
Abstract
Purpose:
The purpose of this study was to explore the perceptions of critical care nurses regarding the withdrawal or withholding of enteral nutrition (EN) and parenteral nutrition (PN) at the end-of-life, which is not allowed according to the current law in South Korea.
Methods:
This was a cross-sectional study utilizing a self-report survey. The participants in the study were 141 nurses working in the intensive care units of a tertiary university hospital. The critical care nurses’ general attitudes about EN and PN at the end-of-life were measured using the questionnaires developed by Lubart, Leibovitz, and Habot. The nurses responded to additional questions on whether withdrawal or withholding of EN or PN at the end-of-life should be legally allowed.
Results:
The mean scores of the general attitude items on EN ranged between 3.03 and 3.35 on a 5-point Likert scale where a value of 1 represents “strongly disagree” and a value of 5 represents “strongly agree,” while those for PN ranged between 2.89 and 3.65. Respecting attitudes toward EN and PN, critical care nurses had more negative attitudes about stopping PN than EN. Regarding attitudes about whether patients should be legally able to refuse EN, 34.3% agreed, while 25.7% disagreed. For PN, 40.0% agreed, while 24.3% disagreed.
Conclusion:
Discussions about making the withdrawal and withholding of artificial nutrition legal should be initiated. Moreover, education regarding evidence about the outcomes of EN and PN during end-of-life care and up-to-date clinical guidelines about it should be provided.
Keywords
Introduction
In 2009, the Supreme Court of Republic of Korea, in the well-known case of “Grandmother Kim,” granted the request of Ms Kim’s children to withdraw ventilator support from Ms Kim, who was an elderly woman in a persistent vegetative state. In doing so, the Court cited respect for Ms Kim’s decision on her own behalf and the need to protect human worth, dignity, and the right to the pursuit of happiness. 1 Prior to this case, cessation of life-sustaining treatments was considered illegal, and a patient’s right to refuse life-sustaining treatments was not ensured. This landmark case was the first in South Korea to cite a patient’s privacy in a decision regarding the withdrawal of life-sustaining treatments. Moreover, through the influence of this Supreme Court case, the Act on Decisions on Life-Sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life (also known as the Act on Decision on Life-Sustaining Treatment) was passed by the National Assembly in 2016. This was the first law to allow decision-making regarding the withdrawal or withholding of life-sustaining treatments in South Korea.
For decades, there had been intense legal, ethical, and social debates, as well as opposition from some religionists, regarding legislation to allow the withdrawal or withholding of life-sustaining treatments at the end of life. 2,3 Nevertheless, the enforcement of the Act on Decision on Life-Sustaining Treatment rapidly affected advance care planning in South Korea. Health-care facilities have made changes in their systems because of this Act. Moreover, during the first 2 months after the enactment of this law, life-sustaining treatments were withdrawn or withheld from more than 3000 patients. 4 This legislation, however, forbids the withdrawal or withholding of artificial nutrition (AN). Article 19 of the Act states that nutrients and hydration cannot be withdrawn or withheld. Therefore, patients or their surrogates cannot refuse AN in South Korea. This issue was addressed by the United States in the case of Nancy Cruzan several decades ago. In this critical 1990 case, the US Supreme Court recognized a patient’s right to refuse AN, which influenced clinical practice and laws worldwide. 5 Currently, in general, refusal of AN is accepted legally and ethically, and there are guidelines for clinical practice regarding the withdrawal or withholding of AN in the United States and European countries. 6 -8
Even in the United States and European countries, laws allowing the withdrawal of AN were enacted after other laws allowing the termination of life-sustaining treatments. In 1976, the New Jersey Supreme Court granted discontinuation of ventilator care in the case of Karen Quinlan. In Quinlan’s case, AN was not an issue. It took decades before AN became an issue, in the case of Nancy Cruzan. 9 Moreover, even in countries where refusal of AN is legally and clinically accepted during palliative care, stopping AN is perceived somewhat differently from stopping other treatments. 6,10,11
Considering the history of palliative care in Western countries, South Korea may be entering a transitional period between an era in which the withdrawal and withholding of life-sustaining treatments other than AN during palliative care are allowed and an era that includes AN. Health-care providers have just begun the practice of withdrawing or withholding life-sustaining treatments from terminally ill patients but do not withdraw or withhold AN, which is not allowed by law. This study aimed to survey Korean nurses’ perceptions about the withdrawal or withholding of AN at this critical time in the history of palliative care in South Korea.
Intensive care units (ICUs) are the places where life-sustaining treatments, including AN, are most frequently provided to patients and where many patients spend their last days of life. One of 5 people dies in ICUs in the United States. 12 According to national data from the Korean National Health Insurance, from 2009 to 2010, for older adults aged 65 years and over, 26% admitted ICUs during the last 30 days of their lives. 13 Moreover, about 40000 Korean people per year utilize ICU services at the end of their life. 14
In addition, in ICUs, parenteral nutrition (PN) as well as enteral nutrition (EN) are often provided to patients. 15 PN only, EN only, or EN plus PN are given to patients in ICUs. Many health-care providers believe that percutaneous endoscopic gastrostomy (PEG) tubes, which are commonly used to deliver EN to terminally ill patients, decrease the risk of aspiration, and prevent or relieve pressure ulcers; however, studies have shown that PEG did not decrease aspiration or pressure ulcer rates at the end of life. 16 It is also reported that PN could be helpful for a patient’s performance status, and patients may prefer PN as their nutrition resource; however, PN is still unethical if it prolongs a patient’s suffering. 16
The purpose of this study was to explore critical care nurses’ perceptions of the withdrawal or withholding of EN and PN at the end-of-life, which is not allowed according to the current law in South Korea. In addition, this study examined whether there were any differences between the nurses’ perceptions of EN and PN. Finally, the degree of agreement regarding whether EN or PN should be legally allowed to be withdrawn or withheld was assessed.
Methods
Setting and Participants
This study was performed in a tertiary training hospital with approximately 2000 beds. Self-report questionnaires were distributed to all the nurses working in adult ICUs, which included a medical ICU, a surgical ICU, a cardiothoracic ICU, a coronary ICU, and an emergency ICU. Of 181 nurses, 144 nurses answered the questionnaires, and the response rate was 79%. Three surveys were incomplete. Ultimately, data from 141 ICU nurses were included in the analyses.
Measures
Attitudes Toward EN and PN
The nurses’ attitudes toward the end-of-life EN and PN were measured using an instrument developed by Lubart, Leibovitz, and Habot. 17 It was translated into Korean using forward- and back-translation procedures by 2 nursing professors who spoke English fluently. One was a board certified nurse practitioner, and the other was a board certified clinical nurse specialist from the United States.
The original instrument consisted of 5 items on EN. 17 This study used these 5 items: (1) EN is an essential tool for feeding, hydration, and medication; (2) EN prolongs suffering and life; (3) we should think about stopping EN; (4) medical staff must make the decision to stop EN; and (5) family must make the decision to stop EN. The current study also used these 5 items to ask about PN after simply changing the term EN to PN. The participants were asked how much they agreed with each item regarding EN and PN at the end-of-life and responded using a 5-point Likert scale: 1 (strongly disagree), 2 (disagree), 3 (neither agree nor disagree), 4 (agree), and 5 (strongly agree).
Attitudes on AN and other life-sustaining treatments under the act on decision on life-sustaining treatment
Participants were asked whether they agreed that the withdrawal or withholding of each treatment should be legally allowed. The first part of the survey asked, “According to the Act on Decisions on Life-Sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life, which is a newly enforced law, the following 4 types of life-sustaining treatments are allowed to be refused for patients at the endoflife. Do you agree with the legal allowance of the refusal of these items inaccordance with the Act?” “According to the Act on Decisions on Life-Sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life, EN or PN is not allowed to be refused for patients at the endoflife. Do you agree that EN or PN needs be included on the list of life-sustaining treatments that can be refused in the Act?”
Ethical Considerations
This study was approved by the institutional review board of the hospital where the study was performed. Participation was voluntary, and small gifts were given as compensation.
Results
Characteristics of the Participants
The socioeconomic characteristics of the participants are shown in Table 1. The mean age was 28.17 ± 4.09 years, and 91.5% of the critical care nurses were female. The participants had an average of 4 years and 9 months of clinical experience. The mean number of dying patients to whom the participants had provided nursing care during the last month was 1.71 ± 2.05.
Characteristics of the Participants (n = 141).
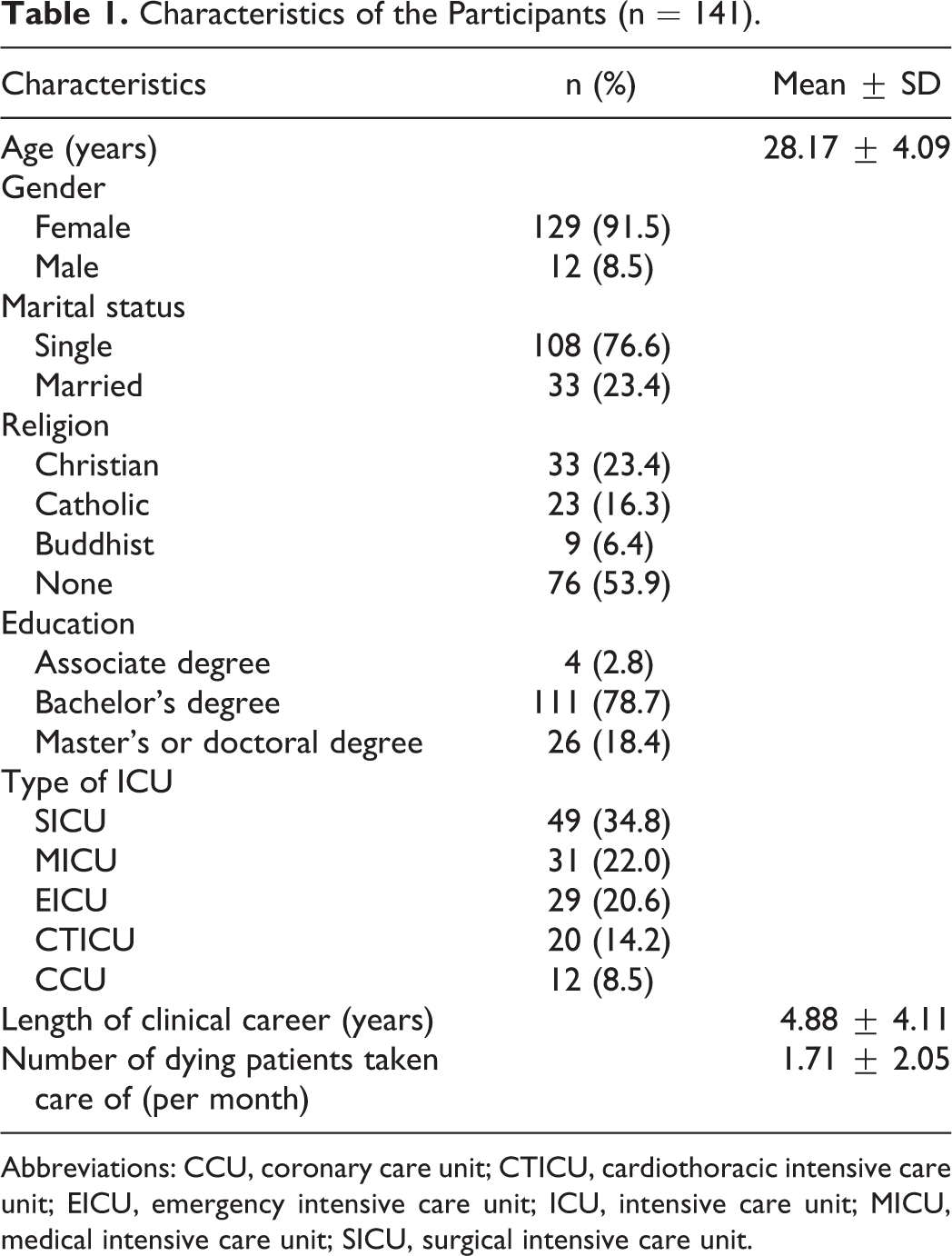
Abbreviations: CCU, coronary care unit; CTICU, cardiothoracic intensive care unit; EICU, emergency intensive care unit; ICU, intensive care unit; MICU, medical intensive care unit; SICU, surgical intensive care unit.
Critical Care Nurses’ Attitudes Toward EN and PN During End-of-Life Care
Nurses’ attitudes about EN and PN during end-of-life care are shown in Table 2. When each of the paired EN and PN items was compared, there were statistically significant differences for all 5 items.
Critical Care Nurses’ Attitudes Toward EN and PN During End-of-Life Care (n = 141).
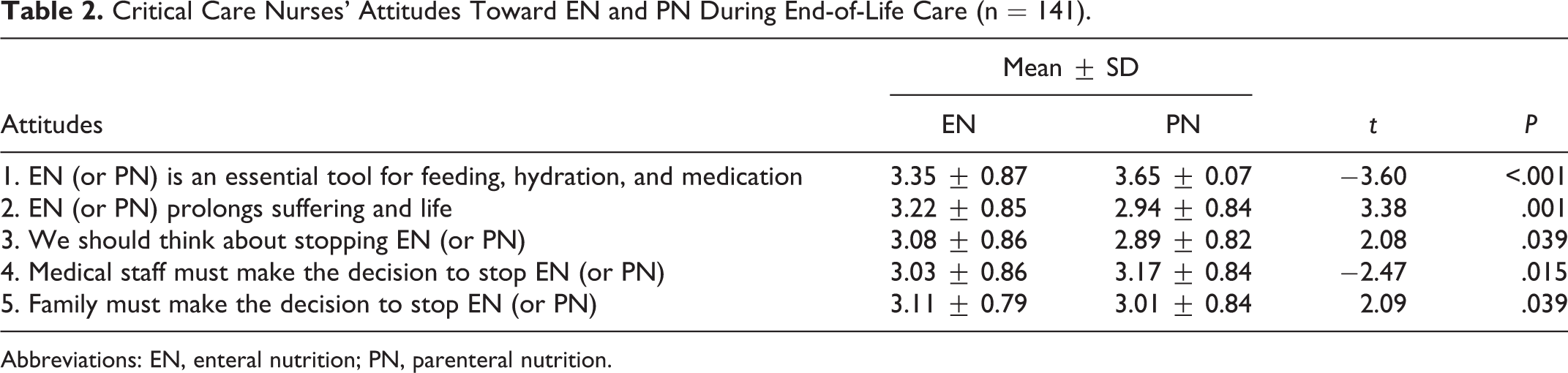
Abbreviations: EN, enteral nutrition; PN, parenteral nutrition.
Factors Associated With Attitudes Toward EN and PN
No factor was significantly associated with attitudes toward EN. In contrast, the number of dying patients cared for per month and the ICU department worked in were significantly related to some items of the nurses’ attitudes toward PN (Table 3).
Differences in Attitudes Toward PN According to Participants’ Characteristics (n = 141).
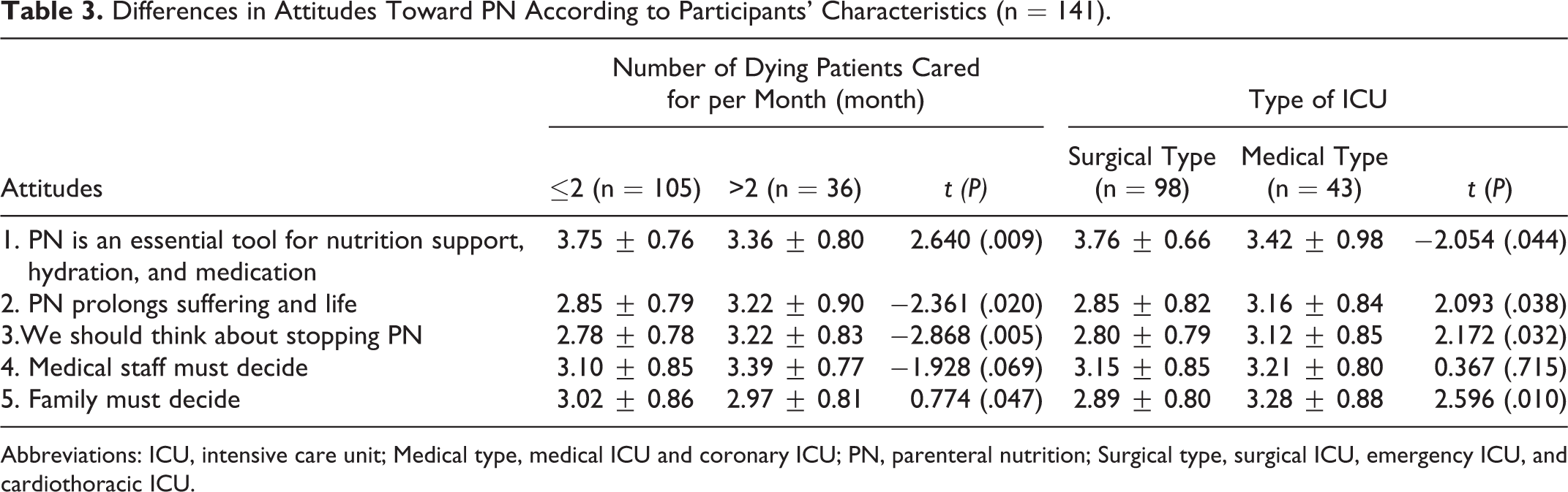
Abbreviations: ICU, intensive care unit; Medical type, medical ICU and coronary ICU; PN, parenteral nutrition; Surgical type, surgical ICU, emergency ICU, and cardiothoracic ICU.
Attitudes Toward AN and Other Life-Sustaining Treatments Under the Act on Decision on Life-Sustaining Treatment
On the first items regarding the newly allowed refusal of life-sustaining treatments, 85.8% agreed or strongly agreed that cardiopulmonary resuscitation became a refusable treatment (Table 4). Moreover, 81.5%, 82.9%, and 66.0% agreed or strongly agreed that hemodialysis, anticancer medication, and ventilator care could be refused, respectively.
Attitudes Toward Artificial Nutrition and Other Life-Sustaining Treatments Under the Act on Decision on Life-Sustaining Treatment (n = 141).
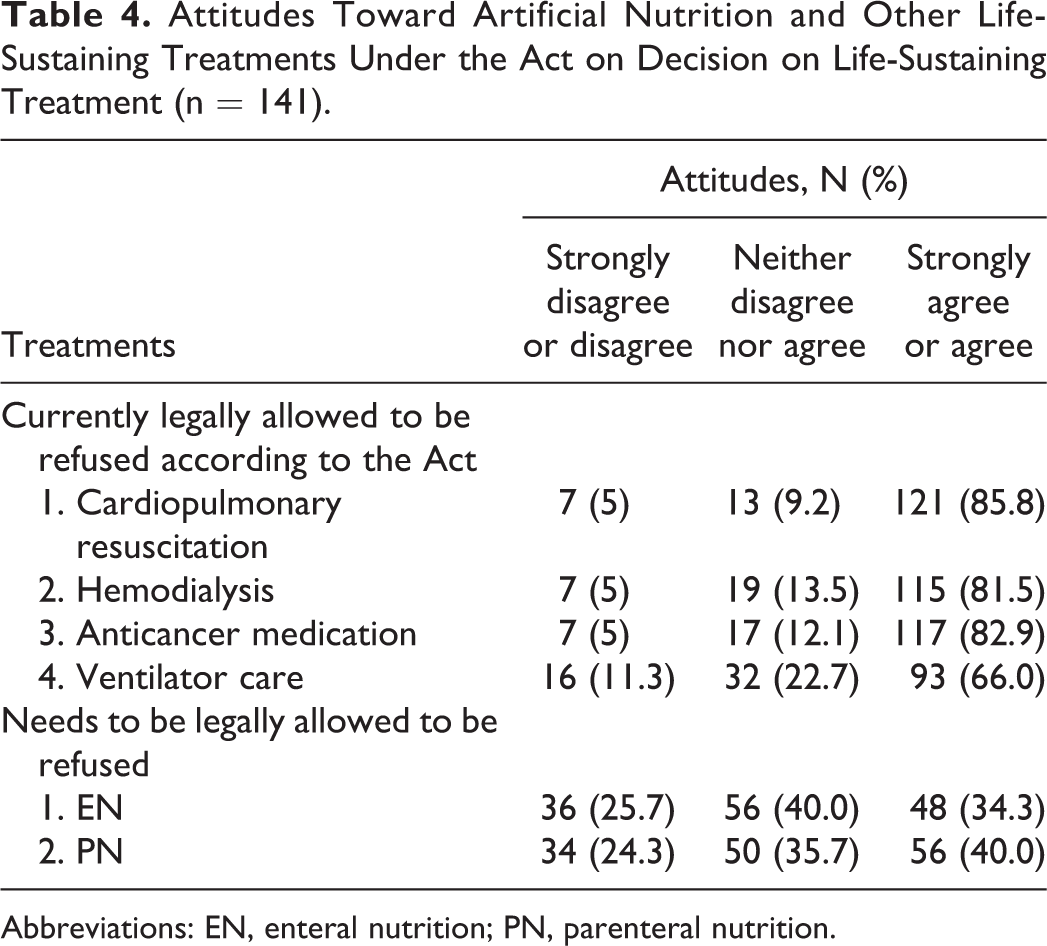
Abbreviations: EN, enteral nutrition; PN, parenteral nutrition.
On the part of the list regarding life-sustaining treatments that cannot be refused, 34.3% agreed or strongly agreed that EN needs to be included on the list of items that may be refused (Table 4). Moreover, 40.0% agreed or strongly agreed that PN needs to be included on the list of items that may be refused.
Discussion
This study described the attitudes of critical care nurses, who care for more patients with life-sustaining treatments at the end-of-life than nurses in any other unit of the hospital, regarding the withdrawal and withholding of AN. In this study, the average score of the responses to the 5 items regarding EN or PN ranged from 3.03 to 3.35 for EN and from 2.89 to 3.65 for PN, based on the 5-point Likert scale. Nurses seemed to show neutral attitudes toward EN and PN. A previous study on nurses conducted by Lubart et al reported a mean score of 4.94 for the item “EN is an essential tool for feeding, hydration, and medication,” 17 while nurses in our study had a mean score of 3.35. Nurses in the study by Lubart et al showed more negative attitudes toward discontinuing EN than nurses in the current study. The reason for the conflicting results could be that Lubart et al focused on dementia patients, while this study focused on terminally ill patients in acute care settings.
Moreover, critical care nurses in this study had more negative attitudes toward stopping PN than EN. When attitudes about EN and PN were compared, more nurses in this study agreed that PN is an essential tool for feeding, hydration, and medication during end-of-life care than those who agreed that EN is an essential tool. In the practice of critical care nurses in this study, AN is not withdrawn or withheld because it is illegal; therefore, critical care nurses in this study are not knowledgeable about or familiar with the international guidelines, as per the guidelines described by the American Society for Parenteral and Enteral Nutrition (ASPEN) and European Society for Clinical Nutrition and Metabolism (ESPEN) regarding the treatment of AN in palliative care. Thus, they might believe that AN is helpful for feeding and hydration to reduce starvation and thirst. The administration of PN alone without EN is common in ICUs, 18 when EN is contraindicated or intolerable for patients. 19 In the current study, some nurses in the ICUs might have perceived PN as a last resort for malnourished patients. In addition, nurses in this study agreed less that PN prolongs suffering than that EN prolongs suffering. Because patients feel more comfortable with PN than EN and prefer PN to EN, 16,20 nurses might perceive that patients given PN suffer less even at the end of life.
The number of dying patients cared for by nurses during the last month and the work unit were factors significantly related to attitudes about PN. Nurses who took care of more dying patients and who worked in medical-type ICUs had more positive attitudes toward discontinuing PN. Patients in medical-type ICUs generally stay in the ICU for more days than those in surgical ICUs and usually suffer for longer durations with chronic diseases. Therefore, nurses in medical-type ICUs experience patients’ suffering more. They have been reported to show more positive attitudes toward the meaning of death and to care more about respecting human life. 21 Nurses in this study who took care of more dying patients and had more experience caring for suffering patients seemed to have more positive attitudes toward the refusal of PN at the end-of-life. Morita et al also reported that physicians who had less experience caring for dying patients were more likely to consider AN to be essential care at the end-of-life. 22 Health-care providers who were more experienced with palliative care were more likely to perceive AN as negatively impacting the comfort of patients in their last days of life. 23
In regard to attitudes toward AN and other life-sustaining treatments under the Act on Decision on Life-Sustaining Treatment, 25.7% of the critical care nurses in this study disagreed that stopping EN needs to be legalized, and 24.3% reported that they disagreed with the legalization of PN refusal. In terms of treatments legally allowed to be refused according to the newly enacted law, 5%, 5%, 5%, and 11.3% of the nurses disapproved of the legalization of the refusal of cardiopulmonary resuscitation, hemodialysis, administration of anticancer drugs, or ventilator care, respectively. Compared to these percentages, the disagreement rate for stopping EN and PN seemed high.
These results may reflect the views of South Korean’s regarding end-of-life nutrition. In a previous study regarding individual’s preferences for their own advance care planning, on a 5-point Likert scale with 1 representing “strongly disagree” and 5 representing “strongly agree,” patients with chronic disease showed a mean score of 2.34 about refusing AN while they showed scores of 3.56 and 3.78 about refusing CPR and ventilation care, respectively. 24 This indicates that they felt less strongly about refusing AN than refusing CPR and ventilation care for their end-of-life care decisions. Moreover, a study on health-care workers regarding their own advance care planning also showed similar results. 25 The reason for this could be that people are not familiar with palliative care practices. Health-care providers, patients, and their family members in South Korea might consider nutrition and hydration to be helpful for patients or consider the refusal of nutrition and hydration to shorten patient’s lives and to be unethical. 26 There has been no empirical study exploring the reasons for Korean people’s preferences regarding AN at the end of life, which could be barriers to the legal and cultural acceptance of AN. Further research needs to examine these features. In addition, there has been no study focusing on South Korean physicians’ perceptions and practice about EN and PN in palliative care. Further studies need to be conducted to describe and compare perceptions among different health-care workers.
On the other hand, even in European countries, decisions on stopping AN have been considered to be more difficult than stopping other life-sustaining treatments. In a study in France on the perceptions of nurses and nurse aids about the withdrawal of AN at the end-of-life, despite the fact that it has been legal in France since 2005, only 59.5% answered that they had encountered situations where the withdrawal of AN was considered. 11 In that study, nurses who were informed about the indications of withdrawing AN were less likely to show ethical difficulty. And further, nurses’ feelings of being uncomfortable, guilty, sense of abandonment of care, or uneasiness were associated with high ethical difficulty regarding the withdrawal of AN.
There is no evidence that PN and EN provide benefits during palliative care. For patients actively dying or in their last days in life, EN or PN increase discomfort. The ASPEN and ESPEN declared that AN is a treatment that patients have a right to refuse according to the ethical principles of autonomy. 8,27 Based on the ethical principles of autonomy, beneficence, non-maleficence, and justice, AN during palliative care needs to be considered the same as other life-sustaining treatments, such as ventilator care, renal replacement, and cardiopulmonary resuscitation. In the last days of a person’s life, he or she should be allowed to refuse insertion of a feeding tube or an intravenous line in the same way that use of a ventilator may be stopped. The right of a patient to request removal of an EN tube or a PN line at the end-of-life should be respected. Anecdotal reports of suffering patients in ICUs who asked nurses to let him/her leave peacefully without any tubes in have been reported in South Korea. 28 An elderly lady’s desire to take all the tubes out and drink a glass of cold juice before dying could not be granted under the current law in South Korea.
Discussions about establishing laws to support the withdrawal and withholding of AN should be begun to protect patients’ rights of autonomy. In this study, 3 of 4 critical care nurses reported at least neutral opinions or agreed that refusal of AN should be legally allowed, while just 1 of 4 disagreed. However, stopping AN is not even discussed in public yet. Health-care providers should be knowledgeable about this issue and should be actively involved in legalization. Moreover, in this study, critical care nurses who had more experience caring for dying patients had more positive attitudes about stopping AN at the end of life. Nurses and physicians in ICUs need more opportunities to be involved in learning the approaches to palliative care and facts about AN in palliative care. A lack of health-care provider education is one of the major barriers to the appropriate practice of AN withdrawal. 16 Specifically, in this study, there were differences between critical care nurses’ perceptions of EN and PN. Education about AN needs to include the aspects that are different between the use of EN and PN in palliative care.
Conclusion
In South Korea, the withdrawal and withholding of life-sustaining treatments during palliative care have become legal due to the enactment of a new law. However, AN is not considered a medical treatment that can be refused. Critical care nurses in this study had neutral attitudes toward each issue surveyed regarding EN and PN because they were not familiar with stopping AN. Nevertheless, nurses who agreed with the legalization of stopping EN and PN at the end-of-life outnumbered nurses who disagreed. There should be active public and clinical discussion about this issue in South Korea.
Footnotes
Authors’ Note
All authors (Ms Seol, Professor Koh and Professor Kim) participated each of the following steps together: designing the study, collecting the data, analyzing the data, preparing the manuscript, and approving the final version for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.