
Abstract
Purpose:
Pain is highly prevalent in advanced cancer and requires aggressive management. However, pain management in cancer is minimally investigated in Pakistan. This cross-sectional study explores the adequacy of pain management in patients with advanced stage cancer in Pakistan.
Method:
From January 2017 to May 2017, a cross-sectional study was conducted at Mayo Hospital, Lahore, Pakistan. A total of 218 patients with cancers were interviewed, and 136 patients with pain ≥5 on a Numerical Rating Scale for pain were included in the study. Demographic of patients and clinical characteristics of tumors were also evaluated.
Results:
Only about one-third of the patients with advanced cancer reported adequate pain management. Chi-square test, χ2 (1, n = 136) = 33.038, P < .05, indicated that pain scores were inversely associated with pain control; inadequate pain control was observed in patients with higher pain score and vice versa. Of the 55.88% of patients who were prescribed morphine, only 6 patients were compliant with treatment recommendations. Most patients were prescribed nonopioid medications and tramadol and codeine, which are weak opioid medications.
Conclusion:
The rate of undertreatment of cancer pain in Pakistan is alarming. Inadequate clinicians’ training, patients’ and caregivers’ beliefs, lack of availability of opioid medications, and socioeconomic factors are some of the barriers to effective pain control. A multidisciplinary team approach is necessary to follow the World Health Organization pain ladder guidelines for the treatment of cancer pain.
Keywords
Introduction
Pain is a common and ominous symptom of cancer. 1 It is prevalent in 50% to 70% of patients with cancer and in almost 90% of patients with advanced illness. 2,3 Pain is poorly understood because it can have many different causes including inflammatory, ischemic, neuropathic, and direct compression effects of the mass. 4,5 Chronic cancer pain is often comorbid with psychiatric illness, and it negatively affects the quality of life of the patient. 3
The global burden of cancer continues to grow, particularly with an accelerated incidence rate in low-and middle-income countries (LMIC). 6 Among the many causes of rising cancer rates in these countries are increased longevity, an exponential growth of population, unhealthy lifestyles, socioeconomic factors, and lack of access to health care. Overall, the prevalence of cancer in Asia is high and most patients with cancer present in an advanced stage of the disease that is commonly associated with moderate to severe pain. 7 It is projected that by 2030, there will be 10.7 million people in Asia with cancer and 7.5 million cancer-related deaths. 8 Cancer is already the second leading cause of death in LMIC. 9
The World Health Organization (WHO) analgesic ladder provides a framework for the treatment of cancer pain. 10 For mild pain, it recommends nonsteroidal anti-inflammatory drugs (NSAIDs) or other nonopioid medications; for moderate pain, opioids along with nonopioid medications; and for severe pain, potent opioid medications are recommended. 11 Despite these guidelines, unrelieved pain in cancer is a well-documented phenomenon. 12,13
Pakistan is the sixth most populous country in the world and has a unique set of demographic and socioeconomic factors that can influence the prevalence and treatment of cancer. There is no national cancer registry; consequently, there is extremely limited data available about the prevalence of cancer in Pakistan. 14 The estimated incidence of cancer is ∼150 000 cases each year, and around 60% to 80% of these patients die with in an year. 15
Pakistan has one of the worst ratios of palliative care services to the population in the world—1 to 90 million. 16 Although cancer is an area of great clinical importance, except for a few institutions palliative care is nonexistent. 17 Consequently, most patients do not have access to the palliative care and die with untreated severe cancer pain. 18
To the best of our knowledge, there is no study in the existing literature about the management of pain in cancer, end-of-life care, and palliative care in Pakistan. This study was designed to fill that void; it explores the adequacy of pain management in the largest hospital in the province of Punjab, Pakistan. The objectives of this study are (1) to identify and describe data for adequacy of the pain management in patients with advanced cancer; (2) to establish a relationship between analgesics prescribed and pain control; and (3) to examine the implementation of the WHO analgesic guidelines in these patients.
Methods
A cross-sectional study was conducted over a period of 6 months from January 2, 2017, to May 8, 2017, at Mayo Hospital in the city of Lahore in Punjab province. Mayo Hospital is the largest tertiary-care teaching hospital in Lahore and serves a population over ten million from urban and rural areas.
A nonprobability convenience sampling was used to select 218 patients from both inpatient and outpatient clinical settings of the Department of Oncology of Mayo Hospital. The selection included patients of both genders, ranging in age from 18 to 70 years, all of who had been diagnosed with stage 3 or 4 cancer with an active complaint of pain. Enrollment in this study was voluntary, and no compensation was offered to participate in the study.
These patients were given printed pages with a Numerical Rating Scale (NRS) and a description of the scale. Authors (A.K. and R.N.) explained the scale to the patients and their caregivers. 19 The patients were assessed for their pain scores using an 11 point NRS that scores pain as 0 (none), 1 to 3 (mild pain), 4 to 6 (moderate pain), and 7 to 10 (severe pain). The NRS is anchored by terms describing pain severity extremes with 0 representing one pain extreme (eg, “no pain”) and 10 representing the other pain extreme (eg, “pain as bad as you can imagine” and “worst pain imaginable”). The respondent is asked to indicate the numeric value on the segmented scale that best describes their pain intensity and this number was recorded.
Of the initial sample of 218 patients, 136 patients with a pain score ≥5 were selected as meeting the inclusion criteria for the study. These patients were then evaluated for their type and stage of malignancy and whether medication choices and analgesia control were according to the WHO criteria.
Statistical Analysis
We used IBM SPSS Statistics 22 for analysis of data collected from 136 patients. Descriptive statistics were computed to examine the personal characteristics (Table 1) such as gender, age, residence, and marital status; clinical features (Table 2) such as stage of malignancy, nature of malignancy, pain score of sample, and analgesic used for pain control (Table 3) such as acetaminophen and tramadol. Hypothetical relationships between nominal variables were tested using chi-square tests.
Demographics.a
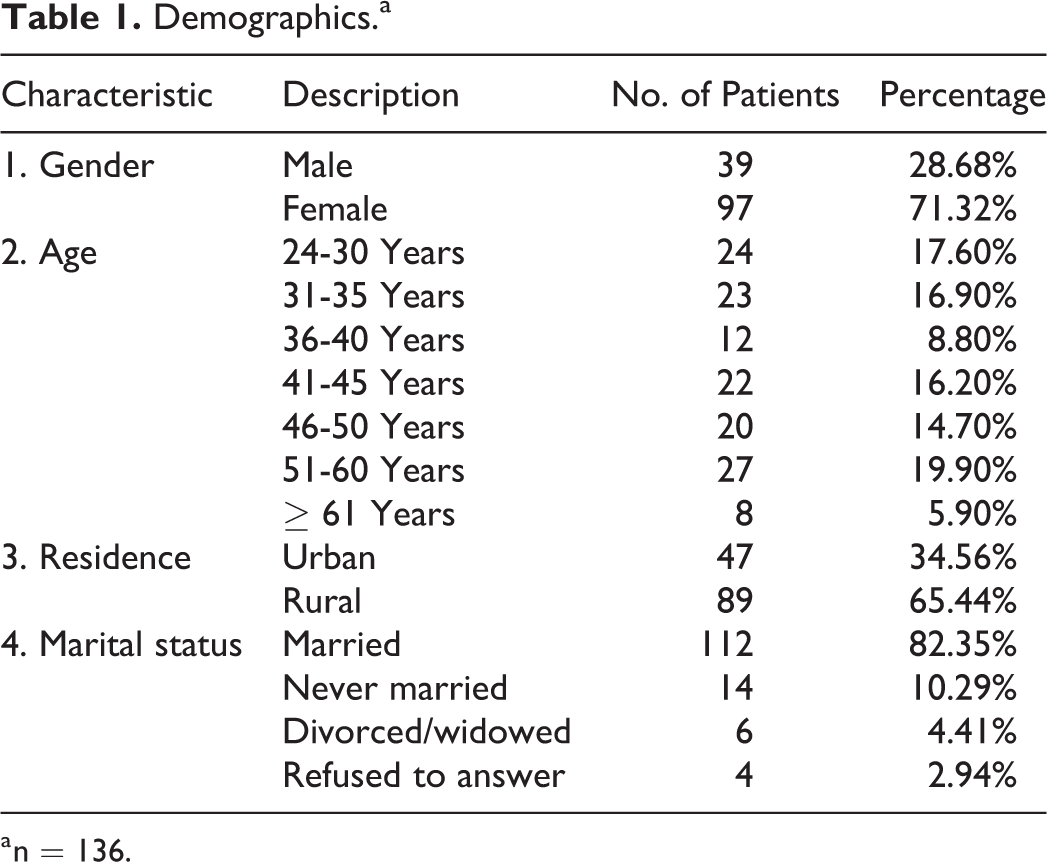
a n = 136.
Clinical Features of Patients in Study.a
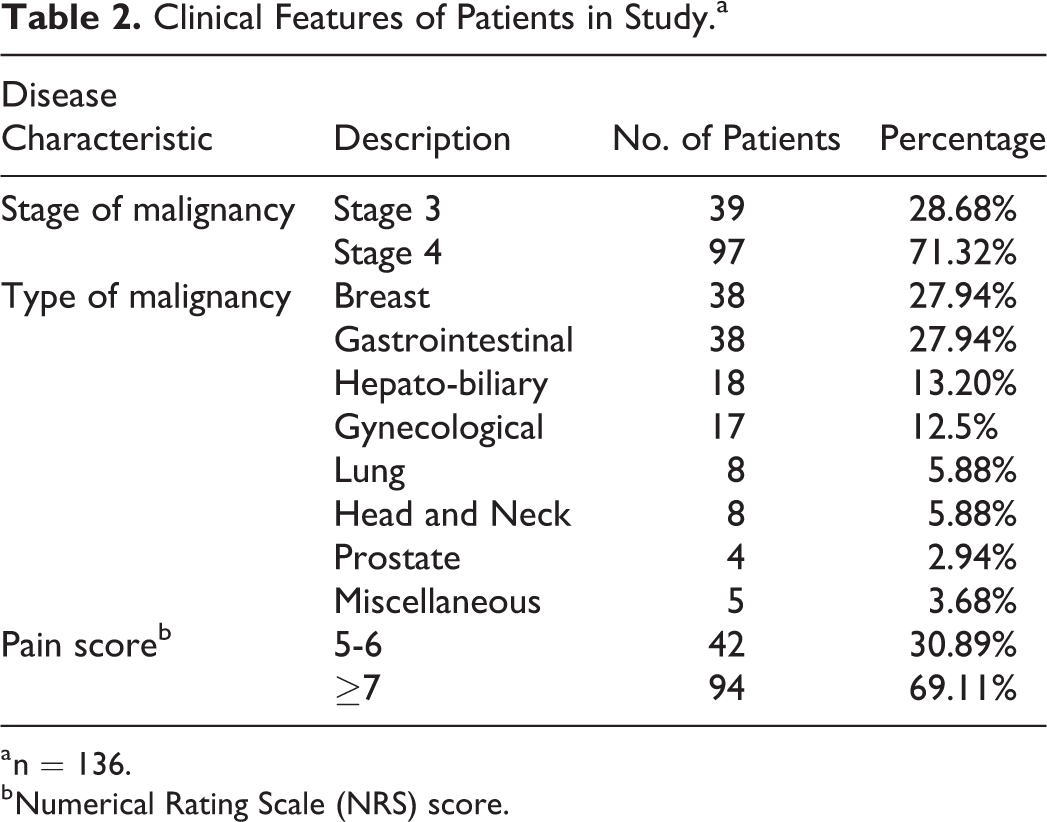
a n = 136.
b Numerical Rating Scale (NRS) score.
Analgesic Prescribed for Pain Control.a
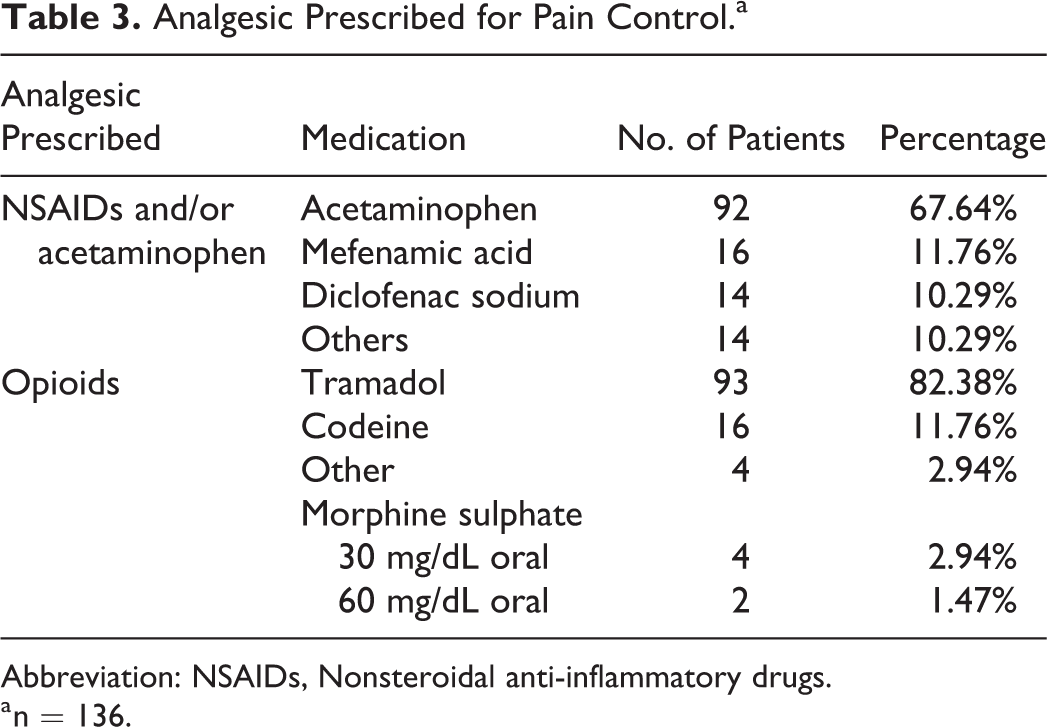
Abbreviation: NSAIDs, Nonsteroidal anti-inflammatory drugs.
a n = 136.
Results
Of 218 patients interviewed, 136 patients (97 females, 39 males) who scored ≥5 on NRS for their cancer-related pain were selected for the study, and their demographics are listed in Table 1. In this cohort, 97 (71.32%) patients had stage 4 and 39 (28.68%) patients had stage 3 cancer (Table 2).
Of 136 patients, 40 (29.41%) presented with stage 3 and 96 (70.59%) patients presented with stage 4 malignancy. Of 136 patients, 94 (69.11%) had a pain score of ≥7/10 (stage 3 = 11, stage 4 = 83). Most common types (27.94% each) of malignancy encountered were carcinoma of breast and gastrointestinal followed by (13.2%) hepatobiliary, and (12.5%) gynecological malignancy (Table 2).
All selected patients were prescribed NSAIDs and/or acetaminophen (Table 3). Of 136 patients, 92 (67.64%) patients were prescribed acetaminophen,16 (11.76%) patients were taking mefenamic acid, 14 (10.29%) were on diclofenac sodium, and 14 (10.29%) were prescribed other NSAIDs (Table 3). Weak opioids were prescribed to 83.08% of all the patients. All patients with stage 4 disease were also receiving opioids. Of 97 patients with stage 4 cancers, 93 (95.88%) were taking tramadol, 16 (14.15%) were taking codeine, and 4 (3.54%) patients were taking other weak opioids. Sustained released morphine sulfate was originally prescribed to 76 patients. However, only 6 (7.89%) patients were compliant with the recommendation. Among these, 4 (66.67%) patients were taking a maximum of 30 mg/d, and 2 (33.3%) patients were taking 60 mg/d of sustained release morphine sulfate (Table 4).
Chi-Square Results of Analgesic Used and Pain Control.
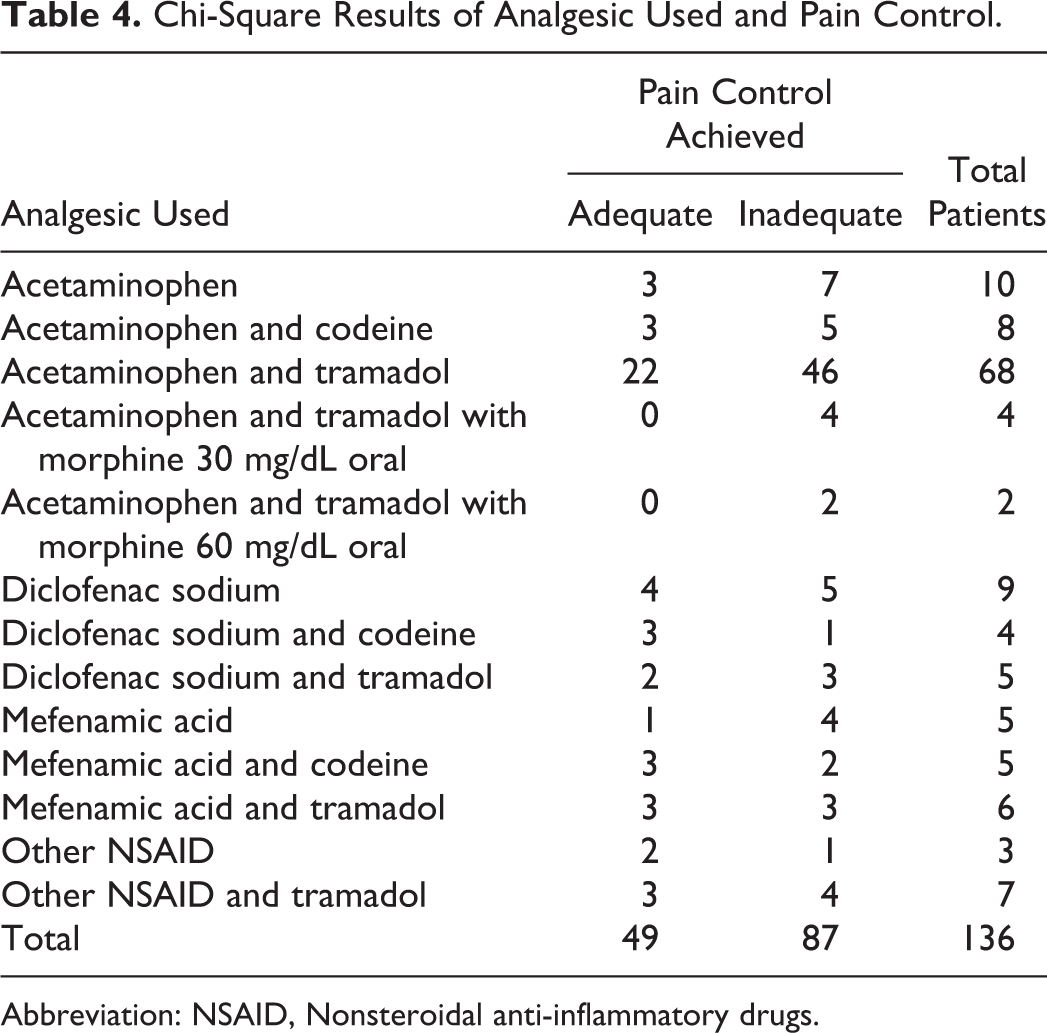
Abbreviation: NSAID, Nonsteroidal anti-inflammatory drugs.
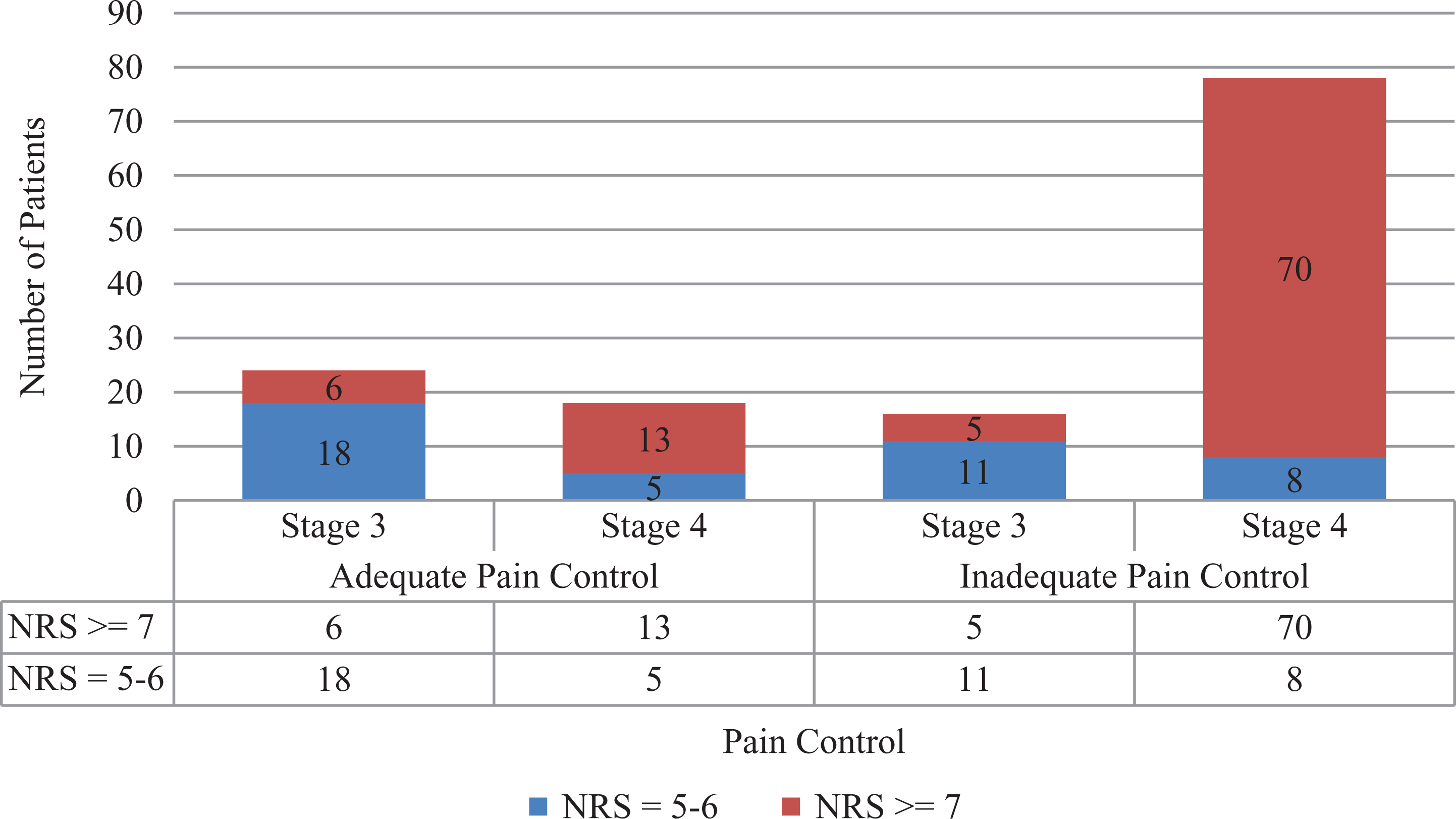
Chi-square test, χ2 (1, n = 136) = 33.038, P < .05, indicated a significant negative relationship between pain score and pain control (Table 5). Patients with higher pain score (≥7) received inadequate pain control; 87 (64%) of the total patients were having a pain score of 7 or more, but only 12 (9%) of them achieved adequate pain control. A total of 94 (69%) of all patients (19 with NRS = 5-6, 75 with NRS ≥7) had higher levels of pain with inadequate pain control (Figure 1).
Chi-Square Results of Pain Score and Pain Control.
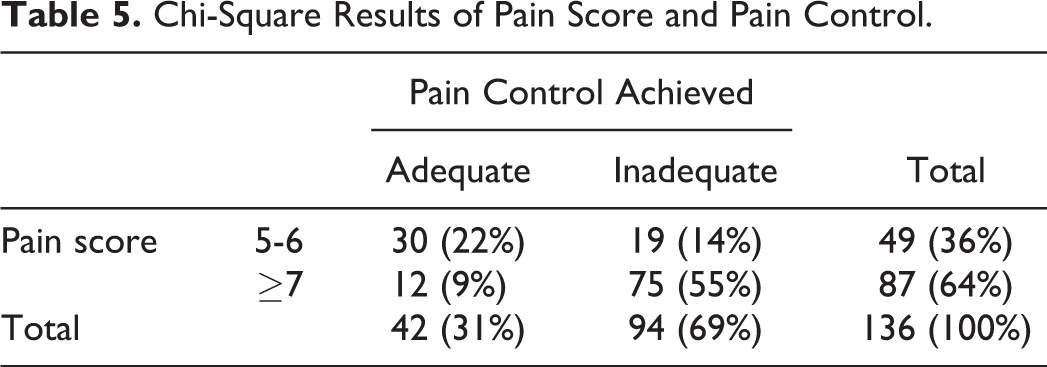
Pain score of patients and level of pain control achieved.
The insignificant association of analgesic prescribed with adequacy of pain control achieved was determined by chi-square test, χ2 = (1, n = 136) = 16.463, P < .560 (Table 4). The medicines that provided adequate control to some patients provided inadequate pain control to other patients. Acetaminophen and tramadol combination was prescribed to 46 patients. It provided adequate pain relief to 17 and inadequate pain relief to the other 29 patients (Table 4). Analgesics were prescribed to 49 patients with a pain score of 5 to 6 of which 30 (71%) achieved adequate pain control. The same analgesics were given to 87 patients with a pain score (≥7) of which only 12 (9%) achieved adequate pain control and the remaining 75 (55%) patients had inadequate pain control.
Those patients who received prescription opioids had a median pain score of 7.8/10. The most common sites of metastasis in these patients were bones (67%), liver (22%), and brain (11%). All patients with brain metastatic disease also received whole-brain radiotherapy. The patients with bone metastasis with the impending risk of pathological fracture and the patients whose pain was not controlled with higher doses of analgesics also received palliative radiotherapy to the site of maximum pain.
Adequate pain control was achieved in only 42 (31%) patients. The remaining 94 (69%) patients still suffered due to insufficient pain management (Figure 1).
Discussion
This study highlights the serious practice gaps in effective pain management in patients with advanced stage cancer in Pakistan. Only about one-third of the patients with moderate to severe pain reported receiving adequate pain management. Mostly, weak opioids were prescribed to the patients, and when morphine was prescribed, the compliance was very poor. This finding of undertreatment provides strong evidence about the failure to implement the WHO guidelines for cancer pain management in an overwhelming majority of the patients in this study.
The rate of undertreatment of cancer pain in this study—approximately 63.97% of patients—is more than double the rate found in other countries in recent studies. With the advent of better and safer analgesic technique, rates of undertreated cancer pain dropped from 43% in 2007 to 31.8%% in 2013. 20,21 These 2 review articles show significant improvement in cancer treatment globally in the last decade. A Canadian study by Vuong et al showed that the prevalence of undertreated cancer pain was 33.3%, although 106 of 196 patients who received potent opioid analgesics still complained of pain. 22
Even those patients who were treated with opioids received weak medications or were unable to obtain and use the medications prescribed. All patients in this study with stage 4 cancers were offered a combination of nonopioids and opioid medications. The most commonly prescribed opioid analgesic were tramadol and morphine followed by codeine. Tramadol and codeine are weak opioids and usually are not recommended as primary medications for treatment of severe cancer pain. 23
One surprising finding of this study was, even in the presence of pain compliance with a potent opioid medication—morphine—pain control was extremely poor. This could be due to a number of factors. Morphine is difficult to obtain in Pakistan. Moreover, only injectable morphine is relatively accessible. Due to the lack of proper nursing services, it could be extremely difficult to find intravenous access to deliver the medication, particularly at home. Socioeconomic factors and poor access to health care may also play a critical role in poor compliance with treatment recommendations for pain management. It has been established that factors for analgesic noncompliance can include patient’s forgetfulness or lack of understanding about how to take their analgesics as prescribed due to illness, belief about pain, or social factors such as lack of proper nursing. These findings are in accordance with the previous studies. 24 Similar findings were also published by Simone et al who reported that lack of recommendations from clinicians, fear of addiction, and poor affordability were factors in patient decisions to reject analgesic use for cancer pain. 25
Furthermore, in Pakistan, there is absolutely no legal accessibility to fentanyl, methadone, and oral immediate-release oxycodone for the treatment of cancer pain. 7 All these medications are considered as the mainstay of pain control in cancer in the developed world. 23 In Pakistan, controlled release oral morphine is rarely available and then only in a limited number of pharmacies. Physicians with a special permit or license can only prescribe these medications with a limit of 14 days of supply at a time. These restrictions can impact the clinician’s prescribing decisions and patients’ and caregivers’ access to the appropriate health care.
No patient in this study was offered any alternative treatment for pain. Usually, psychotherapeutic interventions and other therapies such as yoga or physical therapy are not considered first-line treatment for cancer pain. 26 There is significant evidence that psychosocial and spiritual treatments could help some patients bring down the pain intensity or help the patient to cope better with the pain. 27,28 Moreover, Simone et al found that almost all (94%) of the patients who refused analgesics for cancer pain used alternative therapies for the treatment of their pain. 25
One surprising finding of our study is that females had two and half times higher rates of advanced cancers than their male counterparts. This information is out of sync with other local incidence studies. Yusuf reported that the age-standardized ratios (ASR) for cancers in Pakistan are 1:1.2 for males to females. 15 In a cancer registry from Karachi, ASR was 1:1.9 for males to females. 29 Although results of our study were not recorded as ASR, still the gender discrepancy is noticeable. This gender discrepancy may show that women’s pain is undertreated and thus overrepresented in this study.
There are several practical implications of these findings that could help in designing effective palliative and end-of-life care policies and practices to improve patient comfort. Another constraint in this region is a scarcity of trained medical personnel for cancer pain management or for palliative care. In contrast to the West, in the Asian region generally pain management is seen as a component of disease treatment and is not handled as an essential adjunctive developed branch of medicine. There is already some collaboration in the education of palliative care physicians from LMIC at the University of Wisconsin-Madison in the United States. 30 Physicians trained in end-of-life care and palliative medicine in the West can help to bridge the gap in education and services in Pakistan. 31 Because of the excessive burden of cancer, more physicians should be educated in the effective treatment of pain disorders. 32 Pakistan’s first hospice and palliative care facility is being created and hopes to provide relief to a limited number of patients. 33
However, there are manifest limitations of this study that need to be acknowledged. These include inclusion of all patients from a single setting, the cross-sectional design and convenience sampling technique, and the self-reporting nature of the questionnaire might limit the generalizability of the study. Future studies should explore the knowledge and attitude about cancer pain management in diverse populations in multiple settings with a more rigorous design and sampling technique.
Conclusion
Overall results indicate that patients suffered from high levels of pain in the absence of efficient and effective pain treatment. The rates of undertreatment of cancer pain in Pakistan found in this study are alarming. Patients with cancer have a right to live pain-free and with dignity even with a terminal illness. Clinicians’ training, inadequate pain assessment, patient and caregiver deficient education, lack of availability of opioid medications, extreme opioid regulation, socioeconomic factors are some barriers to effective pain management for patients with cancer. Until these hurdles are overcome, the WHO pain ladder goal of freedom from pain in cancer will not be achieved.
Footnotes
Authors’ Note
Muhammad Hassan Majeed and Ramsha Nadeem are cofirst authors. All authors contributed to collection and assembly of data; data analyses and interpretation; final approval of manuscript; and accountable for all aspects of the work. Ramsha Nadeem and Abbas Khokar contributed in conception and design. Muhammad Hassan Majeed and Ramsha Nadeem contributed in manuscript writing. IRB approval was obtained from Mayo Hospital, Lahore.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.