
Abstract
Introduction
In 2020, an estimated 6000 Canadians were diagnosed with pancreatic cancer and with 5300 deaths. It was the fourth leading cause of cancer-related death among Canadians. 1 Globally in 2020, an estimated 495 773 people were diagnosed with pancreatic cancer and 466 003 died. 2 Lack of cost-effective screening methods and early-stage symptoms result in late stage detection3–5; over 60% of pancreatic cancers are diagnosed at stage III or IV, limiting curative treatment options 1 and resulting in very poor prognosis. One-year survival rate is about 21% 6 and 8% for five-years. 7
With such poor prognosis, pancreatic cancer patients may be referred to palliative and other home care services to support the end-of-life period. These health care services aim to improve the quality of life for patients with late stage pancreatic cancer. Home care provides a wide range of healthcare and other supportive services in patients’ own homes that include personal support/homemaking, physiotherapy, occupational therapy, nurse/physician visits, and palliative care. Home care is shown to be beneficial to patients’ quality of life, and reduce all-cause mortality, and hospitalizations. 8
Palliative care services address complex symptom management issues, aiming to improve the end-of-life experience, which is particularly important in advanced pancreatic cancer with severe symptoms. 9 A meta-analysis involving 23 studies with over 37 500 patients has shown that palliative care reduces symptom burden and increases the chance of dying at home, particularly for cancer patients. 10 In Ontario, home care and outpatient palliative care assessments have been observed to decrease the odds of emergency room visits, intensive care unit admissions, and treatment with chemotherapy in the last two weeks of life. 11 In addition to allowing patient to feel in control of their health, home-based palliative care has been shown to further reduce symptom severity compared to in-hospital care. 12 While most people prefer dying at home,13–16 the majority of deaths occur in hospitals. 17 Palliative home care is rarely offered.18,19 When it is provided, it is often delivered late in the disease process. 18
Despite the poor prognosis and known trajectory of functional decline that often renders a person homebound, little is known about home-based palliative care (referred to as palliative home care in this study) use by pancreatic cancer patients. Furthermore, end-of-life outcomes such as place of death and quality of life are rarely examined in this patient population. This study aimed to to describe the utilization of home care services among patients with pancreatic cancer. In addition to that, this study attempted to investigatefactors associated with early-onset palliative home care as well as the impact of home care services on survival and out-of-hospital death.
Methods
Study Design
Study population
This population-level observational retrospective cohort study used encrypted Ontario universal health administrative data housed at ICES (formerly known as the Institute for Clinical Evaluative Sciences). Data sources were linked through anonymized and de-identified health card numbers. ICES privacy procedures and policies were followed throughout data handling. All incident cases of pancreatic cancer diagnosed in the province between April first, 2010 and March 31st, 2016 were captured from the Ontario Cancer Registry (OCR) using International Classification of Diseases revisions 9 and 10 (ICD-9/10) diagnosis codes of 157.X and C25.X respectively. Follow-up occurred until March 31st, 2017, one year after the end of the study window. Patients with missing demographic information, stage 0 pancreatic tumors, pancreatic neuroendocrine tumors (PNETs, ICD codes 157.4 or C25.4), and patients with a previous cancer diagnosis (within OCR records as early as January first, 1964) were excluded.20,21 Previous cancer diagnoses were excluded as including them would make it impossible to determine whether initiation of home care services was secondary to pancreatic cancer diagnosis, or simply progression of another previously diagnosed cancer. Furthermore, excluding these patients reduces the possibility that patients with non-primary pancreatic cancer are included. Patients that received home care were identified through the Home Care Database (HCD) which captures all home care services provided or organized by 14 Local Health Integration Networks (LHINs) across Ontario. Ontarians have access to universal, publicly-funded healthcare services that are deemed medically necessary, including home care. Patients were also excluded if they received home care service within 2 years prior to pancreatic cancer diagnosis as this investigation aimed to study new home care utilization following diagnosis.
Variable definitions
Registered Persons Database (RPDB) was used to capture the sex, age at diagnosis, and death date if applicable. Postal codes from census data at Statistics Canada were used to determine whether patients were in a rural or urban region of the province as well as the neighborhood income quintile. OCR was used to determine the stage of the pancreatic adenocarcinoma at diagnosis. Comorbidities were captured based on Ontario Health Insurance Plan (OHIP) and Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD), and included 16 chronic conditions, some of which have been chart-validated. 20
Primary outcome
The primary outcome of this study is utilization of publicly-funded home care. Receipt of home care was defined as having received a home care service captured in the HCD. Home care services were classified as short-term, long-term, or palliative, based on service recipient codes that are used to organize service lines through the LHIN (Appendix 1). Patients that received only short and long-term home care services (ie no palliative home care) were defined as patients that received general home care. Patients that received short and/or long-term home care services prior to palliative home care services were defined as patients that received transition-to-palliative home care. Lastly, patients that received palliative home care services prior to any other home care service were defined as early-onset palliative home care.
Secondary outcomes
The secondary outcomes of this study are survival and out-of-hospital death. Survival was defined as time from diagnosis of pancreatic cancer to date of death within a one year follow-up period after the study window. Patients that died after March 31st, 2017 do not have a recorded death in this study. Patients with death records in acute care (CIHI-DAD), complex continuing care (Continuing Care Reporting System), and rehabilitation facilities (National Rehabilitation Reporting System) were considered to have had an in-hospital death. All other patients, including dying in nursing homes (Continuing Care Reporting System), hospices, and retirement homes were considered to have had an out-of-hospital death as these centers are intended for longer stays in patients that do not require highly active medical management or are palliative.
Statistical Analysis
Patient characteristics (age group at diagnosis, sex, rurality, income quintile, stage of pancreatic cancer at diagnosis, multiple morbidities) were compared between those that received any home care service and those that did not using a t-test for continuous variable comparisons and a chi-square test of independence for categorical variables. Multiple logistic regression analysis was used to determine the adjusted odds for receipt of early-onset palliative home care. A multiple logistic regression analysis was conducted to predict the adjusted odds of dying outside of a hospital with adjustment for each home care category. Significance was taken at a two-sided P-value of less than .05. Statistical analysis was conducted using SAS Enterprise Guide 7.1.
Ethics
This study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre in Toronto, Canada.
Results
Cohort
Between April first, 2010 and March 31st, 2016, 10 270 Ontarians diagnosed with pancreatic cancer between the ages of 18 and 105 years were identified (Figures 1 and 2). Excluded persons include 28 with insufficient demographic information, 67 diagnosed with pancreatic neuroendocrine tumors, 1670 with previous cancer diagnosis, and 1617 patients who received home care services within two years of their diagnosis. The final study cohort included 6888 patients with pancreatic cancer.
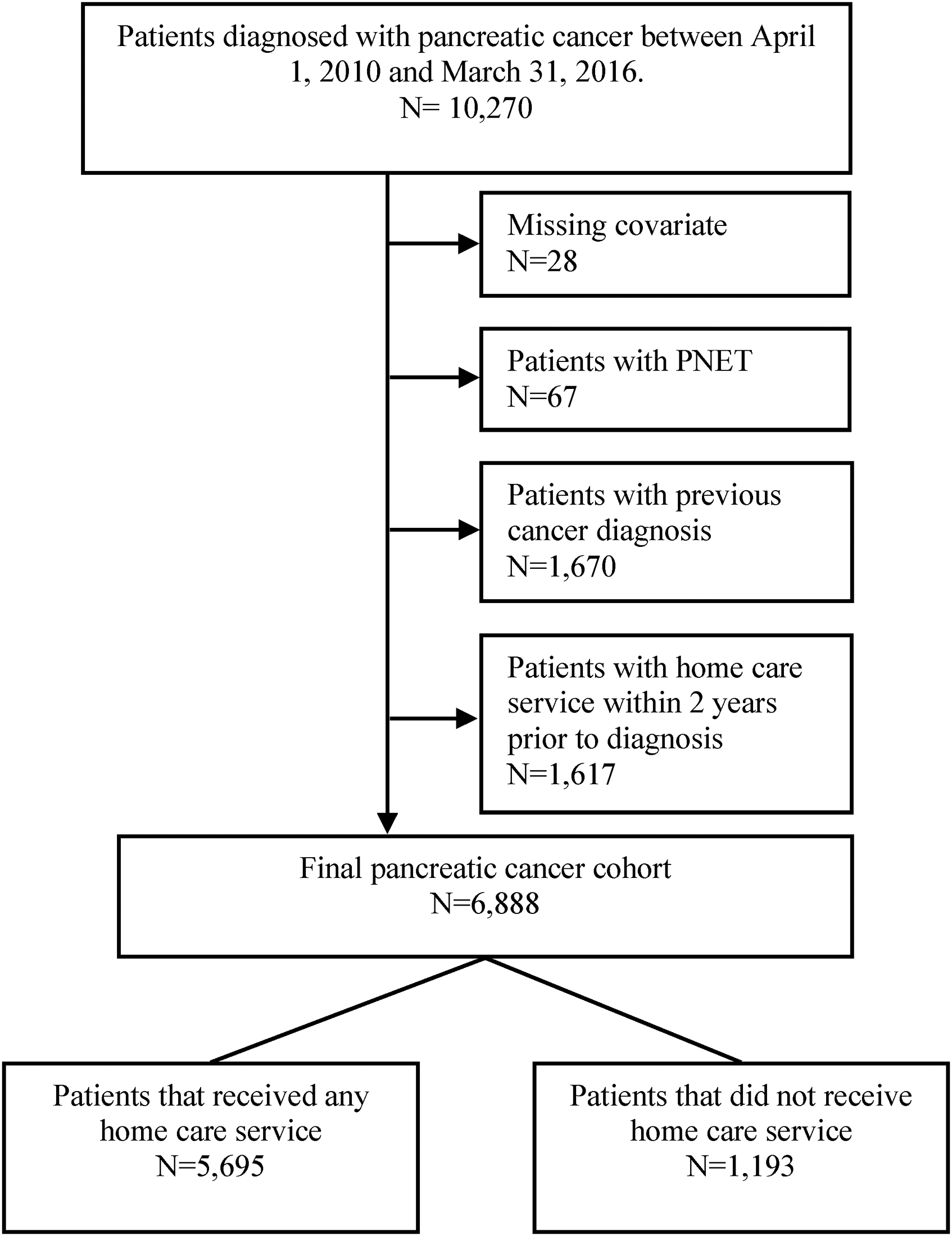
Study flow diagram.

Timeline of home care utilization by different types of home care. First respective home care service post-diagnosis shown in Green (), last respective home care service before death shown in yellow ( ), death shown in red (
), death shown in red ( ). Blue (
). Blue ( ) indicates start of palliative care service in the transition-to-palliative home care group.
) indicates start of palliative care service in the transition-to-palliative home care group.
Home Care Utilization
A total of 5695 (83% of the cohort) had received at least one eligible home care service. Of which, 1780 (31%) received general home care services only, 2137 (38%) received transition-to-palliative home care, and 1778 (31%) patients received early-onset palliative home care (Table 1). A higher proportion of young patients (18-44 years) have received no home care services (6% vs. 3%) as well as a higher proportion of older (85+ years) patients (10% vs. 5%). A significantly higher proportion (P = .02) of patients that received home care reside in a rural region compared to those that did not receive home care services (14% vs. 12%). Compared to patients that did not receive home care, patients that received home care had a greater proportion of stage 2 (12% vs. 5%), 3 (8% vs. 3%), and 4 (30% vs. 16%) pancreatic cancer (P < .01). However, patients that did not receive home care had a greater proportion of stage 1 pancreatic cancer (9% vs. 3%) and missing stage information (68% vs. 47%).
Pancreatic Cancer Patient Characteristics for those that Received and did not Receive Home Care Services.
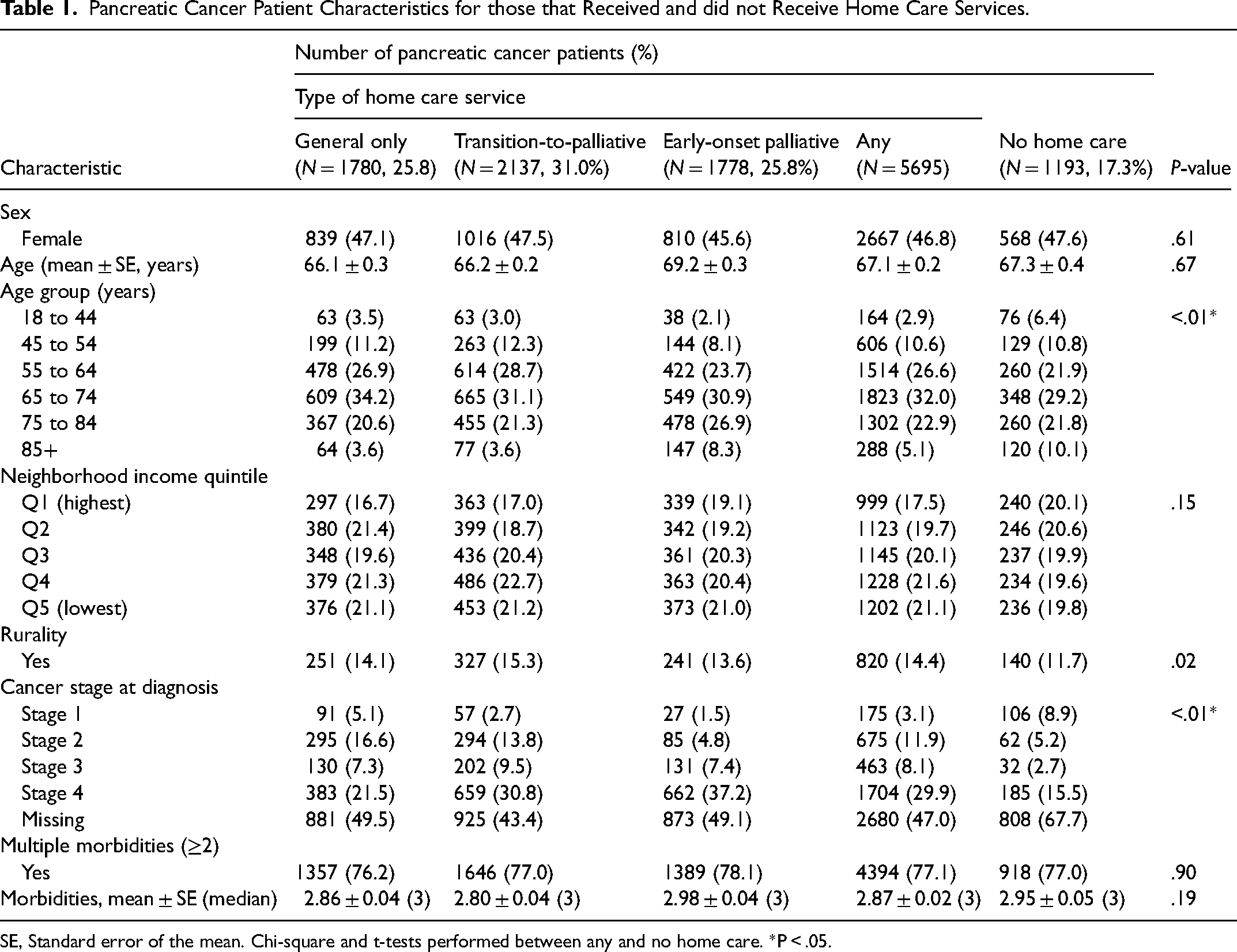
SE, Standard error of the mean. Chi-square and t-tests performed between any and no home care. *P < .05.
On average, pancreatic cancer patients received their first home care service 77 days after diagnosis with a median of 33 days (Table 2). Patients that received general home care services have their first home care service an average of 93 days after diagnosis, while patients that received any palliative home care received their first services earlier at an average of approximately 70 days after diagnosis. Since transition-to-palliative home care patients initially receive general home care prior to palliative home care, the time to palliative home care service was determined for this group and was found to be an average of 266 days with half receiving palliative home care within 155 days.
Home Care Utilization.
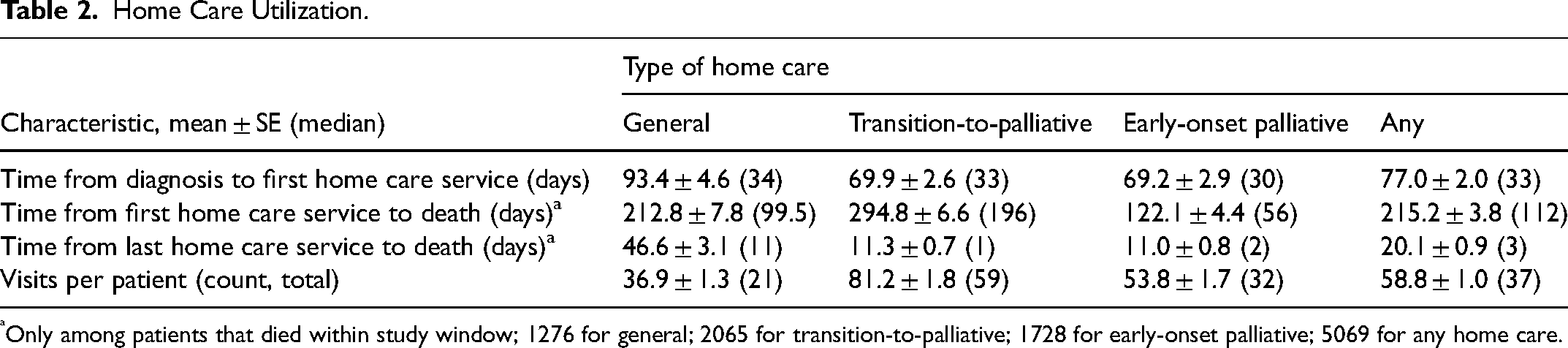
Only among patients that died within study window; 1276 for general; 2065 for transition-to-palliative; 1728 for early-onset palliative; 5069 for any home care.
Among decedents in this study, the overall average time from first home care service to death was 215 days with a median of 112 days (Table 2). The average time from last home care service to death was 20 days with half of these patients dying 3 days after their last home care service. General home care patients received home care services up to an average of 47 days prior to their date of death while patients that received palliative home care services received services an average of 11 days prior to death (Figure 3).
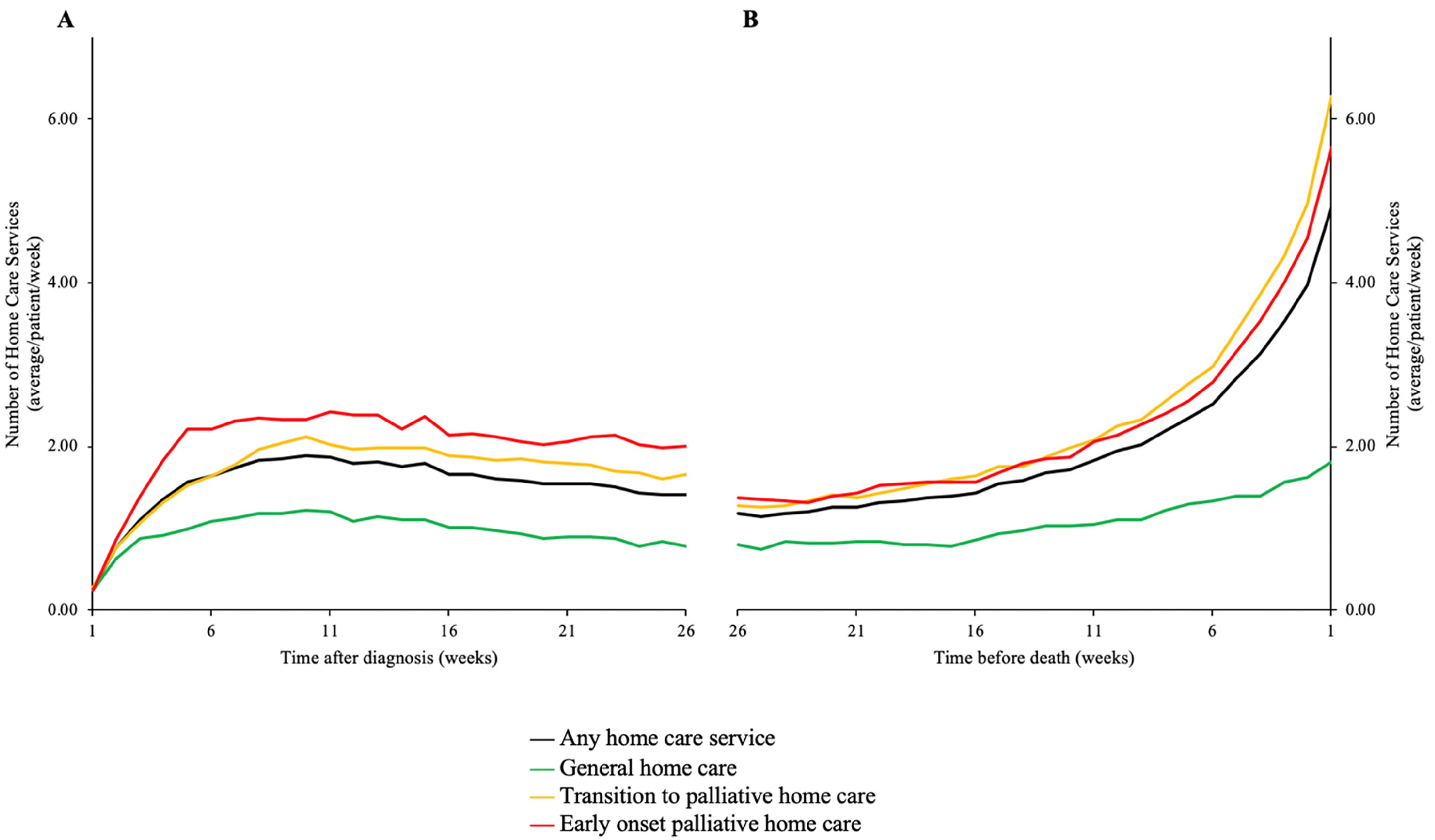
(A) average number of home care services per week for all surviving patients at a given week. (B) Average number of home care services per week for patients up to 6 months prior to death (only among deceased patients).
After diagnosis, patients in the early-onset palliative home care category received the highest intensity of home care services (Figure 3A) with an average of over 2 visits per week, peaking approximately 5 weeks after diagnosis. Transition-to-palliative home care patients received the next greatest intensity of home care, with a peak 2 visits per week around 11 weeks after diagnosis. Patients in the general home care category received the lowest intensity, peaking around 10 weeks after diagnosis with just over 1 home care visit per week.
For all decedent pancreatic cancer patients that received home care, intensity of home care visits increased rapidly prior to death (Figure 3B). The intensity is greatest for patients that received transition-to-palliative home care and early-onset palliative home care, where intensity jumps from just over 1 home care visit per week 6 months prior to death to approximately 6 visits per week in the last week of life. The increase in intensity of home care visits is not as marked in patients that received general home care.
Early-Onset Home Care
In the model that included all pancreatic cancer patients to determine the odds of receiving early-onset palliative home care, sex, income quintile, rurality and multiple morbidities were not found to be significantly associated with receipt of early-onset palliative home care (Table 3). Age was found to be strongly associated with receipt of early-onset palliative home care services. Patients aged 85 years and over had a 3.07 times increased odds (P < .01) of receipt of home care compared to those aged 18 to 44 years. The stage at diagnosis of pancreatic cancer was also associated with receipt of early-onset palliative home care with later stages of malignancy associated with increased odds of receiving this category of home care. Stage 1 and 2 pancreatic cancer patients did not differ significantly, while those with late-stage pancreatic cancer had increased odds, with the greatest being those with stage 4 disease (OR = 4.98, P < .01).
Logistic Regression Describing Factors Associated with Receipt of “Early-Onset Palliative” Home Care Service among Pancreatic Cancer Patients.
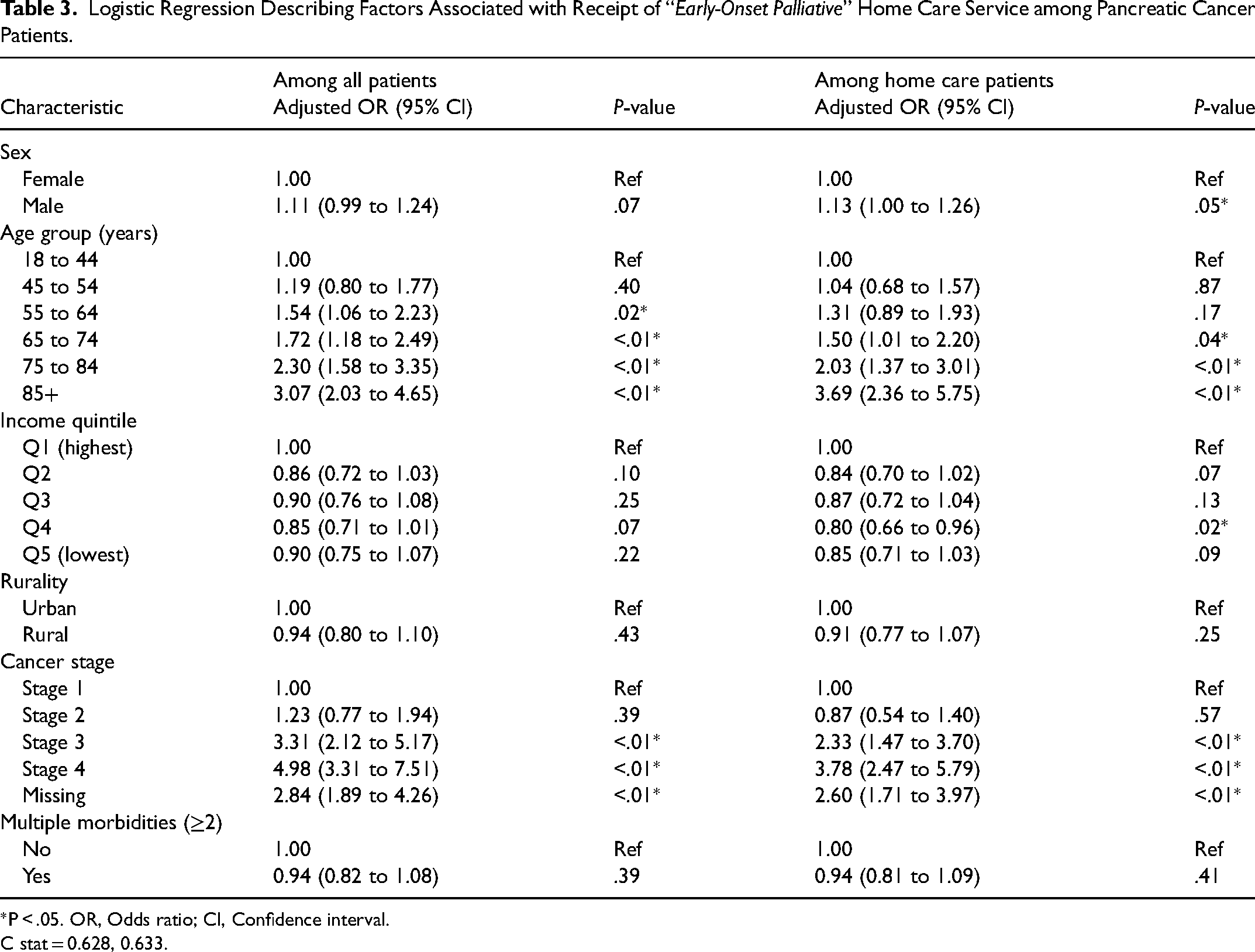
*P < .05. OR, Odds ratio; CI, Confidence interval.
C stat = 0.628, 0.633.
The model describing receipt of early-onset palliative home care that included only patients that received home care services (Table 3) was similar to the model that included all pancreatic cancer patients. One difference observed was that sex becomes a significant determining factor with males being 13% greater odds than females to receive early-onset palliative home care (P = .05). Furthermore, income quintiles approached significance where patients in the lowest income quintile have slightly greater odds of receiving early-onset palliative home care. This association is significant with respect to those that are in the second highest (Q4) income quintile, where patients in this category had 20% lesser odds (P = .02) of receiving early-onset palliative home care compared to the lowest income quintile. Stage of pancreatic cancer continues to be an important determinant of receipt of early-onset palliative home care. Later stage patients were at a considerably higher odds of receiving early-onset palliative home care with the greatest odds being for patients with stage 4 pancreatic cancer (OR = 2.60, P < .01).
Survival and Place of Death
Of the 6888 patients included in this study, 5893 (86%) died within the study follow-up period (Table 4). The overall average survival time among decedent pancreatic cancer patients (Table 4) is 260 days with a median of 152 days. Patients that received any home care service survived for an average of 287 days with a median of 186 days while those that received no home care survived for an average of 93 days with a median of 31 days.
Survival and Location of Death of Pancreatic Cancer Patients.
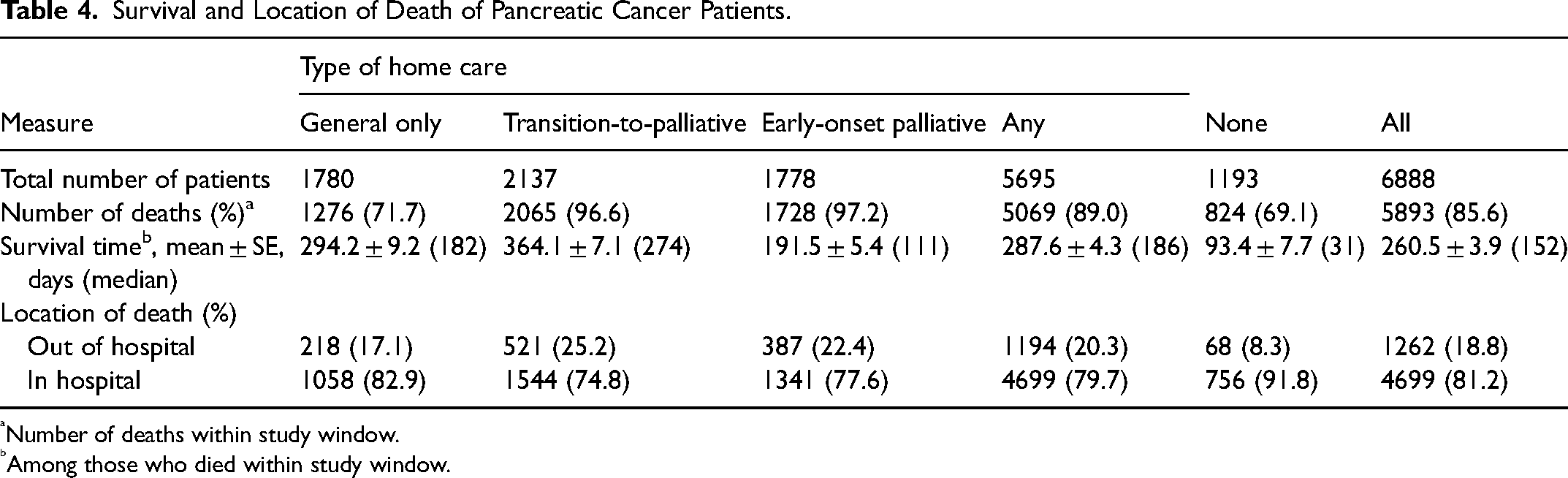
Number of deaths within study window.
Among those who died within study window.
Among decedent pancreatic cancer patients in this study, only 19% had an out of hospital death (Table 4). Only 8% of patients that did not receive home care experienced an out of hospital death. Among home care recipients, decedents that received transition-to-palliative home care had the highest proportion of out of hospital deaths at 25% while those receiving general home care had the lowest at 17%.
In the multiple logistic regression for prediction out of hospital death, each of the categories of home care was found to be significantly associated with an out of hospital death when adjusting for patient characteristics (Table 5). Patients that received transition-to-palliative home care had a 3.69 times increased odds of having an out of hospital death (P < .01) compared to those that received no home care services. Patients that received early-onset palliative home care had a 3.27 times increased odds of having an out of hospital death compared to those that received no home care (P < .01). Patients that received only general home care were also at increased odds of having an out of hospital death compared to patients that received no home care (OR = 2.26, P < .01). Furthermore, patients residing in a rural region of Ontario had a 38% higher odds of experiencing an out of hospital death compared to those living in an urban region (P < .01). Significant associations were not observed with respect to sex of patient, age group at diagnosis, income quintile, cancer stage at diagnosis, or presence of multiple morbidities.
Logistic Regression Model for Predicting Out of Hospital Death. Model based on Decedent Pancreatic Cancer Patients.
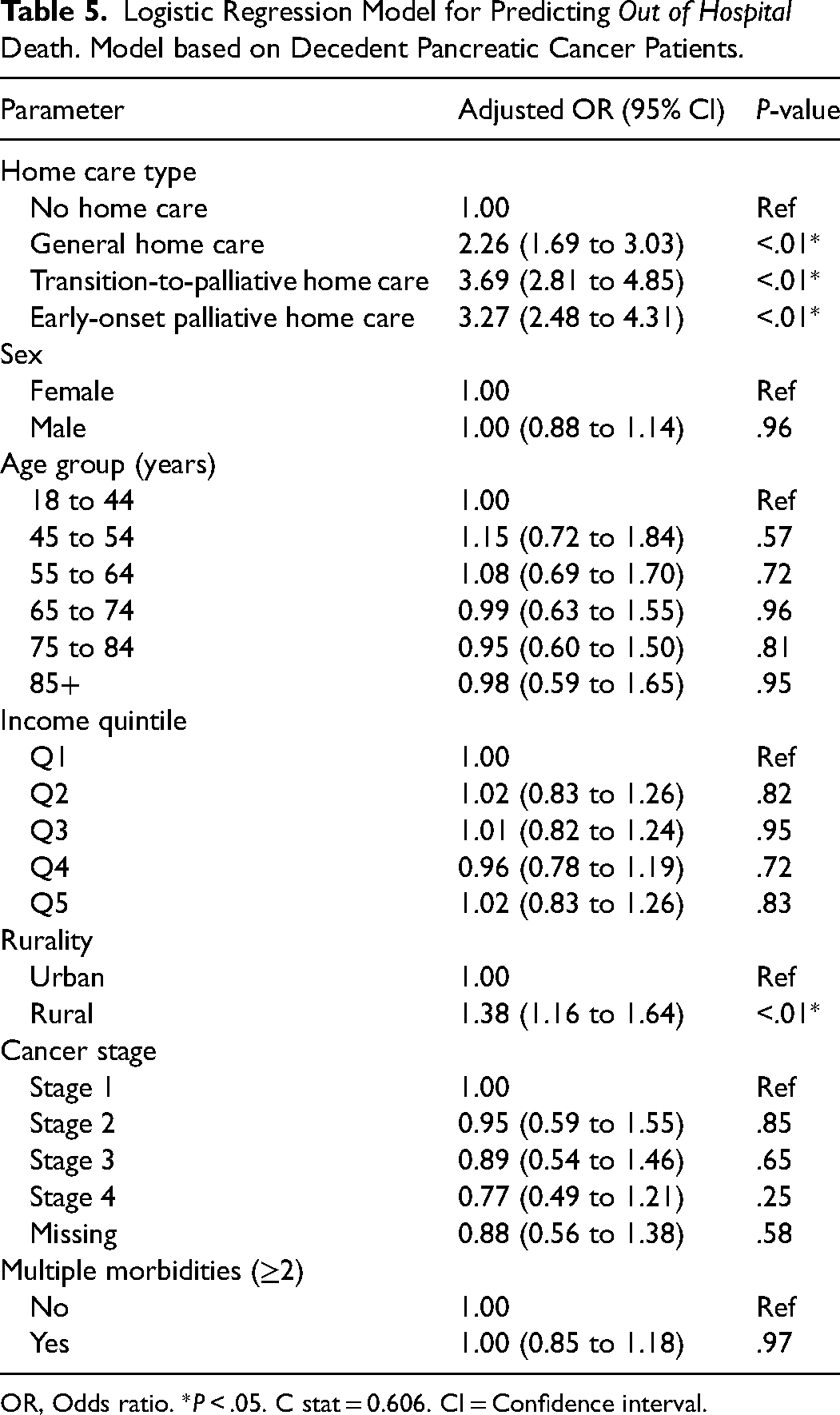
OR, Odds ratio. *P < .05. C stat = 0.606. CI = Confidence interval.
Discussion
This study has shown that a large proportion of patients (over 80%) diagnosed with pancreatic cancer received some form of home care after diagnosis, highlighting the high level of need for support with disease progression. Patients that received home care were generally found to be older patients and those with advanced cancer stage. This is further illustrated by findings in this study that most pancreatic patients (over 50%) receive some palliative home care, which is higher than the 20% of all Ontarians decedents in the last year of life. 18 Most of the home care received by these patients is palliative, emphasizing the relatively high recognition and anticipation of pancreatic cancer as a terminal, predictably progressive disease. Furthermore, we show that any form of homecare is associated with an increased odds of dying outside of the hospital.
This is the first study to extensively describe determinants of home care use by pancreatic cancer patients. Pancreatic cancer patients diagnosed at an older age or at a later stage are known to have a worse prognosis,5,22–25 consistent with our findings that they were referred to palliative home care at a higher rate. Patients that are younger may be healthier or have pancreatic cancer diagnosed earlier,26,27 hence not requiring home care. This is supported by results showing a greater proportion of patients that do not receive home care have stage 1 pancreatic cancer, which often can be treated with surgical resection.28,29 Furthermore, a greater proportion of patients that do not receive home care are missing cancer staging data, potentially because these patients died prior to staging. This study also demonstrates that advanced stage and older patients are also more likely to receive early-onset palliative home care. This shows a recognition of the severe disease burden in these patients, requiring faster palliative care at home. Interestingly, patients with multiple morbidities were not more likely to receive home care services. This is likely reflective of the seriousness of pancreatic cancer where this malignancy drives the need for palliative care.
With overall median survival for decedent pancreatic cancer patients in this study at around 5 months, it is important to receive home care services in a timely manner. In this study, it was found that patients receive their first home care service a median of 1 month after diagnosis, consistent for all three home care categories. This despite patients within the “early-onset palliative” home care category having later stage disease and worse survival (<4 months). One study conducted in Japan found that earlier referral to palliative home care services among patients with advanced cancer is associated with a higher chance of dying at home. 14 It may be beneficial to expedite initiation and delivery of home care services for patients identified as end-of-life and needing palliative care.
This study has shown that patients that receive a transition from general to palliative home care receive home care services closer to the date of death compared to those that receive general home care only. Decedent patients in the general home care category had a home care service a median of approximately 11 days prior to death while patients receiving palliative home care received a home care service 1 to 2 days prior to death. This suggests palliative home care ensures that care at home is provided in the last days of life, when needs are often high. These home care services, especially palliative home care, are believed to improve the end-of-life experience.30–32 Hence, it may be beneficial to closely monitor patients that initially receive general home care for possible transition to palliative home care.
Among decedents, intensity of home care services was found to be highest shortly before death. In the final weeks of life, however, general home care only received less than half of the number of home care services compared to patients that received palliative home care. This demonstrates that palliative home care provides more hours of service closer to death which may facilitate a better end-of-life experience.30–32
Among the common indicators of the quality of end-of-life experience is dying at home.13–16 Consistent with previous studies,33–36 our findings suggest that receipt of home care services increases the chances of dying outside of a hospital. This is the first study to demonstrate this among pancreatic cancer patients. While patients that receive palliative home care appear to have a higher odds of dying at home, even those that receive only general home care have over twice the odds of dying at home than patients that receive no home care. Although we adjusted for multiple morbidities as well as stage of malignancy, a remaining potential indication bias is that patients who receive home care must be at home to receive these services, and thus more likely to die outside of hospital. 34 In contrast to a previous study on all decedents in Ontario which found no association between rurality and place of death, 34 this study found that after controlling for receipt of home care, pancreatic cancer patient residing in rural settings were slightly more likely to die outside of hospital. One potential explanation is that pancreatic cancer patients living in rural regions may be further away from hospitals thus less likely to be transferred to a hospital at time of death. Future work will explore places of care, such as days spent in hospital in last 90 days of life, to better describe the end-of-life experience for these patients.
One limitation of this study is the large percentage of missing cancer staging data (about 50% of patients). This can be mainly attributed to death prior to radiological or surgical staging. Another limitation is that overall survival time is likely an underestimation due to the fact that only decedent patients were used. However, given that 86% of patients in this study died within the study window, the underestimation is not likely to be significant. Furthermore, the external generalizability of our study is limited to similar health care systems in developed countries with universal health care systems.
Conclusion
This study has demonstrated although the majority of pancreatic cancer patients receive home care, important differences exist in the healthcare experience and outcomes between patients that receive general home care and palliative home care. More work is required to investigate what factors influence the timing of the initiation of home care, how it can be improved, and how access to palliative home care can be more widely and appropriately available.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221075088 - Supplemental material for Home Care Use and Out-of-Hospital Death in Pancreatic Cancer Patients: A Retrospective Cohort Study
Supplemental material, sj-docx-1-pal-10.1177_08258597221075088 for Home Care Use and Out-of-Hospital Death in Pancreatic Cancer Patients: A Retrospective Cohort Study by Mehdi Hegagi, MSc, Paul James, MD, MSc, Amy Hsu, PhD, and Peter Tanuseputro, MD, MHSc in Journal of Palliative Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a research grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC) to the Ontario QUILT (QUality for Individuals who require Long-Term support) Network (#255) and from the Canadian Institutes for Health Research (201706PCG-385237-PCI-ADYP-219743). This study was also supported by ICES, which is funded by an annual grant from the Ontario MOHLTC. The views expressed in this paper are the views of the authors and do not necessarily reflect those of the funder. The funders had no influence on the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.