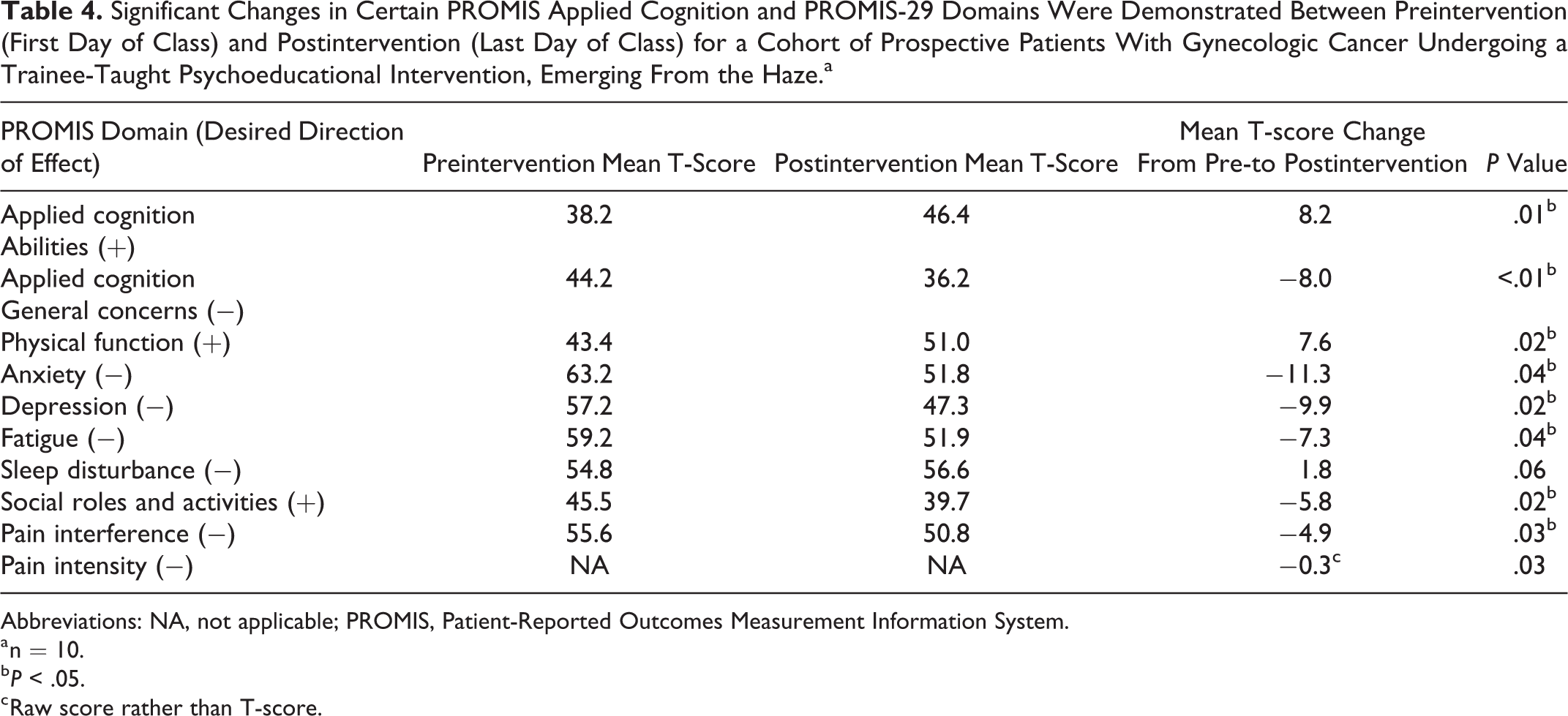
Abbreviations: NA, not applicable; PROMIS, Patient-Reported Outcomes Measurement Information System.
a n = 10.
b P < .05.
c Raw score rather than T-score.
Discussion
Gynecologic cancer survivors who underwent a 15-hour psychoeducational intervention taught by attending clinicians displayed improvements in self-reported cognition using the FACT-Cog, including PCI and QOL subscales. This suggests the applicability of our cognitive rehabilitation program in this specific patient population, where CRCI and its interventions are understudied. Subsequently, a small, prospective group of gynecologic cancer survivors who underwent the same psychoeducational intervention taught by trainee clinicians did not demonstrate statistically significant improvements in self-reported cognition using the FACT-Cog; however, significant improvements were seen on both PROMIS Applied Cognition Abilities and General Concerns. Currently, there is no accepted standard regarding which patient-reported outcome instruments are best used to diagnose or track CRCI. The different findings in these 2 patient cohorts suggest that certain patient-reported outcomes may have varying levels of sensitivity to CRCI or patients with cancer specifically. We applied a threshold from a prior validation study proposing FACT-Cog score of <59 as screening positive for significant PCI to determine eligibility for our prospective intervention group. 8 Furthermore, the MCID threshold of +4.7% to +7.2% increase in FACT-Cog subscales or total score was also used to measure the potential impact of our intervention. For the retrospective attending-taught cohort, the percentage of patients who had clinically significant improvements in FACT-Cog based on these criteria ranged from 33% to 58%. For the prospective trainee-taught cohort, the percentages were slightly higher between 40% and 70%. It is important to note that most of the available validation studies have been conducted in patients with breast cancer, which underscores the importance of exploring these interventions and their impact on patient-reported outcomes in other cancer patient populations. In our prospective cohort, significant improvements were also noted in 5 of 7 domains of the PROMIS-29 including physical function, anxiety, depression, fatigue, and pain interference. These improvements suggest that the intervention may not only have an impact on self-reported cognition but may also have a favorable effect on QOL domains. The prospective cohort also experienced a significant decline in their perception of their social roles and Activities, which was in the opposite direction of the desired effect. This domain likely lies more at the periphery of our curriculum and reflects individuals’ interactions with others outside of the intervention; therefore, the social roles and activities domain may be less sensitive to our intervention. The impact of chronic loneliness and social isolation is discussed during one of our sessions.
Cognitive rehabilitation programs have been previously studied in patients with cancer reporting CRCI, including several wait-list controlled and randomized controlled trials. 13 -15 An in-person memory and attention adaptation training curriculum demonstrated improvements in certain QOL domains and improved verbal memory on neuropsychological testing in a group of patients with breast cancer who had received chemotherapy. 13 Our psychoeducational curriculum is unique in that it seeks to emphasize the likely multifactorial etiology of CRCI; therefore, we combine didactic components related to both neuropsychological compensatory strategies but also to other areas that contribute to overall well-being, such as promoting evidence-based behavioral changes related to stress relief, sleep, exercise, nutrition, and social activities. Attendance in the retrospective group was high, which supports the feasibility of the weekly program structure; however, the inconsistent attendance seen in the prospective group (with an average of 4 of 6 total classes attended) emphasizes the commitment that is required to comply with the intervention, even in a group of presumably motivated individuals who have agreed to participate in a research study. Thus, there may be an important role for home-based interventions or online training programs, which have also previously demonstrated improvements in neuropsychological testing and patient-reported outcome measures for cancer survivors reporting CRCI. 14,15
As a pilot study, our results are limited by small sample size. The FACT-Cog and PROMIS questionnaires ask patients to indicate their responses based on their experiences in the last 7 days, while the UCLA Loneliness Score asks for more broad responses such as “how often” the respondent feels a certain way. Particularly in a small sample, the mean change in these scores may be prone to changes attributable to life circumstances, which are unmeasured in our study, rather than the intervention itself. In addition, the use of hormone replacement therapy in menopausal women could have a favorable, unmeasured effect on QOL independent of the intervention. As there was no control group in our observational study, it is possible that the improvements in patient-reported outcomes that were observed may have also been observed in a group receiving any intervention. The first part of the study is also limited by the biases inherent to a retrospective review. In addition, the attending-taught intervention was distinctive in that it was taught by the 2 clinicians who designed the intervention, which may limit its external validity. This did provide the impetus for the prospective part of the study where we studied the intervention conducted by trained clinicians.
Our pilot study confirmed the feasibility of effectively delivering a trainee-taught psychoeducational intervention to patients with gynecologic cancer. Additional follow-up of the prospective cohort is planned at 6 and 12 months to study whether the observed improvements in PROMIS Applied Cognition or PROMIS-29 scores persist over time. Furthermore, data on a prospective, wait-list controlled study of the attending-taught intervention in a cohort of patients with breast cancer, which also examined the use of live webcasting, will be available in the near future. The described psychoeducational intervention adds a potential treatment option to the small but growing literature regarding the potential benefits of cognitive behavioral rehabilitation on cognitive symptoms and QOL in patients with cancer reporting CRCI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.