
Abstract

Introduction
A number of recent analyses have applied lessons from economics to health care, including discussions of how the economic principle of the tragedy of the commons can explain overuse of medical resources and impacts on patients, providers, and the health-care system as a whole. 1,2 This medical-economic perspective is particularly useful in understanding the paradoxes of end-of-life care, where overtreatment is a serious problem and where costs are high and quality of life may be relatively low. Increasing the reach of palliative care has been proposed as a solution to overtreatment at the end of life, but despite improvements to patient access and provider training, palliative care has not been the panacea many expected. In what follows, we argue that this failure is the result of the clinical and reimbursement structures that limit end-of-life care, creating a tragedy of the commons. We also propose areas to focus reform while acknowledging that systemic reforms that address the root causes of the problem will be difficult to achieve in the current policy environment.
The Promise of Palliative Care
Palliative care is intradisciplinary care focused on maximizing quality of life—physical, mental, psychosocial, and spiritual—for patients with life-limiting illness. 3 Recent work has demonstrated that palliative care is high-value care because it addresses patients’ symptoms and supports families, while lowering costs. 4,5 As such, there is a large push to increase access to palliative care at end of life. 6 The result has been an almost 400% increase in the number of hospital-based palliative care programs in the last 20 years; almost 70% of hospitals in the United States now have a palliative medicine program. 7
This growth in programs has not coincided with improved care however. Despite national efforts to improve end-of-life care, the rate of uncontrolled pain and other symptoms in the last year of life has increased. 8 In addition, although the rate of hospice use has doubled from 21% to 42% from 2000 to 2009, the reality is more complex. The rate of hospitalization, ICU utilization, and mechanical ventilation have all increased during this period; the percentage of patients enrolled in hospice for less than 3 days has doubled from approximately 5% to 10%. 9 These data suggest that despite greater availability of palliative care, these services are not well integrated into usual medical care. The large body of literature on barriers to effective integration of palliative care has focused on 3 domains: (1) Education (eg, inadequate education of practitioners), (2) Implementation (eg, inadequate workforce, poor coordination between sites of care), and (3) Policy (eg, lack of adequate reimbursement, regulatory barriers). 10
End-of-Life Care as a Tragedy of the Commons
While education, implementation, and policy are all important areas for reform, the broader issue is a structural one. Access to palliative care is stymied by poor incentives, lack of cooperation, and limited collaboration, largely because the structure of medical care continues to be specialist-focused and because patients have access to a range of providers without a guiding framework for care in place. Economists looking in from the outside would say that palliative care struggles to maximize benefits for patients and the health-care system as a whole because the structure of end-of-life care is itself a tragedy of the commons.
The tragedy of the commons is most famously laid out in a 1968 article where a common grazing field, belonging to the group as a whole, is used by a number of independent farmers. 11 Each farmer has an incentive to add one more sheep to the field since the cost to him is minimal and the benefit to him is large. Yet each additional sheep added to the field moves the entire group toward the field’s capacity for grazing, eventually overrunning it. The result is poorer outcomes for everyone. Despite declining outcomes, each individual farmer still has an incentive to keep his sheep in the field, since withdrawing his animals, while increasing the benefit to the group as a whole, both reduces his individual profit and opens the door for other farmers to take advantage by adding additional sheep themselves. The commons problem therefore results from a combination of individuals having divergent incentives from each other and from the group and limited ability to coordinate. Farmers who could coordinate with each other to limit overgrazing and keep out intruders would be better able to steward the field in a responsible way, but in the traditional case, such coordination is not possible and the incentives for cooperation do not exist.
End-of-life care is a classic tragedy of the commons precisely because no one is in charge of any particular patient and no single provider can limit the interventions suggested by any other provider. Patients typically have multiple care providers, multiple diagnoses, and multiple locations of care. Research suggests that this complexity of providers and locations of care makes overtreatment more likely. 12,13 In this scenario, the patient herself is a resource that is being “grazed” by various providers precisely because no one provider “owns” the broader outcome of appropriate treatment. Overtreatment is common and quality of life suffers. 14 -16
Solutions to Tragedy of the Commons
Economists and political scientists would argue that the relative failure of palliative care to reduce overtreatment is a natural consequence of the structure of the clinical environment in end-of-life care, one in which it is very difficult to coordinate care among many different providers and where each provider has an incentive to offer and provide additional care. 17 Despite knowing the source of the tragedy of overtreatment, solutions are less clear in the clinical environment than in the farming context. Traditionally, the 2 most common solutions to the tragedy of the commons involve privatizing the commons or making the commons a public good. Privatizing the commons involves creating property rights and allowing an owner to exclude other grazers, as with a field enclosed by a fence with a lock on it. In contrast, converting the commons to a public good requires management from above by some kind of institution that can monitor and enforce rules, such as a community police force protecting a public park. In the medical case, privatization would require a physician to have the ability to shield a patient from other provider input, essentially turning the patient into the private “property” of the individual physician. A public good approach would require some kind of external monitoring agency, like an administrative body or an insurer, to oversee physician activities and determine when overuse is occurring.
Physicians typically resist both these approaches, for good reasons. The first raises ethical questions about limiting patient access to other providers while the second threatens physician independence and the physician–patient relationship. More practically, patients cannot be easily privatized in a hospital environment and management of care by an administrative body, or insurer threatens patient and physician autonomy and leads to bureaucratic bloat. There are, however, other ways of structuring the clinical environment to encourage collaboration and to limit overtreatment. Obvious examples of clinical policy changes—such as making palliative care consults “opt-out” rather than “opt-in” or creating pause points in the provision of care—can allow time for more collaboration, though neither substantially reduces the conflicts of incentives that collaborating physicians would still face. More comprehensive reorganization has the potential to address the incentive problem itself, which is a more complex but more promising task. 18,19
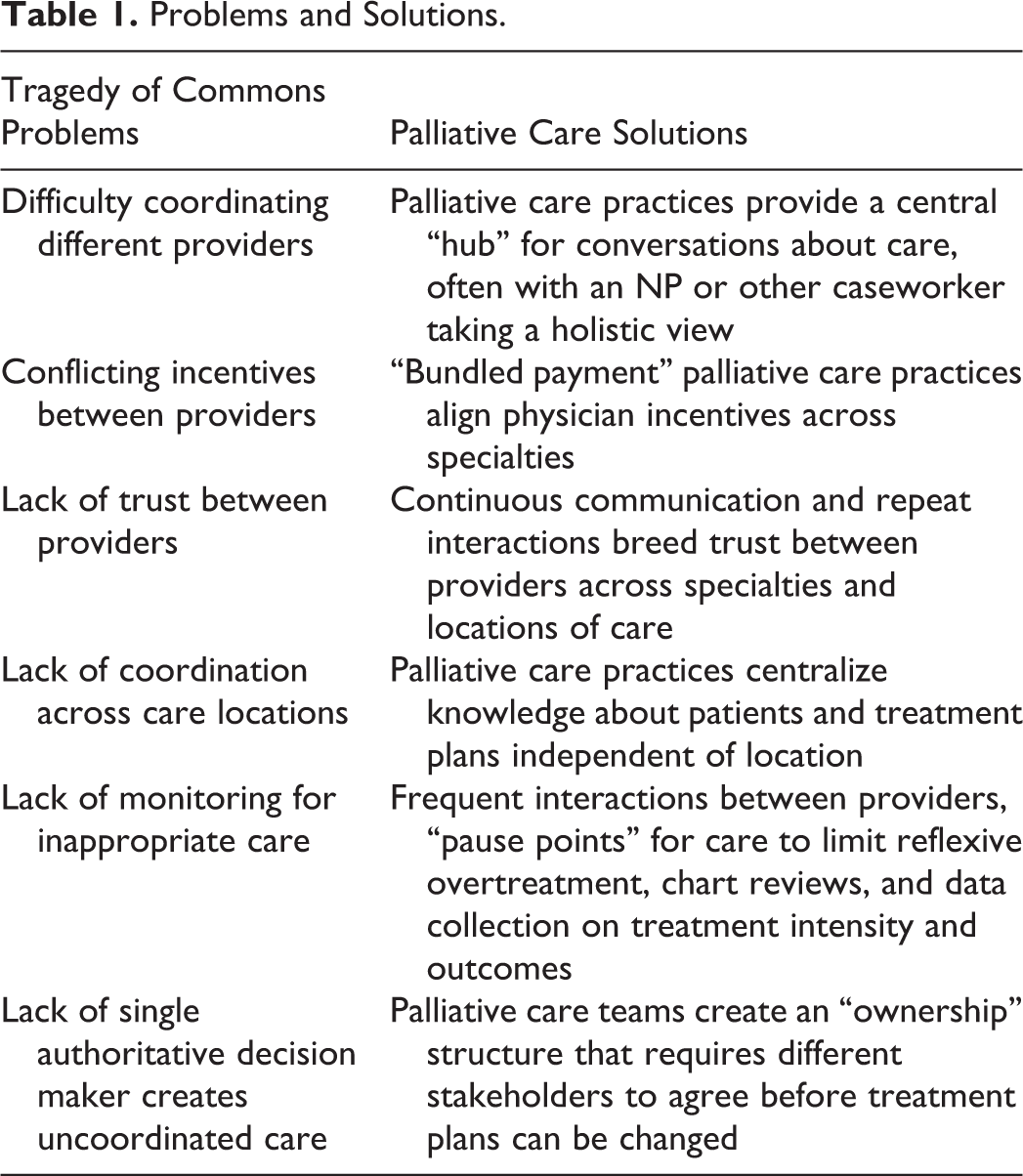
Such a reorganization would require at a minimum moving away from reimbursement policies that privilege procedures and specialists and also structuring care teams to support greater levels of collaboration and trust. The case of Grand Junction, Colorado, is often cited in the literature as an example of bottom–up reform, headed by physicians and possibly capable of replication elsewhere. Crucial elements of Grand Junction’s success that shifted incentives included collaborating physicians pooling resources, continual interactions to create trust, monitoring via chart reviews, outcome and cost data sharing, and peer pressure to maintain treatment norms. 18,20 While such requirements might feel unacceptably limiting if imposed from the outside, physicians were willing to undergo such monitoring of and restrictions on their practices because the restrictions were freely chosen and because the restrictions were in-line with best practices. The imposition of such restrictions from above without physician buy-in would be unlikely to work in the same way, if at all. 18 Many of the reasons Grand Junction is relatively successful are the same reasons palliative care programs can reduce overtreatment and costs, but in both cases, the benefits are hamstrung by the structure of the system itself. Knowing this, broader structural reforms can be envisioned, though implementation will be politically difficult. Table 1 provides a partial list of ways the tragedy of the commons influences medical care alongside potential solutions provided by better integration of palliative care teams.
Problems and Solutions.
Conclusion
As is the case with any tragedy of the commons, the efficacy of palliative care will be limited by hospital policies and the structure of clinical medicine itself. Understanding how the tragedy of the commons influences the provision of medical care does not itself directly point to a solution, but it underscores the need for more systemic change. Aligning physician incentives with best practices for patients will require making collaboration easier, reducing the perverse incentives of current reimbursement policies, and increasing trust between providers from different specialties. What is certain is that until we address the poor incentives at play at the end of life, patients will continue to be caught in a tragedy of the commons that results in overtreatment and lowers quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.