
Abstract
Objectives
Virtual reality (VR) opens a variety of therapeutic options to improve symptom burden in patients with advanced disease. Until to date, only few studies have evaluated the use of VR therapy in the context of palliative care. This case series aims to evaluate the feasibility and acceptability of VR therapy in a population of palliative care patients.
Methods
In this single-site case series, we report on six palliative care patients undergoing VR therapy. The VR therapy consisted of a one-time session ranging between 20 to 60 minutes depending on the patient's needs and the content chosen for the VR sessions. A semi-structured survey was conducted and the Edmonton Symptom Assessment System (ESAS) and the Distress Thermometer were performed pre- and post-intervention.
Results
Overall, VR therapy was well accepted by all patients. Five out of six patients reported having appreciated VR therapy. There were individual differences of perceived effects using VR therapy. The semi-structured survey revealed that some patients felt a temporary detachment from their body and that patients were able to experience the VR session as a break from omnipresent worries and the hospital environment (“I completely forgot where I am”). There was a considerable reduction in the total ESAS score post-treatment (T0 ESASTot = 27.2; T1 ESASTot = 18.8) and a slightly reduction in distress (T0 DTTot = 4.4; T1 DTTot = 3.8). However, two patients were more tired after the intervention.
Significance of Results: Our preliminary results demonstrate that VR therapy is acceptable, feasible and safe for use within a palliative care population and appears to be a viable treatment option. Clinical trials are both warranted and necessary to confirm any therapeutic effects of VR therapy, as is the need to tailor VR systems better for use in palliative care settings.
Introduction
Palliative care patients often experience a variety of physical symptoms and significant psychological distress, including depression, anxiety, feelings of isolation, and an overall poor quality of life (QoL).1,2 Pain is a common symptom in patients with life-limiting illness and can be intensified by emotional and psychological factors like distress, worries, depression, and anxiety.3,4 The management of pain is primarily pharmacological. However, although analgesics like morphine and oxycodone can significantly reduce pain levels, they come with various adverse effects that negatively impact patients’ QoL. 5 Furthermore, during the SARS-CoV-2 pandemic, preventative measures that have been enforced to minimize the further spread of infection — like patient isolation, staff wearing personal protective equipment that hides their faces and covers their hands, and visiting restrictions that significantly curtail interactions with family and friends — have increased distress in dying patients and their families, rendering it more difficult for family and caregivers to communicate and provide comfort to their loved ones in their final days. 6 The COVID-19 pandemic has thus highlighted the need for alternative ways to provide palliative care and support patients and their families during the end-of-life phase. 6 Meanwhile, virtual reality (VR) has opened up a variety of therapeutic options with the potential to improve symptom burdens in patients with advanced diseases.7-9 Importantly, unlike pharmacological approaches to pain and symptom management, VR is free of many of the side effects.
VR refers to the use of computer technology to simulate a three-dimensional, artificial computer-generated environment with 360-degree images and videos, thereby enabling individuals to interact in as real a way as possible using special electronic equipment, including a headset with goggles, headphones, and speakers supporting spatial audio, and a controller. 10 The power of VR derives from multisensory immersion, using concurrent auditory, visual, and tactile cues which, when combined, enhance the feeling of presence. 11 VR has been established as a useful tool in different clinical disciplines, including simulation training, rehabilitation, and pain prevention and treatment.12-15 A number of clinical trials have generated promising results using VR as a therapeutic option to improve symptom burden in different patient populations and clinical settings (eg, children, patients with fibromyalgia or phantom limb pain, patients with heart failure, cancer patients, and elderly people with dementia).16-21 Brief VR sessions of 3 to 30 minutes have also been found to be effective at lowering self-reported pain levels during various unpleasant medical procedures — like venipuncture, wound debridement, acute burn care and physiotherapy, and periodontitis procedures — as well as during labor contractions.22-26
Recently, studies have begun to explore whether a VR experience can help to reduce emotional pain, distress, anxiety, or depression. Some published studies already support the concept of using VR therapy to effectively improve emotional well-being and cognition and diminish levels of anxiety, depression, and fatigue in hospitalized cancer patients.14,15,27-31
Palliative care is an important component of comprehensive care for patients with life-threatening disease, aimed at preventing and relieving suffering and improving QoL among patients and their families through the early identification and relieving of pain and other physical, psychosocial, and spiritual problems. 32 It is possible that VR technology might also have beneficial therapeutic qualities to improve end-of-life care in terminally-ill patients. To date, only a few studies have evaluated the use of VR therapy in the context of palliative care and its effectiveness alleviating symptom burden in this patient population.33-36 The aims of the current case series were (1) to evaluate the feasibility and acceptability of VR therapy, (2) to collect first data in regard to patients’ experiences with VR therapy, and (3) to assess its effectiveness reducing symptom burden in a small cohort of palliative care patients.
Methods
Setting
The University Hospital Zurich, Switzerland is a 900-bed tertiary-care center. The Competence Center Palliative Care is associated with the Department for Radiation-Oncology and consists of two wards with a total of 16 beds. In 2020, the Competence Center Palliative Care served about 400 patients with advanced, incurable diseases of different etiologies. Medical Information was retrieved from the electronic medical records. The proposal for this case series was sent to the ethics committee Zurich for ethics approval. However, due to the nature of this study, no formal authorization from the ethics committee was required for this case series (BASEC-Nr. Req-2021-00850). All patients provided written informed consent prior to study participation. This case series was performed according to the local legislation and institutional requirements. The VR intervention is described according to the “Template for Intervention Description and Replication” (TIDieR) checklist 37 (see supplement material file 1).
Procedure
This case series aimed at evaluating feasibility and acceptability of VR therapy in palliative care patients. The VR therapy was offered in one session to every study participant. The VR therapy was delivered by a VR-trained psychologist and was conducted at bedside in the palliative care unit. Patients’ experiences with the VR therapy sessions were assessed using a brief self-developed survey of semi-structured questions in conformity with Johnson et al., 38 which was conducted after the intervention. In addition, study participants were assessed immediately before and after the VR therapy session allowing to evaluate for pre- and post interventional effects applying the ESAS and DT. The duration of the VR therapy sessions depended on the content chosen by the patient (range 20-60 min).
Participants
Study participants were recruited from our inpatient palliative care service. Eligible patients were adults diagnosed with advanced, life-limiting diseases. Besides the patients’ disease specific therapy (eg, irradiation, chemo- and/or immunotherapy), all patients had access to a specialized multidisciplinary team, consisting of nurses, physicians, physiotherapy, occupational therapy, psycho-oncology, spiritual care, social service, and nutritional therapy, depending on their needs. In order to minimize risk of harm, patients suffering from recurrent nausea, vomiting, dizziness, seizures, epilepsy, motion sickness or decisional incapacity were excluded from this case series. Patients were approached if they met study-specific eligibility criteria as per screening research coordinator. Patients chose the content of their VR experience and decided whether or not they wanted to use the controller. Patients could stop VR therapy at any time.
Immersive VR System
The VR system consisted of an Oculus Quest 2 (oculus Quest 2). It features a Qualcomm Snapdragon XR2 CPU, 6 GB of RAM, including integrated speakers and a microphone. The Oculus Quest 2 has a resolution of 1832 × 1920 pixels per eye with a 72 Hz refresh rate and an approximate 2.5 hours of battery life. The VR software used were NatureTreksVR, Youtube VR, Occulus TV, and Tripp VR. Collectively, these applications offer a variety of VR videos such as landscape scenes and immersive environments that aim to support meditation and promote mindfulness. This VR system was chosen due to its excellent price-performance ratio, the VR system is lightweight (500 grams), portable and easy to set up at bedside. For the purpose of this case series, the default headstrap was replaced with the Elite Headstrap, which enhances ergonomics and comfort during playtime and the face interface was switched with a silicone cover that facilitates disinfection after patient's use.
Primary Outcomes
Feasibility and acceptability
The primary outcome included feasibility and acceptability of the VR therapy intervention. Feasibility was evaluated in terms of recruitment and retention rates as well as technical and logistical issues, including comprehensibility of instructions given, study procedure, and correct operation of equipment. The intervention was deemed to be feasible if more than 25% of the patients inquired were interested to use VR therapy and if the proposed intervention and study procedures could be performed appropriately and without any side effects (eg, pain, suffering, distress or lasting harm). Acceptability was assessed in terms of willingness to participate, engagement and compliance, perceptions regarding barriers and facilitators, the degree of satisfaction and the intervention perceived relevance.
Secondary Outcomes
Secondary outcomes were to assess the impact of the VR therapy on perceived symptom burden (Edmonton Symptom Assessment System) and perceived distress (NCCN Distress Thermometer).
Edmonton Symptom Assessment System
The Edmonton Symptom Assessment System (ESAS) 39 is a simple tool to assess cancer-specific symptoms in palliative care patients. The ESAS includes nine items like pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, wellbeing, and shortness of breath. The symptom severity is rated on a numerical scale ranging from 0 (no symptoms) to 10 (worst symptoms). A total score of 60 can be reached with a higher score indicating higher physical symptom burden. 40
NCCN Distress Thermometer
The National Comprehensive Cancer Network (NCCN) Distress Thermometer (DT) 41 is a 11-point Likert scale visualized as a graphic of a thermometer that ranges from 0 (no distress) to 10 (extreme distress), with which patients indicate their level of distress over the course of the week prior to assessment. A cut-off point of three is considered as most efficient to identify distress. 42
Data Analysis
Descriptive statistics (means, standard deviations, mean differences) were used to summarize demographic characteristics and participants’ assessment and to report on ESAS and DT scores before and following VR therapy. Due to the nature of a case-series which was performed on the grounds of a small sample size, no further statistical analyses were carried out.
Results
Patient demographic and medical characteristics are summarized in Table 1. The prevalent underlying diagnosis was cancer. Patients were hospitalized for palliative irradiation, chemo- and/or immune-therapy and hospitalized between 16 and 36 days. ECOG performance status ranged between 1 and 4. Further patient information is provided as supplemental material (file 2).
Demographic and Clinical Characteristics.
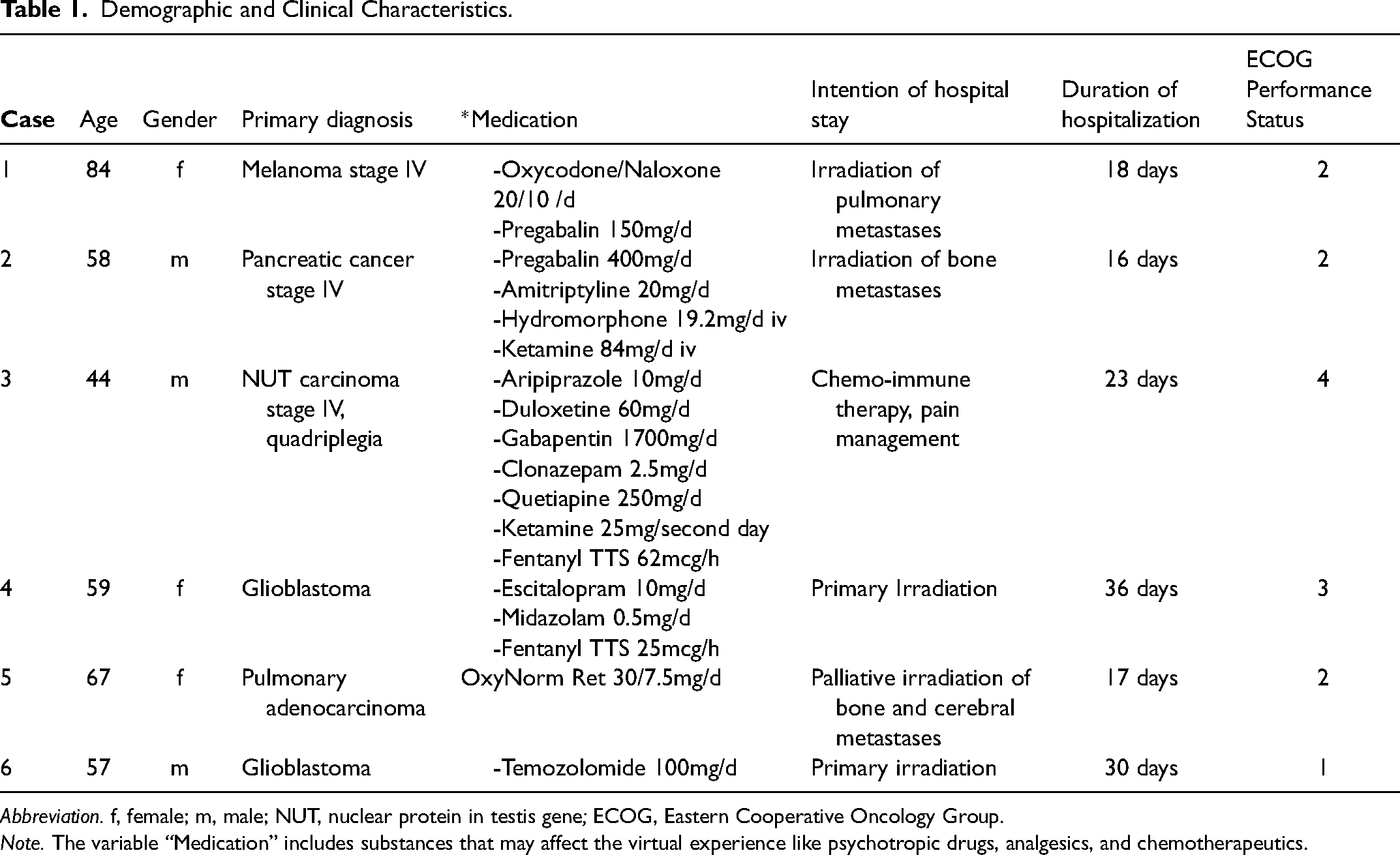
Abbreviation. f, female; m, male; NUT, nuclear protein in testis gene; ECOG, Eastern Cooperative Oncology Group.
Note. The variable “Medication” includes substances that may affect the virtual experience like psychotropic drugs, analgesics, and chemotherapeutics.
Feasibility
Between March and May 2021, study participation was proposed to 29 patients who met the inclusion criteria. Out of this cohort, eight (27%) were willing to participate in this case-series. Main arguments for study disengagement were
Acceptability
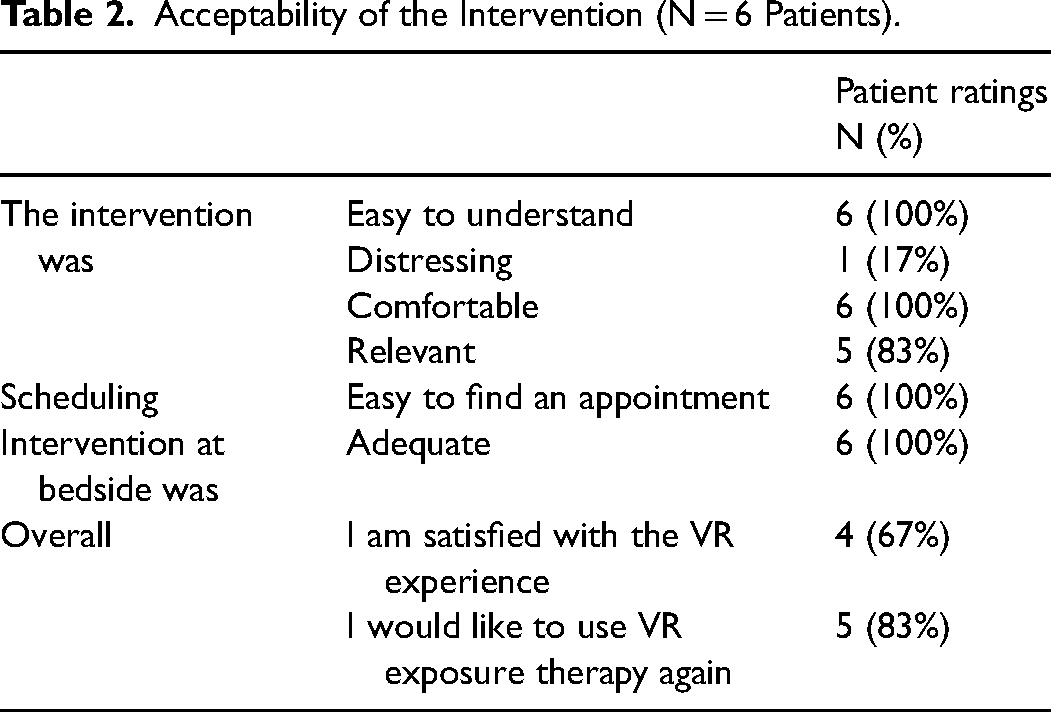
The acceptability questionnaire was completed by all study participants (N = 6). Patients’ ratings with regard to the VR experience are presented in Table 2. The VR intervention was deemed relevant (83%), easy to understand (100%), and only slightly distressing (17%). Most patients found the VR therapy helpful. Almost all patients (67%) were satisfied and would recommend VR therapy to other patients.
Acceptability of the Intervention (N = 6 Patients).
Qualitative Findings
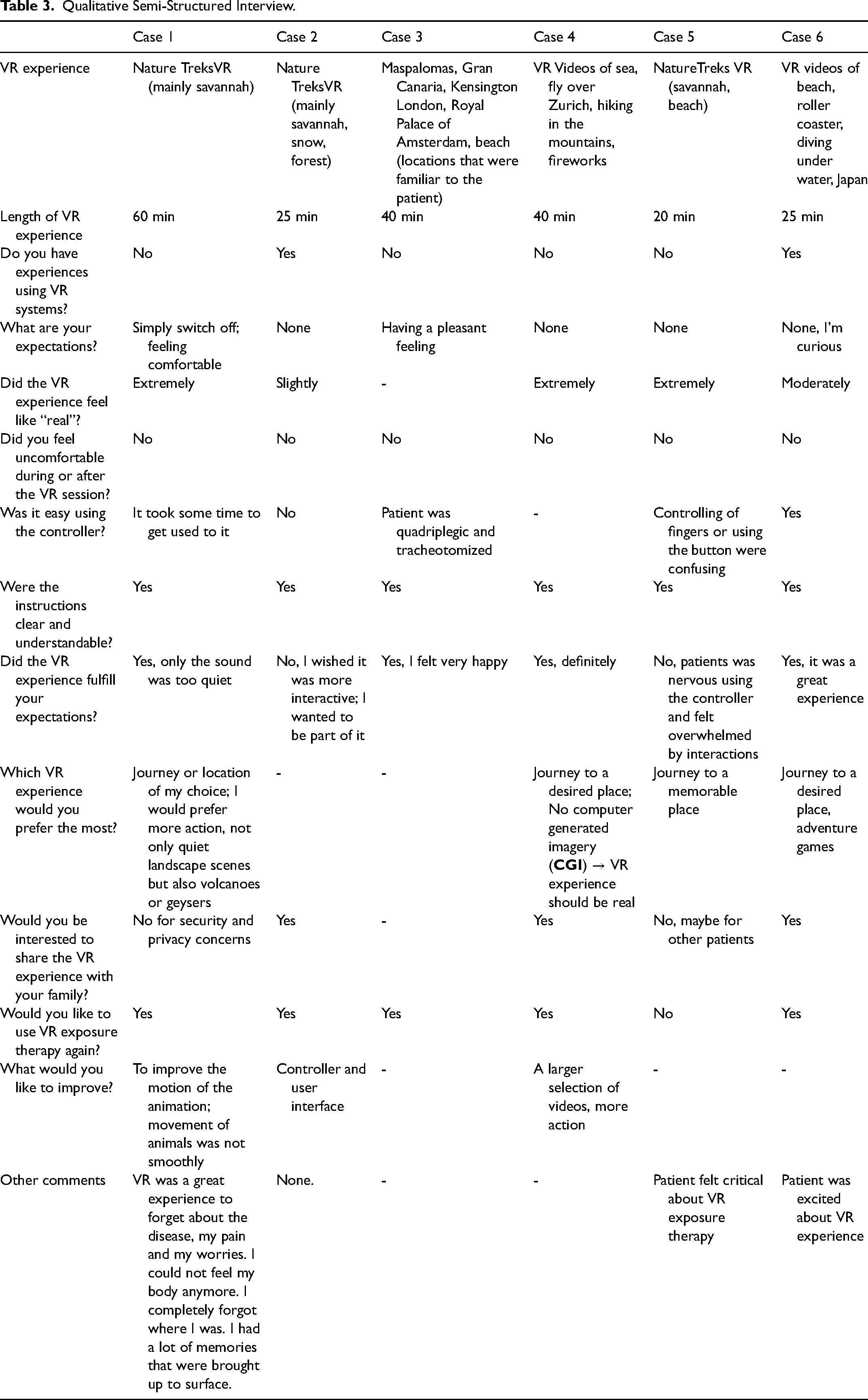
The results of the qualitative survey assessing patients’ experiences with the VR therapy sessions are summarized in Table 3. Four out of six patients reported no prior experience using VR technology. On average, study participants wore the VR headset for 35 minutes (SD = 14.8 minutes, range = 20-60 minutes). Three patients went to memorable places, while three travelled through nature settings like savannah, snow-covered field, or forest during their VR experience. Qualitative analysis revealed both positive and negative perceptions of the VR intervention. Four participants rated the VR therapy as a great experience (“it distracted me from any pain and worries”; “I completely forgot where I was”; “the VR experiences brought up a lot of good memories”). Three said they welcomed the opportunity to share the VR experience with their family, while two were critical due to security and privacy concerns. Overall, most said they would like to have VR therapy again, supporting the potential for VR therapy in palliative care settings. Suggestions for improvement given by the study participants related to the controller and user interface, the motion of the animation, sound quality, and having a larger selection of videos for them to choose from, as well as more actions and interaction options while using the VR system.
Qualitative Semi-Structured Interview.
Secondary Outcomes
The secondary objective was to evaluate potential changes in patients’ perceived symptom burden and distress. Considerable improvement following VR therapy was observed for overall well-being, nausea, anxiety, depression, pain, lack of appetite, drowsiness, and shortness of breath. Two patients said they felt more tired following the intervention. The ESAS total score decreased by a mean of 8.4 points and the DT by 0.6 points following the VR therapy session (Table 4).
Comparison of Change in ESAS Score and Distress Thermometer pre- and Post-Intervention.
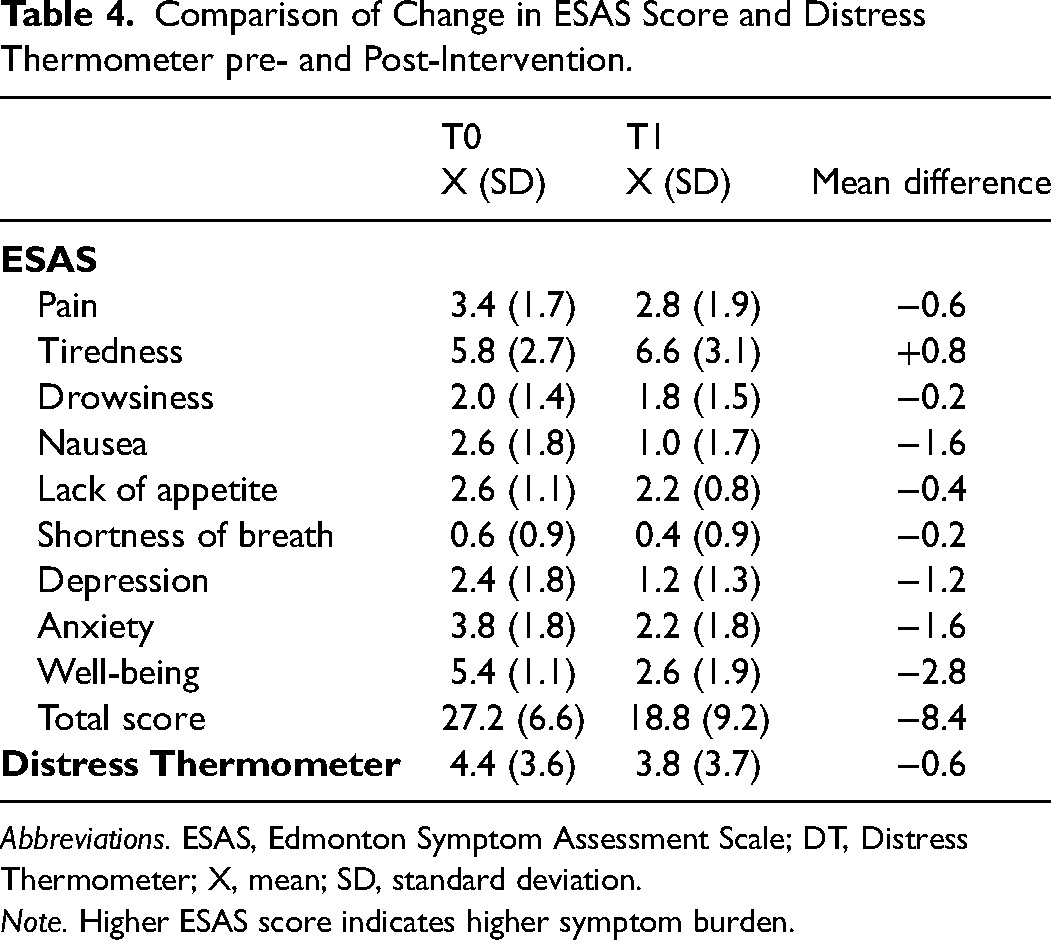
Abbreviations. ESAS, Edmonton Symptom Assessment Scale; DT, Distress Thermometer; X, mean; SD, standard deviation.
Note. Higher ESAS score indicates higher symptom burden.
Discussion
Feasibility and Acceptability
This case series largely assessed the feasibility and acceptability of VR therapy, as well as its perceived effectiveness reducing symptom burden in a small cohort of palliative care patients. The results of this case series support the feasibility and acceptability of the VR therapy. Most of the patients found it easy to use and reported no adverse effects from the intervention.
In our case series, no patient reported any side effects, like nausea, headache, dizziness, or any other physical discomfort during or following VR therapy. These observations are consistent with other reports, documenting only negligible side effects related to VR use in palliative care patients.33-35,43,44 Of note, today the risk of cybersickness might be even easier to avoid, due to next-generation devices. Contrary to expectations, not only younger patients were found to enjoy VR therapy sessions, but also elderly patients despite no prior experience with gaming or VR.
Interestingly, two patients asked for more action and one patient preferred more interactive experiences during their VR therapy session. It is possible that patients with high sensation seeking traits would enjoy more high-tension VR content (eg, volcanic eruption, avalanche on a mountain, snowstorm, etc), which is independent of their severe disease and palliative status. There also may be gender differences in preferences for VR content. 45 Such observations suggest that VR content should include both low- and high-tension material (eg, quiet landscapes and nature settings, as well as adventures and action scenes).
A recent study investigating the impact of interactive versus non-interactive VR content in home palliative care patients did not find any significant difference in terms of symptom reduction (eg, depression, pain, ESAS). 46 However, the sample size included in this study (N = 14) was too small to produce any conclusive results and thus, further studies are needed to become more aware of patients’ preferences and sex differences with respect to VR content in the palliative care context.
Secondary Outcomes
An overall reduction in symptom burden in palliative care patients following VR therapy was observed. What improved most following VR therapy were well-being, anxiety, and nausea. Our results confirm previous findings, underlying the potential of VR therapy as an effective distraction technique, resulting in significant reductions in anxiety, depression, pain, and vomiting in patients with advanced disease.7,28,35,36,38
While the mechanisms by which VR promotes well-being and improves symptom burden are complex and have yet to be clarified, underlying mechanism may be through altered attentional focus during parallel cognitive processing. 47 Similarly, attention-related modulation during cognitive processing has been proposed as an explanation for how VR attenuates pain. 48 According to neurocognitive theories, humans have limited attentional resources available, and pain and other unpleasant feelings require some level of attentiveness. 49 VR could activate positive (happy) memories, thereby distracting from or suppressing negative feelings and reducing an individual's attentiveness to noxious stimuli. 50 Thus, it is plausible that retrieving positive memories of memorable places through VR therapy could significantly increase someone's sense of well-being while reducing their psychological symptoms. In line whit this hypothesis, Moscato et al suggest that interactive VR contents might be more effective in relieving cancer-related symptoms due to a higher demand of attentional capacity and thus, resulting in an increased distraction effect as opposed to non-interactive VR contents that require only passive observation. 46
Future Perspectives
VR has generated technology-driven psychological interventions with the potential to reduce distress and promote meaning at the end of a person's life. This technology can provide psychological care and comfort for patients who are immune-compromised and/or isolated, enabling patients and their families to interact,8,51 It also allows patients to fulfill some of their dying wishes and experience life scenarios on their bucket list, like going on a safari, swimming with dolphins, or visiting a tropical island.28,35 Common symptoms experienced by palliative care patients include pain, appetite loss, fatigue, and sleep disturbances, all of which can be aggravated by distress. Vice versa, distress can cause sleep disturbances, abdominal pain, anxieties and depressed mood. 52 By experiencing a comfortable, relaxing virtual space via VR technology, patients at the end of life may see their level of distress reduced. 53 Similar to meditation and mindfulness relaxation techniques, VR might even have the potential to benefit patients’ endocrine and immune systems, resulting in reduced inflammation and improved immune function.53-56 This said, further studies are needed to better understand the immune changes that occur following VR use.
The current COVID-19 pandemic has emphasized the need for alternative ways to provide care for palliative care patients during their remaining time. VR technologies with high-resolution audio and video functions have the ability to both facilitate remote communication with families, friends, and care givers, and allow for virtually-unlimited VR experiences, both of which have the potential to improve QoL in palliative care patients.33-35,43,44,57
In conclusion, VR technology appears to be feasible, safe, and acceptable in the context of palliative care and might be both effective as a means of enhancing palliative care patient QoL, and highly cost-effective doing so. It also requires little training for healthcare providers. Nonetheless, its short- and long-term effects are largely unknown and it still needs to be determined whether the beneficial effects of VR therapy are sustainable over time or merely a temporary distraction. It also is feasible that multiple VR sessions could have greater therapeutic benefit than a single session, since some time is necessary for users to familiarize themselves with the navigational equipment and operate VR content independently. Because the application of VR in palliative care patients is still novel and little guidance for its safe use in clinical practice exists, further studies are warranted to better understand its efficacy and safety profile in terms of long-term effects and possible adverse reactions.
Strengths and Limitations
Small case series have several limitations, greatest among them the various restrictions that result from the small sample size, like the inability to conduct meaningful statistical analysis and risks generalizing results to other, larger populations. Secondly, because only patients who were interested in trying VR therapy participated in our case series, it is possible that their opinions were already biased in favor of such technology. Third, no comparison group was incorporated into our study design. Lastly, the authors acknowledge a potential risk for confirmation bias. The following precautions were undertaken to reduce the risk of bias: the interviewer's interaction with patients was standardized using a pre-defined set of questions; objective measures were used (eg, ESAS; DT) to evaluate the impressions of study participants; and statistical analyses were performed by a person (A.S.) who was not involved in the study procedures. These limitations notwithstanding highlight that our patients generally appraised their VR experience favorably and none reported adverse effects, suggesting that using VR therapy in palliative care patients is feasible, safe and of potential therapeutic benefit. Our intention is now to study the effects of VR in palliative care patients on a larger scale in a comparative study to identify any potential VR therapy might have as a guided therapeutic approach to help patients and their families optimize the remaining time they have left.
Conclusion
In this case series using VR technology in six palliative care patients, VR therapy was feasible and acceptable. We observed results that should both encourage and inform future investigators seeking to evaluate the effectiveness of VR therapy in palliative care patients. Our preliminary results suggest that VR is a treatment option that appears to be suitable to palliative care patients, as well as safe and potentially of benefit. Clinical trials are both warranted and necessary to confirm any therapeutic effects of VR therapy, as is the need to tailor VR systems better for use in palliative care settings.
Supplemental Material
sj-docx-1-pal-10.1177_08258597221086767 - Supplemental material for Virtual Reality Therapy in Palliative Care: A Case Series
Supplemental material, sj-docx-1-pal-10.1177_08258597221086767 for Virtual Reality Therapy in Palliative Care: A Case Series by A. Seiler, M. Schettle, M. Amann, Sophie Gaertner, Stefan Wicki, S.M. Christ, G. Theile, M. Feuz, C. Hertler, and D. Blum in Journal of Palliative Care
Supplemental Material
sj-docx-2-pal-10.1177_08258597221086767 - Supplemental material for Virtual Reality Therapy in Palliative Care: A Case Series
Supplemental material, sj-docx-2-pal-10.1177_08258597221086767 for Virtual Reality Therapy in Palliative Care: A Case Series by A. Seiler, M. Schettle, M. Amann, Sophie Gaertner, Stefan Wicki, S.M. Christ, G. Theile, M. Feuz, C. Hertler, and D. Blum in Journal of Palliative Care
Footnotes
Author Contributions
All authors have made a substantial, direct and intellectual contribution to the work and approved it for publication.
Competing Interests
The authors have no conflict of interest to declare.
Ethical Approval
This research project met criteria for exemption as reviewed by the ethics committee in Zurich, Switzerland (BASEC-Nr. Req-2021-00850.
Informed Consent
All patients provided written informed consent prior to study participation.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.