
Abstract
Keywords
Introduction
Palliative care has undergone a significant transformation in recent years. What was once primarily bed-side care for terminally ill patients has evolved toward an interdisciplinary practice of medicine involving physicians, nurses, social workers, chaplains, and other healthcare profressions working to provide complex symptom management throughout the course of advanced illnesses.1,2
Numerous studies have highlighted the multude of benefits afforded by palliative care. For example, a randomized controlled trial by Temel et al 3 found that the integration of early palliative care among patients diagnosed with metastatic nonsmall cell lung cancer resulted in improved quality of life, lower rates of anxiety and depression, and even significantly longer survival when compared to patients receiving standard oncological care. Moreover, palliative intervention brings several other benefits such as decreased intensive care utilization and decreased healthcare-related financial burdens, as evidenced by a study by Morrison et al which found that consultations with interdisciplinary palliative care teams significantly decreased hospital costs among Medicaid beneficiaries.4,5 As a result, several guidelines now recommend the integration of palliative care earlier into the management of all patients with advanced malignancies, rather than only limiting it to patients nearing the end of life. 6
Despite the numerous advantages of palliative care and recent guidelines recommending its utilization among all patients suffering from advanced cancer, there remains significant variability in the availability of palliative therapy and an incomplete understanding of its utilization. 6 Recent research has shown that there is a low utilization of palliative care among patients with advanced urologic malignancies such as prostate, bladder, and kidney cancer, with only 13% to 20% of patients receiving these services. 7 However, for rarer malignancies such as upper tract urothelial carcinoma (UTUC), these trends in palliative care utilization remain unclear.
While UTUC is a rare malignancy, 12% to 16% of patients present with metastatic disease and approximately 42% of patients with localized disease will develop metastatic UTUC (mUTUC) within 2 years.8–10 Furthermore, mUTUC carries poor prognosis, with median survival <1 year. 8 With such a significant proportion of patients with a rapidly progressive and incurable condition, it is likely that the mUTUC population would benefit from palliative intervention. However, palliative care usage in mUTUC remains poorly understood.
An important step toward evaluating the current role of palliative care in mUTUC and identifying any disparities in its delivery is to analyze contemporary trends in its utilization. Equally important, however, is to identify factors associated with palliative intervention. In doing so, one can identify targeted interventions that may be leveraged to achieve appropriate utilization of palliative therapy among patients with mUTUC. In this study, we identify patterns of palliative care usage and identify determinants of palliative intervention using a large contemporary cohort of patients with mUTUC.
Methods and Materials
Data Source
The National Cancer Database (NCDB) was queried from 2004 to 2020 for patients with UTUC. The NCDB is a joint project between the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society that collects hospital registry data from over 1500 CoC-accredited facilities and captures approximately 70% of newly diagnosed malignancies in the United States. The NCDB was chosen as it represents the largest dataset that captures palliative care utilization. 11 This study was exempt from ethics review by our institutional review board as it only involved fully anonymized data from the NCDB.
Study Population
Patients with mUTUC were identified using International Classification of Disease-O-3 (ICD-O-3) codes 8120, 8122, and 8130 to 8131 along with topography codes C65.9 (renal pelvis) and C66.9 (ureter). Patients with a prior malignancy, non-mUTUC, missing follow-up information (this included all patients diagnosed in 2020), and missing palliative care information were excluded (Figure 1).
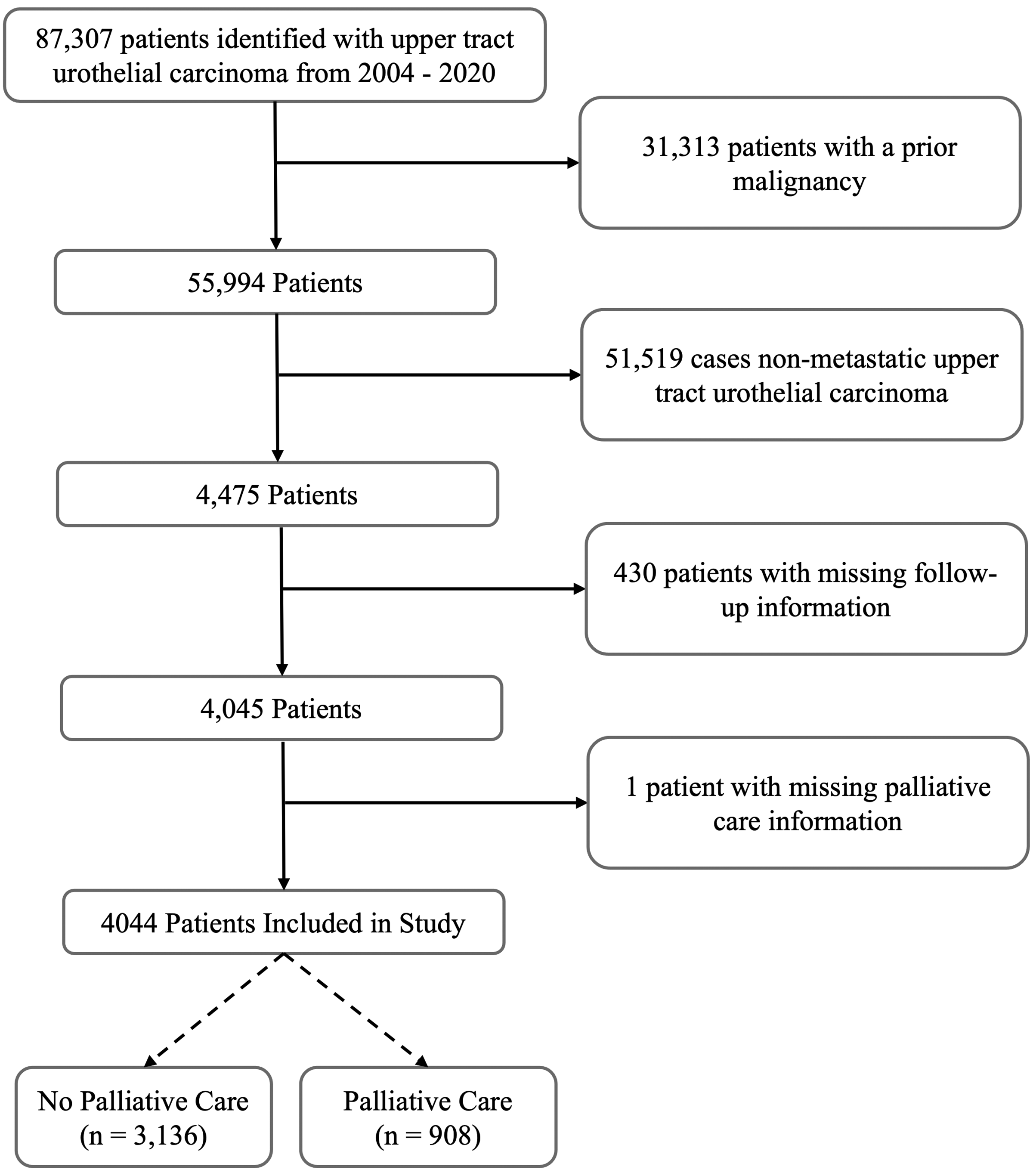
Flow diagram of exclusion criteria for patients with metastatic upper tract urothelial carcinoma (mUTUC).
Study Variables
Receipt of palliative care was the primary outcome of interest, which was treated as a dichotomous variable. The NCDB codes palliative care as 1 of 7 possible palliative interventions: no intervention, surgery alone, radiation alone, systemic therapy alone, pain management alone, a combination of therapies with pain management, a combination of therapies without pain management, or an unknown type of palliative care delivered. The NCDB defines palliative care as a treatment intended to alleviate symptoms without an attempt to treat, diagnose, or stage the primary malignancy. The NCDB does not explicitly differentiate between hospice care and other palliative therapy.
Demographic and baseline characteristics evaluated included age, year of diagnosis, sex, race, Charlson-Deyo score, rural-urban residency, distance to facility, facility type, patients with UTUC volume at facility, whether care was delivered at a minority-serving hospital (MSH), insurance status, county-based family income, and prior treatment. For facility patient volume, the total number of patients with mUTUC treated at each facility from 2004 to 2020 was calculated. Facilities were then stratified by patient volume quartile.
For MSH status, all facilities were ranked in terms of the proportion of minority patients (Black and Hispanic) with UTUC treated at that hospital. Similar to prior studies, an MSH was defined as a facility in the top decile of proportion of minority patients in the UTUC cohort. 12 Given that it is difficult to ascertain the clinical prognosis of a patient's disease from the NCDB with available variables, patients were stratified into survival cohorts to serve as a proxy for mUTUC prognosis. Patients were classified into survival cohorts of patients with an overall survival (OS) <6 months, between 6 and 12 months, and >12 months. These survival intervals were defined a priori and adhered to methodology described by prior studies on determinants of palliative care that also used survival cohorts to approximate the prognosis of patients with colorectal cancer and advanced urological malignancies.7,13
Statistical Analysis
Demographics and baseline characteristics were compared between patients with mUTUC who received palliative care and those that did not. For categorical variables, we constructed contingency tables to compare relative proportions of each variable of interest between groups and evaluated significance using Chi-square tests. For the only continuous variable in the study compared between groups, age at diagnosis, we assessed signicance using Mann-Whitney U tests as age demonstrated a non-normal distribution. Rates of palliative care usage by year of diagnosis was assessed, and a univariate logistic regression model was used to evaluate significance in this trend over time. The proportion of each type of palliative care utilized, if any, was calculated for the entire mUTUC cohort. Univariate and multivariate logistic regression models were used to identify predictors of receipt of palliative care. NCDB variables selected for univariate analysis were determined a priori and reflected factors potentially associated with palliative intervention identified in prior studies.7,11–14 Variables that demonstrated significance in the univariate analysis, defined as a P-value <0.05, were included in a multivariate analysis to determine predictors of palliative intervention. We included a broad array of demographic, facility, and treatment characteristics in the univariate analysis to ensure potential confounding variables could be further evaluated in the multivariate model. To address potential multicollinearity, variance inflation factors were calculated, but no variables included in the multivariate model exhibited high multicollinearity that would distort the model's results. SPSS Statistics Version 28 (IBM Corp., Armonk, NY, USA) was used for all analyses, with a 2-tailed alpha of 0.05 indicating significance.
Results
From 2004 to 2020, 87,307 patients with UTUC were identified. After exclusions, 4044 patients with mUTUC were included in the final analytic cohort, among which 908 received palliative care (22.5%) and 3136 did not (77.5%) (Figure 1). In the entire cohort, median age was 72 [63-79] and most patients with mUTUC were White (84.3%) and male (56.1%). When stratified by receipt of palliative care, those diagnosed in recent years were significantly more likely to undergo palliative therapy (2004-2007: 18.6%, 2008-2011: 20.0%, 2012-2015: 22.8%, 2016-2019: 24.5%), P = .012 (Table 1). Patients who underwent prior nonsurgical treatment were also more likely to receive palliative care (no prior treatment: 17.0%, systemic and/or radiation only: 29.2%, surgery ± systemic ± radiation: 16.9%), P < .001. On the other hand, older patients (<60: 26.4%, 60-70: 25.0%, 70-80: 20.1%, 80+: 20.0%, P < .001), those with prolonged survival (<6 months: 24.6%, 6-12 months: 26.3%, > 12 months: 18.8%, P < .001), and patients treated at an MSH (MSH: 16.5%, non-MSH: 23.0%, P = .008) were significantly less likely to receive palliative care.
Patients With Baseline mUTUC Characteristics by Palliative Care Utilization.
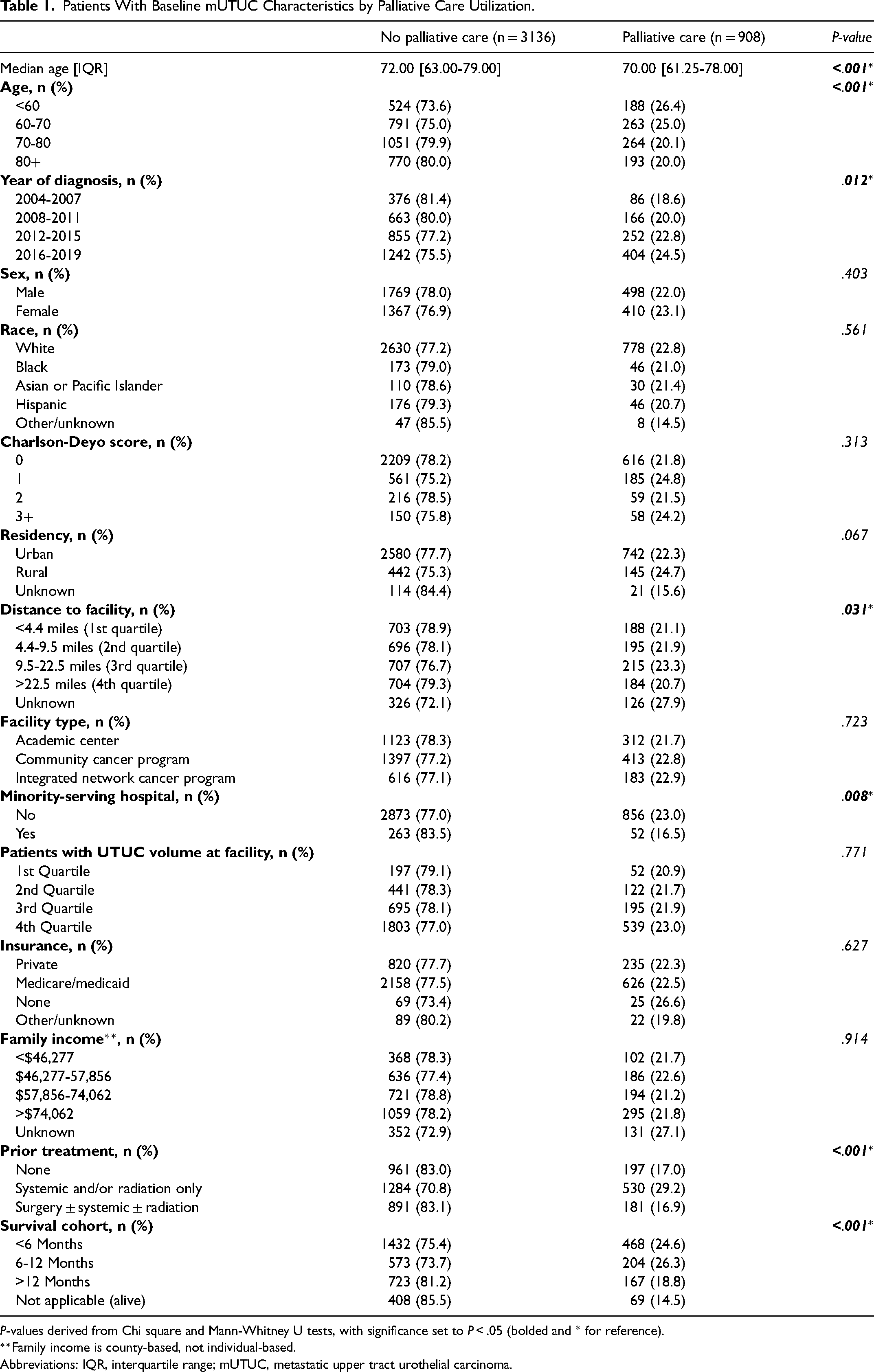
P-values derived from Chi square and Mann-Whitney U tests, with significance set to P < .05 (bolded and * for reference).
Abbreviations: IQR, interquartile range; mUTUC, metastatic upper tract urothelial carcinoma.
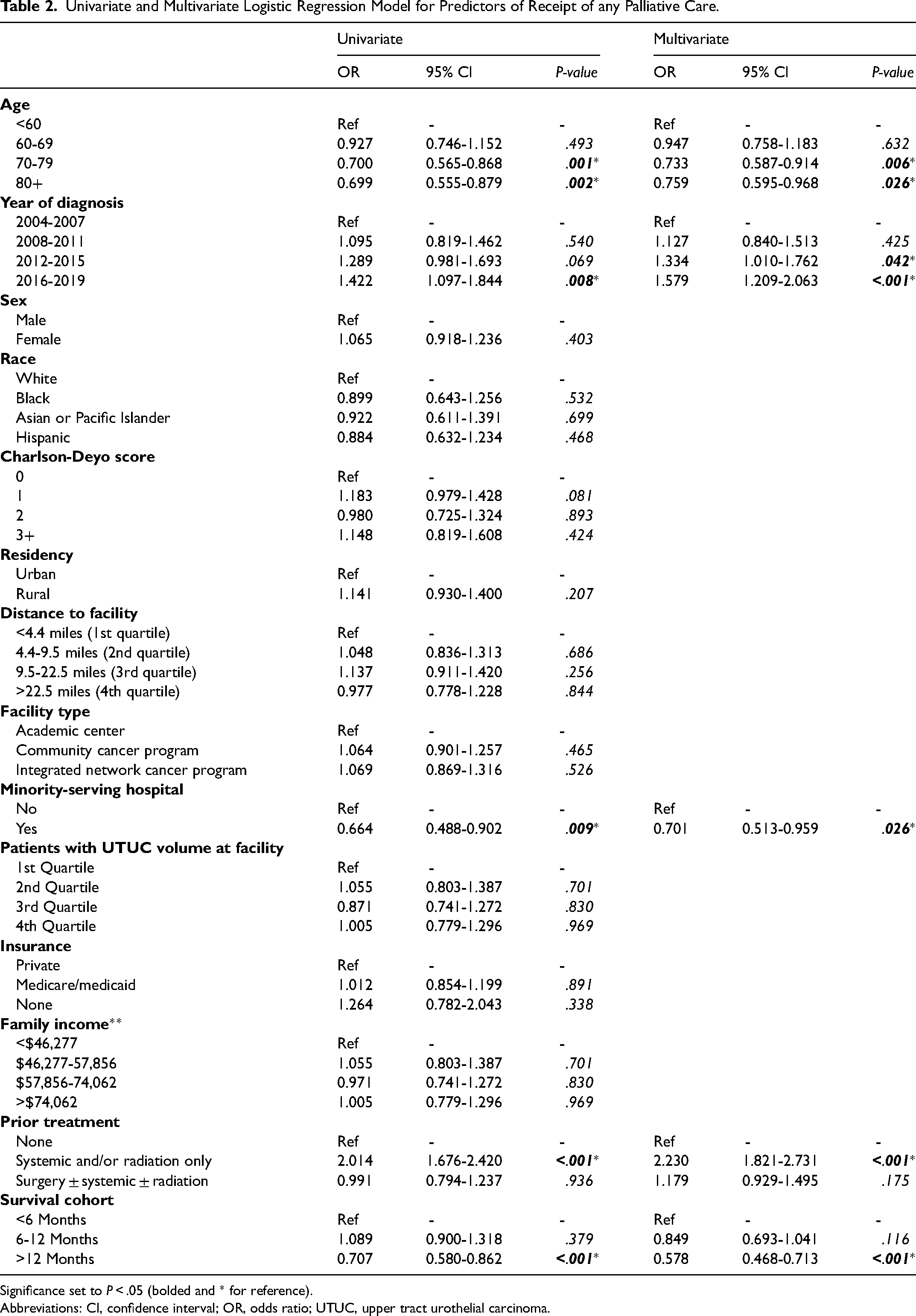
The utilization of palliative care among patients with mUTUC increased significantly from 2004 (15.0%) to 2019 (23.1%), P < .001 (Figure 2). Among those who received palliative care, the most common modality was systemic therapy only (335 of 908, 36.9%), following by radiation only (241 to 908, 26.5%) and pain management only (88 to 908, 9.7%) (Figure 3). On multivariate regression analysis, a recent diagnosis year predicted receipt palliative care (2012-2015: odds ration [OR] = 1.334 [1.010-1.762], P = .042; 2016-2019: OR = 1.579 [1.209-2.063], P < 0.001) when compared to those diagnosed between 2004 and 2007 (Table 2). Receipt of a prior nonsurgical treatment paradigm (OR = 2.230 [1.821-2.731], P < .001) also independently predicted utilization of palliative therapy when compared to patients with mUTUC without prior treatment. Older age (70-79 years: OR = 0.733 [0.587-0.914], P = .006; 80 + years: OR = 0.759 [0.595-0.968], P = .026) and undergoing care at an MSH (OR = 0.701 [0.513-0.959], P = .026) were both negative predictors of receipt of palliative care. Similarly, a prolonged OS negatively predicted palliative intervention (OR = 0.578 [0.468-0.713], P < .001), implying those with a poorer prognosis (ie, OS < 6 months) were significantly more likely to receive palliative care.
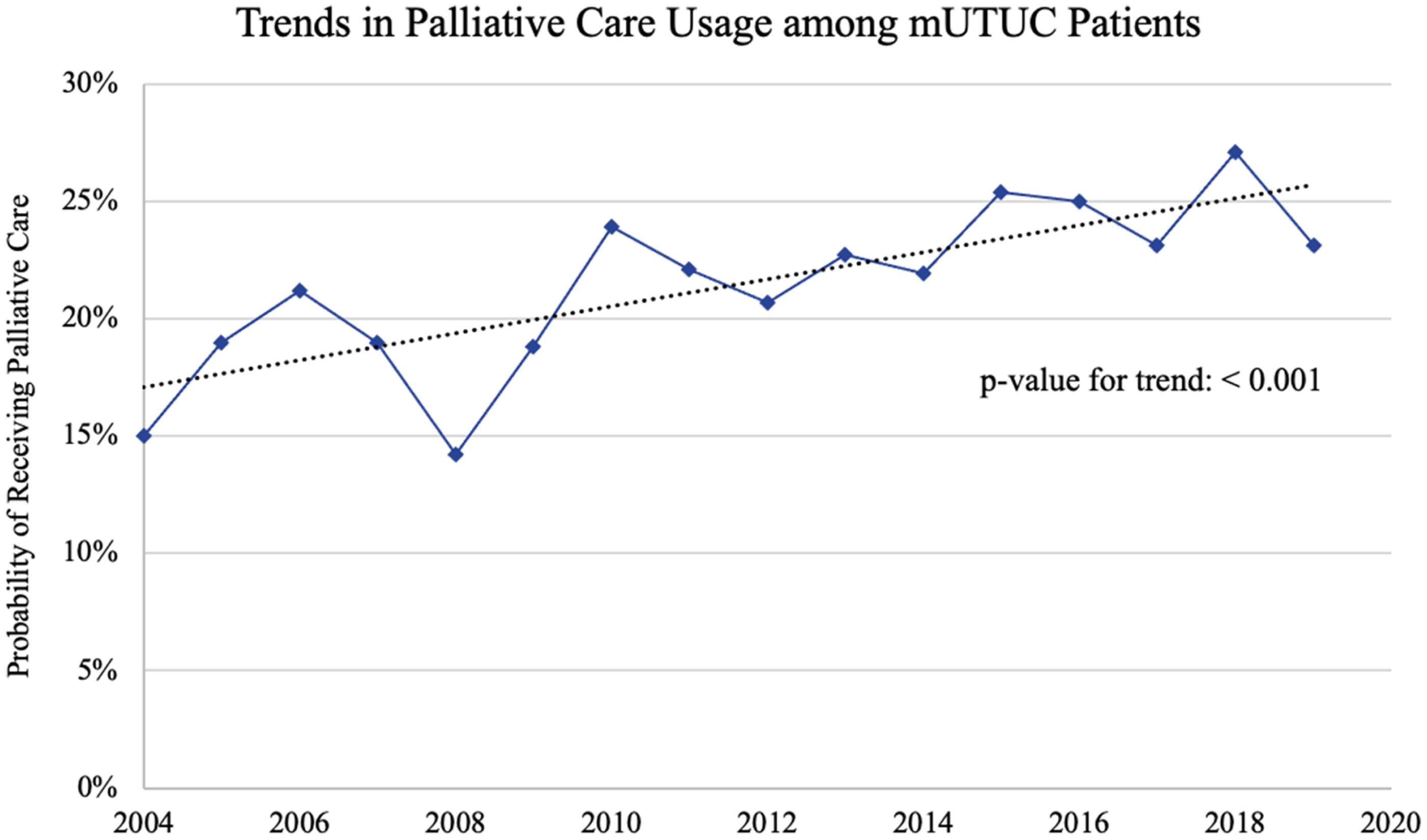
Trend in palliative care utilization for metastatic upper tract urothelial carcinoma (mUTUC) over time.
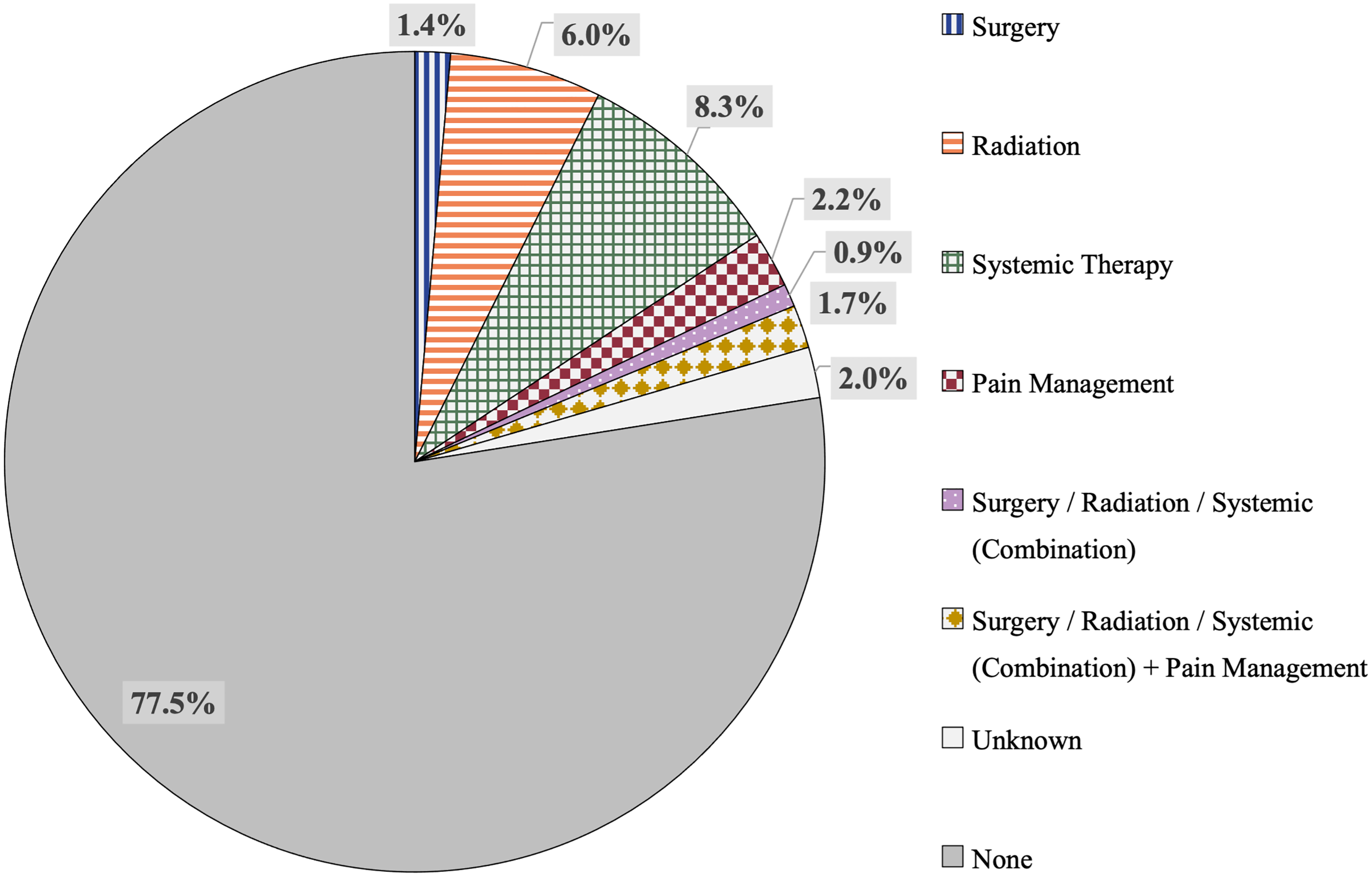
Breakdown of type of palliative care received (if any) among patients with metastatic upper tract urothelial carcinoma (mUTUC).
Univariate and Multivariate Logistic Regression Model for Predictors of Receipt of any Palliative Care.
Significance set to P < .05 (bolded and * for reference).
Abbreviations: CI, confidence interval; OR, odds ratio; UTUC, upper tract urothelial carcinoma.
Discussion
Palliative care plays a crucial role in the management of patients diagnosed with metastatic cancer. However, the trends in the utilization of palliative care for mUTUC remain unclear, and the factors predicting palliative intervention in this population are poorly characterized. Herein, we provide the first study to describe the patterns and predictors of palliative care utilization among patients with mUTUC.
Our study elicited several key findings. First, we found a relatively low but increasing trend of palliative care utilization among patients with mUTUC. Second, we identified several key factors that significantly influenced the receipt palliative care. Notably, a recent year of diagnosis, receipt of a prior nonsurgical treatment paradigm, and an OS <6 months were independent predictors of palliative intervention while undergoing treatment at an MSH and older age were negative predictors.
Our study found an underutilization of palliative care, with less than one-quarter of all patients with mUTUC receiving palliative intervention. This observation exceeded the only other estimate provided in the literature, which found that only 4.4% (n = 54) of patients with mUTUC received palliative care using the Surveillance, Epidemiology, and End Results (SEER)-Medicare linked dataset from 2004 to 2012. 15 The American Society of Clinical Oncology guidelines recommend palliative intervention for all patients with metastatic cancer. 6 Thus, our study suggests that these guidelines have not yet been fully incorporated into the management of mUTUC. Notably, this underutilization persists despite numerous studies indicating quality of life benefits of palliative intervention.3,16,17 Given that curative treatment is generally not possible for patients with mUTUC, improving quality of life vis-à-vis palliation should be a key component of the treatment paradigm in this patient population.
While our study did find a significantly increasing trend of utilization of palliative care, the highest single-year (2018) intervention rate was 27.1%, still representing only a minority of patients with mUTUC. However, this is certainly a promising trend and potentially suggests that recent palliative care guidelines for advanced cancer have begun to influence clinical practice. Future studies should further evaluate this trend in coming years.
There are a host of infrastructural, physician, and patient factors that may contribute to the low utilization of palliative care. Perhaps the most important factor is a shortage of palliative care providers in the United States. Indeed, the current workforce can accommodate only 25% of patients with palliative care needs, and this mismatch is expected to significantly worsen in future decades. 18 On the physician side, potential barriers to utilization include incomplete or inaccurate beliefs about the timing and scope of palliative care or difficulties introducing the concept of palliative care to patients. 19 Other factors contributing to this underutilization include patient-level considerations such as a low awareness of services, a desire to exhaust all established and experimental treatment avenues, and cultural perceptions of palliative care.20,21 For instance, cultural norms play an important factor in Chinese cultures as certain individuals believe in embracing pain with stoicism and often see suffering as an opportunity for spiritual growth. 22 Futhermore, palliative care is often stigmatized by certain cultures and individuals as it can carry a negative connotation of death, dying, and “giving up.” 23 In fact, a study of 2594 US adults found that 44.4% of individuals automatically think of death whan hearing palliative care, 38.0% equate palliative care with hospice, and 15.9% see palliative care as giving up. 24 These cultural nuances and stigmas can significantly impact care utilization, suggesting the need for culturally sensitive education and outreach to normalize and humanize palliative care discussions.
Our study also identified several factors associated with the receipt of palliative intervention. Notably, older patients with mUTUC were less likely to receive palliative care. This finding is not unique and has been consistently reported in the literature.7,13 Differences in symptom burden alone are unlikely to explain this variation, given that research has demonstrated similar symptoms among older patients with advanced malignancies. 25 Rather, a potential explanation for this disparity is the inability to distinguish disease symptoms from frailty, highlighting a potential area of further education for physicians caring for those with advanced cancer. Other contributing factors may include a decreased desire to subject themselves to further treatment and reduced access to palliative services among geriatric patients.13,26
Receipt of care at an MSH was also associated with a lower likelihood of undergoing palliative therapy. Prior studies have demonstrated that minority patients are less likely to receive palliative care for metastatic cancer. 27 However, it is unclear whether this disparity is due to differences in care at an MSH or due to different treatment of minority patients in general. Our study suggests that site of care may be an important contributor to not only lower utilization of palliative therapy for mUTUC but also race/ethnicity-based disparities in the utilization of these services. Similarly, a study by Cole et al 12 also found that treatment at an MSH, but not race/ethnicity itself, was associated with a significantly lower odds of receiving palliative care for those with metastatic prostate, breast, colon, and lung cancer. Together, this highlights an alarming disparity in the delivery of palliative intervention and warrants further investigation into the causes of this discrepancy.
Treatment and survival considerations also represented important predictive factors for palliative intervention. Patients receiving prior nonsurgical treatment were more likely to receive palliative care compared to untreated patients and those that underwent prior surgery. Potential reasons for this difference include that these patients had more advanced disease than those who were able to undergo surgical resection and that patients who refused prior treatment may also have been more likely to refuse palliative care. We also found that patients with a shorter OS were more likely to receive palliation than those who survived longer. This likely reflects a greater tendency to utilize palliative care in patients with the most advanced stages of disease, which may show that physicians are adept at selecting patients who might benefit from these services the most. Alternatively, this could indicate discriminate utilization in actively dying patients, despite current guidelines advocating for the early integration of palliative therapy into the care of all patients with advanced malignancy.3,28
As the armamentarium of treatments for UTUC advances, the prevalence of patients living with metastatic disease will likely rise. Palliative care has been shown to be vital for improving the quality of life and offering holistic support for those living with advanced cancer. Furthermore, its utilization becomes indispensable for individuals facing poor prognoses and limited treatment options, such as those with mUTUC. Our study suggests that despite increasing rates of palliative intervention among patients with mUTUC, innovative solutions are required to overcome the relatively low utilization of palliative care in this vulnerable population. Moreover, if we can target these solutions, and others, toward individuals that may be less likely to undergo palliative care—such as older patients and those treated at MSHs—the impacts of these strategies may be amplified even further.
An important area to focus on to not only increase palliative care access for patients with urological malignancies but all advanced illnesses would be to increase the number of palliative care providers in the United States. One strategy could be to expand the number of palliative medicine fellowship positions and to increase the applicant pool for these fellowships.29,30 Indeed, a study by Kamal et al 30 highlighted that a sustained growth in palliative care fellowship positions over 10 years could reverse the worseneing workforce shortage. Other solutions might involve offering training programs for mid-career profressionals who wish to transition into palliative medicine in order to expand the workforce and meet the projected need for palliative care providers. 31
Another, more-targeted, potential avenue to explore is the expansion of integrated palliative care-urology clinics. These partnerships have already been shown to achieve high rates of end-of-life hospice care as well as advance care planning among patients with urological malignancies, and they will likely be important toward expanding palliative therapy in the future.32,33 However, given the shortage of palliative care clinicians, it may also be important to augment skills in primary palliative care among surgeons. While the American College of Surgeons supports integrating palliative care with surgery and extensive educational resources currently exist to independently develop palliative care expertise, there has been limited integration of formal palliative care education into the training of surgical specialties such as urology. 34 Widespread adoption of palliative care into surgical residency curriculum may result in a more effective delivery of palliative services in surgical settings, likely improving patient outcomes.
The study has certain strengths but also carries several limitations. By relying on the NCDB, our study can offer the most comprehensive evaluation of palliative care trends as it is the largest cancer database in the United States which captures over 70% of newly diagnosed malignancies. Moreover, all chart abstraction is performed by trained registrars, leading to standardized data collection across facilities. However, utilization the NCDB carries inherent limitations including a lack of longitudinal treatment data, patient-reported outcomes, or cause of death in addition to selection bias given that it only includes patients at CoC-accredited facilities. Other limitations in our analysis specific to palliative care include that the NCDB only provides information on palliative intervention, thus it may overlook more holistic and nontraditional approaches to palliative therapy. Additionally, the database does not record the number of times palliative care was received or at what time during the disease course that it was delivered. Lastly, the NCDB does not include information on palliative care consultations or goals of care discussions which means it is not possible to determine whether patients declined palliative therapy. In particular, this means that it is unable to discern whether disparities in palliative care utilization in mUTUC are due to patients being offered palliative care less or that they are refusing intervention at a higher rate. Future studies should explore this concept, particularly for older patients and those treated at an MSH.
Conclusions
There is a low but increasing trend of utilization of palliative care among patients with metastatic upper tract urothelial carcinoma. Older patients, those treated at a minority-serving hospital, and patients with a better survival prognosis were less likely to receive palliative intervention. Expansion of palliative care services remains a key opportunity to improve quality of life and enhance patient-centered care among those with metastatic upper tract urothelial carcinoma. Further studies should explore patient-, physician-, and system-level factors that contribute to discrepancies in evidence-based utilization of palliative care for advanced urological malignancies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.