
Abstract
Keywords
Introduction
High morbidity and mortality rates lead to an association between cancer and death. 1 Cancer progresses insidiously, has unexplained causes, is hard to control, and even causes loss of control from time to time. All these factors, and many more, affect cancer patients and their families physically, psychologically, and socially. They also cause great suffering, and therefore cancer is perceived as more terrible and threatening than other chronic diseases.1,2 Advances in science and technology have made many cancers treatable and increased survival rates. 3 However, all cancer types are still not completely treatable. Even in cases where treatment is possible, the process is long, expensive, painful, and difficult and affects patients and their families physically, psychologically, and socially negatively. Patients with cancer may fear side effects, abandonment, relapse, or changes in body image, refuse treatment, suffer from anxiety, depression, and adjustment problems, and feel the loss of expectations and plans for the future.4,5
Chemotherapy is a significant part of cancer treatment. Although it increases survival, it causes serious physical and psychological symptoms. 6 It is difficult for patients and their families to adapt to changes caused by cancer and chemotherapy. It is even much harder for vulnerable groups, especially the elderly, to cope with cancer-related problems and to adapt to the new situation. 7 The number of older patients with cancer has risen with an increase in the life expectancy of the general population, and in survival rates as a result of advances in cancer diagnosis. Therefore, cancer is now regarded as an aging disease. Sixty percent of tumors and 80% of cancer deaths occur in people aged 65 years or older. Aging and cancer have a number of common characteristics such as functional losses and physical, psychological, and social processes, which require adaptation. 8
Physiological, physical, cognitive, and social functions, which play a key role in coping with cancer, are impaired due to aging. Losses, fragility, and low health literacy-related and financial problems frequently observed in old age limit the access of the elderly to health services. Even in cases where access to health services has been made possible, negative attitudes toward them, such as ageism, may prevent them from receiving optimal care.8,9 Aging-related problems complicated further by cancer become a challenging process for both patients and their families. However, age-specific developmental tasks such as achieving financial independence, establishing a professional career and long-term partnerships, marrying, and starting a family represent additional challenges for younger patients.10,11 Young patients need to adapt to more life fields because they take a more active role in daily life—both physically and socially. Coping skills, which are extremely important in adapting to cancer, may not have developed yet in young cancer patients too. Young cancer patients, who have responsibilities in daily life and more developmental tasks to complete, may have more and different unmet needs.10,12
There are different results in the literature with regard to age-related unmet needs. 13 Age-related physiological changes and psychosocial factors and medical conditions make some of the needs of cancer patients unique and complex.7,13–15 The needs that increase with the cancer experience and while interacting others may differ according to the developmental stages.16,17 Research shows that supportive care needs can vary depending on the technology, health system, time, culture, and age. Some studies argue that an increase in age increases the number of unmet supportive care needs, whereas others report the opposite.11,13,14,18–22 While Puts et al (2012) reported that older patients had more unmet needs, 23 Galán et al (2018) and Bibby et al (2017) reported that younger cancer patients had more unmet needs.14,21 It is observed that the characteristics and fields of individuals to express their current needs, make demands, and seek help are also affected by cultural, age, and gender variables. 11
At the heart of meeting these needs lies the concept of supportive care. In recent years, there has been an increased interest in unmet supportive care needs. The objective of supportive care is to optimize the physical comfort and functionality and social, cognitive, economic, psychological, and spiritual well-being of cancer patients. Unmet supportive care needs lead to reduced care satisfaction and quality of life. 24 Supportive care is a health service that starts from the prediagnosis stage to recovery or the terminal stage and even till death and mourning, to help patients and families cope with cancer.25,26 It is observed that the health care, communication, daily life, physical, psychosocial, spiritual, and social needs of cancer patients are not met.26–28
Providing healthcare to all can be achieved by determining the specific needs of the groups. The aim of this study was to determine whether there was a difference in unmet supportive care needs between older and younger cancer patients in Turkish culture and health system. We believe that the results will be a guide for the development of interventions to meet the supportive care needs of cancer outpatients who receive chemotherapy.
Methods
Design, Settings, and Data Collection
The purpose of this descriptive study was to investigate whether there was a difference in unmet supportive care needs between older and younger cancer outpatients who receive chemotherapy. This study sought answers to the following questions: (1) What are the unmet supportive care needs of cancer outpatients who receive chemotherapy? (2) Is there a difference in unmet supportive care needs between older and younger cancer patients?
The study was conducted between October 1, 2018 and October 01, 2019 in the Daytime Treatment Unit (DTU) of the oncology hospital of a university in Ankara, Turkey. The unit provides short-term infusion and supportive and venous port/catheter care services. The hospital, which is internationally accredited, provides standard care to patients but does not have hospital policies and/or interventions catering specifically to older patients.
The study population consisted of patients older than 18 years who were receiving chemotherapy at the DTU. The sample consisted of two groups: patients aged 65 years or older (first group) and patients aged 18-64 years (second group). The World Health Organization guidelines were considered as the basis to determine the age groups.
29
Both groups were similar in terms of sex, cancer type, and chemotherapy protocols. Power analysis was performed using G*Power with the probability of a type I error and for the power of β = .80 (α = .05, SD: .66), based on the assumption that there is a difference of at least .30 in the Supportive Care Needs Scale-Short Turkish Version (SCNS-SF
The inclusion criteria for the study were as follows: (1) literate, (2) diagnosed with cancer for the first time, (3) at least in the second chemotherapy cycle, (4) not receiving some form of active cancer-directed treatment, and (5) willing to volunteer. Those with physical, psychological, and cognitive impairments that would prevent them from giving effective answers and communicating were excluded from the study sample.
Procedures
The study was approved by the Non-Interventional Clinical Research Ethics Committee of the University. A pilot study was conducted between October 1, 2018 and November 1, 2018 to determine the most proper type of font size in questionnaire forms. Questionnaire forms with contrast colors typed in 16 point fonts were used for elderly patients, while 12 point fonts were used for younger cancer patients. Participants were asked to complete the form, and those participated in the pilot study were excluded from the main study.
Patients were informed about the purpose, procedure, and confidentiality of the study before participation, and verbal informed consent was obtained from those who agreed to participate. Because some older patients had difficulty reading the forms, the first author of the study read the questions to all participants in the main study. The paper questionnaire forms were completed face-to-face in chemotherapy rooms during their chemotherapy treatment. Patient privacy was ensured during data collection. Each participant completed the forms in 20 minutes.
Data Collection Tools
Data were collected using the Patient Information Form and the SCNS-SF
The Patient Information Form was developed by the researcher based on the literature review. The form consisted of 13 items about the sociodemographic characteristics, disease, and treatment of DTU patients.
The Supportive Care Needs Scale (SCNS) was developed by Boyes et al (2009) to determine the unmet supportive needs of cancer patients (Cronbach's alpha ranging from .86 to .90). Ozbayır et al (2017) established the reliability and validity of the SCNS-SF
Statistical Analysis
Data were analyzed using the SPSS, version 23 (IBM) at a significance level of .05. The Kolmogorov–Smirnov test was used to determine whether the data met the assumptions for parametric tests. Socio-demographic and disease-related data were normally distributed; however, the subscale data were not normally distributed. Therefore, nonparametric tests were used for data analysis. The Mann–Whitney U test was used for data comparison between the two groups; the Kruskal–Wallis H test for data comparison between three or more independent groups; and Bonferroni correction for pairwise comparisons of variables with significant differences.
Results
The mean age of younger and older patients was 48.56 (±7.99) and 69.56 (±4.68), respectively, and the difference was significant (t = −21.94; P = .000). The mean duration of diagnosis of younger and older patients was 6.56 (±6.03) and 6.25 (±4.23) months, respectively. The time between diagnosis and study was similar in both groups (t = .41; P = .676). The number of chemotherapies received was also similar in both groups (t = .89; P = .934).
Table 1 shows the participants' socio-demographic and disease characteristics. Among the participants, 81.7% were married, 45.2% were aged 65 years or older, and 28.0% of those below 65 years had a primary school degree. In addition, 71.5% had neutral income (income = expenses), 35.5% were diagnosed with gastrointestinal cancers, 53.8% had an unknown stage, and 66.7% had completed other treatments before chemotherapy.
Age-Dependent Distribution of Participants' Sociodemographic Characteristics and Disease-Related Data.
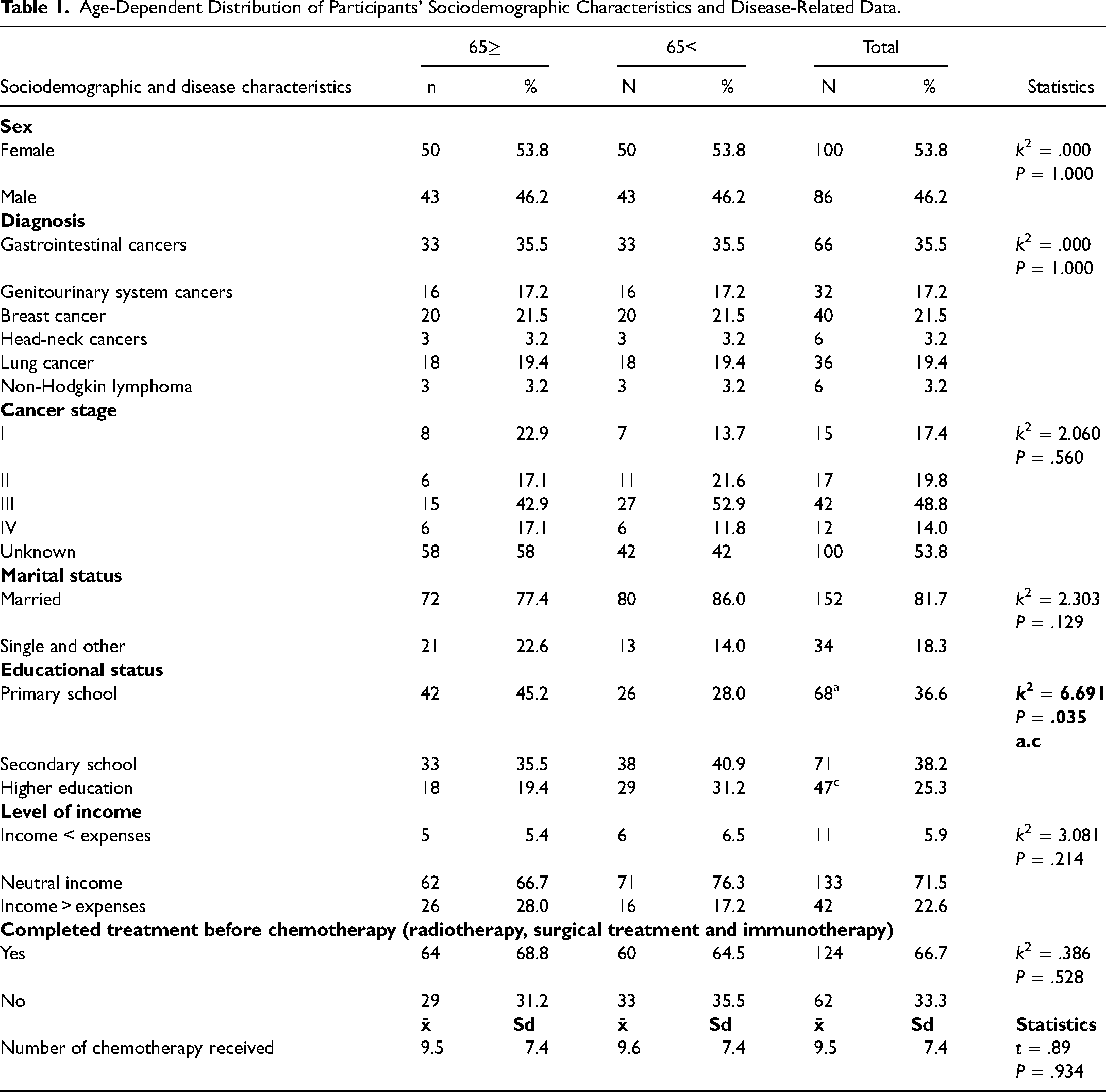
Table 2 shows the median SCNS score distribution, indicating that the participants reported more unmet daily life needs (Med = 2.60 [Min = 1.80; Max = 3.40]) than health care and information needs (Med = 2.00 [Min = 1.65; Max = 2.45]), psychological needs (Med = 1.57 [Min = 1.14; Max = 2.14]), and sexuality needs (Med = 1.00 [Min = 1.00; Max = 1.67]).
Participants' Median SCNS Score Distribution.
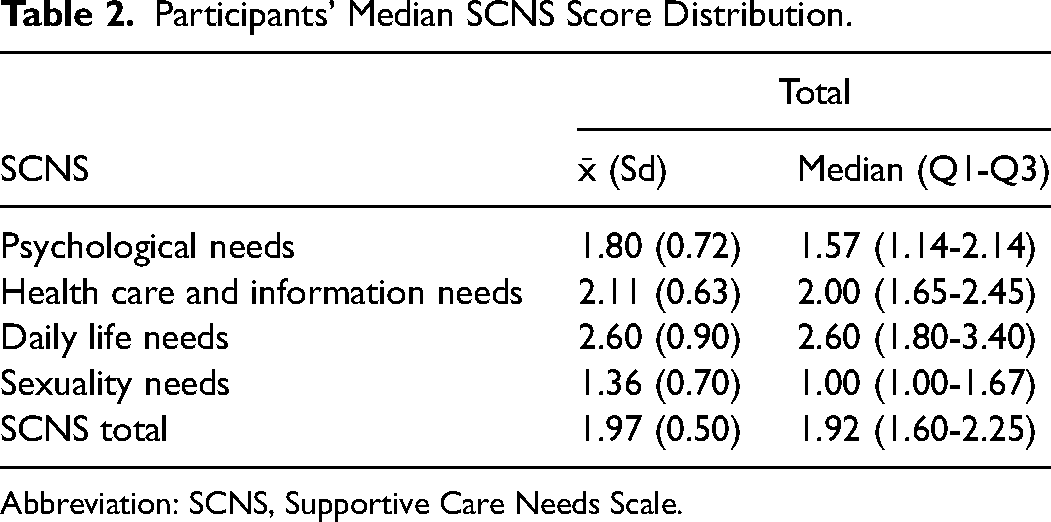
Abbreviation: SCNS, Supportive Care Needs Scale.
Table 3 shows the median SCNS score distribution by age, indicating that younger participants reported more unmet needs than older participants (Z = 3.771; P = .000). Although both groups had similar “psychological needs” (Z = −1.687; P = .090) and “daily life needs” (Z = −1.553; P = .120) subscale scores, the younger group had higher “health care and information needs” (Z = −3.918; P = .000) and sexuality needs (Z = −4.945; P = .000) subscale scores than the older group.
Age-Dependent Distribution of Median SCNS Scores.
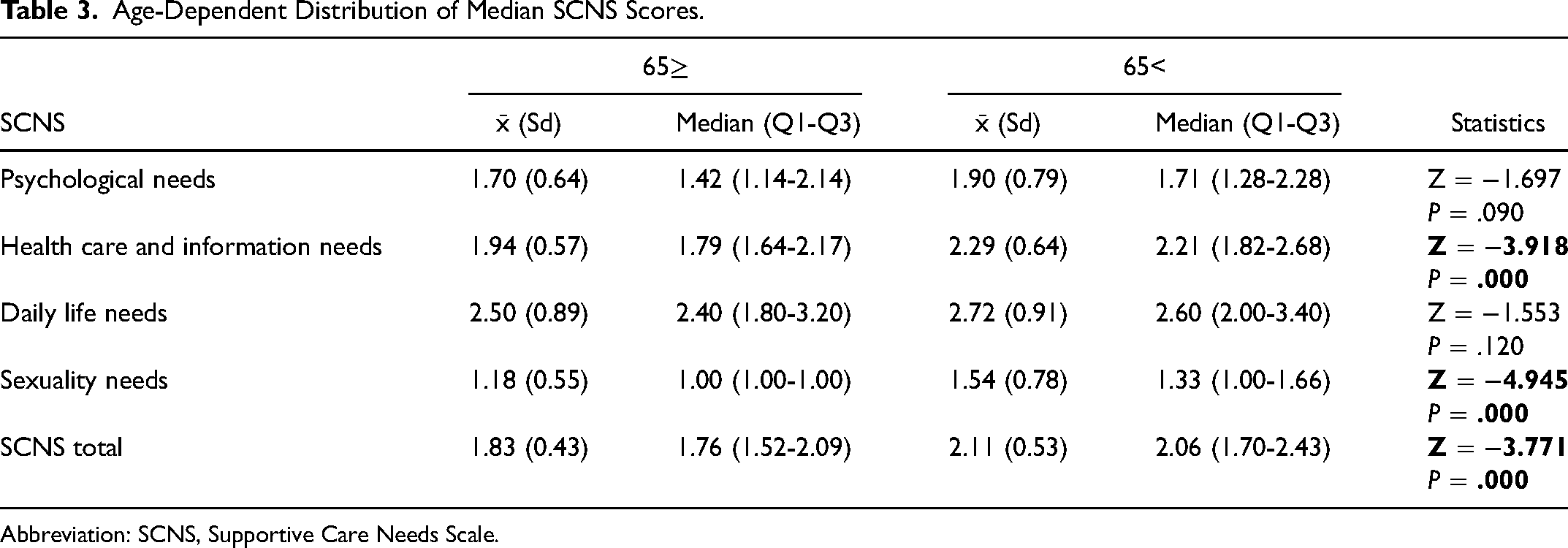
Abbreviation: SCNS, Supportive Care Needs Scale.
Discussion
This study investigated whether there was a difference in unmet supportive care needs between older and younger cancer patients. This section will discuss each research question in two parts.
Participants had low median SCNS total scores (Table 2), suggesting that their supportive care needs are met. Research shows that the supportive care needs of cancer patients vary depending on the health system, cancer type, patient characteristics, treatment type, and stage.19,24,26,31 In Boyes et al’s study (2012), 42% of participants reported no unmet needs, while 21% reported few unmet needs. 32 In Boyes et al’s study (2015), half of the hematologic cancer outpatients reported moderate to high-level needs. 12 Sakamoto et al (2017) conducted a study on Japanese outpatients with colorectal cancer receiving chemotherapy and stated that 42% reported unmet needs. The number of studies on the unmet needs of cancer patients in Turkey is limited, and the existing ones focus merely on daily life and health care along with information aspects of supportive care needs, but do not provide data that would allow for a more complete assessment.27,33
Our participants' “daily life needs” score was highest, followed by “health care and information needs” score (Table 2). Research shows that being or not being in the process of diagnosis or treatment and being an outpatient or inpatient determine the priority of unmet needs.12,26,34 Inpatients mostly report unmet physical and daily life needs34,35, whereas outpatients report unmet psychological needs.12,36 Boyes et al (2012) conducted a study on patients who mostly did not receive active treatment in the previous month and summarized that they reported unmet psychological needs, followed by unmet daily life needs. Although studies show that outpatients mostly report unmet psychological needs, our participants reported more unmet daily life needs than unmet psychological needs, which might be because of the disruptive effect of chemotherapy on daily life. However, Gozum and Akcay (2005) also reported that Turkish outpatients who received chemotherapy mostly reported unmet daily life needs. Temiz and Durna (2019) conducted a study among 450 patients who had received at least two doses of chemotherapy and reported that participants mostly reported unmet daily life needs, followed by unmet psychological needs.
Our participants' “sexuality needs” subscale scores were lowest (Table 2). Research shows that patients report fewer sexuality needs than other needs, regardless of the type of cancer.12,27,32,36 Research on genitourinary cancers, however, shows that patients report numerous unmet sexuality needs,37–39 which is an expected result caused by the nature of genitourinary cancers that directly affect sexuality. Those studies report that patients with genitourinary cancers need information, conversation, and support about sexual health.37,38 Our participants' low “sexuality needs” subscale median score might be because of the fact that the sample consisted of patients with different types of cancer and different cultural characteristics. Research also shows that Asian cancer patients report fewer sexuality needs.34,40,41 Sexuality is viewed as a taboo in Turkey. Even health care professionals prefer not to talk to their patients about sexuality. Patients are embarrassed to talk about their sexuality needs, and when they do, they feel anxious, resulting in a denial or neglect of such needs.
Participants aged below 65 years had a higher SCNS total score than that of older participants (Table 3). Studies on certain types of cancer have reported contradictory results with regard to the relationship between patient age and supportive care needs.4,6,20 Similar to our results, some of those studies suggest that younger patients report more unmet needs.12,20,32,41–43 This result may be because of the fact that younger patients have more limited coping strategies, which are crucial in adapting to the disease, and they are expected to actively participate in life and complete tasks specific to their age. Besides, they think more about their needs and express them more easily than older patients.32,44
The elderly are a vulnerable population who require special care. 8 Puts et al (2012) reported that older patients had more unmet needs. The SCNS assesses older patients' self-reported perceptions. Their tendency to express needs, make requests, and seek help depends on culturally assigned roles and responsibilities related to their ages. 45 Our result might be because of the fact that, in Turkish society, the elderly are expected to be content with what they have and not to demand for more.
Participants aged 65 years or older did not express their unmet sexuality needs (Table 3). Research shows that the deterioration of physical functions and health, death of a spouse, job loss, and financial crises with age are some of the causes of low sexual drive that result in a decreased interest in sexual activity.46–48 Young bladder cancer patients 6 and young gynecological cancer patients 20 reported more unmet sexuality needs than older patients. The misconception that older people do not have active sexual lives and the perception of senile sexuality as something inappropriate, funny, or disgusting are internalized by the elderly, resulting in them avoiding sexuality and having difficulty expressing their unmet sexuality needs. 48
Participants aged above 65 years expressed fewer unmet health care and information needs (Table 3). In the literature on unmet need for information, it was found that patients with higher levels of education indicated a more unmet need for information about the disease.6,41,49 In the research conducted by Temiz and Durna (2019), similar results emerged, and it was found that patients with higher educational levels had higher health care and information needs. 27 In our study, health care and information needs were found to be related to age rather than to educational level. Similarly, Mohamed et al (2016) reported that young patients mostly reported unmet health care and information needs. Caring for aging parents gradually changes parenting roles and even reverses them. The elderly who become dependent on others may become regressed, avoid expressing their needs, lack information on where and how to get help, and, after a certain point, stop seeking help. 45 Health care professionals mostly do not provide information to older patients, but to their families, and they show older patients less respect and spend less time with them, which makes the older patients less aware of their health care and information rights and less inclined to express their unmet needs. 50
This study has some limitations. Although the researchers took measures to protect patient privacy (removing relatives from the treatment room, drawing the curtain between the treatment chairs, closing the door, etc), the data were, nevertheless, collected where the patients received chemotherapy treatment and care. The second limitation is that the researchers read the items aloud, which might have negatively affected the willingness of the participants to respond.
Conclusion
The results showed that younger participants reported more unmet supportive care needs than older participants. Both groups reported health care and information needs the most and sexuality needs the least. Projects should be developed to raise health care professionals' awareness that patients' supportive care needs may vary with age. Cultural factors that we think may be related to the supportive care needs of cancer patients should also be taken into account when developing those projects. Health care professionals should also recognize that older patients are a vulnerable population who may have difficulty expressing their needs.
Footnotes
Acknowledgments
The authors would like to thank the individuals who participated in this study.
Declaration of Conflicts of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Funding Support
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Trial Registration
Not applicable, because this article does not contain any clinical trials.