
Abstract
Objective
There is increasing interest in advance care planning (ACP) and the implementation of various forms of ACP. The purpose of ACP is to define patients’ goals and preferences for future medical treatment and care for patients nearing the end of life (EOL). The aim of this study was to investigate adherence to patients’ preferences for levels of life-sustaining treatment in emergency situations, as documented in a Danish POLST (Physician Orders for Life-Sustaining Treatment) form.
Methods
A retrospective journal review was conducted 2 years after the conversation with the patients about their wishes for treatment and care at EOL. Medical records included electronic hospital records, nursing home records, and general practice records. Patients were assessed nearing EOL and included in the study based on a negative response to the “surprise.”
Results
A total of 120 patients and nursing home residents were included in the study. Overall, there were 2148 contacts with the healthcare system, of which 31 were emergency situations, where the patients were not capable of expressing their own wishes. In 4 contacts (12%), the patients (4) received treatment discordant with their wishes, as documented in the POLST form (and medical record).
Conclusions
Our study shows that patients assessed nearing EOL are a patient group with many contacts with the healthcare system, and the results indicate that having had an ACP conversation and the wishes documented is useful to avoid unwanted treatment in emergency situations.
Keywords
Introduction
Advance care planning (ACP) refers to the process of discussing, identifying, and documenting decisions and preferences about care and treatment at end of life (EOL) with the patient, family, and healthcare personel.1,2 Interest in ACP is growing, as supported by the increase in laws and public awareness on the topic, 2 as well as the implementation of different ACP forms. 3
As the world population is expected to grow older and live with chronic and potential severe diseases longer,4,5 it is likely that more patients would benefit from ACP discussions and conversations about EOL. In addition, discussing ACP preferences may lead to better concordance between preferences and received care and a better match between preferred and actual place of death. 6 This, however, requires an effort from not only palliative care physicians but also physicians from other specialties and healthcare settings to prioritize and conduct ACP conversations. 7
The process of ACP has broadened from completing a legal advance directive to a process that consists of more steps, such as defining values and preferences and communicating these to others. 8 It may also include choosing a surrogate decision-maker.9,10 The purpose of ACP is to be able to define goals and preferences for future medical treatment and care 2 and ACP conversations encourage patients or individuals to share their wishes for future treatment with their healthcare providers and their relatives. 2
A variety of ACP forms are implemented across the world. One of the most researched and used is the American POLST (Physician Orders for Life-Sustaining Treatment) form.11,12 The POLST form is a portable medical order, but a common requirement is that the forms should only be filled out and signed after an in-depth conversation between the patient and a healthcare provider regarding the patient's goals of care.13,14
In Denmark, several regional projects15–18 have shown the benefits of ACP conversations and having patient's wishes documented in the medical record in case of an emergency situations, where the patient is in a state not capable of expressing own wishes. However, no nationwide ACP document is yet developed or implemented and for most physicians using an ACP document is not common practice. 19
In 2017, the American POLST form was translated and adapted into a Danish version, and the Danish POLST (Patient-and-Physician Decisions for End-of-Life) form was tested among Danish patients and nursing home residents. 15 The study showed that the Danish version of the POLST form was assessed by both patients and healthcare personnel as a useful model for obtaining and documenting Danish patients’ preferences for life-sustaining treatment15,18 and the form could ease the invitation to help in conducting conversations about EOL. 20
However, no follow up or investigation of adherence to the wishes documented in the Danish POLST study have been conducted and though the benefits of the American POLST form are well established,12,21 several differences between the Danish and the American healthcare systems make the comparison difficult. The compatibility to the Danish healthcare system is hence unknown. Accordingly, such an investigation is needed to ensure the usefulness of the POLST form in other healthcare systems than the American.
The aim of this study was to investigate the usefulness of and adherence to patients’ preferences for levels of life-sustaining treatment in emergency situations where the patient was not capable of expressing own wishes for treatment and care.
Methods
The Danish POLST Study
From 2017 to 2020, Tuesen et al15,18 conducted “The Danish POLST study,” in which the American POLST form was translated and adapted into a Danish version (see Supplemental Material I), which was tested on Danish patients and nursing home residents. 15 The American POLST form contains 3 topics the patient must decide on: (1) cardiopulmonary resuscitation (CPR), (2) level of medical interventions (full treatment, selected treatment, and palliation only), and (3) artificially administered nutrition.22,23 The American POLST form is a legally binding document and needs to be signed by a healthcare professional to be valid. The form should only be filled out and signed after an in-depth conversation between the patient and a healthcare provider regarding the patient's goals of care.13,14
Study Design
In this project, we retrospectively reviewed the records of the patients in the Danish POLST study 2 years after they participated in the conversation and completed the POLST form with a physician. Medical records included electronic hospital records, nursing home records, and general practice records.
Settings and Participants
The project sites included hospital wards, outpatient clinics, GPs, and nursing homes from both rural and urban areas from 4 out of 5 Danish regions.
Patients were eligible for inclusion in the study if the physician at the project site assessed that they were nearing EOL based on the “surprise question” (Would I (a healthcare professional) be surprised if this patient died within the next 12 months? 24 ) and would benefit from a conversation about wishes for treatment and care in emergency situations. Studies have shown that the risk of dying within a year is higher, with a negative response to the surprise question,25,26 which indicates that these patients possibly are nearing EOL, because of severe frailty, advanced disease, or old age, and might benefit from ACP. 27 Patients were excluded from the study if they were younger than 18 years old and/or could not speak or understand Danish.
After inclusion, the patients had a conversation with their physician and, if possible, a relative to discuss and document their wishes for treatment at the EOL aided by the Danish POLST form. 18 After the conversation, the patient's wishes were registered on the Danish POLST form and in the patient's medical record, since the POLST form was not yet a legal document. 18
In addition, with permission from the patients, the project sites agreed to be contacted and to deliver extracts from the patients’ medical records 2 years after the conversation (Figure 1).
Data Collection
From September 2020 to October 2022, the participants’ medical records were retrieved from the respective project sites either electronically via the hospitals’ journal system or sent by mail or email and accessed by the first author. Only journal material from the project sites was accessible to retrieve data for the current study; if the patient was included from a general practice, only the GP's medical records were available, and vice versa if the patient was included in the hospital, only hospital admissions were retrievable. Depending on the project site, the amount of data materiel differed from 2 pages (eg, recording of 2 annual outpatient visits) to more than 100 pages of journal notes (including list of medicines, test, and blood sample results).
All patient contacts with the Danish healthcare system mentioned in the accessible medical records were recorded during the period from completion of the POLST document to 2 years later. Patient contacts included hospital admissions, outpatient consultations, and consultations with their GP both at the clinic or home visits. Admissions to the hospital or hospice were registered as one contact regardless of the length of the admission.
Contacts by the participants to the healthcare provider by telephone or email, contacts by relatives or home care personnel regarding the participants, renewal of prescriptions and mail correspondences between healthcare settings and the project site were not included in the data.
Contacts were assessed as “relevant” in connection with the study aim if the patient had been in a state in which he or she was not capable of expressing his or her own wishes. The contacts were assessed as “irrelevant” if the patient was capable of expressing his or her own wishes (Table 1).
The definitions of relevant and irrelevant contacts and which contacts to register and not register were made as consensus decisions between the first and last authors. Additionally, baseline data such as age, gender, comorbidities, and possible time of death were registered.
Data Analysis
The data were analyzed with descriptive statistics using the BE Stata 17.0 statistical programme. Categorical data are presented with numbers and percentages. Continuous, normal distributed data are presented with min/max, mean, and standard deviation.
Ethical Considerations
This project was registered with the Danish Data Protection Agency (journal number 17/32456). The Committee on Health Research Ethics for Southern Denmark was contacted before inclusion of patients was initiated in 2017. The Committee assessed the study and concluded that according to Danish law the study did not require ethical approval (March 29, 2017). To ensure data security, a license agreement was obtained with the Open Patient data Explorative Network (OP1202).
Written informed consent agreeing to contact the project sites and retrieve their medical records 2 years after the POLST conversation was obtained from all patients at the time of the POLST conversation. The study was conducted in accordance with the Helsinki Declaration.
Results
A total of 120 patients and nursing home residents were included in the Danish POLST study. For one patient, it was not possible to retrieve the record; hence, this patient's data are unknown, and the patient was excluded from this study. Table 2 shows the characteristics of the patients and their treatment preferences according to the Danish POLST form based on total number of participants, dead within the 2-year follow-up period and survivors. Most of the participants were included from hospital departments (57%), of which 23 (27%) came from oncological departments. A total of 74 patients (63%) died within the 2-year follow-up period. Most patients did not want CPR in the event of cardiac arrest (90%); only 17 (14%) wanted full treatment, and 89 (75%) did not want artificial nutrition if they were unable to consume nutrition orally.
Elaboration of Assessment of Contacts and Patient Capacity.
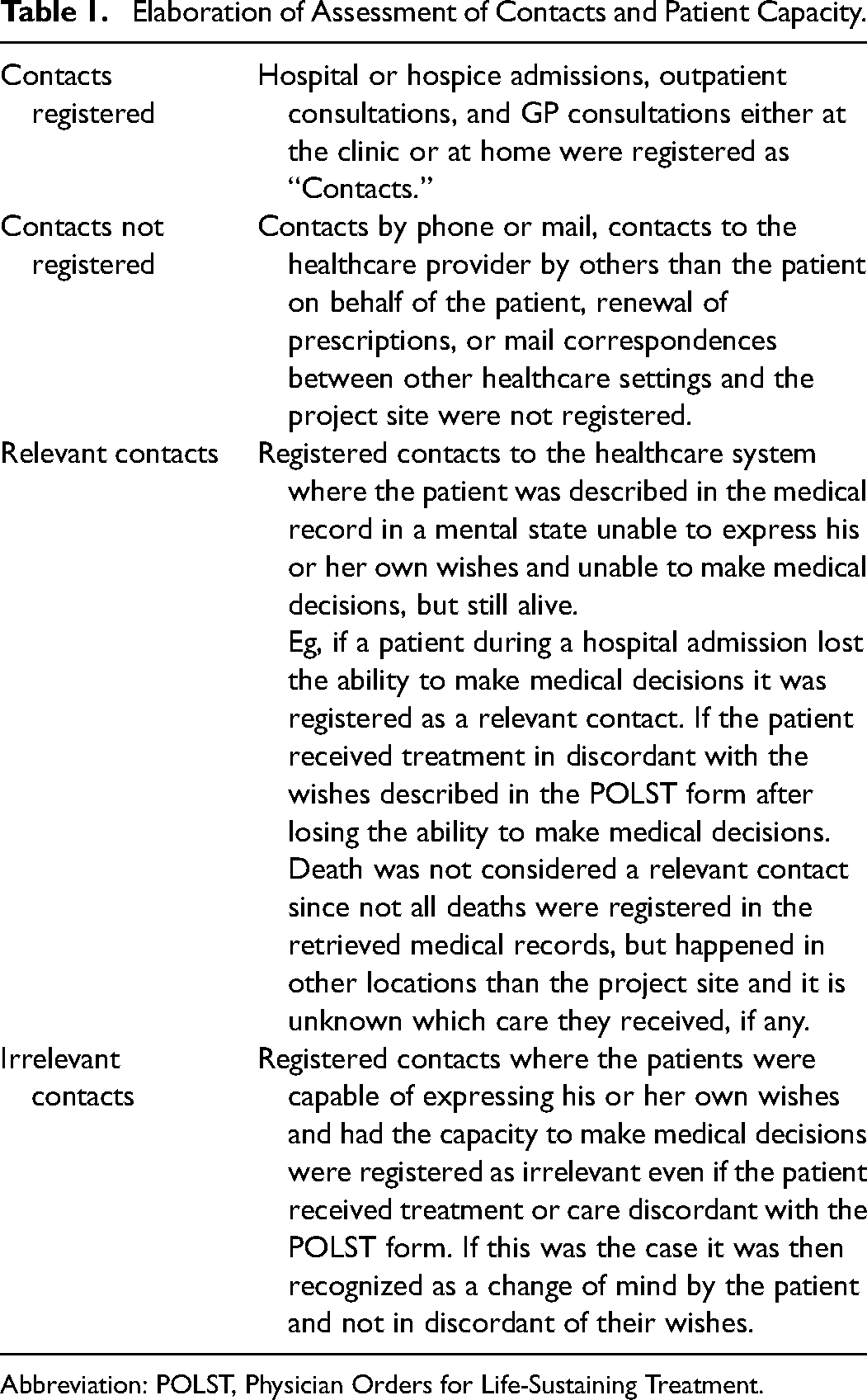
Abbreviation: POLST, Physician Orders for Life-Sustaining Treatment.
Characteristics of the Patients and Preferences According to the Danish POLST Form.
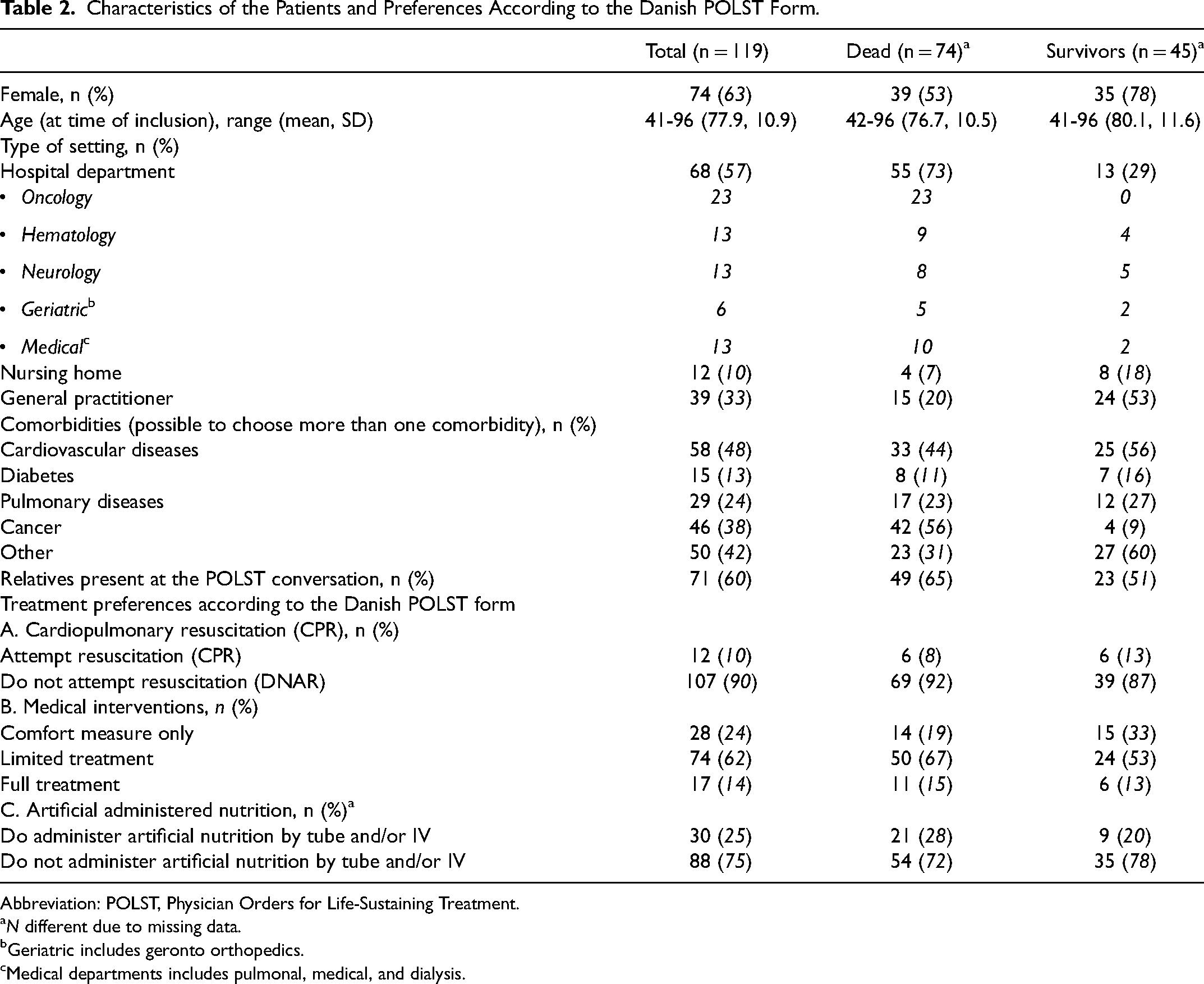
Abbreviation: POLST, Physician Orders for Life-Sustaining Treatment.
N different due to missing data.
Geriatric includes geronto orthopedics.
Medical departments includes pulmonal, medical, and dialysis.
As seen in Table 3, a total of 2148 contacts with the healthcare system were registered during the period from completing the POLST document to the 2-year follow-up. Of these contacts, 31 were assessed as “relevant” and attributed to 26 patients. In 27 of the contacts (attributed to 22 patients), the treatment received was in accordance with the wishes documented in the POLST form, whereas 4 contacts (distributed to 4 patients) resulted in treatment discordant with the patient's wishes. In the cases of discordance, the patients received more aggressive treatment than they wanted in all 4 cases; 1 patient received CPR, 2 patients were admitted to intensive care for life-prolonging treatment, and 1 patient had a feeding tube inserted. In the case of the patient having a feeding tube, the relatives managed to convince that the medical staff terminated the nutrition after a few days, while the patient was still assessed as not cognitively relevant, with reference to the patient's treatment preferences documented in the POLST form.
Number of Contacts With the Healthcare System.
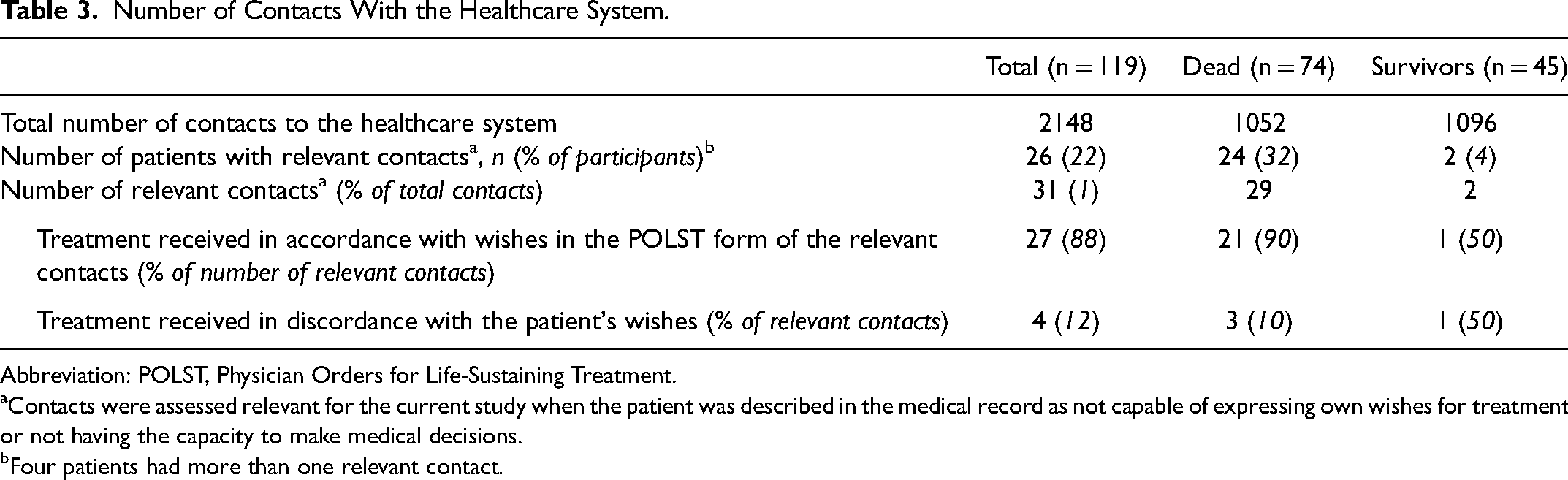
Abbreviation: POLST, Physician Orders for Life-Sustaining Treatment.
Contacts were assessed relevant for the current study when the patient was described in the medical record as not capable of expressing own wishes for treatment or not having the capacity to make medical decisions.
Four patients had more than one relevant contact.
All patients receiving treatment that was discordant with their POLST form had relatives present at the time of completion of the form. All these patients had opted for no CPR, and they all wanted “limited treatment.”
Most of the relevant contacts were registered for patients who died during the 2-year follow-up, and only 2 relevant contacts were found with patients still alive after the 2-year follow-up (see Table 2).
Of the patients who died during the 2-year follow-up, 55 (74%) were included from hospital departments, whereas 4 were included from nursing homes (corresponding to 5% of all deaths and 33% of the total number of patients included from nursing homes) (Table 4). As the only project site, all of the included patients from the oncological departments died within the 2-year follow-up.
Patients Who Died Within the 2-Year Follow-Up Period.
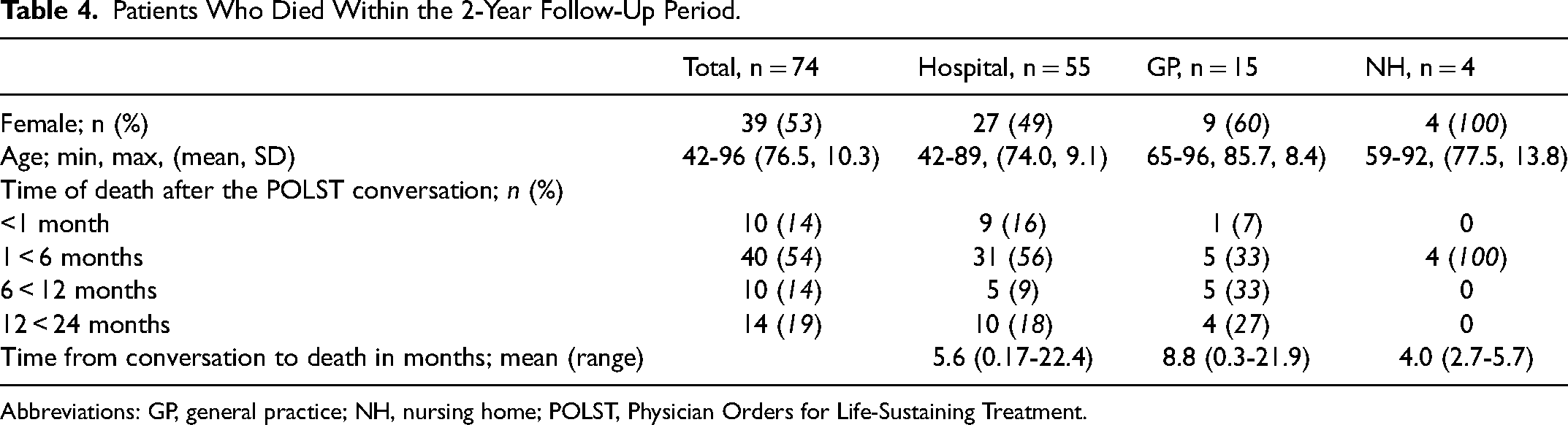
Abbreviations: GP, general practice; NH, nursing home; POLST, Physician Orders for Life-Sustaining Treatment.
As seen in Table 4, most of the patients died within the first year after the POLST conversation (81% of the patients died within the follow-up period; 49% of all included patients), most of them at a hospital department. A substantial number of the patients who died before follow-up (68%) died within the first 6 months after the conversation, and only 19% of the patients died within the second year after the conversation.
Discussion
The patients in this study were all assessed by the surprise question, had a conversation about wishes for EOL and emergency treatment, and filled out a Danish version of the POLST form 2 years prior to this follow-up study. Our results showed that this is a patient group with many contacts with the healthcare system and in risk of losing the ability to make medical decisions. This indicates a patient group for whom it is important to talk about and document wishes for treatment at EOL to avoid unwanted treatment in situations where they are not capable of expressing their wishes for treatment and care.
Our results showed that about one-fourth of the patients had a “relevant contact” (an episode where they were not capable of expressing their wishes regarding treatment and care) with the healthcare system during the 2-year follow-up. In most of the registered cases (88%), the treatment received was in accordance with the patient's wishes documented in the POLST form or medical record. It is not possible to determine whether the patient would have received the same treatment without the conversation and instead based on the physician's assessment, since we did not compare the patients with a POLST form with a group of patients without a POLST form.
What happened in the situations in which the patients received treatment in discordant with the wishes documented in the POLST form is uncertain or unknown. Even though the patients’ wishes documented in the POLST form were also registered in the patients’ medical records, the electronic journal systems used in different healthcare settings across Denmark do not always correspond and the healthcare staff at a hospital would not be able to see what the general practitioner has documented in their journal and vice versa. Hence, in many cases, the wishes for treatment are unknown to the treating physician, unless the relatives present are able to inform the healthcare personnel about the conversation and treatment preferences.
The majority of the patients in the Danish POLST study declined CPR, preferred limited medical intervention or comfort care, and did not wish for artificial nutrition. 18 In all the cases of discrepancies, the patients received more aggressive treatment than they would have wanted. However, in the case of the patient who had a feeding tube inserted, the relatives convinced the medical staff to terminate the nutrition after a few days because of the wishes in the POLST form. This implies that the form was useful as a way for the relatives to know the patient's wishes and to help secure that treatment was in accordance with the patient's wishes. This emphasizes the importance of having relatives present in the conversation.
Identifying patients nearing EOL or patients who might benefit from ACP is known to be a difficult task.28,29 The surprise question is included in several palliative care guidelines28–30 and is widely used across settings. Several studies31–33 have shown that death among cancer patients is easier to predict because of the disease trajectory compared with patients suffering from other diseases or old age. Our results support these findings, as all patients included from oncological departments died within the 2-year follow-up period, whereas patients from nursing homes and GPs were more likely to survive than die within this period. This emphasizes that the use of the surprise question to assess patients who do not suffer from cancer may be inconclusive.24–26 Nevertheless, the surprise question is still considered a valid tool to help identify patients who would benefit from EOL conversations. 24 However, several studies recommend that the surprise question be used alongside other prognostic tools,25,28,30 since not all patients in need of ACP may be captured by a generic tool such as the surprise question. 28
Strengths and Limitations
The strengths of this study are the wide range of different project sites from both rural and urban areas and the inclusion of patients from hospitals, GPs, and nursing homes. This gave a broad and nuanced view of the wishes for treatment at EOL from different patient groups with heterogeneous backgrounds and reasons for nearing EOL. Furthermore, the 2-year follow-up gives the possibility to get an impression of the patient group and their use of the healthcare system, while also the long time follow up gives an indication of the use of the surprise question to assessing patients for ACP conversations.
As a limitation, there might have been a tendency for the physicians at the project sites to select patients of whom they had the impression that the patient already had some opinions about treatment and wishes, and where the physician had a good relationship with the patient and relatives, hence presenting selection biases.
Another and rather substantial limitation was the difference in the amount and quality of journal material depending on the project site which made it difficult to retrieve the same data for all patients. Furthermore, documentation of care and treatment received when the patients were dying was only available if the patient died at the project site. As a consequence it is reasonable to assume that more than the registered “relevant contacts” have occurred during the 2-year follow-up, and it is unknown whether treatment was in concordance in these cases.
Conclusion
The study shows that patients assessed nearing EOL are a patient group with many contacts with the healthcare system. Only in about a tenth of the study-relevant contacts was the treatment provided discordant with the patient's wishes, indicating that having had an ACP conversation is useful to avoid unwanted treatment.
Flowchart of the Danish POLST study and the 2-year follow-up.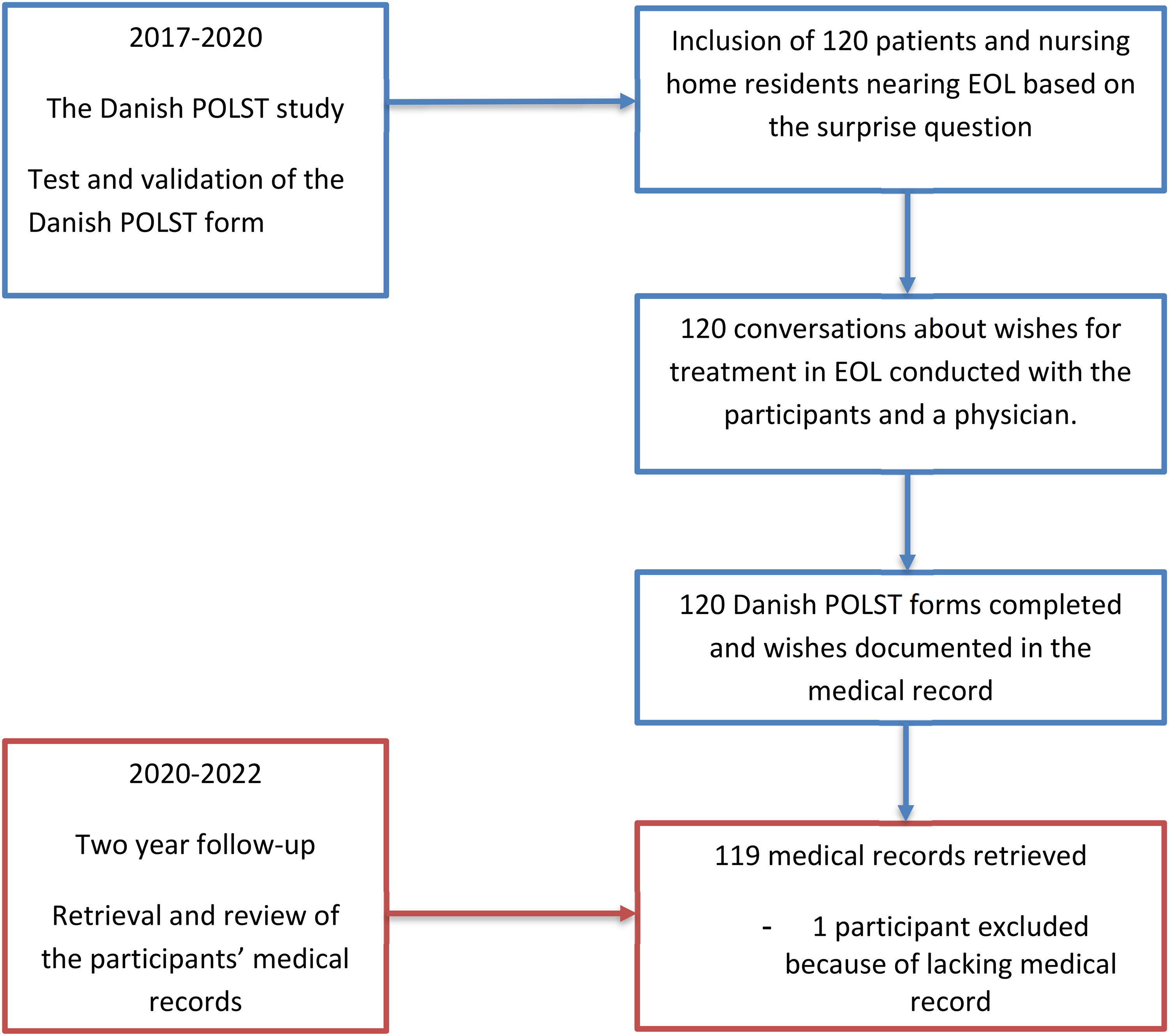
Supplemental Material
sj-docx-1-pal-10.1177_08258597251329842 - Supplemental material for Adherence to Patients’ Preferences for Levels of Life-Sustaining Treatment: A 2-Year Follow-Up Study
Supplemental material, sj-docx-1-pal-10.1177_08258597251329842 for Adherence to Patients’ Preferences for Levels of Life-Sustaining Treatment: A 2-Year Follow-Up Study by Mette A. Smith, Anne C. Brøchner, Helene K. Nedergaard and Hanne I. Jensen in Journal of Palliative Care
Footnotes
Authors’ Note
Availability of Data and Materials: The data are available from the first author upon reasonable request.
Acknowledgments
The authors would like to thank the project sites for forwarding journal material for the study and Open Patient data Explorative Network for the secure storage of the data.
Authors’ Contributions
The study was designed by HIJ, and MAS collected and analyzed the data and drafted the manuscript. HIJ, MAS, ACB, and HKN participated in the discussion of the findings, critically revised the manuscript, and approved the final version. *Note: Since completing the research MA Smith has moved to Department of Anesthesiology and Intensive Care, Odense University Hospital, Odense, Denmark.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
This project was registered with the Danish Data Protection Agency (journal number 17/32456). The Committee on Health Research Ethics for Southern Denmark was contacted before inclusion of patients was initiated in 2017. The Committee assessed the study and concluded that according to Danish law the study did not require ethical approval (March 29, 2017). To ensure data security, a license agreement was obtained with the Open Patient data Explorative Network (OPEN) (OP1202). Written informed consent agreeing to contact the project sites and retrieve their medical records 2 years after the POLST conversation was obtained from all patients at the time of the POLST conversation. The study was conducted in accordance with the Helsinki Declaration.
Funding
This study was supported by the Development and Research Fund, Danish Regions and the Health Cartel (15.2.2017), the Region of Southern Denmark, Lillebaelt Hospital, University Hospital of Southern Denmark and the University of Southern Denmark.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.