
Abstract
Introduction
Cancer-related fatigue (CRF) is a persistent, subjective sense of physical, emotional, and/or cognitive tiredness or exhaustion It is associated with cancer or cancer treatment from the first diagnosis until the end of life that is not proportional to recent physical activity.1,2 CRF is usually accompanied by pain, sleep problems, emotional distress, and anemia. Common factors, such as comorbidities, side effects of treatment, sleep problems, pain, nausea–vomiting, and depressive mood, and the side effects of medication used in the management of these symptoms, physical, psychological, and pathological factors play a role in the etiology of CRF.1–5
CRF has been reported by up to 40% of patients at diagnosis, 90% of patients treated with radiation, 80% of those under chemotherapy treatment, and between 17% and 53% after treatment. 4 The rate of CRF depends on the type and stage of cancer. Fatigue was reported to be the most common symptom in the patients with gynecological cancer.6–8 Emotional and cognitive fatigue scores were reported to be increased in patients with breast and gynecological cancer. The level of fatigue in gynecological cancers was reported to be varied before and after treatment, and the psychological distress affected this situation. 6
CRF is one of the most difficult and complex symptoms to manage. Fatigue management should include personalized pharmacological (psychostimulants, corticosteroids, erythropoies-stimulating agents, antidepressants etc) 9 and nonpharmacological interventions according to the stage of the cancer. Nonpharmacological methods, such as exercise, yoga, acupressure, acupuncture, massage, mindfulness-based stress reduction intervention 10 and cognitive behavioral therapy, have more or less positive contributions and distinct advantages in the management of CRF,1,2,11,12 but they have limitations in clinical practice. Applications that require expert assistance and professional guidance, such as cognitive behavioral therapy, can be time-consuming. 13
Bright white light (BWL) therapy, which is among the circadian therapies, suppresses melatonin released from the pituitary by stimulating photoreceptors and suprachiasmatic nucleus through the retina, thereby regulating the disrupted circadian rhythm. To reduce CRF, BWL may either directly or indirectly affect inflammatory cytokine activity.1,14,15 BWL, which has been described in studies as a simple and low-risk intervention, may be a good option for CRF management.16,17
Johnson et al (2017) found in their blinded randomized controlled studies that 10,000 Lux BWL administered in the morning hours reduced fatigue by 17% in patients with cancer and that the mean fatigue scores of patients decreased from 29.43 to 9.48 compared to before the light administration. In this study, BWL was applied to patients for 30 min. a day for 4 weeks. 14 According to NCCN (2020), BWL of 10,000 lux can be applied for 30–90 min in the morning hours to regulate sleep and manage fatigue in the post treatment period as well as in cancer patients receiving active treatment. 1 However, studies on this subject consist of small sample groups, and more studies are needed to identify the risks and benefits of the application and to determine the optimal application time and duration. The present study was aimed to evaluate the effect of BWL on the fatigue levels of patients with gynecological cancer who were treated with chemotherapy. We hypothesized that BWL changes general fatigue and interference of fatigue with daily life scores in patients with gynecological cancer.
Methods
Study Design
This is a randomized controlled trial investigating the fatigue level of a 10,000 lux luminescent BWL compared to a control group without light application.
Setting and Participants
This study was carried out in gynecologic oncology clinic of Eskisehir Osmangazi University Health, Practice and Research Hospital in Eskisehir, Turkey from May 2019 to June 2020. The sample size in this study was 72 subjects: 36 in the intervention group and 36 in the control group.
Inclusion and Exclusion Criteria
Patients aged over 18 years, had a normal state of consciousness, had no communication disorders, did not work in the night shift, had a general fatigue level score of ≥1 according to the Brief Fatigue Inventory,18,19 have received at least second or more chemotherapy and could perceive light were included in the study. Patients who had natural/artificial lenses or used medication that causes photosensitivity (tetracycline, doxycycline, nalidixic acid, voriconazole, amiodarone, hydrochlorothiazide, naproxen, piroxicam, chlorpromazine), eye disease, or contact lenses and had a change in their treatment plan in the last 6 weeks were not included in the study.
Randomization
The individuals were assigned to the study or control group in equal numbers and randomly using the stratified (by severity of fatigue) randomization method. The individuals were initially stratified according to the severity of fatigue (1–3 points, mild; 4–6 points, moderate; 7–10 points, severe fatigue), 20 then patients were included in the study and control groups in a balanced way by block randomization method. For block randomization 20 blocks (permutations block 6 and block of size 3 with 1:1) was used. 21 (Figure 1).
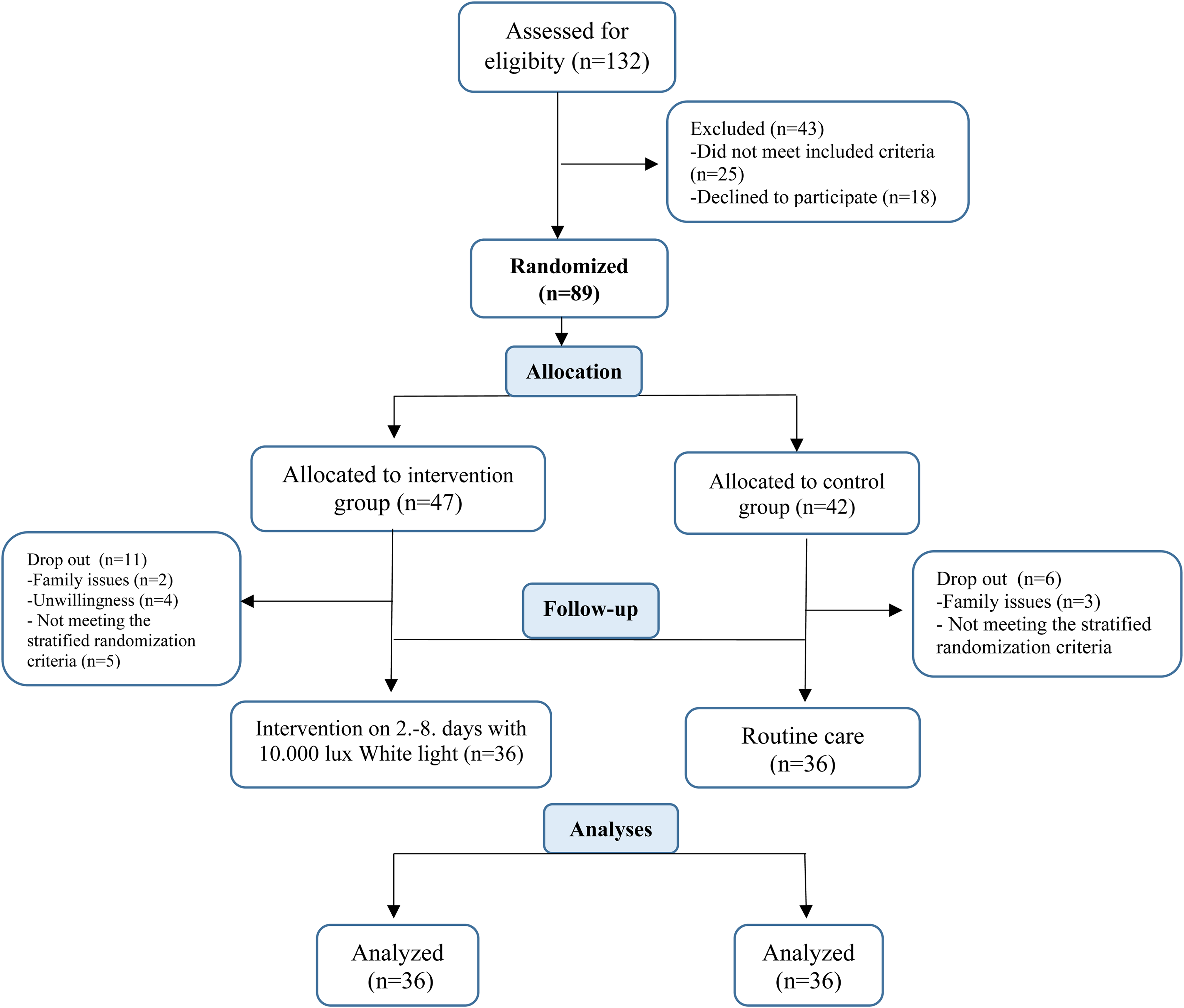
CONSORT diagram of the study.
A researcher among the authors who was not involved in patient care and implementation of interventions evaluated patients for eligibility, enumerated them, collected baseline data, and assigned them to research groups. Moreover, this researcher assigned the research groups at the beginning of the research, the intervention group “A,” whereas the control group was coded with the letters “B.” Two nurses were research assistant (RA) of the study. They had a bachelor's degree, and were independent of each other and the researchers. The first nurse (RA1) applied BWL to the intervention group. The post-intervention evaluation of the patients and the entry of the data into the statistics program were made by the other nurse (RA2) who was not informed about group assignment. Thus, the nurse (RA2) who conducted the evaluations, were blinded. During data entry and analysis, coding of the groups was continued. Thus, biostatistician, were blinded.21,22
Data Collection
Observation, interview, and measurement methods were used to collect the data. “Brief Fatigue Inventory (BFI)” and “Descriptive Information Form” were used to evaluate the fatigue level of the patients on the first, ninth, and twenty-first days. The patients’ demographic and medical characteristics were obtained from their medical records.
The Descriptive Information Form
This form was used to collect information on the sociodemographic characteristics, diseases, and treatments of the patients.
The Brief Fatigue Inventory (BFI)
This inventory was developed by Mendoza et al (1999) to evaluate the “general fatigue” level and “interference of fatigue with daily life” in patients with cancer. 18 The study evaluating its validity and reliability for the Turkish context was carried out by Çınar et al(2000) Cronbach's alpha internal consistency coefficient of the inventory was found as 0.98. 19 The BFI consists of nine items in total, with three evaluating general fatigue and six evaluating the effect of fatigue on daily life. Individuals rate all items on a scale of “0” (no fatigue) to “10” (the most severe fatigue you can experience), taking into account their status in the last 24 h. The “general fatigue” level is calculated by taking the average of the first three items of the inventory. The average of the last six items yields a score for interference of fatigue with daily life. According to the scores obtained from the BFI, the severity of fatigue of the individual was “0, no fatigue; 1–3, mild; 4–6, moderate; and 7–10, severe fatigue”. The Minimal clinically important difference for BFI was found that 7 point. 19
Baseline Period
Descriptive Information Form and the BFI were administered to the patients in both groups and their baseline assessment was made on the first day of the study at clinic. Afterwards, as a part of routine care, patients in both groups were informed about interventions for energy conservation and energy enhancement (organizing the patient's sleep–rest hours, supporting activities of daily living, organizing the living environment, adequate and balanced nutrition, etc). The patients were informed about the study procedure.
Practice Period
The first day in the study was the day of chemotherapy treatment. Between days 2 and 8 of chemotherapy in the intervention group were administered a standard BWL at 10,000 Lux intensity by an independent nurse (RA1) in their home environment using a Litebook Elite light source (The Litebook Company Ltd, Medicine Hat, AB). The distance between the light source and the patient's face was set at 50 cm, and the intensity of the light for each patient was checked using a Lux Meter. The intervention was applied between 07:00 and 10:00 in the morning for 30 min without interruption, and it was continued for seven successive days. The light application procedure was followed based on the previous studies on oncology patients.14,23 The patient was asked to engage in other activities during the light administration, such as watching television, reading books, and not to look directly at the light. The second and third evaluations of the fatigue status of both groups of patients were completed on the ninth and 21st days by an independent other nurse (RA2).
Data Analysis
The statistical analysis was performed on IBM SPSS v.24 (SPSS, Chicago, IL) software package. Shapiro-Wilk test of normality and Q-Q graphs were used to evaluate the data distribution. To compare the socio-demographic characteristics of groups, independent groups t-test and chi-square analysis were used. Multi-factor analysis of covariance from general linear models (MANCOVA) was used for repeated measurements in the comparison of BFI scores between and within the groups according to measurement times and stratas. Bonferroni test was used in post-hoc analysis for pairwaise comparisons. The intention-to-treat method was not used in the analyses. Data of patients who dropped out of the study were not included in the analysis. Statistical significance level was accepted as p <0.05.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Clinical Research Ethics Committee of Faculty of Medicine Eskisehir Osmangazi University (Date: May 24, 2018/No: 80558721-050.99-E.58639). Written and verbal informed consent was obtained from the participants of the study.
Results
The mean age of the participants in the intervention group and control group was 57.69 ± 12.48 years and 55.17 ± 13.11 years, respectively. There was no statistically significant difference in the mean age and other demographic characteristics of both the groups (p = 0.405) (Table 1). The majority of patients in both groups were in stage four (41%), and other clinical features were similar (p > 0.05) (Table 1). There were no patients who received pharmacological treatment for fatigue in either group.
Distribution of Patients by Their Demographic and Clinical Characteristics.
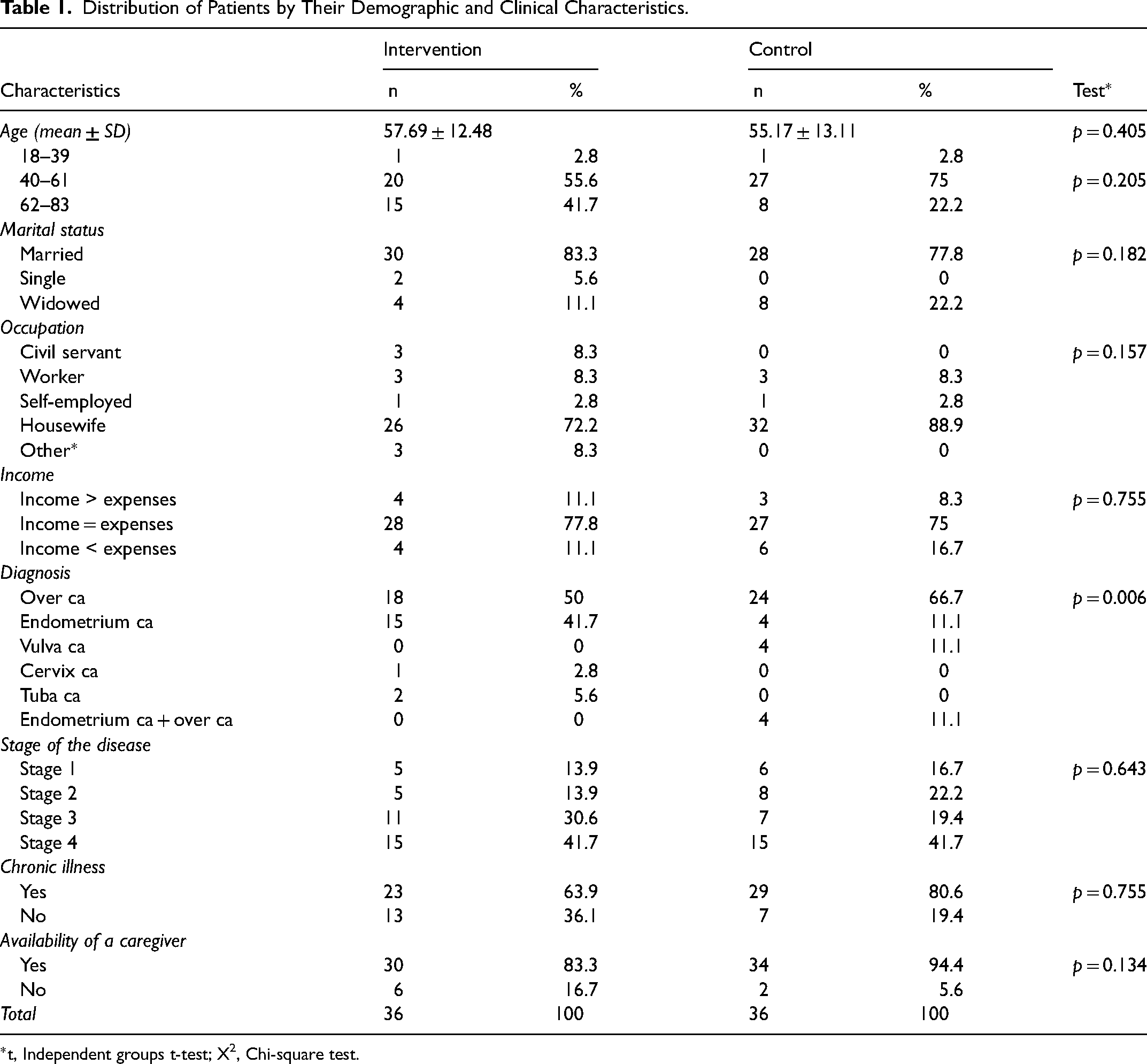
t, Independent groups t-test; X2, Chi-square test.
The mean general fatigue scores of the intervention group were found to be 4.876 ± 0.000 on the first day, 4.384 ± 0.270 on the ninth day, and 4.387 ± 0.258 on the 21st day and those of the control group were 4.876 ± 0.000, 5.033 ± 0.270, and 4.984 ± 0.258 on the first, ninth, and 21st days, respectively, according to the examination of the general fatigue scores of the groups in the study by the time of evaluation. The results of Mancova analysis models showed no difference between the groups in terms of the distribution of mean general fatigue scores (p = 0.099). Statistically significant difference was found between the first, ninth, and 21st day general fatigue score values when all the study participants were taken into account (p = 0.007). There was no difference between the groups in terms of the first, ninth, and 21st day general fatigue score values in this study (p = 0.100) (Table 2). The change in the general fatigue severity of the patients in the intervention and control groups by strata over time is shown in fig. 2.
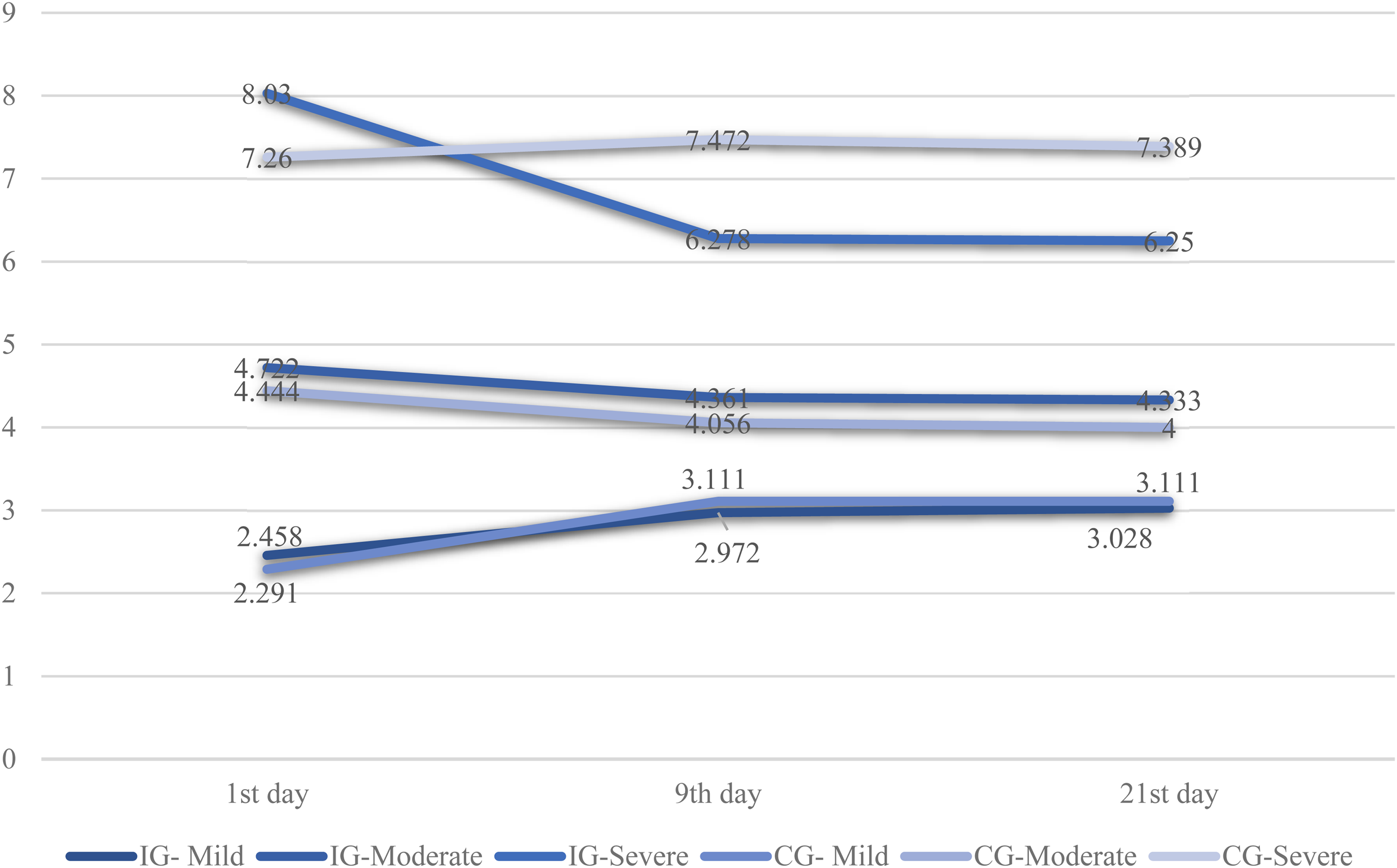
Changes in the general fatigue score of the groups over time according to the strata. IG: Intervention group; CG: Control group.
Distribution of the Patients’ General Fatigue Scores by Group and Time.
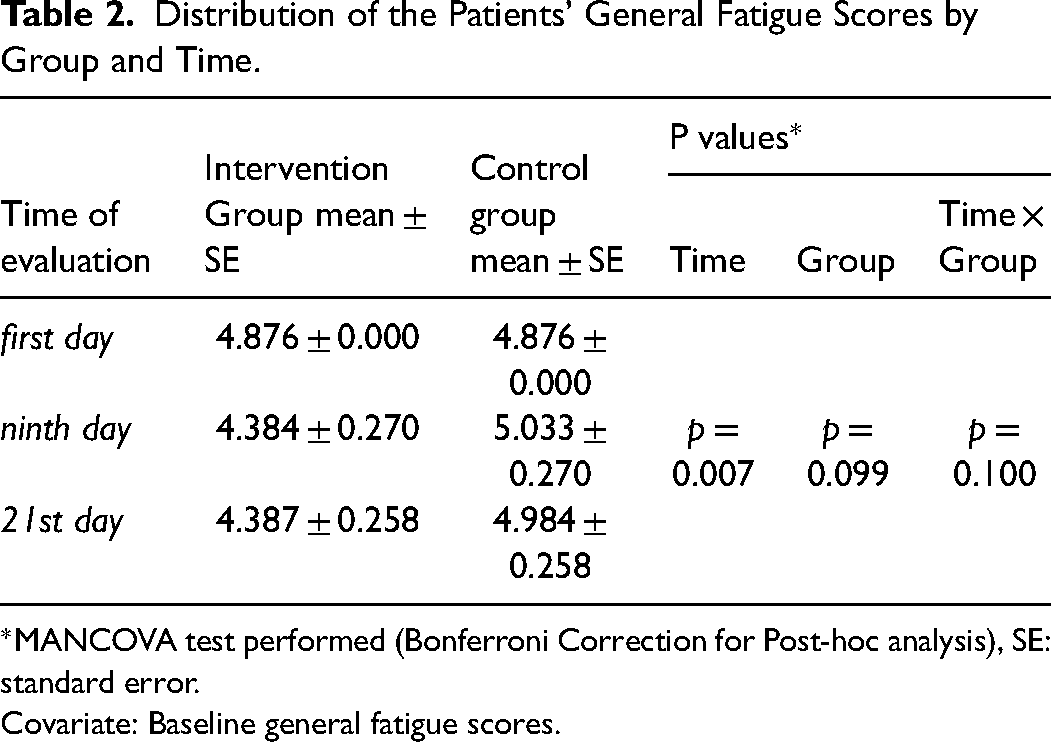
MANCOVA test performed (Bonferroni Correction for Post-hoc analysis), SE: standard error.
Covariate: Baseline general fatigue scores.
The mean interference of fatigue with daily life scores of the intervention group were found to be 4.55 ± 0.26 on the first day, 3.53 ± 0.23 on the ninth day and 3.57 ± 0.22 on the 21st day and those of the control group were 4.95 ± 0.26, 4.79 ± 0.23 and 4.82 ± 0.22 on the first, ninth, and 21st days, respectively, according to the examination of the interference of fatigue with daily life scores of the groups in the study by the time of evaluation. There was difference between the groups in terms of the distributions of mean interference of fatigue with daily life scores obtained as a result of the Mancova analysis models and comparisons (p = 0.001) (Table 3). When all the individuals participating in the study were taken into consideration, a statistically significant difference was no found between the first, ninth, and 21st day interference of fatigue with daily life scores (p = 0.246). A statistically difference was also found between the groups in the study in terms of the first, ninth, and 21st day interference of fatigue with daily life scores (p = 0.029) (Table 3).
Distribution of Patients’ the Scores of Interferences of Fatigue with Daily Life by Group and Time.
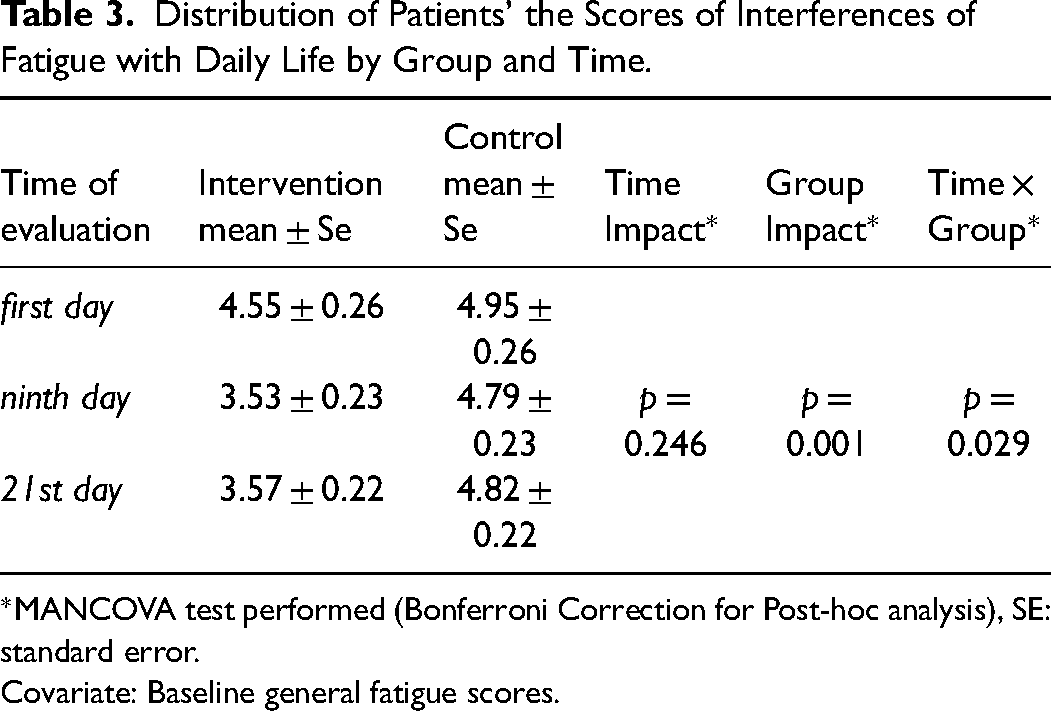
MANCOVA test performed (Bonferroni Correction for Post-hoc analysis), SE: standard error.
Covariate: Baseline general fatigue scores.
According to the Mancova test performed for pairwaise comparisons to show which group and time this change is related to was found a statistically significant decrease in the interference of fatigue with daily life score on the ninth and 21st days in the intervention group compared to the first day (p = 0.001, p = 0.002) Although there was a similar decrease in the control group, that is, the ninth and 21st day scores were lower than that of the first day; this decrease was not statistically significant (p > 0.05) (Table 4).
Pairwaise Comparisons of Patients’ Interference of Fatigue with Daily Life Scores by Group and Time.

MANCOVA test performed (Bonferroni Correction for Post-hoc analysis), SE: standard error.
Covariate: Baseline general fatigue scores.
p values <0.05 are in bold
Discussion
The initial general fatigue and interference of fatigue with daily life levels of both groups were moderately similar. Although there was no significant decrease in the general fatigue levels in the ninth and 21st day evaluations in both groups compared to the first evaluation, the level of interference of fatigue with daily life decreased significantly in the group that was administered BWL for 30 min in the mornings for 8 days. In the intervention group, the mean score of the interference of fatigue with daily life level decreased by one unit on the ninth and 21st days compared to the first evaluation. This finding supports the information that BWL administration has a positive effect on the level of interference of fatigue with daily life in patients with cancer. The general fatigue level did not show statistically significant difference between-group comparisons according to strata. However, the general fatigue level of the patients in the “severe” stratum of the intervention group decreased. It was thought that the lack of significant difference in the level of general fatigue might be because of the limitation of BWL application time to 8 days.
CRF is caused by a variety of factors, including disease burden, treatments, neuroendocrine changes, nutritional problems, pain, inflammation, circadian rhythm changes, sleep problems, and anemia.3,4,24–27 Due to its strong effect on the regulation of circadian rhythm, it is known that BWL therapy, in particular, is used in the management of sleep problems and fatigue in cancer patients. 1 In a study, considering this situation, were excluded from the research sample individuals with medical problems such as anemia, any physical or psychological problems including sleep problems and it was determined that BWL significantly reduced fatigue. 23 However, in our study, regardless of the causes of CRF, BWL was used, and it was determined that it was ineffective on the general fatigue level. This situation suggested that the reason for the general fatigue seen in our research sample could be related to factors other than circadian rhythm disorder and it was predicted that the efficacy of BWL might not be due to this situation. For this reason, before using BWL in the management of fatigue, nurses must conduct a thorough evaluation, both in the studies to be conducted and in the clinic. Although the light therapy used in the management of CRF differs in the literature13,14,16,23,28,29 its effectiveness has been determined when it is applied for various reasons (such as depression, regulation of sleep-wake cycle, inflammatory response, serum melatonin, and cortisol level). It was reported that BWL administered to patients with various types of cancer for 30 min every morning for 4 weeks showed positive results and reduced the severity of fatigue.14,23,30 According to Crabtree et al (2020), 30-min/8-week BWL administration in the mornings is an applicable and acceptable method for the fatigue management of young patients with cancer. 16 Jeste et al (2013) stated that BWL applied during four cycles improved the fatigue-related quality of life. 31 Another study reported that BWL administered for 30 min in the morning for 12 weeks was effective in improving depressive symptoms in cancer patients. 29 BWL application was considered to be more effective than other methods in a meta-analysis examining the results of a study using non-pharmacological interventions in the management of CRF. 32 Again, in some studies, BWL was applied regardless of the normal distribution of the fatigue level of the groups,13,14,23 whereas in our study, the patients were randomized into groups according to their fatigue level and 10,000 lux BWL was applied for 30 min/8 days. However, this application has not been found to be effective in CRF. This situation led us to believe that 8 days of BWL application may be insufficient for the management of CRF and that a longer period of light should be applied in future studies.
Fatigue was reported to be the most common symptom in the patients with gynecological cancer.6–8 The severity of this symptom was reported as moderate and high.33,34 Sleep problems, emotional state, comorbidity, and young age are reported to trigger the symptom.6,32 Although the pathophysiology of CRF is not clear, when it is not managed well, it can trigger physiological and psychological problems, affect activities of daily living, and decrease in quality of life.8,32 For this reason, experts of the field emphasize the regular screening of CRF in the cancer population and the use of objective measurement tools while screening.2,35 BWL application is one of the integrative methods among independent applications of nursing and is recommended in CRF management.1,32,36
The lack of evaluation of fatigue-related sleep problems, pain, anemia and the emotional state are the weakness of the study. The limitations of the study are that the sample included gynecological cancer patients and the application period was short. Eight-day BWL administration was not adequate in the management of CRF, as the study result shows. Therefore, it is recommended that BWL should be administered for 30 min in the mornings for an average of 4 weeks.
Conclusion
The BWL decreased interference of fatigue with daily life in patients. Based on the available data, it is possible that the application of BWL may have a positive effect on general fatigue when the number of samples and the application time are increased.
Footnotes
Acknowledgments
We would like to thank the participants for their contribution. We also thank Prof. Dr Ferhan Elmalı, Izmir Katip Celebi University Faculty of Medicine Department of Biostatistics who provided consultancy in the statistical evaluation of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Projects Unit of Eskişehir Osmangazi Üniversitesi, (grant number 2018-2220).
Consent to Participate
Participants who completed the consent process provided free-given, informed consent to participate in the study.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Clinical Research Ethics Committee of Faculty of Medicine Eskisehir Osmangazi University (Date: May 24, 2018/No: 80558721-050.99-E.58639). Written and verbal informed consent was obtained from the participants of the study. The study was registered with ClinicalTrials.gov (reference #NCT05009693) in August 2021.