
Abstract
Objectives
Recently, atrial fibrillation (AF) has contributed to an increase in cardiovascular deaths in the U.S. Palliative care (PC) and atrial ablation (AA) procedure can elevate quality of life of high-risk AF patients, who are associated with multiple comorbidities. We explore the combined PC and AA management among high-risk mortality groups with AF.
Methods
This pooled cross-sectional retrospective data used the National Inpatient Sample (2016-2021) and included national estimates of 2,965,334 hospital discharges in the high-risk mortality group with AF. Multivariable regression was performed to determine the factors associated with AA procedure and PC centered on CHA2DS2-VASc score, systolic heart failure, and in-hospital mortality. Race/ethnicity, health insurance, and hospital location were controlled in multivariable analyses.
Results
Palliative care utilization was on an uptrend from 9.02% in 2016 to 12.29% in 2021. Factors that were negatively associated with PC utilization were increasing CHA2-DS2-VASc score (OR = 0.878), systolic heart failure (OR = 0.976), AA procedure (OR = 0.287), racial minorities, and rural residents. Atrial ablation was positively associated with systolic heart failure (OR = 2.920) and was negatively associated with increasing CHA2-DS2-VASc score (OR = 0.951) and PC utilization (OR = 0.283). Racial minorities and rural residents were less likely to receive AA procedure.
Conclusions
Palliative care utilization was associated with lower probability of AA procedures by approximately 75%, and vice versa. Atrial ablation procedures and PC utilization were discrete choice patterns indicating healthcare providers’ tendency to favor the status quo and current practices rather than initiating change. Health disparities in PC utilization and AA procedures were identified in racial minorities and rural residents. Call to action is warranted to increase PC awareness and harmonious approach of PC and AA procedure for those with high-risk mortality AF patients in the U.S. hospitals.
Introduction
Atrial fibrillation (AF) is one of the most common heart rhythm disorders, affecting millions of people worldwide and significantly increasing the risk of mortality, reaching about 276,373 cardiovascular deaths from 2011 to 2018 in the U.S. 1 The complications and multiple comorbidities associated with AF increase mortality and worse health outcomes. 2 The prevalence of AF is projected to increase to 12.1 million in 2030, with approximately 2.6 million new diagnoses expected within the same year in the U.S. 3 Most patients diagnosed with AF are symptomatic, manifested by palpitations, fainting, dyspnea, dizziness, and fatigue. 4 Atrial fibrillation is also positively correlated with an increased risk of heart failure (HF) and stroke. As such, patients with AF accompanied by HF have significant systolic dysfunction, resulting in advanced cardiac disease that raises mortality and hospitalizations. 5 Additionally, those with higher CHA2DS2-VASc scores are at risk of developing stroke, ultimately leading to poorer health outcomes. 6
Atrial fibrillation tends to occur in the older adult population, and it is therefore associated with other health conditions such as cognitive impairment, falls, and disability. 7 Notably, poor health outcomes are reported among AF individuals with unfavorable social determinants of health; for example, public health insurance payor (Medicare, Medicaid) and rural residence.8,9 Individuals with AF are often hospitalized in critical condition due to advanced, complex, and multiple comorbidities. Palliative care (PC) is well recognized as an optimal comprehensive approach for hospitalized individuals with advanced illnesses in cancer and noncancer conditions.10–12 Palliative care provides benefits of quality of care in cardiovascular disease by promoting hospital course understanding, symptom management, decision-making, goals of care establishment, and end-of-life preparation. 11 A recent national study on acute HF identified the above benefits of PC; however, its utilization remains limited, with only 4.1% PC encounters. 13 Despite this, HF has been recognized as a condition that reduces quality of life and lowers survival after hospital discharge. 14 A similar study found that only 4.5% of patients received inpatient PC for critical conditions, for example, cardiogenic shock, with in-hospital mortality rate of 35% to 40%, despite its increasing adoption in cardiovascular conditions. 15
Hospitalized individuals with AF may be advised to undergo certain procedures to improve their quality of life. One such procedure is atrial ablation (AA), aimed at restoring sinus rhythm with resulting reductions in recurrent AF and progression to HF. 16 The AA procedure is considered a first-line approach to manage symptoms related to uncontrolled AF. 17 Furthermore, AA reduces cardiovascular deaths not just in patients with AF but also in those with HF, 18 thus improving clinical outcomes. However, despite the promising outcomes of AA procedure, patients with AF, especially those at higher risk of mortality, may benefit from advanced care management planning. The burden of symptomatic AF and its associated multiple comorbidities highlights the necessity of PC.
Hospitalized AF individuals are often critically ill and in need of both PC and AA procedure. Yet, this simultaneous combined management of PC and AA procedure is largely unexplored among high-risk mortality hospitalized AF individuals. Therefore, using a nationally representative dataset and analyzing AF individuals’ high risk of mortality, we aim to (1) investigate factors associated with PC and AA procedure and to (2) determine the health disparities associated with PC and AA procedure.
Methods
Data Source and Study Sample
This study utilized a pooled, cross-sectional, retrospective data analysis using the National Inpatient Sample (NIS) database from 2016 to 2021. The Institutional Review Board (IRB) at the University of Nevada Las Vegas found that the data included in the analysis is de-identified thereby safeguarding privacy and confidentiality concerns, and the current study to be exempt (IRB no. 1098939-3). Informed consent was waived due to the de-identified data nature of the NIS. The NIS is a product of the Healthcare Cost and Utilization Project, sponsored by the Agency for Healthcare Research and Quality, including about 7 million unweighted and 35 million weighted hospital stays in the U.S. 19 Additionally, the NIS is developed to provide projections of illnesses and interventions to specific demographic groups as well as estimations of healthcare utilization, cost, quality, and outcomes.19,20 Our study includes hospital discharges in the high-risk mortality group by using the All-Patient Refined Diagnosis-Related Group subclasses 3 (major complications) and 4 (extreme complications) that were approximately 60% of all cases and are described elsewhere.12,19,20 Atrial fibrillation individuals were identified through the International Classification of Disease, Tenth Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS). Supplemental Table 1 presents ICD-10/PCS codes in detail. Our final study cohort consists of 2,965,334 hospital discharges in the high-risk mortality group and admitted with AF, with a weighted national total of 14,826,664 in the 6 years.
Measures and Data Analysis
There were 2 primary dependent variables, PC and AA procedure; both were dichotomous variables. Our analysis focused on the proportion of PC utilization by year and how PC utilization affects the AA procedure. The main independent variables in multivariable models included risk of stroke measured by the CHA2DS2-VASc Score, ranging from 0 to 9, 21 occurrence of systolic HF, and in-hospital mortality. We used multiple logistic regression for data analysis. In each of the multivariable models, we specified the covariates included time, with 2021 as the reference year), patients’ race/ethnicity (Black, Hispanic, Asian and Pacific Islander, Native American/others, and White [reference]), payer source (Medicare, Medicaid, uninsured, others, and private insurance [reference]), age in years, hospital location (rural, nonrural [reference]), and length of stay (LOS).
Results
Table 1 exhibits the characteristics of the study cohort from 2016 to 2021. The mean age was 75.97 years. Slightly less than half were female, 78.96% were Whites, and 82.59% were Medicare beneficiaries. Approximately 1 in 4 had systolic HF, and the average CHA2D-VASc score was 4.48. Atrial ablation procedure recipients were 0.65%. Figure 1 demonstrates PC utilization trends 2016 to 2021. Palliative care utilization during the 6-year period, steadily and monotonously increased from 9.02% in 2016 to 12.29% in 2021. In addition, 8.88% died in hospital. The average LOS was 7.46 days, and 16.68% were at rural hospitals.
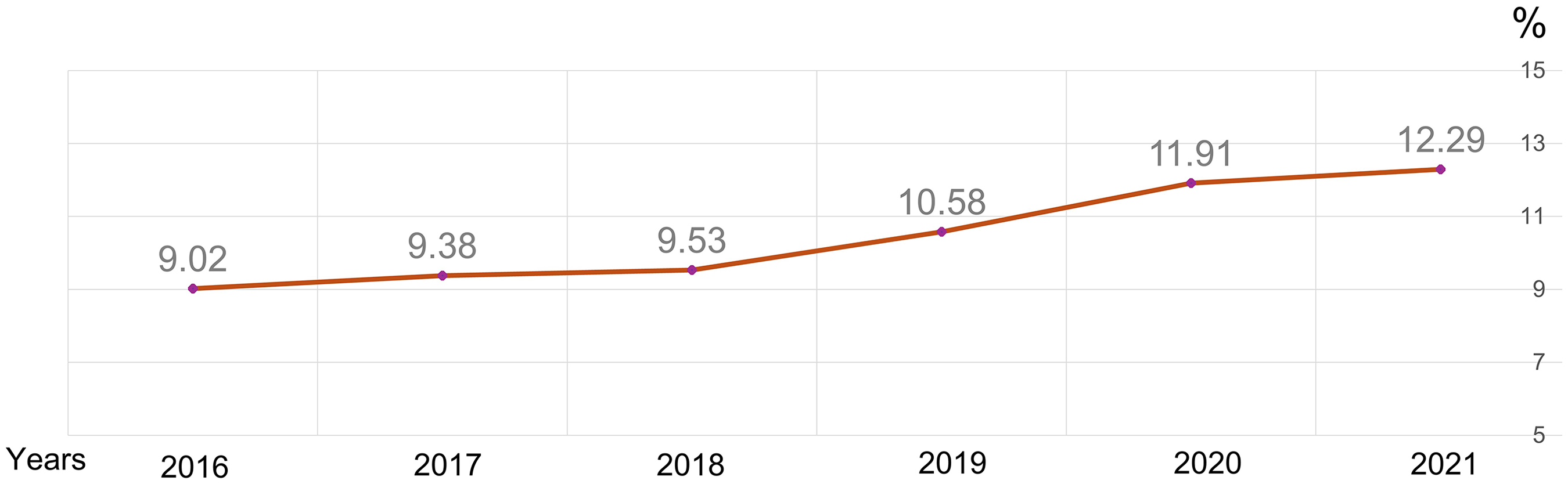
Palliative care trends (%) 2016 to 2021.
Patient and Hospitalization Characteristics in High-Risk Mortality Group of Individuals With Atrial Fibrillation (2016-2021). a
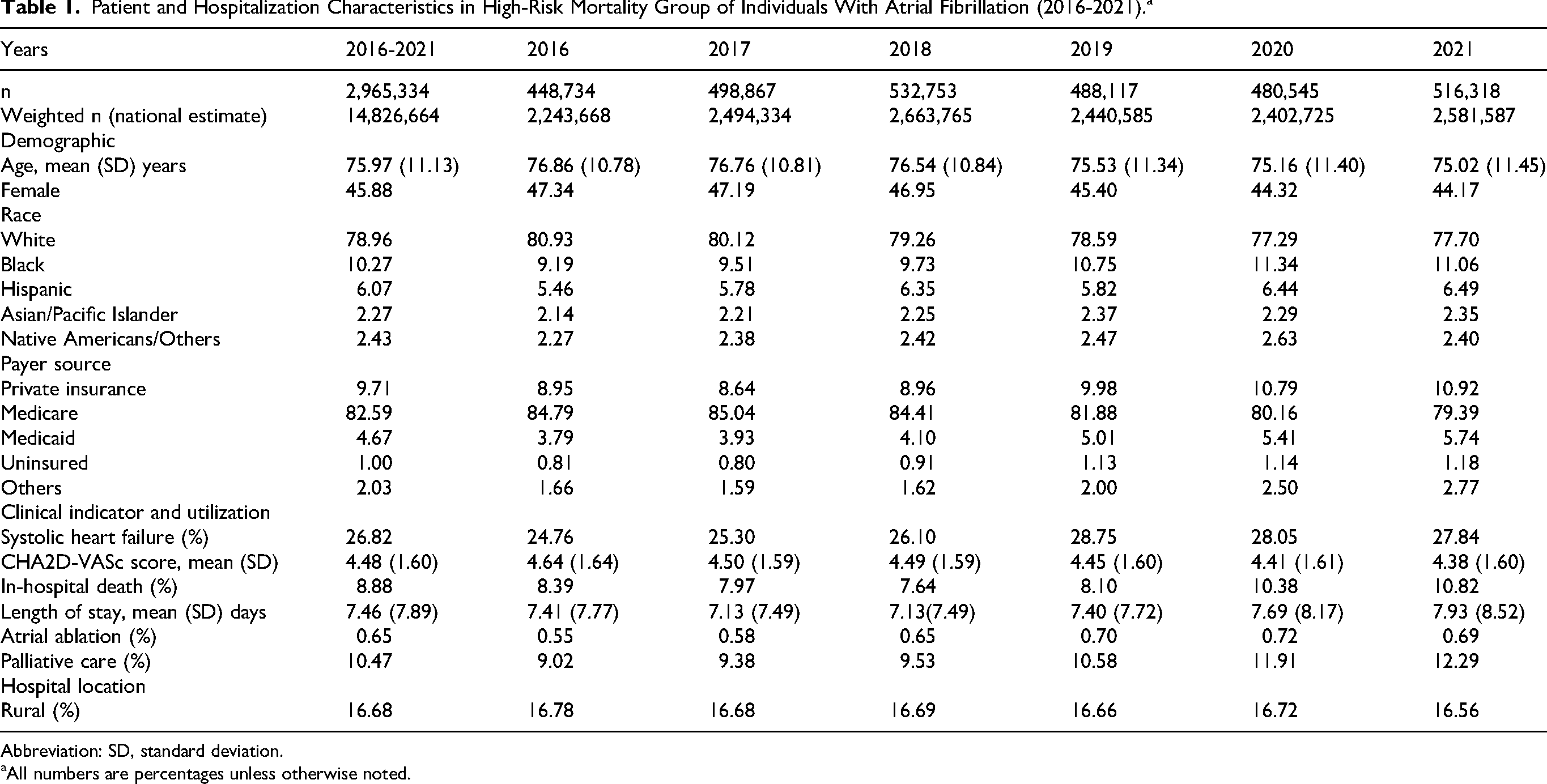
Abbreviation: SD, standard deviation.
All numbers are percentages unless otherwise noted.
Table 2 illustrates multivariate analysis results of factors associated with PC utilization. Age was positively associated with PC utilization, whereas women were more likely to receive PC than their male counterparts (OR =1.204, CI = [1.195-1.214]). Compared to Whites, both Blacks and Hispanics/Latinos were less likely to utilize PC. As compared with private insurance, both Medicare and Medicaid beneficiaries were less likely to utilize PC (OR = 0.736, CI = [0.726-0.746] for Medicare beneficiaries OR = 0.962, CI = [0.939-0.985] for Medicaid beneficiaries), whereas the uninsured were more likely to receive PC (OR = 1.054, CI = [1.011-1.099]). In terms of clinical indicators, a one-point increase in the CHA2-DS2-VASc score was associated with a decline in 12.2% of odds in utilizing PC (OR = 0.878, CI = [0.875-0.881]). Systolic HF was also negatively associated with PC utilization (OR = 0.976, CI = 0.967-0.985). Moreover, AA procedures were much less likely to have PC consultation (OR = 0.287, CI = [0.264-0.313]), and so were patients attending rural hospitals (OR = 0.887, CI = [0.878-0.897]).
Multivariable Analysis Results for Factors Associated With Palliative Care Utilization.
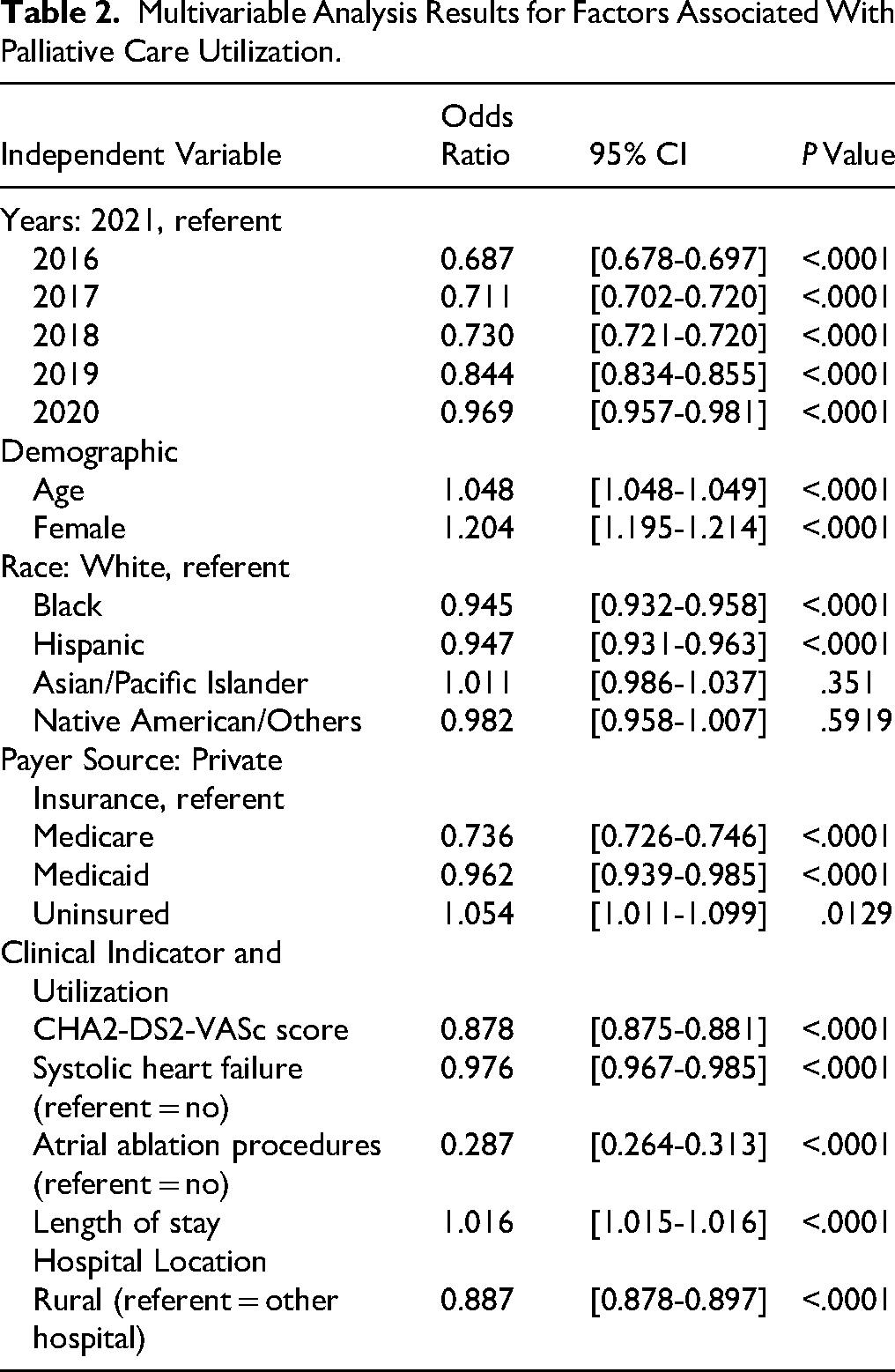
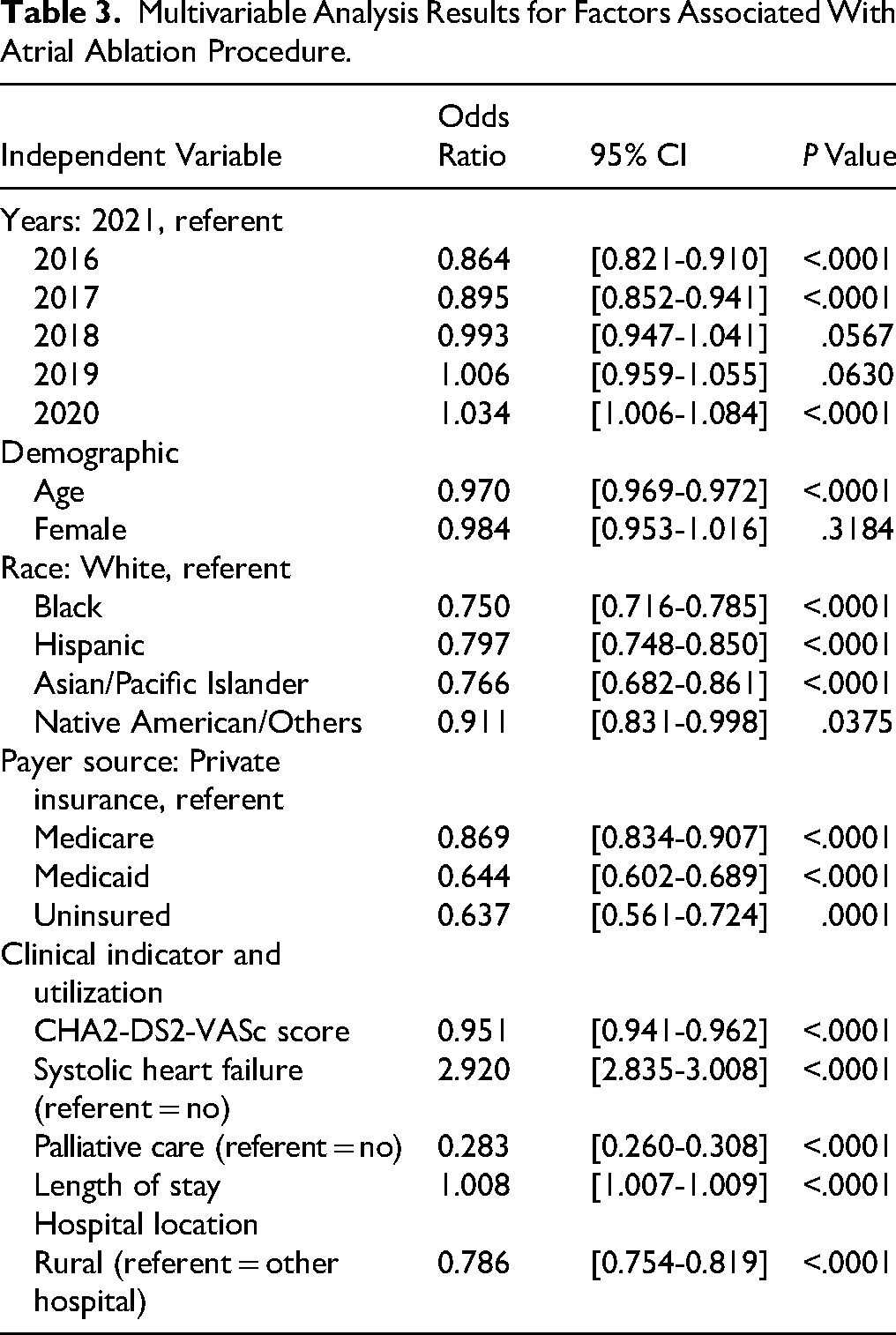
Table 3 presents sociodemographic and clinical factors associated with AA procedure in patients with AF. Age showed a negative association with receipt of AF. Compared to Whites, all racial minorities were less likely to undergo AA procedures, especially for Blacks (OR = 0.750, CI = [0.716-0.785]), Hispanics/Latinos (OR = 0.797, CI = [0.748-0.850]), and Asian/Pacific Islanders (OR = 0.766, CI = [0.682-0.861]). Further, compared with their privately insured counterparts, both Medicaid beneficiaries (OR = 0.644, CI = [0.602-0.689]) and uninsured patients (OR = 0.637, CI = [0.561-0.724]) were less likely to undergo AA procedures. As for clinical indicators, an increase in one point of the CHA2-DS2-VASc score was associated with a decrease in 4.9% of odds in undergoing AA procedures (OR = 0.951, CI = [0.941-0.962]). In contrast, systolic HF was positively associated with increased AA procedures (OR = 2.920, CI = [2.835-3.008]). Furthermore, PC utilization experienced a 71.7% decrease in odds of undergoing AA procedures, compared to their counterparts without utilizing PC (OR = 0.283, CI = [0.260-0.308]).
Multivariable Analysis Results for Factors Associated With Atrial Ablation Procedure.
Discussion
During the 6-year period from 2016 to 2021, the national trends indicated that the PC utilization among the high-risk mortality group with AF in the U.S. hospitals steadily increased but remained about 10%. Once PC was chosen, the probability of choosing AA procedures was reduced by approximately 75%, and vice versa; Once AA procedures were chosen, the probability of choosing PC was reduced by approximately 75%. These findings indicated that healthcare providers’ tendency of favoring the status quo and current practices rather than initiating change. 22 The lack of cardiovascular workforce training opportunities is a plausible explanation for the discrete choice patterns of AA procedures and PC. According to the nationwide cardiovascular fellowship program survey, most respondents reported dissatisfaction with the quantity (62%) or quality (59%) of the PC education in cardiovascular fellowship training. Indeed, it is challenging to implement formal PC curricula in cardiology training programs. 23 Integrating PC as an essential part of cardiovascular disease fellowship curriculum competencies would enhance cardiovascular experts’ capacity of caring for high-risk mortality AF patients with more patient-centered decision-making. The impact of PC training for the cardiovascular workforce may lead to greater distribution of PC benefits to the AF patients with high-risk mortality, including but not limited to the following: proactive symptom management, goals of care establishment, and end-of-life preparation. Frustration from patients and caregivers with critically ill conditions occasionally stems from sudden shifts in goals of care from life-sustaining treatment to PC. 10 This challenge is more common in racial minorities with limited awareness of PC and reluctance to discuss end of life. 24 In this study, those with systolic HF were more likely to receive AA procedures and were less likely to utilize PC. Those with higher CHA₂DS₂-VASc were less likely to receive AA procedures. This can be interpreted as conservative management is more favored for those with a higher probability of stroke.
While AF is associated with multiple comorbidities, care planning remains inaccessible for hospitalized AF patients. An array of disparity challenges plays a substantial role in care variation access. Evidence in this study indicates differences in the use of utilizing PC among Blacks and Hispanics/Latinos, Medicare and Medicaid beneficiaries, and rural residents. Explanation for these findings remains incompletely understood, but several associations can be considered. Between 2016 and 2021, many AA procedures or treatment strategies were changed, thus the above outcomes might have been improved.
Health Disparities in PC
Palliative care misconceptions are evident, with only 28% of the U.S. population being familiar with care management. 25 Notably, ethnic and racial patients, particularly Blacks and Hispanics/Latinos, were less likely to consult for PC which was demonstrated in this study. This may be due to less awareness of PC and fear discussing end-of-life treatments among minorities. 24 Research mentioned that 26 PC was the least recognized type of care among Hispanics and Blacks, while factors such as age, education, and income were significantly associated with recognition of the care management. Additionally, language barriers, cultural differences, and other socioeconomic barriers may play a role in the lower PC utilization among minorities. 27
Disparities in payor sources also show variations in PC utilization in this study, while it indicates lower use among Medicare and Medicaid beneficiaries, a surprisingly higher PC consultation is observed among uninsured AF patients. This could be attributed to the need for PC rather than initiating life-sustaining treatments, which are considered more expensive for uninsured patients. In contrast, reimbursement restrictions among providers show evidence of limited discussion of advance care planning for Medicare beneficiaries. 28 This illustrates the barriers in continuing care, especially PC among Medicare beneficiaries with advanced illnesses.
Furthermore, disproportions of PC utilization were also associated with area location in this study, showing a lower PC consultation in rural hospitals. Research showed that most rural residents were less likely to understand the benefits of PC due to insufficient resources in the area, while others viewed PC as “dying care” which is only utilized at the end-of-life stage. 29 Moreover, a study using a community-based participatory research approach, identified PC misconceptions, untrained providers, late involvement/education, financial constraints, cultural differences, and geographic location as barrier to lower rates of PC services in rural areas. 30 This may explain why patients in rural areas received lower PC than those in urban areas.
Besides variations in consultation for PC among AF patients, receiving AA procedure also shows inconsistencies. The findings in this study reveal lower ablation procedures among racial and ethnic patients, Medicaid and uninsured individuals, and residents in rural areas compared to their counterparts. Explanations for these findings are mentioned below.
Atrial Ablation Procedure Disparities
This study depicts all ethnic and racial minorities, especially Blacks, Hispanics/Latinos, and Asian/Pacific Islanders, were associated with decreased AA procedures compared to their White counterparts, showing disparities in accessing cardiovascular care planning. This aligns with the previous literature, 31 indicating that Blacks and Hispanics were less likely to receive AA procedures for AF, compared to Whites; however, the study has not mentioned any Asian peers. Clinician biases for preferences and advocacy for rhythm control are pointed out as discrepancies among ethnic and racial AF minorities. 32 Other factors include patient preferences, biases, insufficient health sources, and other socioeconomic-related barriers. 33
Additionally, this study illustrated lower AA procedures among uninsured and Medicaid beneficiaries than those with private insurance. Similarly, a national study of 397,161 hospitalized AF patients showed favor of AA procedures among privately insured individuals compared to those with other types of insurance, and they were more likely to be younger, male, and White. 34 Another study suggests that uninsured patients receiving lower AA procedures may reflect on their inability to pay while lower fee reimbursement from federally funded care plans is associated with physicians’ reluctant to offer the procedures. 35 This challenge generates diminished health outcomes among AF patients, particularly those with a lower chance of receiving ablation procedures, mainly, for Medicaid beneficiaries and uninsured individuals.
The underutilization of AA procedures in rural hospitals was also evident in this study, showing variations in accessing the procedure in isolated areas. This may be explained by inadequate AF care planning in rural areas and issues with expenses, transportation, quality of care, physician experience, and other associated barriers. 36 Furthermore, a cross-sectional examination of AF patients comparing in-hospital mortality (urban vs rural) reveals, that besides patient's characteristics, practice patterns including catheter ablation were different across urban and rural hospitals. 37 This shows that AF patients who received lower access to care were more likely to reside in rural areas and were more at risk of mortality.
The findings of this study highlight potential efforts to enhance PC benefits in cardiology to benefit patients with AA procedures that are useful as the first-line treatment in symptomatic and recurrent AF to aim to improve prognosis in those with HF. 38 Additionally, incentives motivate providers to dedicate additional time and effort to talk with patients and their conditions. Furthermore, the significance of medical education and cardiovascular fellowship on PC increases providers’ awareness of care management; thus, discussion of symptom relief, support, and end-of-life preparation will be more evident towards patients with serious illnesses.
Call to Actions in Health Policy and Clinical Education
In real-world hospitalized AF patients care, not only medical conditions (eg, systolic HF) but also geriatric syndromes (cognitive impairment, falls) and advance care planning are essential competencies and training curriculum. Interprofessional and simulation curriculum is urgently warranted for hospital workforce, particularly, cardiovascular workforce. American Heart Association Certified Care for palliative and hospice HF program is an example of key care standards and training resources for cardiovascular workforce. 39 Telehealth can enhance access to advance care planning for those with advanced HF as well as PC utilization, particularly, for underserved communities and rural locations. 40
Limitations
Although our large sample size provides potential benefits in the analysis of the relationship between PC and AA, several limitations are noted. First, we relied on ICD-10-CM/PCS that may not provide detailed clinical information of high-risk AF patients, highlighting the need to examine patients’ EHR information to generate more comprehensive health details. For example, early or integrated palliative interventions could not be differentiated from terminal care. Second, we cannot track a single patient who has multiple hospital admissions. Third, using the CHA₂DS₂-VASc score as a proxy for mortality or disease severity was limited for interpreting analysis results, as the CHA₂DS₂-VASc score is the stroke risk predictor among patients with AF. Despite these limitations, we believe that this study will provide contributions for health policy enhancements, better clinical approaches, and disparity investigations.
Conclusion
This study provides valuable insights into the association between PC utilization and AA procedures among high-risk AF patients in U.S. hospitals. Palliative care utilization steadily increased among AF patients, yet when combined with AA procedures, they remain underutilized. Health disparities play a significant role in PC utilization and AA procedures, making it a barrier for marginalized patients to access care planning. Further efforts are imperative to expand these 2 combined care plans and improve the quality of life of these patient groups.
Supplemental Material
sj-docx-1-pal-10.1177_08258597251372721 - Supplemental material for Association of Atrial Ablation Procedure and Palliative Care for High-Risk Mortality Group With Atrial Fibrillation in U.S. Hospitals: 2016-2021 National Inpatient Sample Analysis
Supplemental material, sj-docx-1-pal-10.1177_08258597251372721 for Association of Atrial Ablation Procedure and Palliative Care for High-Risk Mortality Group With Atrial Fibrillation in U.S. Hospitals: 2016-2021 National Inpatient Sample Analysis by Fye Angelyn Pinera, Pearl Angela Pinera, Pearl Kim, Leora Frimer, Pengfeng Jin, Gregory-Thoams Castaneda Stanger, Iuilia Ianitoaia-Chaudhry, Ronald Tan, Faizan Sheraz, Sebin Park, Hayden Leung, Ji Won Yoo and Jay J. Shen in Journal of Palliative Care
Footnotes
Authors’ Note
Study's contribution to the scientific literature: Palliative care utilization increased from 2016 to 2021 among high-risk group with atrial fibrillation (AA) in U.S. hospitals. Palliative care utilization and atrial ablation procedure were not provided harmoniously for high-risk mortality group. Health disparities of PC utilization and AA procedure were identified in the populations of racial minorities and rural residents.
Study's relation to the previously published work: Recently, atrial fibrillation has contributed to an increase in cardiovascular deaths in the U.S. Palliative care and atrial ablation procedure can elevate quality of life as high-risk AF patients are associated with multiple comorbidities. However, combined management of PC and AA among high-risk mortality groups with AF is largely unexplored.
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board at the University of Nevada, Las Vegas (no. IRB no. 1098939-3) with the need for written informed consent waived.
Author Contributions
Conceptualization—Pearl Kim, Jay J. Shen. Data curation—Jay J. Shen. Formal analysis—Fye Angelyn Pinera, Jay J. Shen. Funding acquisition—Ji Won Yoo. Investigation—Fye Angelyn Pinera, Jay J. Shen. Methodology—Leora Frimer, Pengfeng Jin, Gregory-Thomas Castaneda Stanger. Project administration—Iulia Ioanitoaia-Chaudhry, Roland Tan, Faizan Sheraz, Sebin Park, Hayden Leung. Resources—Jay J. Shen. Software—Jay J. Shen. Supervision—Ji Won Yoo, Jay J. Shen. Validation—Fye Angelyn Pinera, Jay J. Shen. Visualization—Fye Angelyn Pinera, Sebin Park, Hayden Leung, Ji Won Yoo. Writing (original draft)—Fye Angelyn Pinera, Pearl Angela Pinera, Pearl Kim, Leora Frimer, Pengfeng Jin, Gregory-Thomas Castaneda Stanger, Iulia Ioanitoaia-Chaudhry, Ronald Tan, Faizan Sheraz, Ji Won Yoo, Jay J. Shen.
Funding
The author Ji Won Yoo received U.S. Department of Health and Human Services, Bureau of Health Workforce Geriatric Workforce Enhancement Program #U1QHP53032 for this work. Funding sponsor does not play a role in study design, analysis and interpretation of results.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data are available for purchase from the Healthcare Cost Utilization Project (HCUP) National Inpatient Sample between January 2016 and December 2021. Others can access the data by contacting HCUP through Central Distributor (![]() .) and purchasing the relevant years of data. This is how the authors accessed these data; the authors did not have any special access privileges others would not have.
.) and purchasing the relevant years of data. This is how the authors accessed these data; the authors did not have any special access privileges others would not have.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.