
Abstract
Purpose:
Caregivers of patients with cancer cope with socioemotional challenges, which can adversely affect their well-being. We developed an intervention, expressive writing and reading (EWR), to promote emotional processing and social connectedness among caregivers. In a single-arm pilot study, we assessed its feasibility and perceived usefulness.
Methods:
Caregivers participated in weekly 1.5-hour EWR workshops offered over 20 weeks. After 4 sessions, they completed semistructured interviews, which were analyzed using qualitative descriptive analysis.
Findings:
Of 65 caregivers approached, 25 were eligible, 18 consented, and 9 (50%) caregivers completed at least 4 workshops and the interview. Their responses revealed 3 themes: “inner processing,” “interpersonal learning,” and “enhanced processing and preparedness.” Perceived benefits of EWR included emotional and cognitive processing (individual and collaborative), learning from the emotions and experiences of other caregivers, and preparing for upcoming challenges.
Conclusions:
Expressive writing and reading can be a safe and cost-effective supportive intervention for caregivers of patients with cancer.
Introduction
In 2012, there were 14 million new cancer diagnoses worldwide. 1 With the rate of survival increasing, significant caregiving responsibilities are being transferred to informal caregivers who are usually spouses, adult children, friends, and relatives of the patients. 2 These caregivers are tasked with managing medications, symptoms, and distress. 3 They often face social, physical, and psychological challenges, which can take a significant toll on their health. 4 -6 Up to 35% of family caregivers experience depression and anxiety 7 and feelings of helplessness, hopelessness, and anticipated loss and grief. 4,8 For this reason, caregivers have been recognized as “second-order patients,” who should be receiving supportive care. 9
The distress experienced by caregivers may be in part related to isolation and inadequate social support. 10,11 Loneliness is common to patients with cancer and their caregivers, but as compared to patients, caregivers report feeling less socially and emotionally supported by their families and health-care professionals. 11,12 Caregivers express a desire for increased communication and support from their social networks. 13 Social support may be particularly important in the final stages of illness, when the burden of caregiving is accompanied by the stress of preparing for bereavement and anticipating loss. 12 Unfortunately, few family care services have been incorporated into clinical oncology settings. 5 There is a need for safe and cost-effective interventions to support caregivers in their difficult journies. 14,15
One existing psychosocial intervention that may address this need is expressive writing (EW). Expressive writing involves sessions of solitary and unconstrained writing about personal experiences and life events. 16 Expressive writing promotes emotional and cognitive processing when writers articulate and explore their thoughts and feelings. 17 -19 Despite small effect sizes, it has been associated with improved well-being and various health-related outcomes in different samples (for a meta-analysis, see the study by Frattaroli 20 ). Importantly, it is simple and implemented with minimal clinician intervention, making it a cost-effective strategy to enhance well-being. 21 -24
Concerns about loneliness and social isolation among informal caregivers 11 suggest that enhancing EW with a social component may be useful. In samples of general practitioners and nurses, reflective writing and sharing in a group setting has been found to promote a sense of community and personal exploration. 25 Such an intervention may provide social and emotional support for caregivers of patients with cancer, allowing them to foster connections with others experiencing similar challenges.
Caregivers of patients with cancer report being open to participating in structured support programs led by professionals. 13 However, it is unclear whether an EW intervention with a social component is feasible to implement and useful for this sample. To address this issue, we developed an Expressive writing and reading (EWR) intervention, characterized by professionally facilitated group writing and sharing. This intervention involved weekly sessions of EW and a novel sharing component where caregivers read their writing out loud and received feedback from group members. In a pilot study, we evaluated caregiver experiences with EWR. We report findings from qualitative interviews conducted with 9 caregivers who completed 4 or more EWR workshops.
Methods
Participants
Study recruiters approached caregivers in waiting rooms of a comprehensive cancer treatment hospital in a large Canadian city, and they distributed brochures and posters. The study was described as a group workshop for family and friend caregivers of patients with cancer, focusing on a writing technique to help reduce distress and promote well-being. Participants were asked to attend a minimum of 4 workshops at the hospital. Eligible individuals were 18 years of age or older, able to read and write in English, and caring for a patient with cancer treated at the hospital. Exclusion criteria included a self-reported diagnosis of acute mental illness, loss of a close loved one within 6 months of study participation, an unwillingness to attend at least 4 EWR sessions, or an unwillingness to receive and provide feedback in a group setting. Prior to the first workshop, participants were notified by telephone of all workshop dates and provided basic demographic information (Table 1).
Characteristics of Caregivers Who Attended At Least 4 EWR Workshops (n = 9) and of the Patients They Cared for (n = 9).
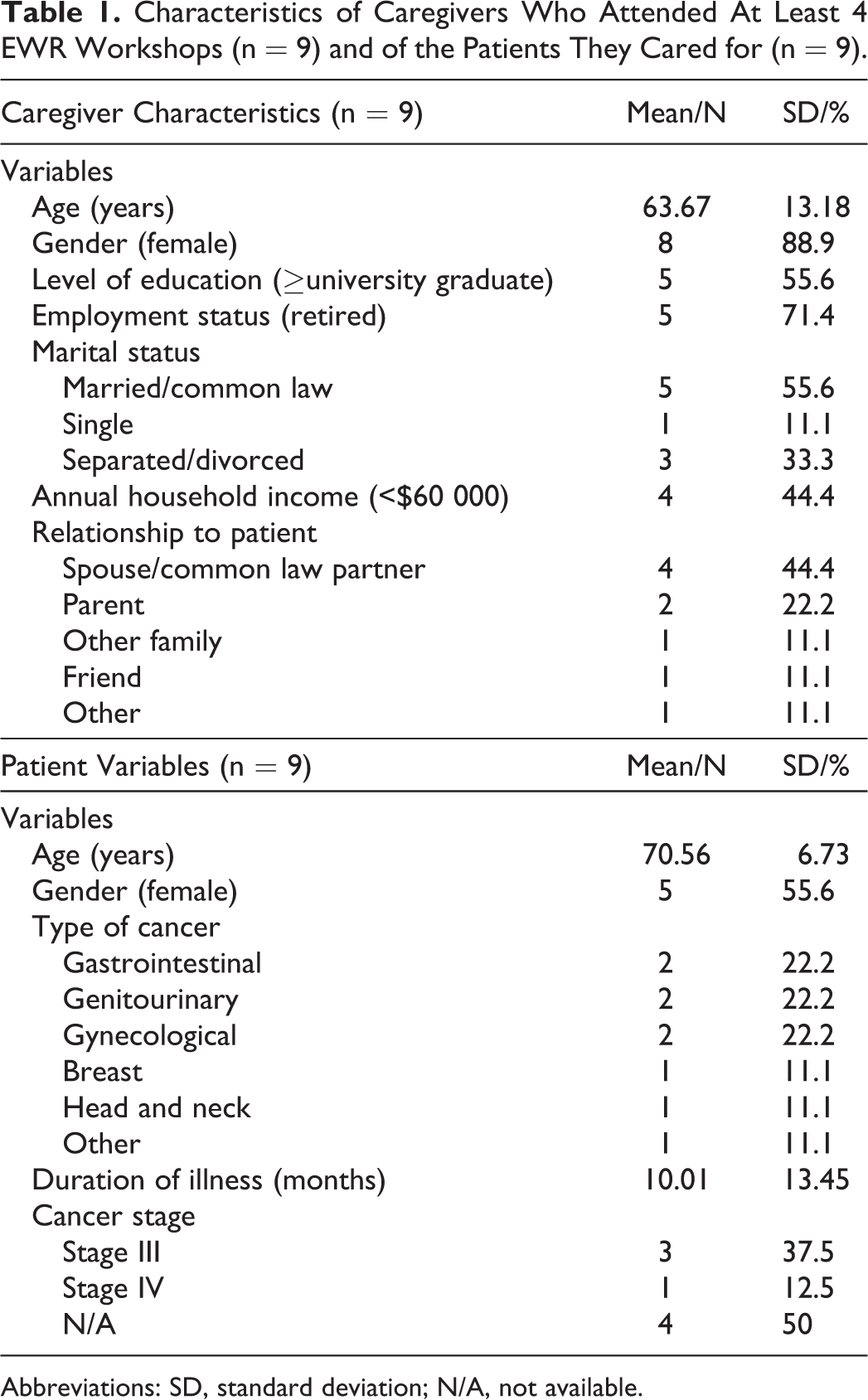
Abbreviations: SD, standard deviation; N/A, not available.
Ethics
This study was approved by the University Health Network’s Research Ethics Board, and all study procedures were performed in accordance with this institution’s ethical standards. Written informed consent was obtained from all individual participants included in the study.
The EWR for Caregivers Workshop
Two psychiatry residents (M.A.H., P.U.) trained in narrative-based intervention, 26 with experience in EW and group therapy, conducted the workshops. They cofacilitated 1½-hour weekly EWR groups at the hospital supervised by a staff psychiatrist (A.P.) from a different hospital.
Each group included 4 to 8 caregivers, and one of the residents was designated as the group leader. At the beginning of each session, the group leader provided instructions for writing. Participants were told that they would be writing about a prompt, and they were instructed to “really let go and explore their very deepest emotions and thoughts” 16 (full instructions are provided in Appendix A). Participants were then assigned writing prompts that were not all specific to cancer. Some prompts were vague and either positive (eg, “describe a happy family memory”) or negative (eg, “describe your worries”). Others were specific to caregiving (eg, “describe a highly meaningful event in caregiving”; Appendix B). After being assigned a prompt, participants brainstormed for 5 minutes and then wrote freely for 20 minutes. After writing, each participant was asked whether they would be willing to share their writing with the group.
Sharing was always voluntary, and usually one or two participants agreed to read their writing out loud. The rest of the session was dedicated to sharing interpretations, thoughts, and feelings about the writing. The reader was instructed to listen to the discussion for 15 minutes without responding or commenting, to allow a free flow of ideas. Afterward, the reader was reinvited to address concerns and questions raised by the group.
Qualitative Interviews
Y.W.L. conducted hour-long qualitative interviews with participants who completed 4 or more EWR workshops (Appendix C contains the interview questions). The interviewer began by asking participants what they expected from EWR. Next, the interviewer inquired about aspects of the session, such as the experience of writing, sharing, and listening to others. At the end, participants offered additional comments and suggestions to improve the workshop.
Qualitative Data Analysis
The qualitative interviews were analyzed using a modified version of the Qualitative Descriptive Method. 27 To preserve the integrity of each story, transcripts were read multiple times to outline summaries for each individual case, which included remarkable and distinctive elements. Concept maps and session notes were used to aid concept organization and topic development. As topics emerged, we validated each by returning to each case to look for evidence. Finally, a thematic profile was created to describe the overall story of the studied phenomenon that was representative of all cases.
Results
Response Rates
A total of 65 caregivers were approached over an 8-month period from 2014 to 2015, and 4 responded to the posted brochures and flyers. Five individuals were deemed ineligible as they did not answer phone calls from the research staff, 13 did not return telephone calls, and 22 had scheduling conflicts. Among 25 eligible caregivers, 18 (72%) consented to the study, 15 (83%) of 18 participated in at least 1 workshop, and 9 (50%) participated in at least 4 workshops and completed a postworkshop interview. Two of these 9 participants attended 4 workshops, 2 attended 6, and 5 attended 8 or more workshops. We called participants who attended less than 4 workshops to inquire about their absence, and most reported not attending due to a scheduling conflict.
Qualitative Findings
Two overlapping themes emerged from our qualitative analysis of interviews with participants (depicted in Figure 1). The first theme, “inner processing,” referred to emotional and cognitive processing typically derived from the EW component of the workshops. The second theme, “interpersonal learning,” described the ways participants learned from others during group sharing. The intersection of these 2 themes produced a third theme, “enhanced processing and preparedness.” This theme describes benefits related to the combined impact of writing and sharing, such as gains in insight and preparedness for the future. These themes are detailed below.
Thematic structure of responses from qualitative interviews with participants.
Inner Processing
The first theme describes EWR’s provision of a safe space for participants to release, process, and reflect on their caregiving experiences. These experiences often involved sadness, anger, or fear of the unknown. For some participants, reflecting on the challenges of caregiving was overwhelming and produced negative feelings or exhaustion that lingered in the days following EWR (Table 2). However, these lingering sensations may reflect cognitive processing or attempts to “understand, evaluate, or figure out” the negative emotions explored in the workshop (Table 2). Participants noted that writing was particularly helpful in promoting emotional and cognitive processing. It allowed participants to contextualize their experiences as having “a beginning, middle, and end” (Table 2). Participants mentioned that writing organized and clarified their inner states, which helped them recognize meanings and patterns in their thinking (Table 2). For some, writing was an opportunity to resolve a challenge, gain a new perspective, or achieve self-discovery (Table 2). For another participant, it simply provided a silent moment to accept her mother’s illness (Table 2). Overall, writing and reflecting allowed participants to concretely explore and process their emotions and thoughts. Although this aspect of EWR was often difficult or unpleasant, it yielded benefits such as clarity, insight, and self-awareness.
Three Themes Emerging From Qualitative Interviews About EWR and Supporting Quotes.
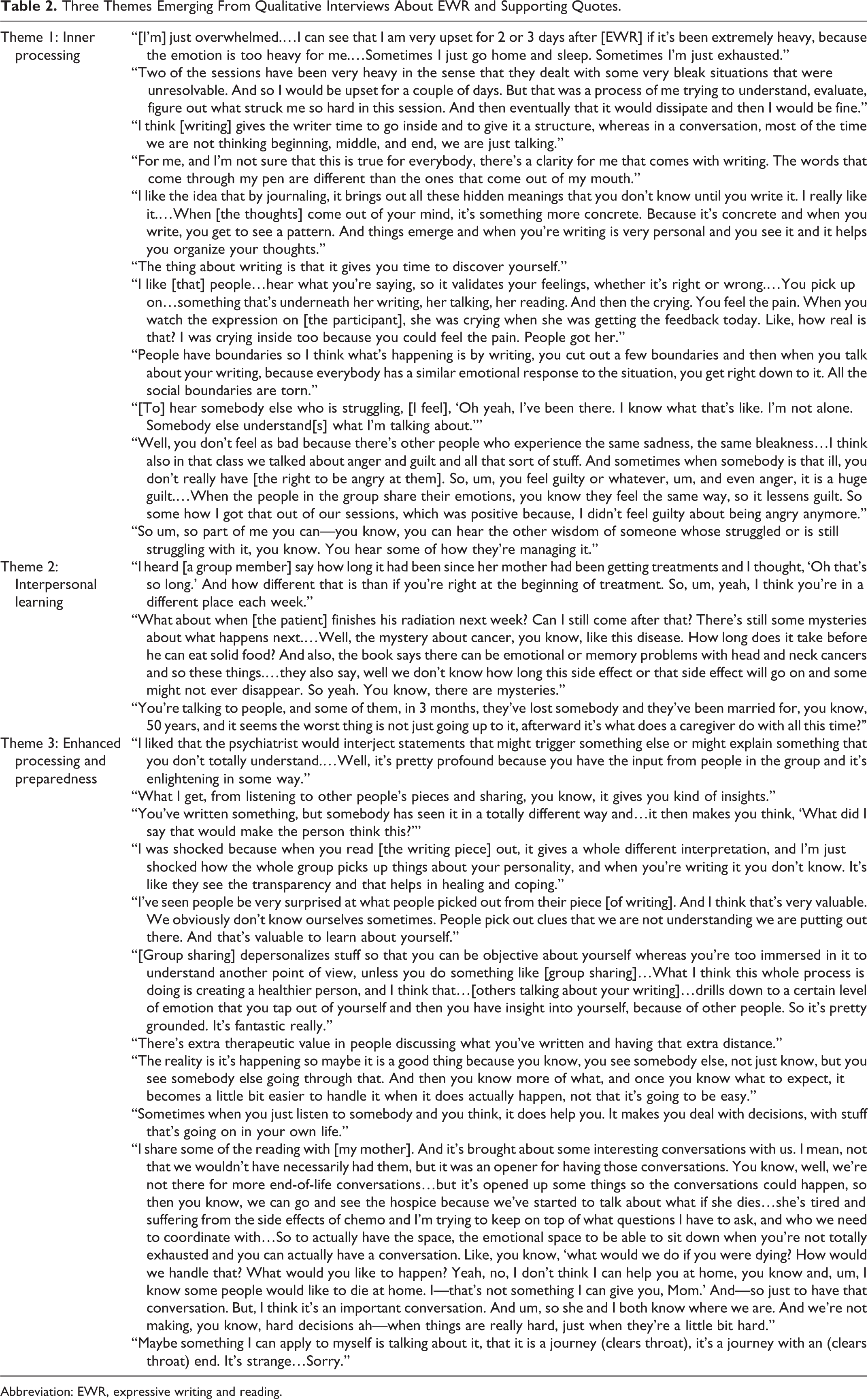
Abbreviation: EWR, expressive writing and reading.
Interpersonal Learning
The second theme captures participant feedback on group sharing, which is the novel component of the study’s intervention. By listening and empathizing with other caregivers, participants removed “social boundaries” and fostered a sense of connectedness and community (Table 2). Importantly, participants learned that others felt the same way they did, which validated their emotions. One participant took comfort in knowing that like her, other caregivers felt guilty about being angry (Table 2). Group discussions also allowed caregivers to exchange practical information. Participants benefitted by learning from the “wisdom” of others and seeing “how they were managing (the caregiving experience)” (Table 2). This learning not only occurred through the explicit exchange of strategies and advice. Considering the experiences of others who were at different stages of the caregiving experience offered a glimpse into the past or future. Participants could reflect on their early caregiving experiences, as well as gain insight into what may happen next, which helped them cope with the “mysteries of cancer” (Table 2). Group discussions provided an opportunity for participants to contemplate bereavement and what they might expect following the death of a loved one, such as the possibility that they may struggle with the sudden onset of free time (Table 2). Overall, the group component of EWR not only provided social and emotional support, it seemed to promote various forms of interpersonal learning among group members as well.
Enhanced Processing and Preparedness
In the qualitative interviews, participants described experiences with EWR that reflected an overlap between the 2 abovementioned themes (Figure 1). Combining inner processing and interpersonal learning allowed participants to gain a better understanding of themselves. Feedback from others provided a different lens or interpretation on participants’ writing. Based on this feedback, participants gained insights into aspects of their personalities and experiences that were previously overlooked (Table 2). These insights were identified as being “profound” and valuable for their health and the process of healing and coping (Table 2).
One mechanism by which insight or processing may have been enhanced in a group setting is depersonalization. Expressive writing and reading seemed to temporarily remove participants from their typical state of being, which was immersed in the day-to-day responsibilities and difficulties of caregiving. By distancing themselves from their own experiences, participants adopted a different or objective view, which appeared to have “therapeutic value” (Table 2).
Focusing on others was also useful in preparing participants for further caregiving challenges, such as end-of-life care and bereavement. Participants described how they applied what they learned about themselves and others during EWR into aspects of their lives, such as handling decisions (Table 2). Writing and sharing seemed to prompt caregivers to consider the future and take preparatory action earlier than they otherwise would have. One participant noted that seeing another caregiver struggle with a difficult stage of caregiving helped manage her expectations for upcoming caregiving experiences (Table 2). Another participant shared what she wrote during workshops with her mother as an opportunity to discuss end-of-life care. The stress and demands of her mother’s illness interfered with important conversations about the future, so this participant used EWR to initiate discussions about the logistics of her mother’s ongoing care. In this way, EWR helped her prepare for the future sooner, so she would not be making “hard decisions when things are really hard, just when they’re a little bit hard” (Table 2). Simply being exposed to discussions about late stages of caregiving and bereavement seemed to initiate emotional processing for participants who were not ready for these topics. One participant noted that although he knew his wife would pass away, he was not ready to talk about it with his family or even in his writing. However, he applied group discussions to his own experiences in acknowledging that his caregiving journey, like the journey of many others, will inevitably end (Table 2).
In sum, writing and sharing during EWR may have enhanced participants’ emotional and cognitive processing, perhaps by way of depersonalization. One aspect of this processing involved anticipating future challenges, such as the logistics of end-of-life care or the emotional impact of loss.
Suggestions for Improvement
Six of 9 participants offered their suggestions for improving the EWR workshop. Consistent with a low completion rate, caregivers expressed difficulties in accommodating EWR into their schedules. Suggestions to address this issue included offering EWR online, completing writing at home to allocate more time at group meetings for sharing and discussion, or sharing only parts of writing, such as a particularly evocative sentence, thought, or emotion. Another concern related to improving EWR’s accessibility for non-native English speakers. Strategies to increase accessibility involved an option for caregivers to complete EW in another language and displaying EW prompts visually or providing them ahead of time to allow for idea percolation. There was also a concern that some EWR workshops might be too heavy and emotionally exhausting for participants (Table 2). One caregiver suggested ending each workshop with a positive activity, such as sharing jokes or anecdotes, to help dissipate any lingering negative emotions. Another caregiver asked for guidance in implementing EW or other coping strategies at home, for example, with additional resources or writing prompts.
Discussion
Three themes emerged from interviews with caregivers following EWR: “inner processing,” “interpersonal learning,” and “enhanced processing and preparedness.” Caregivers reported that writing promoted emotional and cognitive processing, which led to clarity and self-awareness. Once participants had the opportunity to process their own thoughts and emotions, group sharing shifted their focus to other caregivers. In this novel component of the intervention, participants learned from the emotions and experiences of others. This learning helped participants gain a better understanding of themselves, which in turn affected their abilities to cope with, and prepare for, upcoming caregiving challenges. In sum, our findings suggest that the EWR intervention was useful for informal caregivers of patients with cancer.
Expressive writing and reading may be useful because it addresses the loneliness and lack of social support reported by caregivers in oncology settings. 11 Sharing allowed caregivers to form supportive networks. Caregivers consistently referred to the benefits of knowing that other caregivers experienced similar emotions and understood their experiences. This emotional validation and mutual understanding may have allowed caregivers to feel a sense of connectedness and belonging. 28
In addition to fostering connections, EWR seemed to enhance the processing that occurred during writing to impact the caregiving experience. Consistent with previous studies, 20, 29 caregivers reported emotional and cognitive processing during EW, which was sometimes accompanied by negative feelings. Transient increases in negative emotion during EW have been observed in many studies. 21 However, negative emotions may be important for deriving EW’s therapeutic effects. Habituation to negative emotion and cognitive processing have emerged as primary explanations for why EW promotes well-being. 20,21 As noted by a participant in our study and consistent with previous work, 30 the impact of these negative emotions tended to decrease over time. However, gains in insight or self-awareness derived from cognitive processing during EWR may continue to exert positive effects on participants and their caregiving experiences. 20,30
Furthermore, sharing and discussing in a group setting may have similarly offered a safe place to process emotions and thoughts in a social, collaborative way. Group feedback validated caregivers’ emotions, making it easier for them to confront guilt, anger, or other negative emotions during caregiving. Participants consistently reported that EWR helped them achieve insight and self-awareness, for example, by extracting new meanings from their experiences or patterns in their thinking. Studies suggest that caregivers who derive meaning and satisfaction from caregiving have better mental health outcomes. 31,32 Expressive writing and reading might therefore buffer against the emotional costs of caregiving by promoting personal growth, with its social component complementing and enhancing these therapeutic effects.
This socially augmented processing may help caregivers anticipate the loss of their loved ones, as described in evidence emerging for our third theme. Feeling socially supported and prepared for loss during caregiving is related to lower levels of complicated grief postbereavement. 33,34 By learning from experiences of others, EWR may prepare caregivers for upcoming challenges pragmatically and emotionally. Expressive writing and reading provided an opportunity for caregivers to consider and discuss logistical concerns, such as potential locations for end-of-life care. Because loss and bereavement were topics that often emerged organically in the workshops, EWR also provided opportunities for participants to prepare emotionally for the possibility that their loved ones pass away and the anticipated loneliness and grief. Thus, EWR may promote feelings of social support and preparedness, which may make end-of-life care and bereavement more manageable for caregivers. Even if the caregivers are no longer in touch when they are bereaved, they may continue to derive insights or support from their experiences with EWR.
Limitations
Participants self-selected into the study. Those attending 1 or 2 sessions may not have found EWR positive or beneficial, but their input was not included in the study. A randomized controlled trial is needed to systematically assess the benefits of EWR reported in our study (eg, insight, interpersonal learning, preparedness for the future). An important future direction also involves assessing whether EWR enhances caregiver adjustment to loss and bereavement.
Additionally, our sample size was small. One of the most cited setbacks related to low completion was that the workshop conflicted with caregivers’ schedules. This setback may help explain why interventions for caregivers have generally not been incorporated into clinical oncology settings. 5 However, EW has been administered online, with promising results. 35 To increase convenience, it may be possible to administer EWR remotely, perhaps via confidential web conferencing.
Conclusions
Findings from our pilot study suggest that EWR can be a safe and cost-effective intervention for caregivers of patients with cancer. In addition to the provision of social support, benefits of EWR included emotional and cognitive processing (individual and collaborative), interpersonal learning, and preparing for the anticipated loss. During group sharing, caregivers gained a better understanding of themselves and their caregiving experiences and better equipped themselves to cope with upcoming challenges. Incorporating a social component into the EW intervention is feasible and potentially useful in supporting the difficult journey of caregiving. Future research should employ randomized controlled trials of EWR and assess web conferencing as a mode of delivery.
Footnotes
Appendix A
Appendix B
Appendix C
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by University of Guelph-Humber Research Grant Fund 2014-2015. Y.W.L was supported by Ontario Cancer Institute Knudson Post-doctoral fellowship 2013-2014. M.M.M. was supported by the Discovery Fund Fellowship at the Centre for Addiction and Mental Health.