
Abstract
Background:
There is a growing movement to increase palliative care consults from the emergency department (ED) to reduce healthcare costs and improve quality of life. The surprise question is a screening tool that emergency medicine physicians may be able to use towards achieving this goal.
Objective:
The objectives of this study were to increase awareness of hospice and palliative care medicine (HPM) among emergency medicine (EM) providers and to evaluate whether this heightened awareness increased palliative care consults among participating emergency medicine providers.
Methods:
We conducted an anonymous convenience sample survey and two educational interventions about HPM including the surprise question among emergency medicine resident and attending physicians at a large urban public academic quaternary care center from July to November 2018. A report of palliative care consults ordered between August 1, 2017 and January 1, 2019 was generated from the electronic health records used by the hospital. The number of palliative care consults made before and after the educational intervention was compared.
Results:
After the first educational intervention centered on the surprise question, palliative care consults from the ED increased from an average of 2.25 per month (range 0 to 8, SD: 2.38) to 12.67 per month (range 9 to 19, SD: 4.01, p < .001).
Conclusion:
Educating EM physicians about the surprise question can increase the number of palliative care consults from the ED, thereby potentially improving patient care and decreasing costs by avoiding unwanted healthcare interventions.
Introduction
The emergency department (ED) is the location where most patients, including the terminally ill, seek urgent and emergent care. 1 Frequently, the ED is the primary setting where terminally ill patients receive treatments such as intravenous pain medications, antimicrobial therapy, and diagnostic imaging. However, there has been a movement in the emergency medicine (EM) community to improve clinical practice in terms of palliative and end-of-life care. 2 As our nation ages, an ever-increasing number of people will die from chronic conditions after a period of years, where they suffer from frailty, morbidity, dementia, and organ failure. 3,4 Those numbers of people do not even include those suffering from the heavy burden of cancer.
Every day our EDs are becoming more crowded and costs are escalating. Emergency department care is a major component of increasing expenditures of end-of-life care due to several factors including invasive life-sustaining measures. 5 The EM community is moving away from automatically performing acute aggressive interventions for terminally ill patients. Instead, there is a shift toward patient-goal assessments and identifying patients in the last stages of life, prioritizing symptom management, noncurative treatment, and quality of life. 1 Therefore, the ED is strategically placed to help reduce health-care costs and improve quality of life by addressing any unmet palliative care needs.
Palliative care is the branch of medicine that deals with the relief of symptoms that can negatively impact the quality of life for patients with life-threatening illnesses. 6 For patients with these ailments, the management of noncurative treatment is an important part of their care. Palliative care does not seek to impede curative treatment for life-threatening illnesses. 1 Rather, it seeks to help provide constant reevaluations of life-prolonging curative treatments, especially when those treatments no longer prolong life. Other goals include avoiding sustained suffering, improving symptom management, and supporting caregivers.
Unfortunately, physicians have shown reluctance to incorporate palliative care into their practice. 7 Particularly, physicians have failed to identify and refer patients to palliative care even when appropriate. One reason for the lack of referrals to palliative care services is the lack of an easily accessible screening tool to identify patients with unmet palliative care needs. 8 In the ED, little emphasis is sometimes placed on the identification and management of palliative care needs. Also, there is a lack of hospice and palliative medicine (HPM) education during EM residency and medical education in general. 9,10
For patients over 65 years of age, nearly 75% visited the ED in the last 6 months of life and 51% visited the ED in their last month of life. In addition, for those patients who visited the ED in the last month of life, 77% were admitted and of those, 68% subsequently died during their admission. 11,12 Therefore, the ED is an ideal place where EM physicians can identify which patients would benefit from palliative care consultation. 13 By shifting to palliative treatment, EM providers hope to improve quality of life for patients while decreasing health-care costs. 14,15
The surprise question (SQ) “Would you be surprised if this patient died in the next 12 months?” is one tool that has been used in a variety of populations to seek out appropriate patients for palliative care. The SQ has been shown to be effective in identifying end-stage renal disease and patients with cancer who are at an increased risk of mortality 16,17 and has been used in the emergency, primary care, and inpatient settings. 8,18,19 Though previous studies have shown that the SQ can easily be used by ED providers, it has not been validated as a method to increase the number of palliative care consults for patients in the ED. 8,18
With this in mind, we set out with 2 goals. The first was to create a short educational intervention centered around the SQ to increase knowledge about palliative care for our EM practitioners. The second was to test if this educational intervention would lead to an increase in palliative care consults requested from our ED.
Methods
Study Design and Population
We conducted an anonymous convenience sample survey of EM resident and attending physicians from July to November 2018. The survey and educational intervention were performed at a large urban academic public quaternary care center with over 90 000 adult ED visits annually. The EM residency is a 3-year program with 15 residents per year. Didactic curriculum includes end-of-life discussions, goals of care, and palliative care. The study was approved by the institutional review board of the hospital.
Institutional Palliative Care Consult Procedure
Institutional procedure for consulting palliative care for admitted patients was informal. Hospital palliative care teams include physicians, nurse practitioners, fellows, clergy, and social workers. The EM physicians can consult palliative care from the ED. There are no formal hospital criteria for when to consult palliative care. Prior to the study, physicians did not receive formal education or guidance on the early identification of eligible patients. The decision of whether to involve palliative care was at the discretion of the provider. After discussions between the departments of EM and HPM, the consensus chosen to consult palliative care for admitted patients was for the EM physician to decide whether to answer “No” to the SQ.
Educational Intervention
To implement the SQ in helping EM physicians identify patients appropriate for palliative care consultation, we created an educational intervention that consisted of a 15-minute PowerPoint presentation module (Supplement 1) centered on the definition and application of the SQ. We also included information about the universally recognized hospice criteria of 6 months or less left to live 20,21 and the American College of Emergency Physicians (ACEP) Choosing Wisely campaign, which recommends the involvement of hospital palliative care services from the ED when appropriate. 22 Similar information was disseminated in weekly e-mails to physicians and staff about the SQ and HPM criteria after the educational intervention.
On August 17, 2018, we informally presented the educational intervention during resident didactics as part of the regular curriculum. This session did not include a pretest or posttest. In October 31, 2018, we formally presented again the educational intervention to both residents and attending physicians. On November 7, 2018, we presented the educational intervention to the remaining attending physicians who were not present at the initial intervention. For the two latter formal presentations of the educational intervention, we performed a pretest and posttest. In addition, we began to distribute information to EM physicians about the definition of the SQ and how to use it to identify patients appropriate for palliative care.
Survey Content and Administration
To measure change in knowledge and attitudes in relation to the SQ and HPM, a survey developed from a literature review using current information from EM and HPM was administered before and after the educational interventions. Surveys were labeled as either “Pretest” or “Posttest” and were identical (Online Appendix A). Participants were asked to anonymously respond to inquiries about demographics, comfort with disease prognostication, knowledge about HPM criteria, ACEP Choosing Wisely campaign, and the SQ.
Palliative Care Consults
Our institution uses Cerner Millennium electronic health records (EHR). All specialty consultations must be ordered via the EHR and are trackable by date, practitioner, and location. Consults may be ordered by both resident and attending physicians. A report was generated for all HPM consultations from the ED dated August 1, 2017, through January 31, 2019.
Results
Palliative Care Consults
The number of palliative care consults from July 1, 2017, to Aug 1, 2018 (before the first educational intervention) averaged 2.25 per month (range: 0-8, standard deviation [SD]: 2.38). From August 1, 2018, to Jan 31, 2019 (during and after the educational interventions), the number of consults increased to an average of 12.67 per month (range: 9-19, SD: 4.01). There was a significant increase in the number of palliative care consults placed by EM providers after the educational intervention (P < .001, 2-tailed t test performed in Excel, Figure 1). For an analysis of the survey results, we used descriptive statistics to evaluate our findings (Table 1). For the number of pretest and posttest responses, we received 46 and 43 responses, respectively. The number of responses decreased between the pretest and posttest survey because 3 respondents had to leave prior to completing the educational intervention.
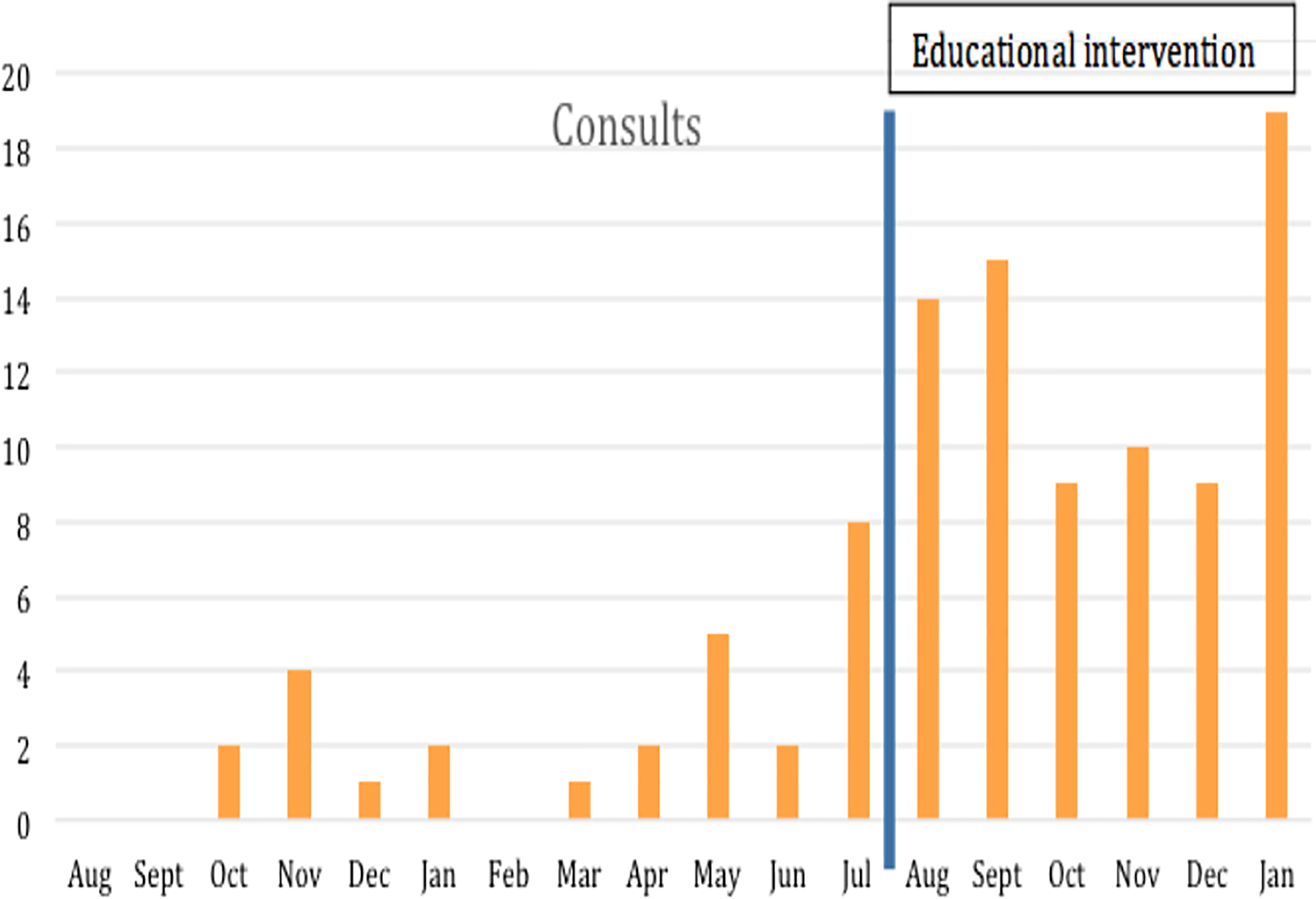
Number of ED-based palliative medicine consults, before and after initiation of educational interventions. ED indicates emergency department.
Pre/Post-Test Survey Questions and Results.
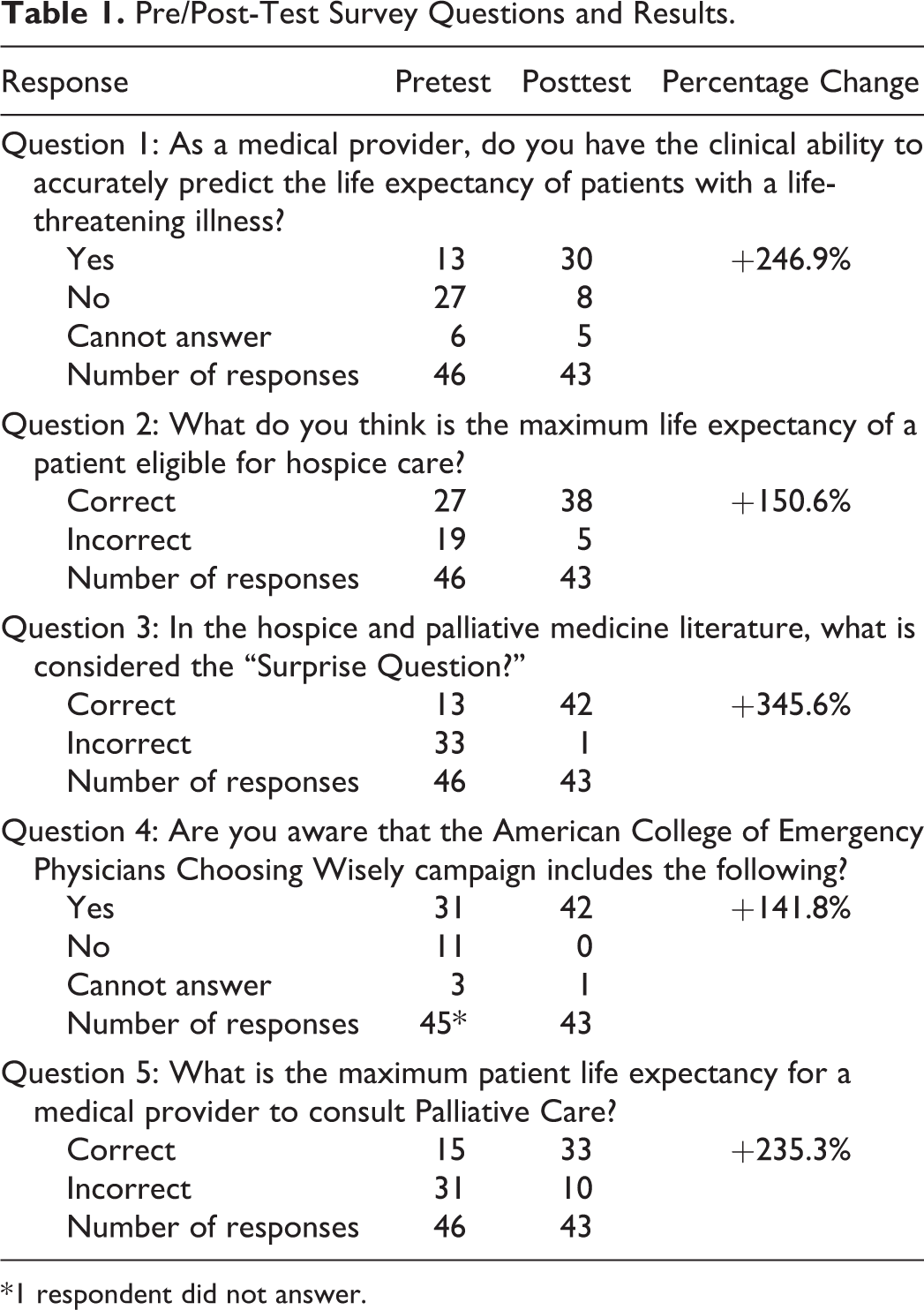
*1 respondent did not answer.
Regarding EM physician attitudes toward determining disease trajectory, we found that just under a third of respondents felt they were qualified to do so (28.2%, 13/46). After the intervention centered around the SQ, more than two-thirds of EM physician believed that they could determine disease trajectory (69.8%, 30/43). In terms of knowledge about the 6-month estimated life expectancy for hospice referral, most EM physicians knew that information (58.7%, 27/46). After the educational intervention, there was a 150.6% increase (88.4%, 38/43).
To gauge awareness of the SQ among EM physicians, only a minority could correctly identify the definition of the SQ (28.3%, 13/46). After the educational intervention, the percent of respondents who could accurately identify the definition of the SQ more than tripled (97.7%, 42/43). Regarding the ACEP Choosing Wisely Campaign, the majority of respondents expressed familiarity (68.9%, 31/45; 1 respondent did not answer). After the educational intervention, there was a 141.8% increase (97.7%, 42/43).
For institutional awareness about appropriate life expectancy for inpatient consults to palliative care, only a minority of respondent physicians knew it was 12 months of life or less (32.6%, 15/46). After the educational intervention, knowledge about the institution life expectancy guideline for inpatient consults to palliative care more than doubled (76.7%, 33/43).
Discussion
The SQ is a useful instrument for finding eligible patients in the ED because it simply asks physicians to determine if they would be surprised if their patient were to die in 12 months. So that patients can benefit most from palliative care, it becomes important to recognize these patients early on in their hospital stay. The increase in palliative care consults straight from the ED at the time of admission can better help plan for the deterioration of disease process through instruments such as do not resuscitate/do not intubate and physician orders for life-sustaining treatment/medical orders for life-sustaining treatment. 23 Since HPM has been shown to decrease hospital lengths of stay and increase quality of life, the identification of eligible patients from the ED at the time of admission allows EM physicians to contribute to and improve the overall process. 24,25,18
Our pretest survey results showed that our EM physicians did not uniformly feel that they were qualified to determine disease trajectory. This is somewhat surprising since EM physicians are trained to determine “sick or not sick” and assess acuity. Part of that feeling of uncertainty may stem from the lack of palliative care training in residency programs. 9,26 One solution could be to incorporate more palliative care instruction into EM education. Our study suggests that by simply educating EM physicians about the SQ and HPM, we were able to increase their perceived ability to determine life expectancy, leading to a statistically significant increase in ED-generated palliative care consults.
Nonetheless, there are shortcoming to the SQ. In one study of primary care physicians, the SQ did not accurately predict death in 1 year. 27 Yet, a “No” response to the SQ has been shown to be significantly associated with mortality in 1 year. 16,17 When the SQ is combined with other validated prognostic indicators for mortality, it can become a valuable tool in the ED to increase the demand for palliative care consults subsequent to an ED visit. 28 Emergency medicine physicians need to feel comfortable and qualified to broadly determine life expectancy in the ED in order to consider the SQ in their clinical practice. There remains work to be done in educating EM physicians about the basics of HPM and its application in the ED.
Our study did not consider terminally ill patients who were discharged from the ED. The educational intervention did not address outpatient referral to palliative care for discharged patients. Outpatient palliative medicine services are an integral part of improving quality of life for chronically ill terminal patients. Future studies may address strategies to increase outpatient referrals to palliative care from the ED.
Limitations
Several limitations should be considered when interpreting this study. Our intervention was performed at one academic center with a focus on educating and enhancing the palliative care services for patients admitted through the ED; our findings may not reflect the experiences at other institutions. Survey tools used were informal, and as such tool reliability and validity are unknown, and there was no blinding or randomization of the study. Finally, the number of palliative care consults was counted in a 6-month timeframe after the educational intervention was performed. Due to the unpredictable nature of knowledge retention, it is unknown if the significant increase observed will be sustained over time. Despite these factors, we still believe that our study shows a useful snapshot of the effectiveness in educating EM physicians on the SQ and HPM.
Conclusion
The early identification of patients with unmet palliative care needs in the ED is crucial to improving quality of life and can make a real difference in their goals of care. Our research suggests that educating EM physicians about the use of the SQ can increase the number of ED driven palliative care consults. By increasing palliative care consults, we can assess any unmet needs for terminally ill patients during their inpatient stay. It is conceivable that these consults from palliative care can help decrease costs by avoiding unwanted health-care interventions and improve patient care holistically. Though imperfect, the SQ is a tool that can easily be taught to EM physicians and can increase ED-initiated palliative care consults. Additional research will be required to evaluate its predictive value across the ED and how to help EM physicians determine disease trajectory.
Supplemental Material
Supplemental Material, -Appendix_1_survey_xyz213152cf144b4 - Would You Be Surprised if This Patient Died in the Next 12 Months? Using the Surprise Question to Increase Palliative Care Consults From the Emergency Department
Supplemental Material, -Appendix_1_survey_xyz213152cf144b4 for Would You Be Surprised if This Patient Died in the Next 12 Months? Using the Surprise Question to Increase Palliative Care Consults From the Emergency Department by Henry Zeng, Paul Eugene and Mark Supino in Journal of Palliative Care
Supplemental Material
Supplement_1_slides_xyz21315f13cbfbe - Would You Be Surprised if This Patient Died in the Next 12 Months? Using the Surprise Question to Increase Palliative Care Consults From the Emergency Department
Supplement_1_slides_xyz21315f13cbfbe for Would You Be Surprised if This Patient Died in the Next 12 Months? Using the Surprise Question to Increase Palliative Care Consults From the Emergency Department by Henry Zeng, Paul Eugene and Mark Supino in Journal of Palliative Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.