
Abstract
Keywords
Introduction
Palliative care (PC) aims to improve the quality of life of patients diagnosed with an advanced illness and their families.1,2 Family members, who often play an integral role as primary caregivers, need to provide personal care, 3 manage symptoms 4 and deliver psycho-social and emotional support, 5 in addition to usual household chores 6 and/or their paid work. Caring for a loved one with an advanced illness can be physically exhausting, 7 psychologically distressing,2,8 and financially stressful.9,10 In most developing countries, where patients are often diagnosed at an advanced stage and cure usually not possible,11-13 PC is inadequate or non-existent,14-16 and the evidence for support needs of family caregivers is limited.17,18
Bhutan is a tiny Himalayan kingdom with a population of 771 608. 19 Bhutan is known to the world for Gross National Happiness, a concept where the country's development takes a holistic approach giving equal importance to non-economic aspects of wellbeing. 20 Healthcare is provided through a three-tiered system based on a primary health care approach (Figure 1).21,22 Traditional medicine is integrated into the national health system. 21 It provides treatment mainly through behavioral modification, herbal medicines and spiritual healing. 23
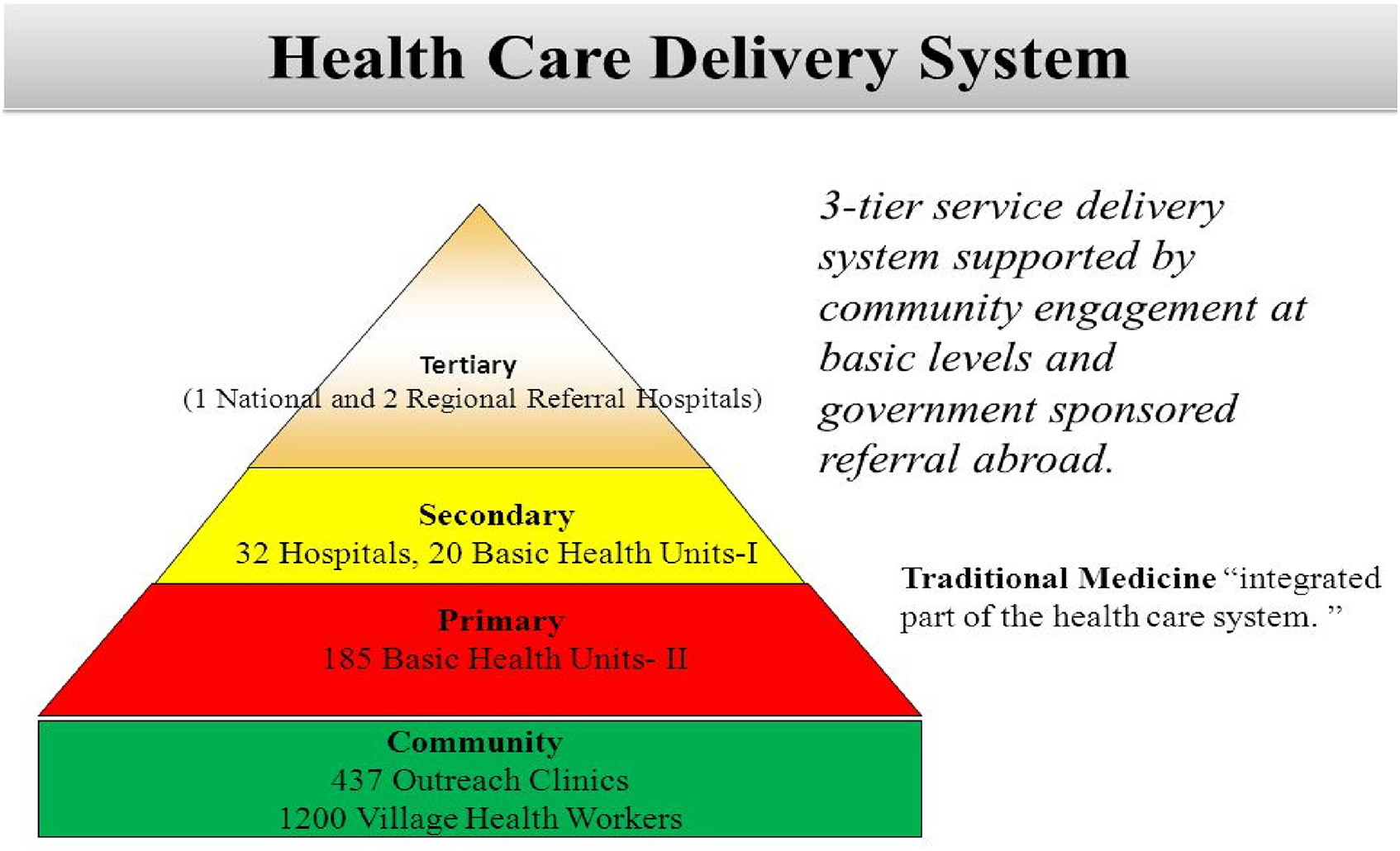
Health care delivery system in Bhutan. 22
Similar to other developing countries, the prevalence of non-communicable diseases including cancer and organ failure has increased in Bhutan over the last 20 years, while infectious diseases like HIV/AIDS and multidrug resistant tuberculosis (MDR-TB) continue.24,25 From 2005 to 2019, the incidence of cancer has increased from 8.7 (per 10 000 population) to 26.8 and diabetes from 14.9 to 75.0. 25 The total number of reported MDR-TB cases increased from 6 in 2005 to 70 in 2019. 25
While other healthcare services significantly increased in Bhutan since the early 1960s, 21 just as in most developing countries, PC remains a young concept. 26 In 2018, a small home PC service was started at the national referral hospital where three beds were also allocated for PC in the oncology ward. 26 In 2020, the Ministry of Health launched a PC service package integrating traditional medicine into PC service. 27 Over the years, the need for PC in the country has been emphasized.21,28,29
Despite being a small and sparsely populated mountainous nation, the socio-economic circumstances in Bhutan are similar to many developing countries. Like elsewhere in the region, Bhutanese family members play a vital role in patient care, both in hospitals and at homes. As the curative aspect of treatment diminishes, the family members usually take over the burden of managing symptoms including the psychosocial, emotional and spiritual distress of their critically ill loved ones. However, the needs of these family members have not been studied so far. Therefore, this study explored the support needs of family members caring for loved ones diagnosed with advanced illnesses. This study is expected to inform a bigger research project – development of a suitable PC model for Bhutan, and may have implications for similar countries.
Methods
Study Design, Setting, Population and Sampling
This is a cross-sectional descriptive study. Data were collected during May-August 2019. Study sites included the national referral hospital, the two regional referral hospitals, four district hospitals and four Basic Health Units (BHUs), Grade I and II, spread across Bhutan (Figure 2).
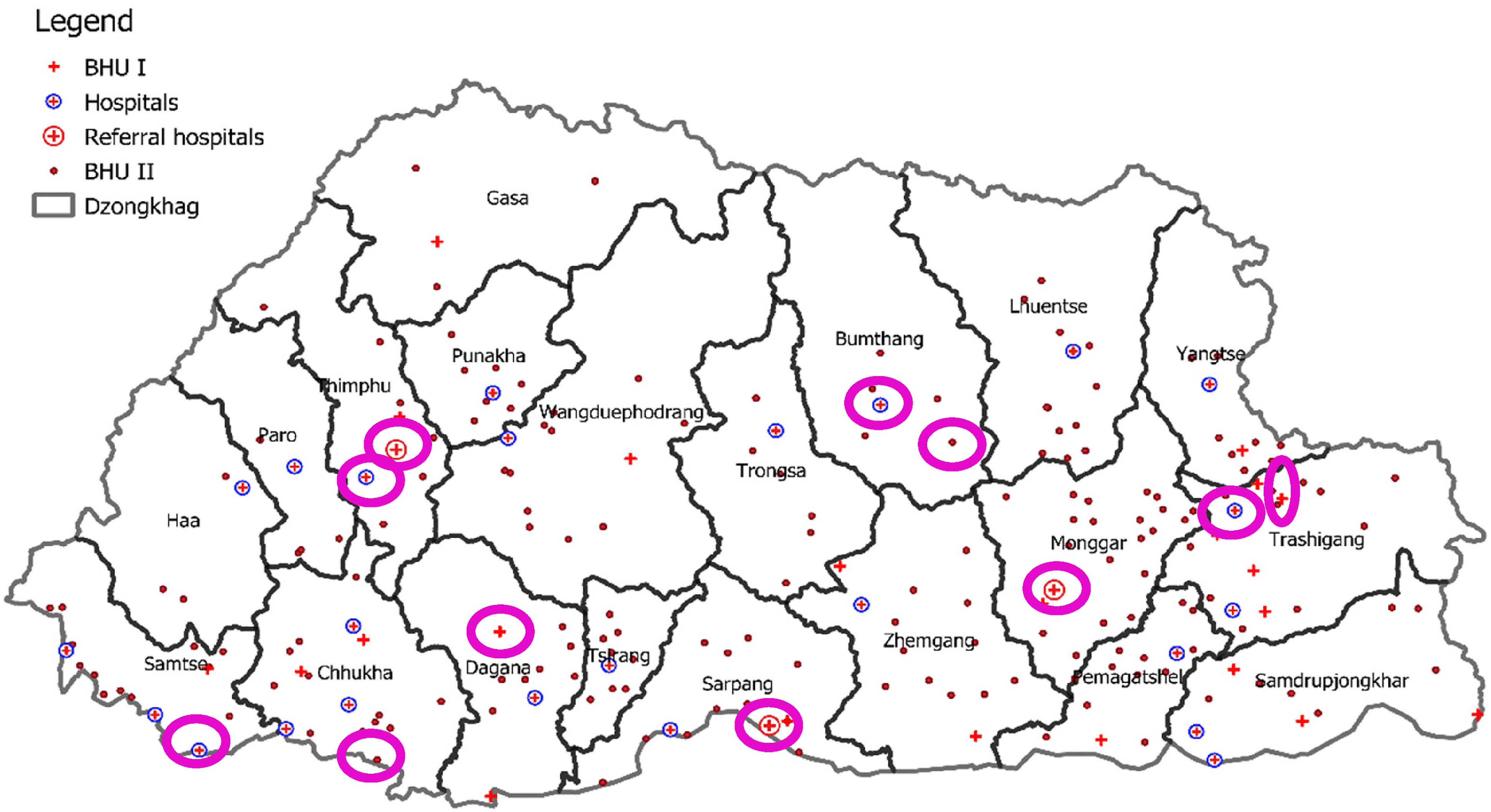
Map of Bhutan showing the study sites indicated within the circles. (Used with permission from the Policy & Planning Division, Ministry of Health, Bhutan).
Firstly, patients with advanced illnesses (cancer, organ failure, motor neuron disease, dementia, HIV/AIDS and MDR-TB) or at end-of-life (acutely dying irrespective of the diagnoses) were identified with the help of health professionals at each study site. In Bhutanese hospitals at least one family member is present continuously with the patient. Inclusion criteria included participants to be a primary caregiver, 18 years or older, able to provide informed consent and interested/willing to participate in the study. The identity of a primary caregiver was confirmed with the patient if conscious and capable. To recruit participants at home, a snowball sampling strategy was applied where clinicians in the hospitals informed TDL (principal author) about the location of chronic patients in the communities. TDL visited those patients at their homes and then approached the eight eligible family members for participation in the study. The fieldwork involved simultaneous data collection among patients with advanced illnesses and healthcare professionals. Given the duration of fieldwork, number of study sites and amount of work involved, a sample size of 70 to 100 family members was initially planned. However, several challenges, described in the ‘field notes’ section, resulted in recruiting only 46 family members, 41 from the identified hospitals and five from the communities, by the end of fieldwork.
Materials
A structured questionnaire was developed including socio-demographic characteristics, duration of caring, awareness of patient's diagnosis, and the 14-item Carer Support Needs Assessment Tools (CSNAT). The latter is an evidence-based, comprehensive tool to assess support needs of informal carers with good face, content and criterion validity.30,31 It includes assessment of physical, psychological, social, spiritual, financial and practical support needs of family members/friends caring for very ill or dying patients. 30 The CSNAT items are measured in four categories: no (1); a little more (2); quite a bit more (3); and very much more (4). 31 Total CSNAT scores can range from 4 to 56. Given the complexities of low literacy levels and the prevalence of several non-written dialects, translating the CSNAT was not undertaken. Permission to use the tool was obtained from the developers.
A pilot test was planned for 7 to 10 family members, 10% of the initially planned sample size, 32 at the identified study sites. However, since TDL is based in Australia, her healthcare colleagues in Bhutan, who volunteered to collect the pilot data on her behalf, faced challenges in recruiting family members who were willing to participate, given PC is a new concept. They also found it time consuming to conduct face-to-face interviews as most of the potential participants were illiterate. Hence, only four family members participated in the pilot test which performed well regarding feasibility, clarity and sensitivity of the questions.
Data Collection
The majority of the family members were illiterate. In Bhutan, the adult literacy rate is 66.6%. 33 Dzongkha, the national language, and English are the languages of instruction in schools. Those who are illiterate or not from western Bhutan cannot speak Dzongkha and most other dialects are only spoken and not written. Hence, for the illiterate family members, face-to-face interviews were conducted by TDL, who is fluent in all the main dialects of Bhutan, by translating the questionnaire at the bedside and then completing it in English based on the responses. When responses were not clear, TDL involved the local healthcare team to help clarify. Most family members preferred to participate at the bedside, however, in the intensive care units participants were interviewed in a separate room. Participants who could read and write English were offered to complete the survey but many preferred to fill the questionnaire along with the researcher. Only 11 participants completed the questionnaire independently.
Data Analysis
Statistical analyses were conducted using Statistical Analysis System software, version 9.4. 34 Descriptive statistics (mean, standard deviation, frequency and percentage) were produced. Independent samples t-test, pending satisfactory normality checks, was used to compare the means between family members caring for cancer and non-cancer patients. Logistic regression was used to assess the statistical significance of potential predictors of level of needs which were categorized as low (14-43) and high (>43-56). These cut offs were decided based on the distribution of the actual data obtained. Logistic regression models were performed separately for carers of cancer patients and those of non-cancer patients, as evidence indicates that their support needs vary. 35 Statistical significance was set at α = 0.05.
Ethical Approval
This study was approved by the Human Research Ethics Committee at the University of Western Australia (RA/4/20/4990) and the Research Ethics Board of Health in Bhutan, (REBH/Approval/2018/097). Permission to access the participants was granted by the executive of each study site. Informed consent was taken in the form of signature or thumb print.
Field Notes
Field notes were maintained to record experiences during field work. Several unforeseen challenges hindered data collection. Following a severe cyclone 36 which resulted in a tragic bus accident, 37 the government issued a caution against public travel. Recruitment was slower than expected because the concept of PC was so unfamiliar it took a long time to explain to patients and families. Face-to-face interviews were time consuming.
Results
Among 60 eligible participants identified, 46 (77%) agreed to participate. Reasons for refusal included lack of awareness of PC (29%), too distressed about the relative's condition (14%) and being busy (14%). One participant did not believe, despite explanation, that this was research, believing it was a type of online business. One participant could not provide consent due to hearing deficit. The remaining (29%) participants did not provide any specific reason.
Sociodemographic Characteristics
Family members’ age ranged from 24 - 72 years (mean 42.9, SD 10.1). The sociodemographic characteristics are summarized in Table 1. These characteristics are also not significantly different from those of the pilot sample (see Appendix 1).
Sociodemographic Characteristics of the Participants (n = 46).
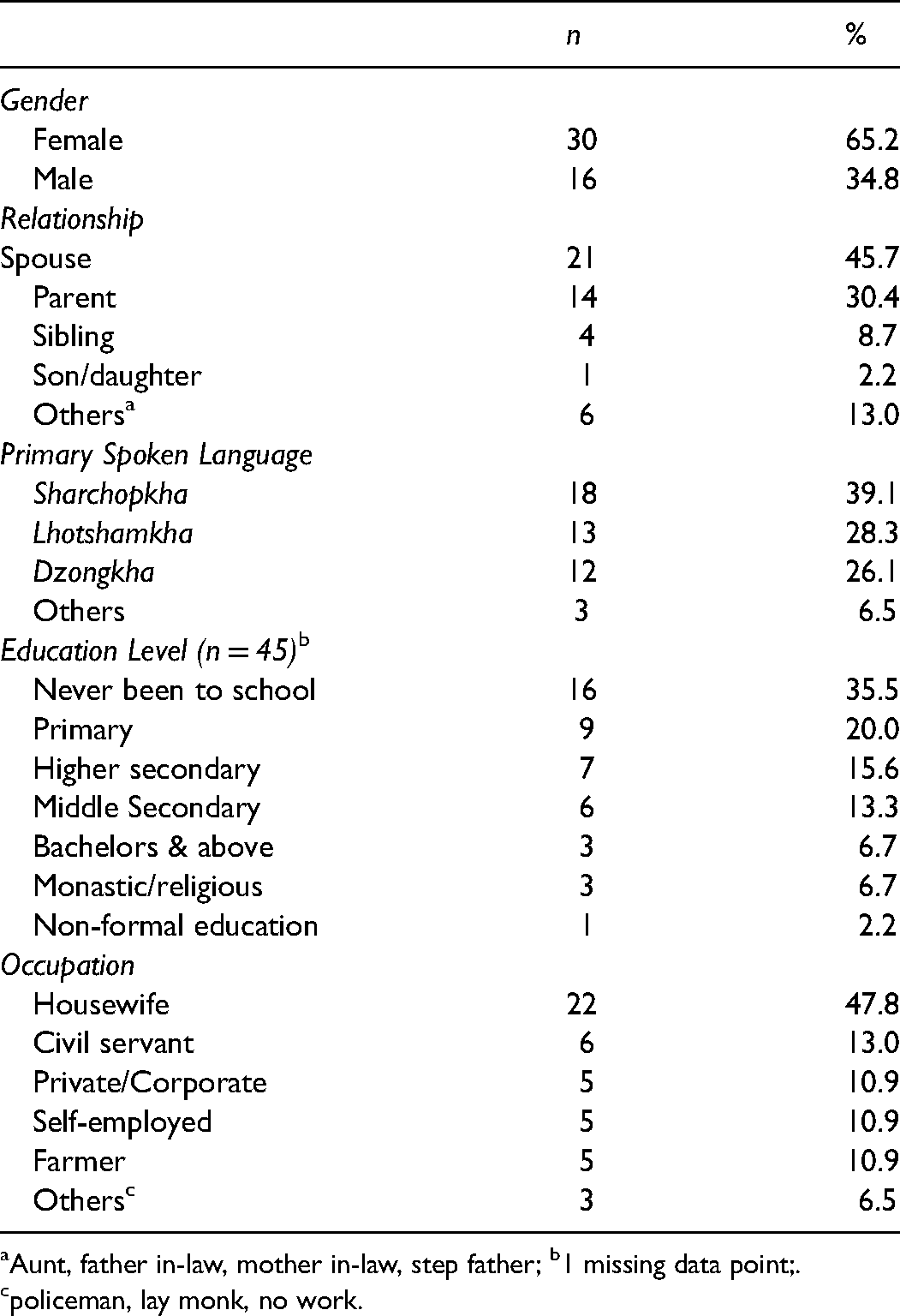
Aunt, father in-law, mother in-law, step father; b1 missing data point;.
policeman, lay monk, no work.
Duration of Caregiving and Awareness of Diagnosis
The duration of caregiving ranged from <1 month to 15 years. Forty-three (94%) family members knew the diagnosis of their loved one and 29 (63%) mentioned that their sick relative also knew. The diagnoses of their loved ones are presented in Figure 3. Three elderly patients were bedridden: one had a massive bedsore, another had a below knee amputation and the third was very frail.
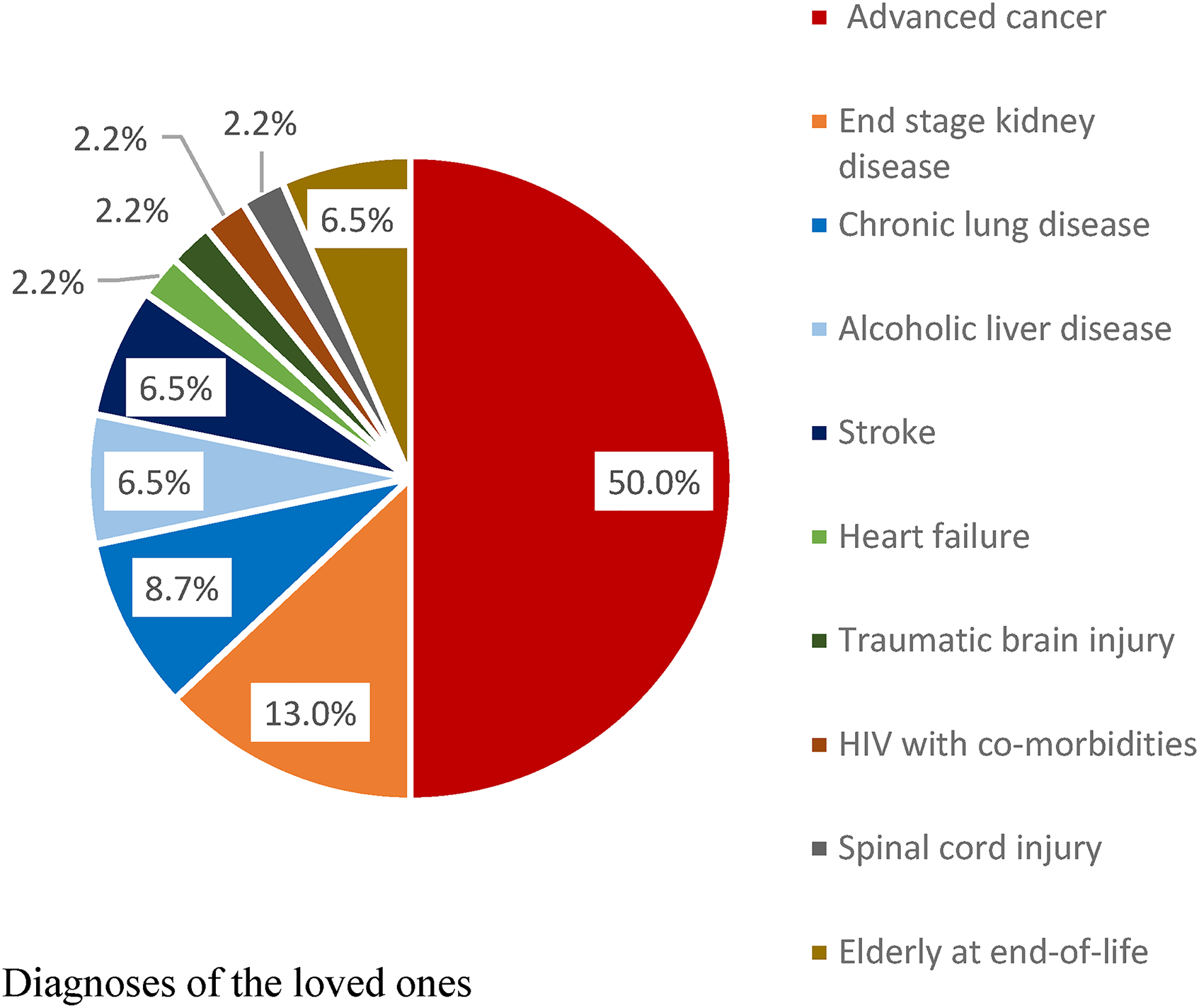
Diagnoses of the loved ones.
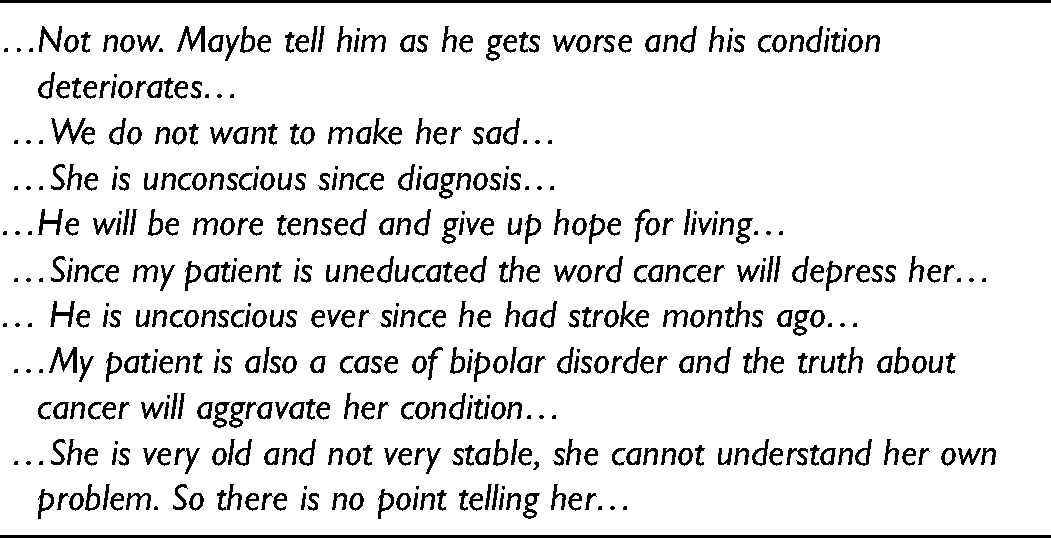
Among the 17 (37%) who said their sick relatives did not know the diagnosis, 9 (53%) wished that they knew. The remaining 8 (47%) did not want their relative to know the diagnosis and the reasons are presented in Table 2.
Reasons why Family Members did not Wish to let their Relative know the Diagnosis (n = 8).
Support Needs for Family Members
Family members indicated that they required substantial support in almost all domains of CSNAT (see Figure 4). Maximum support (‘very much more’) was required by >50% participants in the areas of understanding their relatives’ illness, managing symptoms, providing personal care, financial and legal aspects, dealing with their own feelings and emotions and knowing what to expect in the future. A significant amount of support (‘quite a bit more’ + ‘very much more’) was needed by >65% of participants for the following questions: whom to contact if needed; time for family members themselves; understanding and reflecting on their own beliefs and spirituality; practical help at home; and, getting a break overnight.
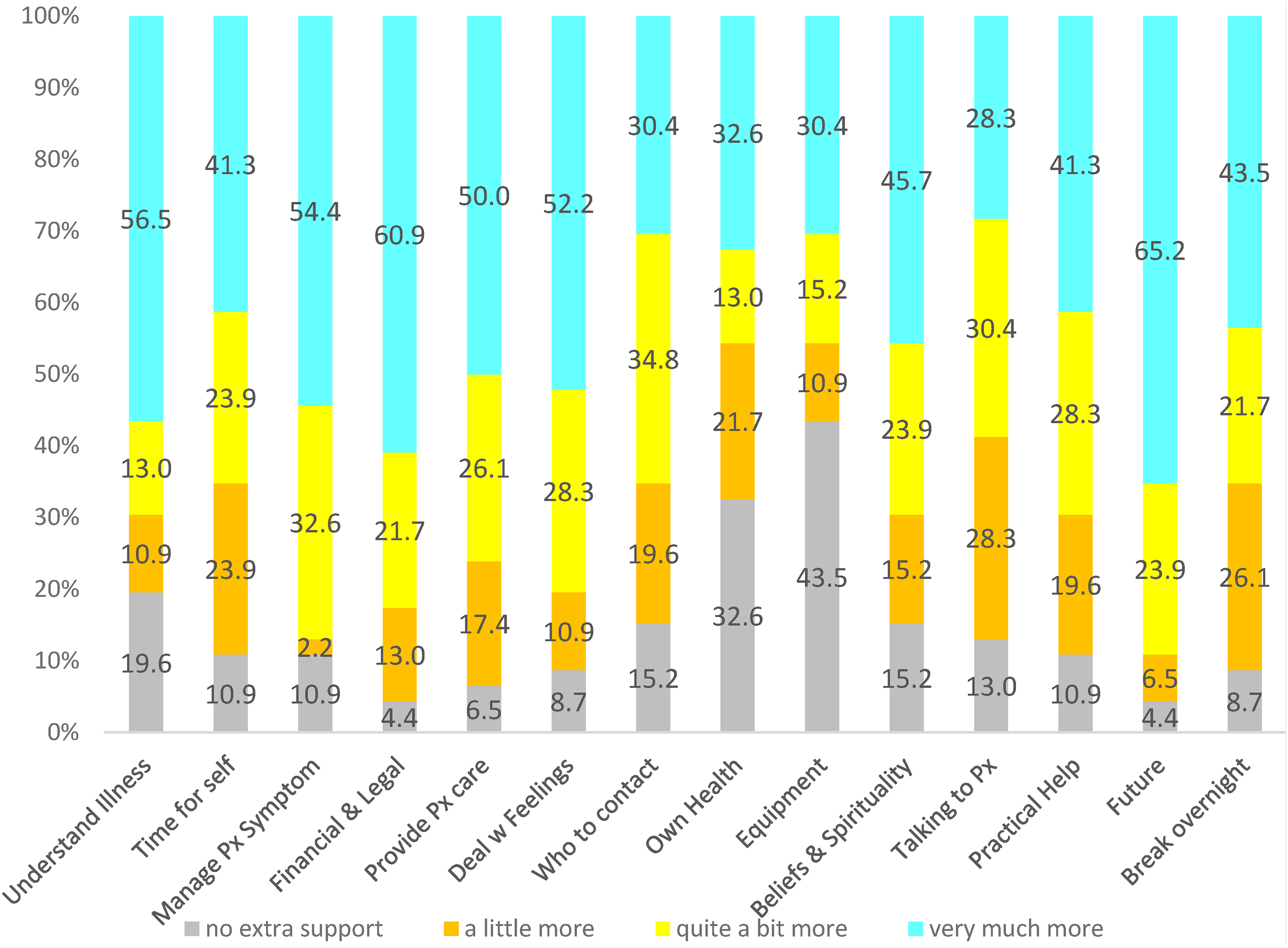
Percentage of family members expressing need for more support with each item of the CSNAT.
There was no significant difference in the needs of family members caring for cancer patients when compared to those caring for non-cancer patients (difference 0.7; 95% CI −4.8, 6.1, P = .811). Potential predictors of higher total CSNAT scores including age (> = 45 vs. <45), gender (male vs. female), level of education (primary and below vs. above primary) and duration of care (<1 year vs. > = 1 year) were assessed. Family members caring for non-cancer patients for less than one year were 7 times more likely to report high support needs than those caring for non-cancer patients for more than one year (Table 3), although it did not reach statistical significance (P = .054).
Assessing Statistical Significance of Potential Predictors of High Levels of Needs Reported by Family Members (n = 46).
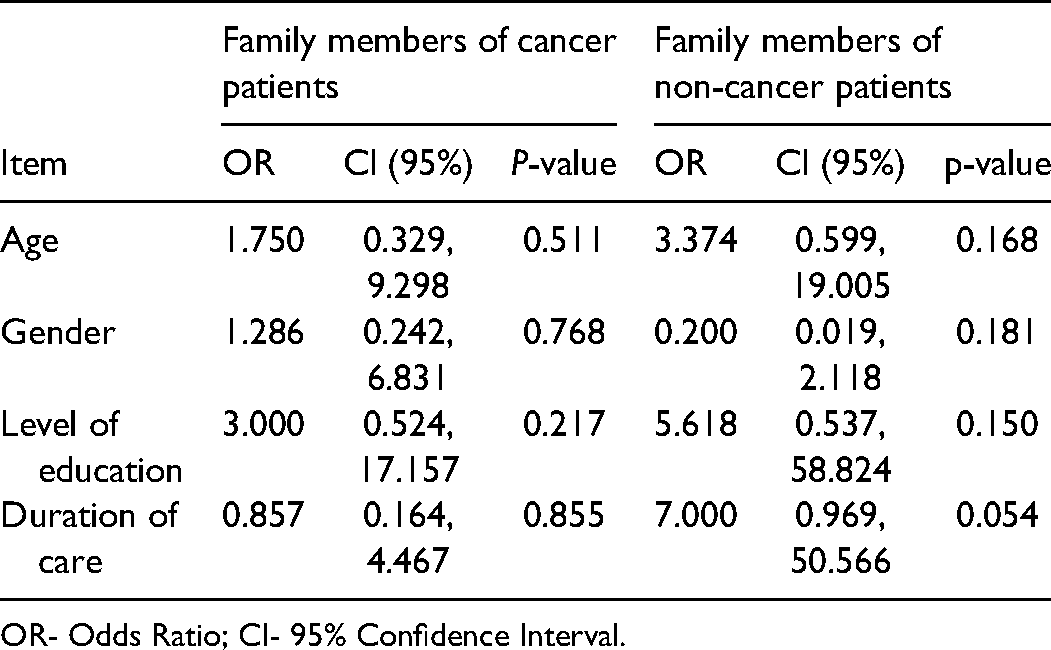
OR- Odds Ratio; CI- 95% Confidence Interval.
Discussion
The World Health Organization (WHO) recommends integration of PC using a public health perspective with a focus on four key strategies: policies; PC medicines (opioids in particular); education, training and awareness; and implementation.38,39 The assessment of the specific PC needs of patients, families and healthcare providers within a community should contribute towards the service model. 11 Accordingly, for Bhutan, PC needs among patients with advanced illnesses was explored. 28 Concurrently, besides this study, studies on the perspectives of healthcare professionals on the need for PC and how it should be delivered are underway. The findings of these studies are expected to drive policy changes to integrate PC into the Bhutanese healthcare system.
According to the WHO ‘support for family caregivers is a core aspect of palliative care provision.’ 2 (p13) This study found that the majority of family members caring for very ill loved ones had high support needs. They needed significant support across two broad areas: support that enabled care for their sick relative, and support that related directly to their own well-being. This is consistent with Ewing's study 30 which found that the support needs for family members were distinctly identified in the same two domains. Although family caregivers are often positive about their role, they face considerable challenges related to physical, emotional, financial and social impacts when caring for terminally ill relatives.40,41 The negative ramifications of caregiving can result in family members becoming ‘secondary patients’42,43 with their needs often equal to, or even greater than, those of the patient.2,7,18
This study indicated that many participants did not have a reliable source of income and the majority (83%) needed “very much more” financial and legal support. Those who were interviewed face-to-face reinforced that the financial component was very important. Although medical treatment including referral abroad is funded by the government, 44 families in Bhutan often incur huge additional expenses when caring for very ill relatives. Many take their loved ones abroad privately even when the government health panel does not recommend. The need for repeated travel to referral hospitals for advanced treatment is often a financial burden to the family. Further, Bhutanese strongly rely on traditional healing practices when confronted with life-limiting illness. 45 Many of the rituals, prayers, offerings and other traditional healing practices involve huge expenses.
The findings of this study are consistent with other studies in developing countries. In Malawi, the need for financial support among family members caring for HIV/AIDS patients was critical along with the need for respite support, training and education. 46 Thus, socioeconomic interventions were considered a core component of their PC model. 47 In Kerala (India), the Trivandrum Institute of Palliative Sciences support families through food kits, financial help and educational opportunities for children who are at risk of dropping out of school due to poverty aggravated by family illness. 48 In Bhutan, since financial support was also a significant need among patients with advanced illness, 28 PC services should include financial support as a key element.
The majority of the family members in this study reported a need for more information as they cared for their very ill loved ones. This is consistent with the findings of studies even in developed countries where ‘what to expect in the future’ was the highest need expressed.30,49 Lack of information from health professionals on the patient's prognosis left family caregivers feeling mentally unprepared as patient's condition deteriorated.50,51 Trained PC professionals can provide adequate information in an empathic way about the illness, available treatment options and what to expect in future which can reduce fear and anxiety among patients and family members. 2 In developing countries, since end-of-life care is largely provided by family caregivers, enhancing their knowledge and skills is crucial. 52 A study in China described educational programs for families in topics like dealing with emotions, talking about death and dying, being aware and respecting patients’ rights, and making decisions. 53 Such programs may be applicable in Bhutan.
Although evidence indicates that family members caring for cancer patients have a higher burden, 35 there is less literature on the family support needs for non-cancer conditions. 7 In this study, half of the participants were in the latter group. Despite our small sample size, the study found that family members caring for non-cancer patients for less than one year were more likely to report high support needs than those caring for more than one year. With regard to diagnosis, although all patients in the concurrent study 28 wanted to know their diagnosis, not all family members in this study were willing to disclose, mainly for fear of causing additional distress and hopelessness. Willingness to disclose a diagnosis, particularly of incurable cancer, is known to depend on social context, cultural norms and family traditions. 54 In Pakistan, a culture-sensitive society, 55 the majority of patients wanted truthful disclosure of their cancer diagnosis but the relatives did not reveal. 56 Despite their religion's emphasis on truth, diagnoses were often concealed as acts of love and compassion. 57 In Bhutan, adequate support from PC trained professionals, counselors, social workers and spiritual leaders may enhance family members’ understanding of the importance of truth telling.
Family members during caregiving and bereavement expect support that respects family beliefs and values.2,58 This is particularly crucial in Bhutan where caregiving is largely determined by culture and the spirituality of the family and community. Thus, PC models developed elsewhere cannot be replicated for Bhutan. It has to be unique to its socio-economic, cultural, and spiritual context.59,60 Dame Cicely Saunders, the founder of the modern hospice and PC movement, stated “Go around and see what is being done and then see how your own circumstances can produce another version; there is need for diversity in this field.” 16 (p 47)
Palliative care, an important public health response,38,61 is designed to address the needs of both patients and family caregivers. 40 Appropriate support of caregivers improves their quality of life and also facilitates better symptom control and increased patient survival.62,63 In developed countries, to alleviate caregiver stress and burden, several practical community services exist, including support groups, adult-day care, in-home assistance, home care nursing, respite services, social networking, problem-solving and education.43,64,65 Some of those may be applicable to Bhutan. Effective family support can also help reduce the overall healthcare costs by reducing unnecessary visits to the emergency department and prolonged hospital admissions at the end-of-life.2,66
Strengths and Limitation of the Study
A strength of this research was the distribution of sites across the country where TDL could include family members with varying cultural and belief systems in response to chronic illness, dying and post-death rituals. The study findings can be widely applicable within Bhutan and maybe generalized to other developing countries with similar socio-cultural contexts.
However, the sample size is small. Recruiting those 46 family members involved substantial challenges and, hence, may be difficult for others to repeat. The experiences of those living with poverty in remote locations and speaking different dialects can be hard to research and this study has allowed them a voice.
Conclusion
This study has highlighted important family caregiver considerations to inform the development of a public health-focused PC model modified to Bhutanese culture and spirituality, socioeconomic circumstances and healthcare system, as recommended by the WHO.
Footnotes
Acknowledgments
We would like to thank our family member participants who participated despite knowing that there was no benefit to their ailing loved ones but with faith that the research will make a difference in the future.
Authors’ Contributions
TDL collected the data and prepared the manuscript. CJ conceived the idea. CS, CJ and KA reviewed and edited the manuscript. All authors read and approved the final manuscript. HN performed the quantitative data analyses, provided interpretation for these results, and reviewed and edited the manuscript.
Availability of Data and Materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical reasons.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval was provided by the Human Research Ethics Committee at the University of Western Australia and the Research Ethics Board of Health in Bhutan with Reference numbers, RA/4/20/4990 and REBH/Approval/2018/097, respectively. Informed consent was taken from every participant in the form of signature or thumb print.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.