
Abstract
Most mental disorders often onset during the adolescent years, providing opportunities for educators, health care providers, and related stakeholders to work collaboratively in addressing adolescent mental health care needs. This report describes early implementations of various components of the School-Based Pathway to Care Model currently applied in Canada, identifies lessons learned, and suggests future directions. The School-Based Pathway to Care Model engages students, teachers, student service providers, parents/families, health care providers, and the wider community through various training programs and both formal and informal linkages between the school, community, and health providers. Preliminary evaluation of the model in whole and in part shows promising outcomes for its application in secondary schools within the wider framework of enhancing system capacity for addressing mental health needs of students. Future focus should be directed towards more rigorous research on the model and its various components.
Approximately 70% of mental disorders can be diagnosed before the age of 25 years (American Psychiatric Association, 2000; Kessler et al., 2005; O’Connell, Boat, & Warner, 2009), the majority of which are mild to moderate in intensity (Kessler et al., 2012). The adolescent years are a period of high risk for the onset of mental disorders (Kessler et al., 2005; Lancet Global Mental Health Group et al., 2007), providing an opportunity for possible preventive interventions and early identification of mental disorders that can lead to appropriate diagnosis and effective treatment, thus potentially improving both short- and long-term social, academic, economic, and health outcomes (Kessler, Foster, Saunders, & Stang, 1995; O’Connell et al., 2009).
Some researchers and practitioners in both education and health systems have realized that cross-sector collaboration is key to improve understanding about mental health/mental disorders amongst youth and educators, help change stigmatizing attitudes towards mental illness, enhance health and help-seeking behaviours, and improve access to mental health care for adolescents (Adelman, 2006; Kutcher, Hampton, & Wilson, 2010). Various approaches have been advanced to address aspects of this issue in many developed countries, such as the School-Based Health Centres and System of Care in the United States (Aviles, 2006; UCLA School Mental Health Project, Center for Mental Health in Schools, 2009), the Social Emotional Learning initiative in the United Kingdom (Department for Children, Schools and Families, UK, 2009), the Mentally Healthy School initiative in New Zealand (Ministry of Health, New Zealand, 2003), and the whole school approach Mind Matters in Australia (Wyn, Cahill, Holdsworth, Rowling, & Carson, 2000).
In Canada, while a number of initiatives have been created to promote interagency collaboration to address youth mental health needs in a number of provinces, such as the Kids and Learning First strategy in Nova Scotia (Nova Scotia Department of Education, 2012) and the School Mental Health ASSIST initiative in Ontario (http://smh-assist.ca/), there is an absence of a national framework to systematically conceptualize roles of different sectors and develop strategies and practical guidance to advance this approach (Wei, Kutcher, & Szumilas, 2011). The importance of this need has recently been acknowledged in the Evergreen document, the national child and youth mental health framework created for the Mental Health Commission of Canada under the auspices of the Child and Youth Advisory Committee of the Mental Health Commission of Canada (Kutcher & McLuckie, 2010). In this document, both the importance of school mental health and the necessity of linking school mental health initiatives with the most appropriate health providers (primary care and specialty mental health services) are highlighted. Similarly, the recently released report of the School-Based Mental Health and Substance Abuse Consortium Knowledge Translation and Review Team (2012) and various policy experts (Kutcher, Davidson, & Manion, 2009; Kutcher et al., 2010) have noted the need for a comprehensive and integrated approach in which schools and health providers become part of the pathway into care and through care for young people with a mental disorder. One challenge to this innovation has been the need for a model that demonstrates how this integration can be achieved in different settings and across different social, economic, and cultural domains. The School-Based Pathway to Care Model (the Model; details below) provides a framework that meets this need, and it is currently being applied in whole or in part in numerous settings across Canada and internationally.
This article reports on an early implementation of the School-Based Pathway to Care Model (access to the full evaluation report available at: http://teenmentalhealth.org/resources/entries/mental-health-integration-and-navigation-mh-in-evaluation-report) and describes some of the applications of various individual model components that are being undertaken across Canada, provides lessons learned from these, and suggests future directions.
School-Based Pathway to Care Model and Its Components
The School-Based Pathway to Care model (Figure 1) was first created in 2009 to address adolescent mental health through facilitating an holistic collaborative framework including educators and health care providers within the context of a secondary school setting (Wei et al., 2011). It addresses pathways into and through the most appropriate mental health care as well as the linkages amongst various components necessary for successful implementation of that pathway by identifying key stakeholders and describing key functional components, such as capacity building through training, and integration of health and human services providers both within and external to the school setting. Key stakeholders identified include the following: students, teachers, student services providers (e.g., guidance counsellors, school psychologists, school social workers, and school health centre staff), school administrators, parents/families, and health providers (primary care and specialty mental health services). Capacity building through training includes the following: mental health literacy for students and teachers (the Mental Health and High Schools Curriculum Guide (the Mental Health Curriculum) and teachers training program (Sun Life Financial Chair in Adolescent Mental Health & Canadian Mental Health Association, 2007), early identification of, internal and secondary triage and ongoing student support for youth with mental disorders (the “go-to” educator training program), and on-site or community-delivered evidence-based mental health interventions (primary care training programs).
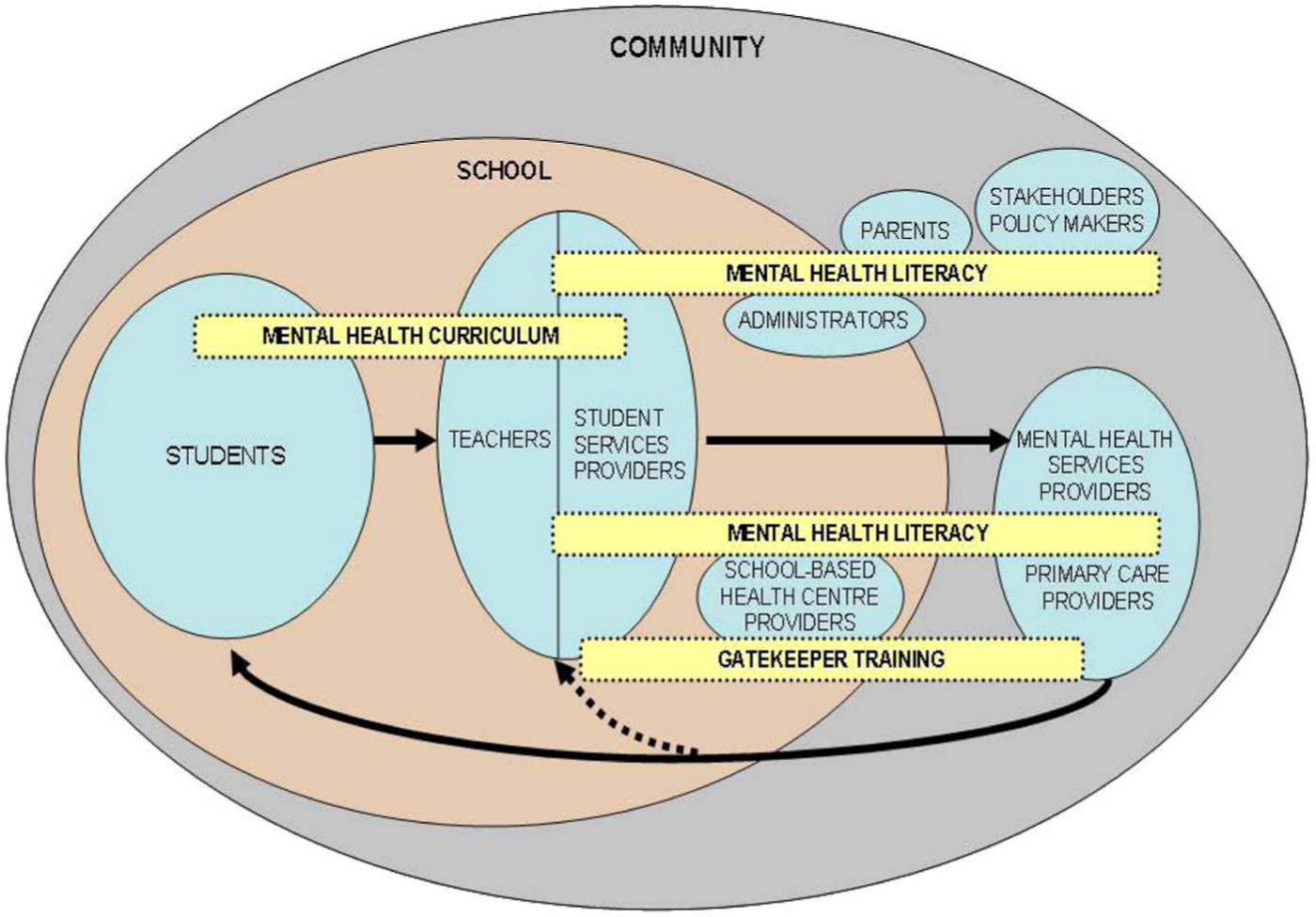
School-Based Pathway to Care Model.
Formal and informal linkages into and through the pathway to care are created by application of the model components with key stakeholders participating in collaborative training experiences. For example, the “go to educator” training is primarily directed towards teachers and other school staff who students usually “go to” when they have a problem. It helps teachers better understand the mental health and common mental disorders in adolescents, assists in the identification of youth at high risk for having a mental disorder, provides information on useful support strategies (and identifies limits of teacher responsibilities), and reinforces within school mechanisms for triage and student support. However, joining these sessions are student support staff (e.g., guidance counsellors, school psychologists) and local health and human services providers (e.g., mental health and addictions program staff, primary care clinic staff). This common training reinforces common understanding and communication and enhances or may create cross-jurisdictional linkages that then can better facilitate the progress of an identified student into and through care (including return to school).
Experiences of the School-Based Pathways to Care Model
This model, although heuristically appealing, must stand the test of empirical validation through both quantitative and qualitative evaluations. Below, we describe various components of the development of this validation process, demonstrating a hierarchical approach to its evaluation and including preliminary research conducted by the developers of the model and research conducted by independent scholars.
Pilot of the Model in Whole With a Local Secondary School
Participants and Process
The model was applied and evaluated at a rural Nova Scotia high school under the direction of an implementation team including the school principal, school guidance counsellor, Student Services staff from the Department of Education, and the Schools Plus program coordinator by the knowledge translation team (the Team) that developed this model. All Grade 10 students (n = 74) and classroom teachers (n = 6) participated in the Mental Health Curriculum component. The “go-to” educator training included teachers, guidance counsellors, school psychologists, and local mental health/addictions and human services providers. Primary care involvement was linked through the local District Health Authority.
Model Component 1—Mental health literacy for classroom teachers and students
Mental health literacy refers to the appropriate understanding of mental health and mental disorders, knowledge and skills about stigma reduction, and enhancement of appropriate help-seeking behaviours. Mental health literacy (addressed through the Mental Health Curriculum and training programs) is foundational to the model. The Mental Health Curriculum (Sun Life Financial Chair in Adolescent Mental Health & Canadian Mental Health Association, 2007) was applied by six Grade 10 classroom teachers. It consists of a teacher self-study package and six modules for students. The self-study package provides basic information about mental health/mental disorders contextualized for the school setting. The six modules for students address the following: (a) stigma, (b) understanding mental health and mental illness, (c) specific mental disorders typically onsetting during adolescence, (d) lived experiences of mental illness, (e) help-seeking and support, and (f) the importance of positive mental health.
To facilitate the teaching of the Mental Health Curriculum, the Team designed an accompanying training program for teachers. The training was held in February 2010 for all participating teachers. This included an overview of mental health and mental disorders contextualized for the school setting as well as a review of the Mental Health Curriculum, with supplementary educational resources and teaching strategies. Following the classroom teacher training, teachers prepared class materials together and taught them in groups of two teachers with each group teaching two modules. The Mental Health Curriculum was delivered over a period of 1 week, taking approximately 8 hours total duration.
Model Component 2—“Go-to” educator training
“Go-to” educators are school staff (such as teachers, coaches, and guidance counsellors), known to principals, whom students frequently go to when they need help or advice. As such they are uniquely placed to identify students at high risk for having mental disorders if they are trained to do so. Based on a needs identification evaluation conducted by the Team, a “go-to” educator training program was created to address the understanding of mental health and mental disorders; identification of mental disorders, stigma, evidence informed support; professional and institutional responsibilities and their limits; triage principles and processes; and linkage to local mental health care providers (specialty services and primary care). The training was delivered in March 2010 to a group of “go-to” educators plus local mental health/addictions and community human services providers.
Model Component 3—Parents/family engagement
Strategies to involve parents and families were discussed throughout the process. The school suggested that a combination of online information and face-to-face information sessions as a way to improve the understanding of mental health by parents and families. The Team proposed providing information on the school website, by emailing fact sheets to parents, along with three information sessions at three sites within the school’s catchment area. The Team designed all the materials needed for the school to upload on to their website; however, the information sessions were not delivered due to logistical complications, especially the lack of transport for parents to attend the sessions.
Model Component 4—Primary care team mental health training
General practitioners and other primary care providers are often a youth’s first health contact, and therefore it is essential that they are able to properly identify, diagnose, and treat many of the common mild to moderate mental disorders in young people. Working together with the school, the District Health Authority invited general practitioners and other primary care providers to participate. The Team conducted a needs assessment with eight general practitioners and a paediatrician in January 2010, who identified training needs in five areas: Depression, Social Anxiety Disorder, Panic Disorder, Attention Deficit Disorder, and Obsessive Compulsive Disorder (OCD). On review, OCD was considered to be more suitable for direct referral to mental health services and a training program addressing the other domains was created. However, due to changes in the administrative structure of the District Health Authority, this program could not be delivered.
Model Component 5—Establishment of the pathway into care and referral mechanisms
“Go-to” educators and local mental health care providers were brought together at the “go-to” training to identify strategies to facilitate linkages between the school and providers. An in-school triage process for identified students was created and a single point of referral contact between the school and mental health team was determined. A method of tracking and assessing types of referrals and an ongoing support feedback loop was created. Issues pertaining to confidentiality were raised and clarified.
Program Evaluation
Both quantitative and qualitative techniques were used in the evaluation. Students and classroom teachers were administered the same questionnaire before (t0) and after (t1) the training, and at a 3-month follow-up (t2). “Go-to” educators were tested with another questionnaire matching the training content before (t0) and after (t1) the training, and at a 3-month follow-up (t2). The evaluation of referral process was documented on forms created for this purpose, tracking the number of students through the referral process and documenting what mental health care needs are were identified. Two focus groups (students and teachers, separately) were conducted to gather feedback on the interventions.
Student quantitative data were imported into statistical software (STATA) for analysis. Student mean scores were calculated and compared using t test. Mean scores of classroom teachers and go-to educators were also computed but not compared with t tests due to the limited number of participants (n = 6). Qualitative data were analyzed using a grounded theory approach to identify relevant themes. When completed, the program evaluation was posted in the public domain as noted above.
Results
Students’ mental health knowledge increased significantly (M = 59.3 [t0]; M = 72.2 [t1]; p < .001), immediately after the curriculum delivery, but this was not retained at the 3-month point (M = 57.8; Figure 2). Both teachers’ (M = 76, SD = 7.9 [t0]; M = 88, SD = 3.6 [t1]; M = 89, SD = 8.4 [t2]) and “go-to” educators’ (M = 77, SD = 10.8 [t0]; M = 87, SD = 6.7 [t1]; M = 81, SD = 12.9 [t2]) knowledge increased significantly and persisted over the 3-month period.
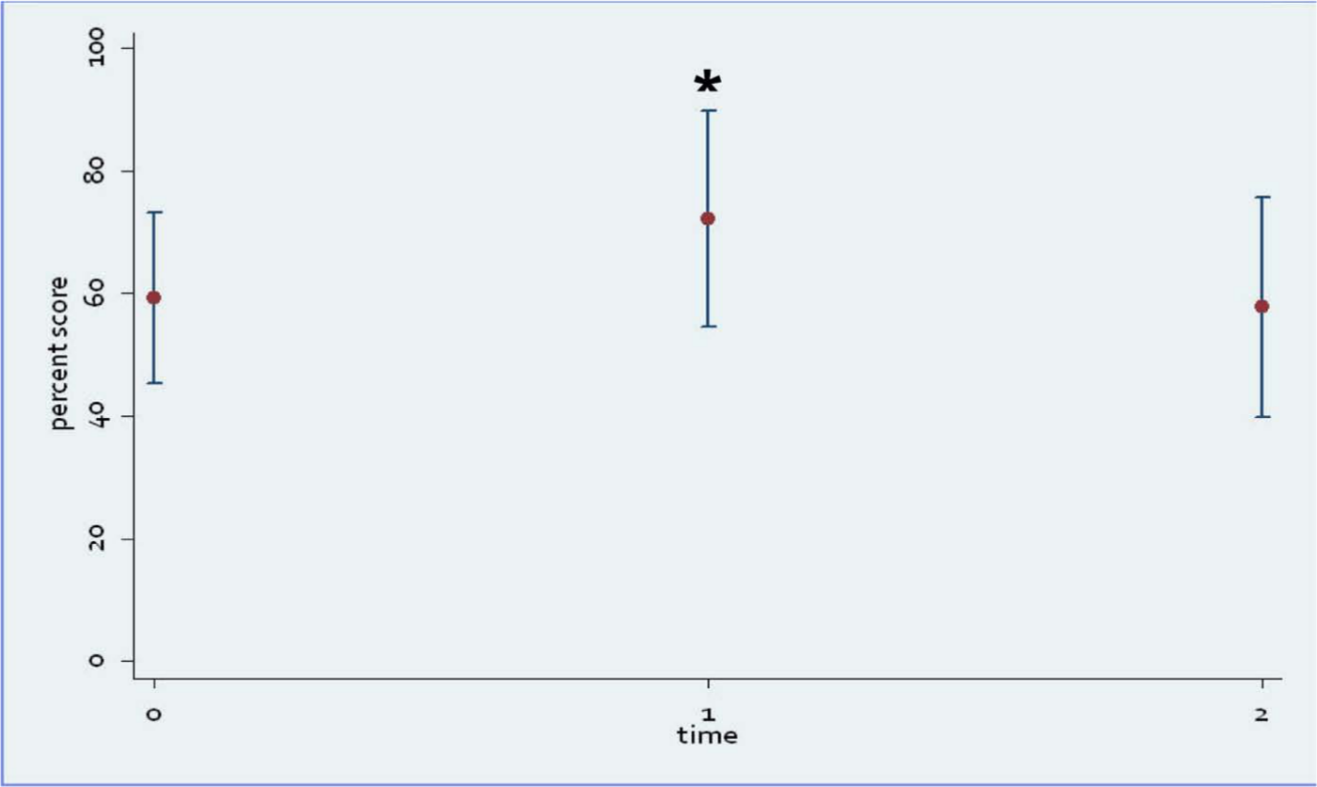
Change in students’ score on knowledge test over time (pilot of the whole model)
Student focus group discussions generated a number of themes. First, students reported feeling more comfortable responding to people with mental illnesses after taking the Mental Health Curriculum. Second, they suggested mental health training should be provided to parents and teachers since they often seek help from them. Third, they wanted more digital resources and interactive classroom activities in the Curriculum. Fourth, they reinforced the need for integration of the material into usual educational structures, such as examinations. Reports suggested that since they were not going to be examined on the material prior to the final post-test, they did not approach the Mental Health Curriculum with the same diligence as subjects in which examinations were applied.
Classroom teachers identified three areas for improvement: enhancement of education about the brain, more integration of local community resources in classroom presentations, and the clarification of policies regarding parental consent and confidentiality. “Go-to” educators requested more in-depth training pertaining to mental health services system navigation and additional mental health resource toolkits. Both classroom teachers and “go-to” educators reported that the model helped integrate the school with the local mental health care provider to better meet students’ mental health care needs.
The process evaluation indicated that, compared with the previous year, the number of referrals did not significantly increase over the project period (December 2009-June 2010), as some health providers expected. However, the quality of the referrals increased (referrals were judged to be “more appropriate for mental health services”), and both school and mental health clinic staff reported improved working relationships. Concerns about consent and the lack of a common consent form across education/health systems were raised and brought to senior administrative levels in the Provincial Departments of Health and Education for clarification and address. This led to clarification of misperceptions related to consent held by educators and the creation of a process to develop a common consent form to be used across Departments.
Further Implementations of Individual Model Components
Model Components 1 and 2—The Mental Health Curriculum and “Go-To” Educator Training
Based on the above experience, the Team, in collaboration with various educators and health providers, refined the model components and made them available for further application, in whole (the entire model) or in part (portions of the model of greatest interest to specific educational or health settings). This approach is consistent with the flexible, locally adaptable nature of the model in which the pathway into and through care is built on available resources and modified to meet local realities, including readiness for application and availability of resources.
In one application (February 2012), two Nova Scotia secondary schools (one English and one French) delivered Model Components 1 and 2. All Grade 10 classroom teachers (n = 17) participated in the Mental Health Curriculum training, which had been enhanced with additional supplementary online resources. The Mental Health Curriculum was then delivered in both schools (n = 35 students in English school; n = 41 students in French school) over the course of one semester. “Go-to” educator (n = 12) training was also provided as previously described. A program evaluation was conducted and results were posted at http://teenmentalhealth.org/images/resources/TCRSB_curriculum_and_go-to_educator_training_report_Jan_20_2012.pdf. Participant knowledge was measured using pre- and post-tests. Data were analysed using SPSS 17 for statistical analyses (t test). Results demonstrated a statistically significant increase of knowledge in students in both the English school (M = 50.6, SD = 13.8 [t0]; M = 57.2, SD = 10.5 [t1]; p < .05) and the French school (M = 52.4, SD = 15.5 [t0]; M = 60, SD = 14.9 [t1]; p < .01). Similar results were found amongst teachers (M = 80.3, SD = 11.5 [t0]; M = 85.9, SD = 8.7 [t1]; p < .10) and “go-to” educators (M = 74, SD = 8.3 [t0]; M = 86, SD = 6.7 [t1]; p < .005). Focus groups were also held with all participants and generated two key themes. One theme was that collaboration between the education and health systems is the key to success, and the other theme was that multimedia and interactive activities are important to enhance learning outcomes. Based on the success of this project, the local school board where the two schools are situated decided to roll out the Mental Health Curriculum and “go-to” educator training across all schools in the board in 2012.
Model Component 1, the Mental Health Curriculum and its accompanying teacher training, is also undergoing a large independent randomized controlled trial in the province of Ontario to evaluate its effectiveness in knowledge acquisition, attitude change, and help-seeking behaviours, involving more than 40 secondary schools. Another large-scale cross-sectional research study is being conducted in partnership amongst the Team, a comprehensive mental health services provider, and four school boards in Ontario.
Model Component 3—Parent/Family Involvement
Informed by these experiences and with the input of the educator advisory committee to the Team, new effects to actively engage parents were initiated. One approach that was developed is the “Junior High Chat” initiative where parents and teachers from local junior high schools (Grades 7-9) meet with Team members to discuss any parent driven concerns related to adolescent development. This has received substantial positive feedback from parents, principals, and school boards alike. An evaluation format for this initiative is being planned. Additionally, the Team has developed two brochures, Parenting Your Teens and Teening Your Parents (see www.teenmentalhealth.org), to promote better understanding of adolescent development and mental disorders for parents and youth and to help facilitate discussion of these topics. Evaluation formats for this approach are currently being considered.
Model Component 4—Primary Care Training
Modifications to the primary care common adolescent mental disorders training program were made to create a daylong session for all primary care team providers. Ongoing evaluation of this program is currently underway in two sites in Ontario. A further development from this approach has been the creation of the College of Family Physicians certified CME program developed by the Team and the British Columbia Medical Association (PSP), which is now in the process of extensive field evaluations.
Discussion and Lessons Learned
Experiences in the application and ongoing development of the School-Based Pathway to Care Model indicate that it is possible to implement the model as a whole or to apply individual components that serve the goals of each component within the wider framework of enhancing system capacity for addressing mental health care needs of secondary school students. This dialectic or praxis process has provided rich program evaluation data that have been used to improve the components of the model and to inform approaches to its application. Following are key lessons learned.
First, it is necessary to identify local champions within education and health sectors (primary care and mental health) that can help apply the model and mould it to fit local realities. These champions also serve to help overcome obstacles within and across systems. These champions ideally could be brought together as an action committee to develop, apply, and evaluate the model as well as engaging key players from the different sectors involved. The “go-to” educator training sessions provide an ideal opportunity for these champions to engage their representative communities and to begin to establish or enhance linkages between schools and health providers: both formal and informal. These linkages require both personal and system-level participation to help establish and reinforce their application. The combination of formal (system administrative structures) with informal (combined training) approaches to integration seem to be a key component for success.
Second, there is no “best” application of the model. Its flexibility allows locations to choose the components that they wish to or have the ability to apply. Additional components can be applied as local opportunities permit. For example, although primary care capacity in diagnosis and treatment of adolescent mental disorders is part of the model, two of the jurisdictions were not at the point to develop this component of their health care delivery system. In another setting, this was able to proceed because a commitment had been made to address this issue. This feature differentiates the model from programs that demand a high degree of fidelity for application. The flexible nature of the model and its ability to show good outcomes without demanding fidelity are particular strengths, as this allows the model to meet the needs of people and settings rather than the other way around.
Third, supplementary mental health resources available at a single point of contact are useful to teachers applying for the Mental Health Curriculum. As a result of these lessons, the Team has established a wealth of such resources, both on its own website (www.teenmentalhealth.org) and in collaboration with Taking It Global (www.tig.com), an international educational resource. Embedded in the (teenmentalhealth.org) website is the ongoing development of a repository hosting mental health resources screened and validated to meet criteria for quality and classroom utility for teachers. An online discussion forum for teachers is also soon being added to this online resources repository.
Fourth, train-the-trainer and online learning approaches will be necessary for the broader dissemination of the model and its various components. The Team is now responding to this need by building e-learning modules on their website (www.teenmentalhealth.org) and creating train-the-trainer programs.
Fifth, at the systems level, it is important that both Components 1 and 2 of the model be addressed concurrently. Putting the Mental Health Curriculum into place without implementing the in-school capacity to recognize and respond to students with mental disorders is unfair to students, schools, and providers alike. School boards are thus encouraged to simultaneously address both components. As an example of this understanding, the new educational strategy for the Province of Nova Scotia, Kids and Learning First (Nova Scotia Department of Education, 2012), has incorporated this lesson into its approach in addressing school mental health in the Province.
Meanwhile, we note that there are some challenges that need to be further addressed so that there can be improvement in the model’s application. For instance, it remains challenging to link primary care with the school system, although this component has shown early promise in British Columbia. To change current primary care practice and to better integrate mental health care into primary care will require substantial support from policy makers and related stakeholders. Perhaps the approach currently being applied in parts of British Columbia will inform responsible parties as to the value of and need for this approach once the program evaluation has been completed and can be disseminated. Another major issue is that of measurement of mental health literacy for each group of the participants—students, teachers, student services providers, health providers, and so on—needs to be refined. The development of this part of the school mental health field is in its infancy and members of the Team have identified this as an upcoming priority. Lastly, although work to date has demonstrated encouraging results, more rigorous research has yet to be conducted to provide stronger evidence for both short- and long-term outcomes of the model application.
Nonetheless, and with the above caveats considered, we feel that there is reasonable comfort in the data currently available to support the implementation of the School-Based Pathway to Care Model, especially its tested components, such as the Mental Health Curriculum, its companion teachers training program, and the “Go-to Educator” training program. To our knowledge, the Mental Health Curriculum is the only evidence-based high-school mental health curriculum available globally, and the approach that is applied within the School-Based Pathway to Care Model is consistent with national mental health policy considerations such as they have been articulated in both Evergreen (Kutcher & McLuckie, 2010) and the Mental Health Strategy for Canada: Changing Directions, Changing Lives (http://strategy.mentalhealthcommission.ca/). Further independent research directed towards various components of the model, especially with regard to linkage to and interaction within primary care, would be very useful.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sun Life Financial; The T. R. Meighan Family Foundation; The IWK Health Center; The Dalhousie Medical Research Foundation; The Katheryn H. Weldon Charitable Foundation and the Department of Psychaitry, Dalhousie University; the IWK Foundation.