
Abstract
Introduction
Palliative Care (PC) is a public health priority. Pain is one of the most frequent symptoms of the many illnesses that require PC. Morphine, essential in PC practice 1 , is widely used to alleviate moderate and severe pain, as well as dyspnea. 2 Pain relief also plays a vital role in helping control other symptoms such as psychological anguish. 3
The lack of proper access to PC and availability of opioids could result in its under medication, less effective symptom control, lack of timely referral of patients to PC treatments 4,5 , as well as blocks on developing interpersonal relationships, and difficulty identifying the correct pharmacological therapy for pain. 1
Every country should guarantee access to medicines and technologies for pain relief 6 and correctly regulate the use of opioid analgesics. 7 However, most of the world’s population lives in countries with low access to opioids. 8 PC and pain relief are still a priority worldwide 9 and the global pain crisis is one of the most serious health and equity issues of our society. 10
Although this topic might already be addressed adequately in developed regions, countries like Ecuador still need contextualized data to better advocate for PC and pain relief. The distribution of morphine (DOMED) in Ecuador is 6.5 kg and, compared to other countries in Latin America, it has a “regular” collaboration between prescribers and regulators of opioid analgesics. 11 Another study conducted with health professionals in Ecuador states that there are weaknesses in the health system that increase the difficulty of prescribing morphine due to its unavailability. 12
Educating the public on the matter could act as a complementary approach to overcome low health literacy, 13 and allow patients to advocate for this kind of care if needed. Few studies report the perspective of the public who might be the recipients of PC, while others report this omission as a limitation of their studies. 4 This research aims at describing the perception of the uses and risks of morphine in PC in the general public in Ecuador.
Methods
This was a cross-sectional descriptive study requiring subjects to complete an online anonymous questionnaire regarding beliefs about PC and opioid use. The questionnaire was hosted on SurveyMonkey, from September 2019 until January 2020. The link to the survey was posted on the individual and professional social media (Twitter, WhatsApp, and Facebook) of the authors, the research team, and the School of Psychology of Universidad de Las Américas. The average time to complete it was 15 minutes and participants did not receive any compensation. Using snowball sampling, a total of 257 people living in Ecuador completed the survey. Informed consent was obtained digitally prior to the beginning of the questionnaire. Approval for this study was obtained from the Ethics Committee of Universidad San Francisco de Quito (IR-E55-2019-CEISH-USFQ).
This study is part of a larger study examining beliefs about PC in the general Ecuadorian population. A survey was developed for the initial study after a literature review and validated by PC experts in the Ecuadorian context. It consisted of sociodemographic questions and statements about PC and opioids. Only 5 items of the survey, those exploring beliefs about morphine use, were considered in the current study (1. Morphine causes addiction, 2. Morphine use accelerates death, 3. Morphine is only used near the end of the patient’s life, 4. Oral morphine does not have the same effect as intravenous morphine, and 5. The use of morphine should be delayed because it accelerates the death of the patient). A 5-point Likert Scale format was used (Strongly disagree to Strongly agree). Participants were asked to answer questions honestly about their level of knowledge regarding PC.
Descriptive statistics were used to characterize the sample and responses. ANOVAs and Pearson r correlation were used to examine the relationship between agreement with item and sociodemographic variables, Post-hoc analysis was performed where appropriate.
Results
Of the 257 participants who completed the survey, 89 were male (34.6%) and 168 female (65.4%). The mean age was 43.08 (SD = 16.16) and most participants had a college degree (40.1%), followed by postgraduate education (36.2%), tertiary education (7.8%), and high school (16%). Most of the sample was single (45.9%), followed by married (39.3%). Approximately half the sample (51.8%) reported that their actual occupation was related to health care. Of the total sample, 109 participants (42.2%) endorsed having had experience providing care to others as an informal caregiver, and 20 participants (7.8%) reported having received PC.
Regarding perceptions of morphine use, 23.8% of participants disagreed or totally disagreed that morphine causes addiction in a PC setting, similar to the 25.3% of participants that disagreed or totally disagreed that oral morphine does not have the same effect as intravenous administration. Beliefs about morphine as it relates to the death of the patient were generally consistent: 63.1% disagreed or totally disagreed that morphine use accelerates death, slightly higher to the proportion of participants (56.1%) that disagreed or totally disagreed that it should be delayed because it accelerates the death of the patient. Similarly, 60.3% disagreed or totally disagreed that morphine is only used near the end of the patient’s life.
Agreement on the items did not vary significantly by age, sex, nor marital status. Occupation and education effects were noted for several items, as well as whether the participant had experience with PC as patients or caregivers (Table 1). Regarding item 1, Morphine causes addiction, lower agreement was associated with higher education, having received PC, and having provided PC as either formal or informal caregiver. On item 2, Morphine use accelerates death, lower agreement was associated with having a health-related occupation, higher education, and having provided PC as a formal caregiver. Item 3, Morphine is only used near the end of the patient’s life, had significantly lower levels of agreement for health-related occupation, higher education, and having provided PC as formal or informal caregiver. On item 4, Oral morphine does not have the same effect as intravenous morphine, lower agreement was related to higher education, having received PC, and having provided PC as formal or informal caregiver. Lastly, on item 5, The use of morphine should be delayed because it accelerates the death of the patient, lower agreement having a health-care occupation, higher education, having received PC, and having provided PC as formal or informal caregiver.
Means and SD for Variables Significantly Related to Survey Items.
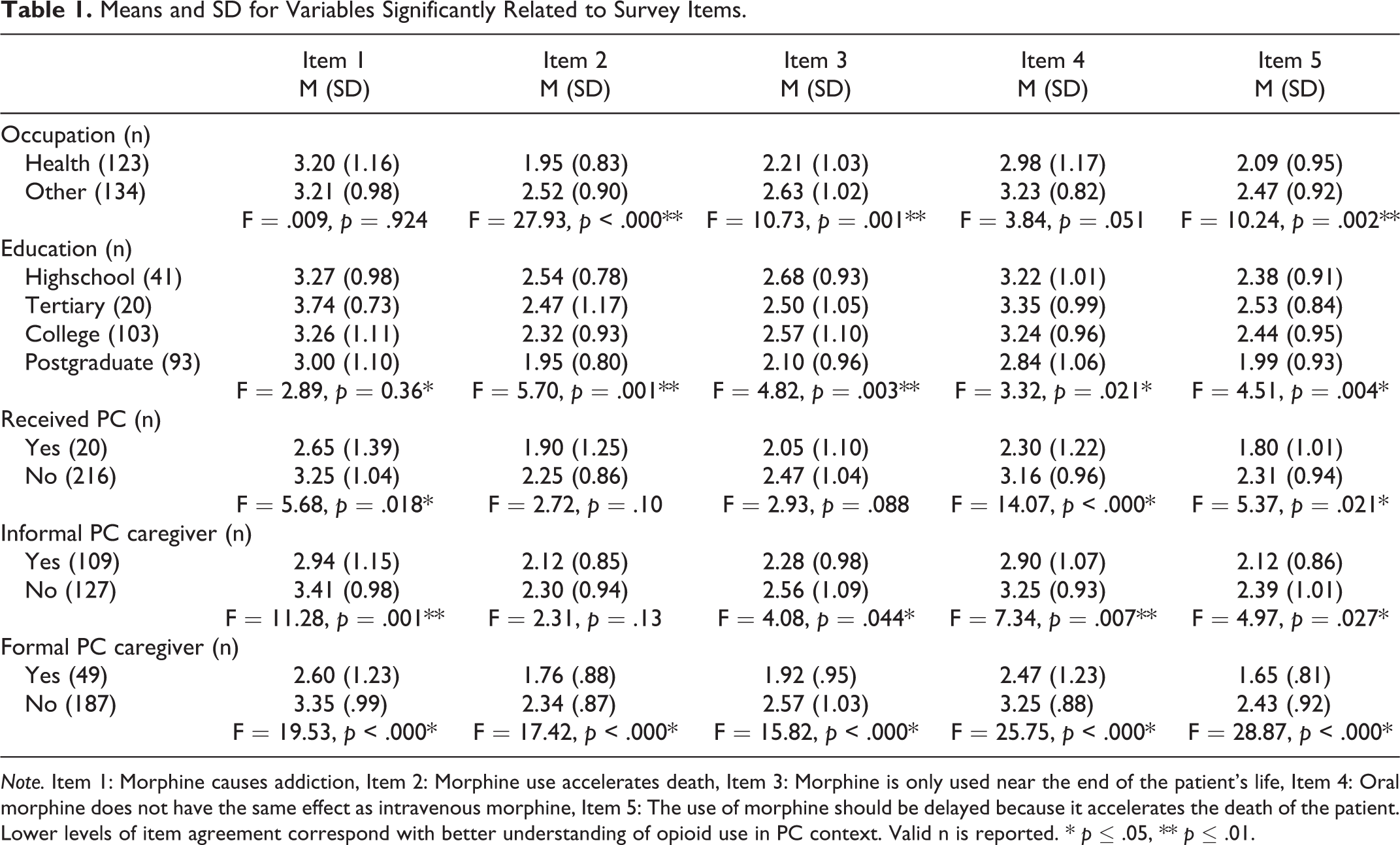
Note. Item 1: Morphine causes addiction, Item 2: Morphine use accelerates death, Item 3: Morphine is only used near the end of the patient’s life, Item 4: Oral morphine does not have the same effect as intravenous morphine, Item 5: The use of morphine should be delayed because it accelerates the death of the patient. Lower levels of item agreement correspond with better understanding of opioid use in PC context. Valid n is reported. * p ≤ .05, ** p ≤ .01.
Discussion
To promote PC, it is vital to identify the myths around the use of pain control drugs, as well as the prejudice and misinformation on the appropriate use of opioids (opiophobia). 10 According to the results of this study, education is still needed to overcome some misconceptions.
A great percentage of the participants either agreed or totally agreed that morphine causes addiction, even though the questions were in a PC context. In the case of effectiveness according to its route of administration, results also indicate misinformation and show that informal caregivers and people who have received PC have better knowledge about morphine use. Similar to other research, overall, participants did not associate morphine with death and dying. 14
The effectiveness of morphine is well established. 15 Yet, these results point to a lack of knowledge about it. Contrary to prior research that shows that more experienced nurses recognize that drug addiction is not a major problem when using morphine for pain control in PC, 16 there were no significant differences in beliefs about addiction and effectiveness according to occupation.
Physicians tend to prescribe opioids less due to the perceived resistance of the patients and the fear of adverse effects. 17 However, people would accept morphine if it was recommended and monitored by a doctor, but patients perceive not all doctors like prescribing it. 14 A better understanding about opioids is required for effective adoption of pain management strategies, particularly considering that patients who are prescribed opioids are more likely to access PC 18 which has documented benefits for patients, families, and health systems. 19
The findings of this cross-sectional study are limited to the local experience of people living in Ecuador, which may vary in other socio-cultural contexts. Also, the data was obtained from an online survey, and sources of information were self-reported. In addition, the sample was highly educated and a large number of them had direct experiences either receiving or providing PC. Finally, health professionals appear overrepresented in our sample, considering that data shows there are 2.0 physicians per 1000 persons in Ecuador. 20 Therefore, it will not be appropriate to generalize the results. Future research could replicate this study on a larger sample from different socio-cultural contexts.
Despite its limitations, this study adds to the body of work that highlights the importance of including PC training into the education curriculum at all levels to normalize practices of pain management. 3 It also illustrates the importance of designing educational policies and targeted interventions to improve the use of PC services taking into consideration cultural and social aspects of patients and families and how they perceive and treat pain. 13,16
Footnotes
Acknowledgments
The authors would like to thank Gabriel Osejo, Anna Belén Marcillo, Diego Miño, and Matías Mendoza for their contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the General Research Department of Universidad de Las Américas through an internal Grant awarded to the corresponding author.