
Abstract
Introduction
When patients cannot make treatment decisions for themselves, healthcare providers must rely on surrogate decision makers (SDMs). Recent data suggests that as many as 40% of hospitalized adults 1 nearly 50% of older adults 2 and up to 95% of patients in intensive care units (ICUs),1,3 rely on SDMs to make medical decisions.
In a systematic review of the literature published before July 1, 2010, 4 the effect on surrogates of making treatment decisions for incapacitated adults was assessed. Wendler and Rid 4 identified 40 studies that provided data on 2854 surrogates, more than half of whom were family members of the patient. Of note, at least one third of the surrogates from the quantitative studies reported negative emotional burden as a result of SDM. Negative emotional burden was also reported among most of the qualitative studies SDMs. Surrogates reported they experienced significant negative effects for months, and even years, in some cases. The most common negative effects reported were stress, guilt over decisions made, and doubt that they had made the right decision.
There are several reasons to revisit a systematic review of the effect of surrogate decision making. Having a better understanding of the effect of surrogate decision making can inform studies whose aim it is to reduce SDM's burden. Reduction of SDM burden is important as it is known that SDM role stress reduces the decision maker's ability to make appropriate treatment decisions. 5 Additionally, as there has been more than a decade of literature published since the previous systematic review, it would be valuable to investigate whether recent studies have reported the same negative effects on SDMs.
The purpose of this current study was to perform a scoping review of literature published from 2010 to 2020 in order to assess the evidence on the effect of being a surrogate decision maker for an incapacitated adult.
Methods
A scoping review was undertaken, focused on the span of coverage of literature conducted on the effects of SDM. This approach was selected as it allowed for the review primary studies with diverse methodologies for the purpose of identifying recent reports of surrogate decision making burden and their effect. Additionally, this approach allowed for identification of gaps in the existing research literature. 6
Identifying the Research Questions
As researchers and clinicians working with family members who serve as surrogate decisions makers for people with dementia, we were interested in assessing the evidence about the impact of being a surrogate decision maker. To achieve this aim, we performed this scoping review to map the studies, to explore what is currently known about surrogate decision making, and to identify gaps in the literature base. The research questions were: (a) what is the effect of treatment decision making on surrogate decision makers (SDMs)? (b) What are the gaps in the evidence related to the effect of surrogate decision making for incapacitated adults?
Identifying Relevant Studies
Inclusion/exclusion criteria
Study inclusion criteria were: both surrogates and the incapacitated adults age 18 or older; human studies; disseminated in English; and observational studies, clinical trials, qualitative research, quantitative research and meta-analyses. Studies were excluded if they: focused on biological [surrogate] markers; systematic reviews, case reports, clinical guidelines, opinions and editorials. Additionally, in keeping with Wendler and Rid, “articles were judged to be ineligible if the reviewer was confident, on the basis of their titles, that they would not satisfy the inclusion criteria of providing quantitative or qualitative empirical data, by evaluating surrogates, about the effect on surrogates of making treatment decisions for an incapacitated adult.” 4
Data sources and search strategies
We searched CINAHL, PubMed, and PsycINFO for empirical studies that were indexed from July 1, 2010 to February 29, 2020. The search strategy yielded a total of 4,835, duplicates were removed. Forty-seven full-text articles were reviewed based on inclusion/exclusion criteria to identify the final set (10) of articles (see Figure 1).
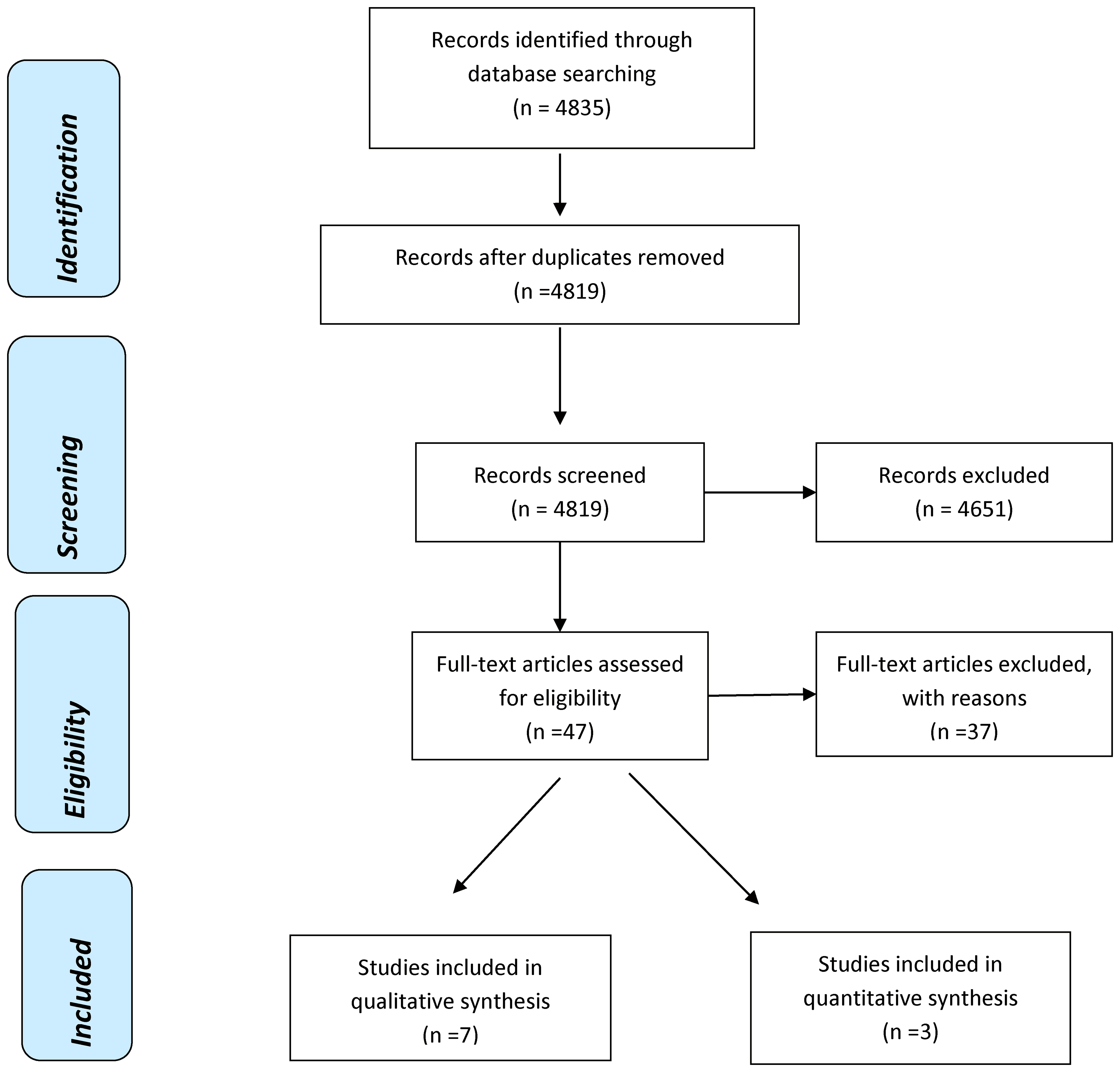
PRISMA flow diagram of effect on surrogates of making treatment decisions for others.
Study Selection
Title and abstract screening
Initially the first author reviewed the articles’ title, excluding articles if exclusion criteria were identified. This initial screening yielded 168 articles with a specific focus on the effect on surrogates of making treatment decisions for an incapacitated adult. Titles that were deemed ineligible or duplicate among the three databases were eliminated.
Full text screening
The first author read the abstracts of 168 potentially eligible articles, or the first page of articles with no abstracts, applying the same inclusion criteria. Of those, 47 articles were then deemed potentially eligible for inclusion. Both authors then read the full text of the 47 articles. After discussion of which ones satisfied the inclusion criteria, both authors then agreed that 10 articles were left for inclusion in the manuscript.
Charting the Data
Data extraction
The first author extracted data on the study location, number and type of surrogates, response rate, timing of data collection, type of treatment decisions, patient setting, methods, and main findings.
Collating and Summarizing the Results
Results
Study Demographics
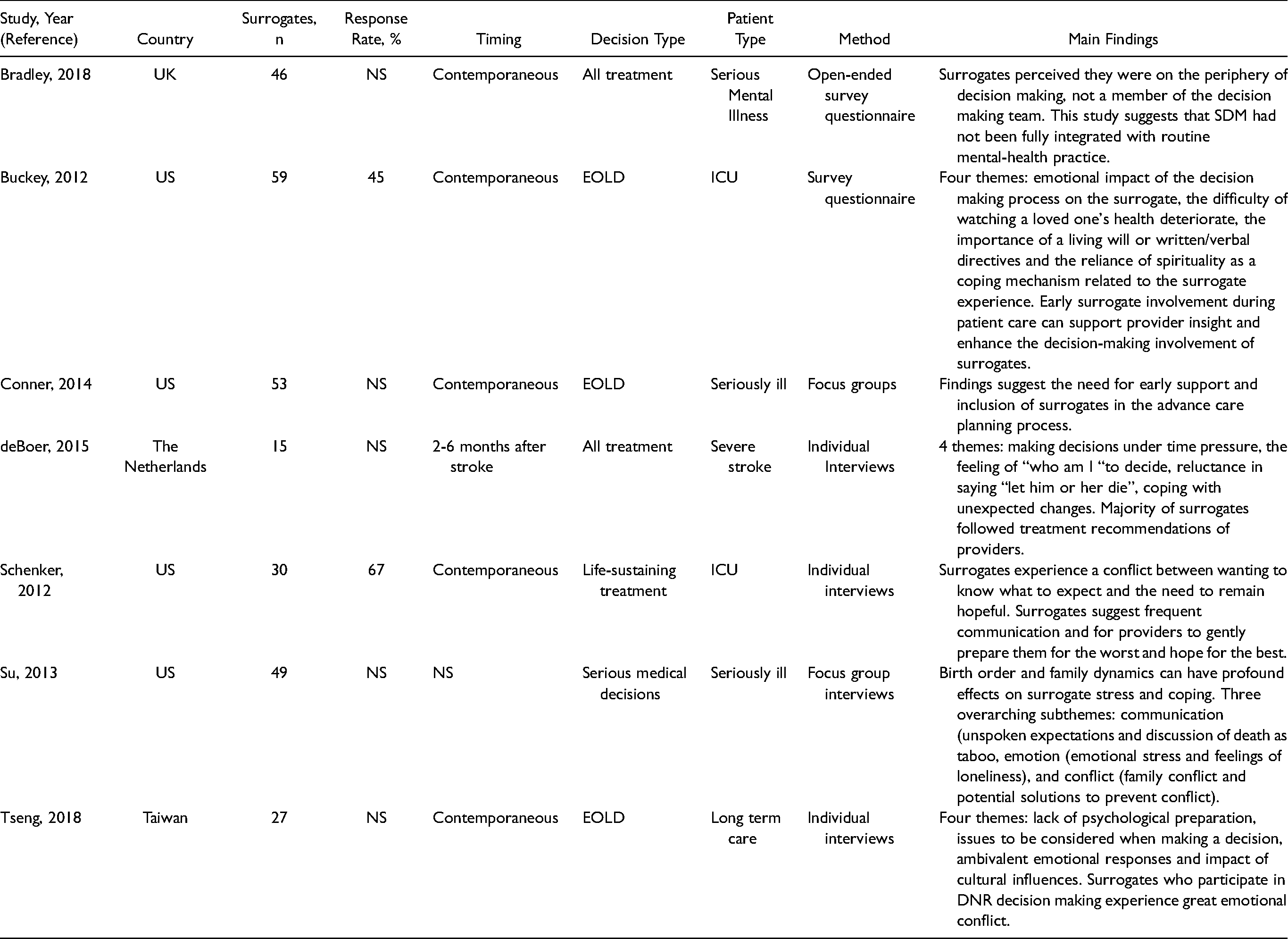
The 10 articles in the review were published between July 2010 and February 2020. One study was conducted in each of the following countries: UK, The Netherlands, Taiwan, and Australia. Six studies were conducted in the U.S. Three studies were quantitative and seven used qualitative methods. Decisions studied included: any treatment (n = 4); end-of-life (n = 4); life-sustaining treatment (n = 1); and serious medical decisions (n = 1).
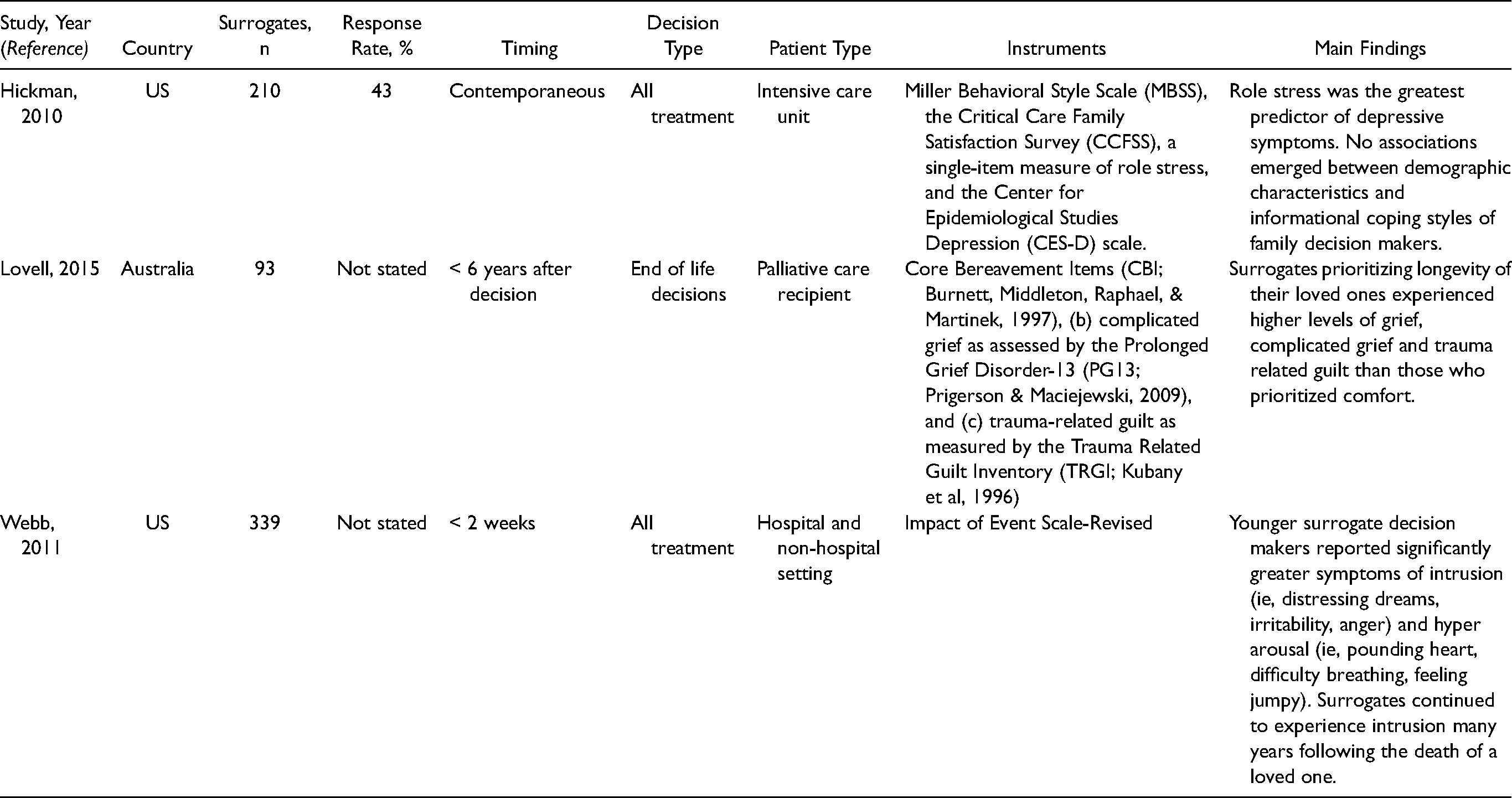
The number of participating surrogates ranged from 15, a qualitative study conducted in The Netherlands, to 339, a quantitative study conducted in the US. The total number of SDMs for all 10 studies were 921 participants (Tables 1 and 2). Of those, 90% of SDMS were patient family members. The interval for making treatment decisions and participation in their respective studies ranged from one day to six years.
Qualitative Studies of the Effect on Surrogates on Making Treatment Decisions for Incapacitated Adults.
Quantitative Studies of the Effect on Surrogates on Making Treatment Decisions for Incapacitated Adults.
Effect of Treatment Decision Making on Surrogates
Nine of the 10 articles reported that surrogates experienced the effects of stress, anxiety, conflict, or other emotional burden related to decision making for an incapacitated adult.7–12 Of the seven qualitative articles, six gave examples of specific stressors or distress associated with decision making (ie, family conflict, congruent decision making, lack of medical insight).7–12 All three of the quantitative studies reported role stress associated with SDM.,5,13,14
Similar to Wendler and Rid, 4 reports of surrogate emotional burden were consistent across study locations and methodologies, interval between treatment decisions and data collection, relationship to patient and types of treatment decisions. Buckey and Molina 8 described one surrogate's account of their SDM's experience as having painful and intense emotions, leaving them feeling “emotionally destroyed” (p. 267). Many surrogates described conflicting emotions as a result of wanting to know what to expect related to treatment or prognosis and their desire to remain hopeful. 13
The level of effect did vary based on several factors. Lovell, Smith, and Kannis-Dymand 13 found that surrogates prioritizing longevity when making end-of-life decisions, versus comfort, later experienced significantly higher levels of grief, complicated grief and trauma. Hickman, Daly, Douglas, and Clochesy 5 found that informational coping styles may influence depressive symptoms in SDMs. SDMs with information seeking coping styles had higher appraisal scores of depressive symptoms when compared to SDMs information avoidance coping style. 5 Age was also found to influence SDM burden. Webb and Guarino 14 reported that young SDMs experience significant distress related to hyperarousal and intrusion as measured by the Impact of Event Scale-Revised. 15 This heightened level of distress may be attributable to the loss of a support system, such as a parent. 14
Duration and Sources of Effect on Surrogates
The longer the progression and deterioration of the loved one's health, the more painful the decision making experience for the SDM. 8 The process of watching a loved one's health deteriorate over time, lose their quality of life or become severely disabled was described by many SDMs as stressful and very sad. 8 Buckey and Molina 8 found that “undergoing extensive tests or prolonged treatments with their loved ones increased surrogate stress and anxiety” (p. 267), to the extent the SDM's reports of emotional distress paralleled the descriptions of their loves one's physical decline.
Webb and Guarino 14 found that SDMs reported greater distress many years post death of a loved one when compared to non-SDMs. For non-SDMs, time was found to reduce distress from intrusion, ie, thoughts at unwanted times, dreams or a sense of preoccupation with the death. 14 Levels of distress for many SDMs were still considered mild to moderate, even after the lapse of many years. 14 Webb and Guarino 14 reported “time did not ease these difficulties for those who had served in the decision-maker role; yet, for those who had not served as decision makers, intrusion scores decreased over time” (p. 383).
Several of the studies described SDM stress or emotional difficulties as a result of attempting to honor expressed or perceived wishes, of not only the patient, but family members as well. The difficulty to honor the wishes of the loved one and/or family member was compounded when there was no advance directive, rather, a reliance on the SDM to simply “know” these EOL care and treatment preferences. 16 The Connor and Chase 16 study of African Americans’ SDMs described their strongly expressed desire to honor promises while at the same time describing deep raw and intense emotions associated with it. Tseng 12 reported when patients had not expressed their treatment preferences or there is not consensus among family members, the SDM was likely to feel they were bearing all of the responsibility and associated stress. Deviation from the patient's prior expressed medical preferences was also described as a source of conflict and stress among family members. 11
Mitigation of Effects on Surrogates
Several studies cited increased or improved communication as a means to mitigate the negative effects on SDMs.5,7–10,12,16 Many SDMs are reluctant to assert their power as decision maker, struggling with “who am I to decide”. 9 de Boer 9 asserted that with better provider-SDM communication, the SDM's confidence in their abilities would increase, helping to alleviate their distress related to decision making. Schenker 10 suggested that providers be attuned to the preferred communication styles and emotional needs of the SDMs. Schenker 10 explained, “By recognizing avoidant coping behaviors as responses to a common tension, physicians’ support families who are struggling to balance informational and emotional needs” (p. 248). Similar to the assertions of Schenker, 10 Hickman et al 5 found that the assessment of the SDM's coping style is a useful approach to tailor communication practices, yielding rational and informed decisions. Bradley and Green 7 contended that effective provider-SDM communication served a dual purpose, to help inform decisions and support SDM as carers.
Discussion
Incapacitated adults must rely on SDMs for treatment decisions. It is well known that the majority of SDMs are family members or close friends. Like the prior work of Wendler and Rid, 4 our study evaluated hundreds of SDMs and found that medical decision making for an incapacitated adult creates emotional distress and burden for the majority of the SDMs.
We found that the negative effects on SDMs were linked to variety of stressors. The fear of not knowing what the patient would want or being unable to fulfill the patient's actual or perceived wishes, particularly at end-of-life, resulted in an emotionally distressing experience. 8 The emotional distress of feeling unprepared to assume the role of a SDM led to descriptions of feeling overwhelmed, unsupported and alone, 11 Watching a loved one's health deteriorate over time was described as stressful and sad. 8
Our study did identify ways in which to mitigate the effects on surrogates. Similar to the prior findings of Wendler and Rid, 4 improving communication was cited by SDMs among multiple studies from various care environments as a means to decrease their emotional burden.5,8–12,16 SDMs within this study recommended regular and honest communication from the provider about prognosis and treatment options. 10 Bradley and Green 7 asserted that provider-SDM exchange serves a dual purpose, inform decisions and support SDMs as carers.
The authors of this study have identified several limitations. Though there were three studies that provided context for the cultural perspective related to the effect of surrogate decision making, there were no studies that focused specifically on racial and ethnic influences on SDMs’ experiences. With countries that have historically low reports of ACP conversations having begun to transition to promotion of ACP implementation, 17 it is imperative to examine the effect on these surrogates. Lastly, like Wendler and Rid, 4 we felt it would have been beneficial to have data related to the evaluation of the effect of surrogates both before and after they make treatments decisions.
In summary, we found that serving as a SDM for an incapacitated adult was emotionally burdensome for the majority of the participating surrogates. Though surrogates detailed the beneficial effects of timely, frequent and inclusive communication, more research should be conducted to identify ways to reduce caregiver burden. Future research also needs to be conducted to elucidate the emotional burden of culturally diverse SDMs. It is imperative to evaluate a range of diverse SDMs to determine if the effects differ across groups.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.