
Abstract
Radiation therapy service quality is not only defined by the technical aspects of care—the patient’s involvement and satisfaction also contribute largely to determining the quality of care received. Although there have been recent increases in support for the development of patient engagement activities throughout Canada, the lack of guidance and knowledge of patient engagement techniques within the radiotherapy context limits implementation. Without processes to obtain first-hand insight from patients, the need for these programs is overlooked. With a commitment to improving quality and consistency of care, the Canadian Partnership for Quality Radiotherapy recognized the need for a set of national guidelines on patient engagement in radiation therapy service delivery. Making use of the perspectives and first-hand experience of patient representatives, this initiative aims to develop a pan-Canadian guidance document that radiation therapy centres can adopt for successful integration of patient engagement through core activities of service delivery.
Introduction
In 2014, it was estimated that there were approximately 191,300 new cases of cancer within Canada, 1 and almost 118,350 courses of radiation treatment were administered, according to the Canadian Association of Radiation Oncology annual workload survey. With more than 40 radiation treatment facilities in Canada, quality assurance plays a critical role in radiation treatment planning and delivery, given the increasing complexity and rapid pace of technological innovation. However, while there have been extensive studies that aim to develop standards for equipment quality, personnel qualification, and safe practices in radiotherapy, the number of initiatives designed to measure patient engagement is limited. It is important to note that the level of quality in radiotherapy is not only defined by the technical aspects of care—the interpersonal component, or the patient’s involvement and satisfaction with the care process, also contributes largely to determining the quality of care that is received. 2
The Canadian Partnership Against Cancer (CPAC) strives to improve the patient experience across the cancer journey by supporting ‘person-centered care’ initiatives that are respectful and responsive to individual patient preferences, needs and values. 3 Within Canada, several patient engagement initiatives are already put into place, as CPAC continues to provide funding for these programs. Organizations such as Cancer Care Ontario, Cancer Care Nova Scotia, and the Calgary Cancer Project have developed patient engagement advisory groups, which allow patients with cancer, survivors, and their families to come together and discuss their unique experiences. 4 It has already been demonstrated that these types of patient experience and reporting programs can improve levels of patient satisfaction and the management of symptoms. 5
Although there has been a recent increase in support for the development of patient engagement policies and implementation of patient-centred programs, barriers such as workload pressure and complex organizational systems may limit these engagement methods and prevent efforts to permanently implement these policies in clinical cancer settings. 6,7 Within a radiotherapy context, the lack of guidance and knowledge of patient engagement techniques may limit implementation, and without processes to obtain first-hand insight from patients, the need for these programs may be overlooked.
With a commitment to improving quality and consistency of care, the Canadian Partnership for Quality Radiotherapy (CPQR) recognized the need for a set of national level guidelines that radiation therapy centres can adopt to ensure successful integration of patient engagement throughout the core activities of service delivery. The CPQR also recognized that not only current patients, but potentially affected people (the public), are affected by the decisions made within a radiation therapy program and have a right to be involved with the decision-making process. To ensure that a rigorous and comprehensive approach was utilized in the development of these guidelines, the CPQR utilized a three-phase approach that included an environmental scan, a national baseline analysis, and internal/external review followed by public engagement and finalization. All phases made use of the perspectives, expertise, and first-hand experience of patient representatives. The present article outlines the rationale behind the selection of 12 guidelines as recommendations for successful integration of patient engagement in Canadian radiation therapy service delivery. It also outlines how each individual guideline commits to a specific level of public engagement. For the purpose of this article, the term patient will apply to those currently affected and those in the public who may potentially be affected.
Materials and methods
The development and refinement of the guideline document involved three distinct phases.
Phase 1: Environmental scan
A preliminary set of guidelines were developed by drawing on elements of accreditation documents as well as the CPQR Quality Assurance Guidelines for Canadian Radiation Treatment Programs 8 document, which outlines the overarching organizational structure and processes that are required to assure quality and safe radiotherapy.
To evaluate the current national and international practices in radiation therapy patient engagement, a comprehensive literature search was carried out. Electronic databases searched included MEDLINE, PubMed, PubMed Central, and ScienceDirect. The following words were used either singly or in combination: patient engagement; radiation oncology; quality indicators; patient-centred care; cancer; shared decision making; radiotherapy; patient communication; informed consent; patient feedback; patient reported outcomes; access; barriers. All searches were limited to articles published between the years 2003 and 2015. Data regarding the current views and practices on patient engagement in countries such as Canada, United Kingdom, United States of America, and Australia were collected. Common themes were collected, and the findings from this review were incorporated into the guidance document.
Phase 2: Internal and external review
In the guideline review and development phase, various groups and individuals were given the opportunity to thoroughly review the document and assess the value of each individual guideline. The document was first distributed to the CPQR Steering Committee for initial feedback and an in-person meeting. The professional expertise and first-hand experience of the Steering Committee members allowed for valuable feedback to be given during this phase 2 review period.
Following an in-person review by the steering committee, the document was continually reviewed in-person and electronically by the CPQR Patient Engagement Working Group (PEWG; Figure 1). The PEWG is led by members of the steering committee who have professional experience in patient engagement techniques and programs. Additionally, in order to obtain first-hand patient opinions on the contents of the guidance document, CPQR recruited patient representatives to sit on both the steering committee and the PEWG meetings. They were each encouraged to share their unique experiences, insights, expertise, and perspectives to the development of the document.
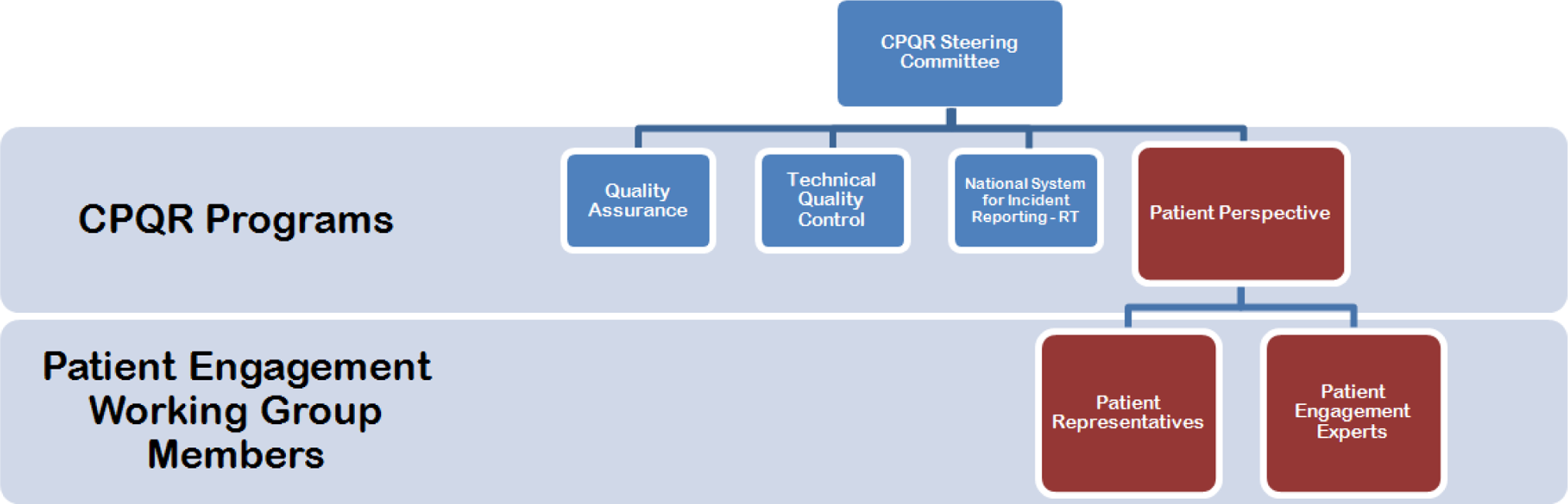
Canadian Partnership for Quality Radiotherapy (CPQR) patient engagement program
The revised document was also distributed to a group of external individuals involved in patient engagement activities at the following centres across Canada: Princess Margaret Cancer Centre (Toronto), Alberta Health Services, Nova Scotia Cancer Centre, British Columbia Cancer Agency, and Provincial Health Services Authority (British Columbia). At an in-person PEWG meeting, the feedback was discussed alongside the value and phrasing of each individual guideline.
In order to realistically assess the baseline level of patient engagement activities across Canada, a patient engagement survey was distributed to CPQR National Quality Assurance Committee (NQAC) members at various cancer treatment centres. The on-line survey asked radiation therapy program leaders questions about current patient engagement practices at their cancer centre and were based on the key concepts of the guideline document. During the entirety of the internal and external review phase, results of these surveys were collected and summarized.
Phase 3: Public review and finalization
The final refinement phase consists of a thought leader workshop and broad community review. The thought leader workshop was attended by leading patient engagement experts from across Canada. A third of attendees were patients. Participants were provided an overview of patient and public engagement activities taking place both nationally and provincially and were asked to review each proposed statement for feasibility and clarity. Further revisions to the guideline were made based on the workshop and a final draft was circulated for community review.
Based on the community review, revisions were then made to the guidance document followed by a finalization of the resulting set of guidelines. Figure 2 provides a timeline of the steps that were undertaken to finalize the guidance document. A final version of the guideline document is now available on the CPQR website.

Next steps for the finalization of the guidance document
Results
The environmental scan and literature review in phase 1 allowed for the identification of 18 guidelines that fell under eight key concepts of patient engagement in radiation therapy: educational resources, patient communication and informed consent, disclosure of adverse events, patient feedback, evaluation of services, patient-reported outcomes (PROs), barriers, and utilization rates.
The various internal and external review processes throughout phase 2 allowed for key discussions regarding the relevance of each specific guideline. With the help of patient representatives who have each been through a unique radiation treatment and care journey, each draft of the guideline document was assessed for its accuracy in addressing the realistic needs of radiation therapy patients.
Concurrently, we collected the results of the national patient engagement survey from CPQR NQAC members. Altogether, we received responses from 40 radiation therapy programs with representation from British Columbia, the Prairies, Ontario, Quebec, and Atlantic Canada. The survey was answered by various healthcare professionals from radiation oncologists to admin staff, working at different types of radiation therapy programs.
Figure 3 summarizes the results of the survey. While just over half of the programs reported active patient engagement, 36% provided solely educational materials and a mere 3% of the participating programs had patient representation in their Radiation Therapy Quality Assurance Committee. The collection of patient feedback showed a higher level of implementation, with roughly 65% of participating centres encouraging patient feedback in their educational material development. However, roughly 50% of programs did not provided their patients with an opportunity to provide feedback through survey or focus group or were unsure of their method of collecting feedback. A large majority of the radiation therapy programs (∼80%) had processes for reviewing patient complaints and reported acknowledging the feedback within 48 hours.
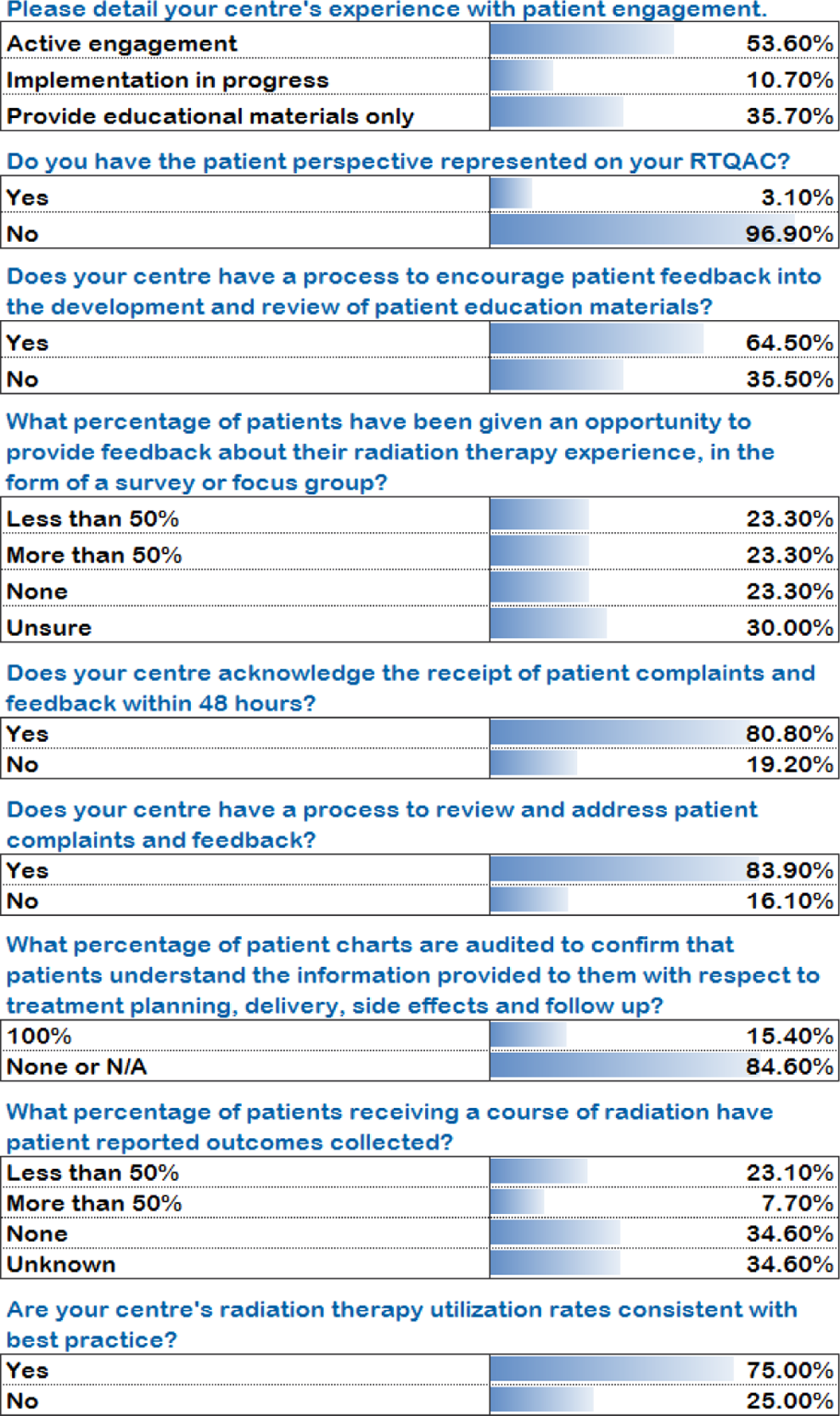
National patient engagement survey responses
A drastic 85% of participating programs did not regularly review patient charts to ensure that informed consent was given by the patient, and only 8% of programs gave their patients an opportunity for their PROs to be collected. Finally, 75% of the participating programs believed that their utilization rates were consistent with best practice.
At the end of phase 2, the document had expanded from 18 to 21 guidelines. These 21 guidelines were brought to the day-long thought leader workshop in phase 3, where the document was reviewed and discussed by a group of patients and patient engagement experts from across Canada.
At the workshop, the International Association for Public Participation (IAP2) core values of public participation were discussed. International Association for Public Participation is an international leader in public participation and has developed a set of core values for use in the development and implementation of public participation processes. The main purpose of these values is to help groups make better decisions, which reflect the specific interests and concerns of potentially affected people and entities. 9 As such, the group realized the importance of reaching not only current radiation therapy patients but those in the public who may potentially require radiation therapy treatment. The document underwent a final revision in order to apply each guideline to a specific level of public engagement, taken from the IAP2 spectrum of public participation 10 .
Final concepts and guidelines
1. Educational resources
There is evidence to indicate that patients currently want more education about the cancer treatment and care process than they actually receive and that the most common source of patient dissatisfaction is the failure in communication of information about illness and treatment. In the United Kingdom, Macmillan Cancer Support developed a Patient Experience Working Group, which compiled key recommendations for improving the patient experience within the broad field of cancer care. The working group believes that the information should not only educate the patient about their treatment and disease but it should also give them a realistic idea of prognosis, allow them to understand the likely outcomes, enable them to assist in self-care, provide reassurance, and connect them with self-help groups. 11,12
Furthermore, the working group highlights the reality that patients’ information needs are highly diverse. The information provided by the medical professional can be extremely beneficial, especially if it is personalized to the patient. Previous research has shown that providing patients with personalized materials can decrease their treatment anxiety levels, teach them something new about their illness, and increase levels of emotional support through discussions and sharing with friends and family. 13,14 In order to personalize information, not only should the information be specific to the type of cancer care given, but it should also take demographic characteristics such as age, sex, and cultural background into consideration. 15
In 2001, McPherson et al. 11 conducted a systematic literature review of randomized controlled trials in order to identify the most effective methods of providing information in cancer care. The investigators concluded that resources such as written materials, telephone help lines, teaching aids, and audiovisual aids have a positive effect on patient outcomes such as knowledge, recall, symptom management, service satisfaction, and healthcare utilization.
Based on these authentic patient opinions and recommendations, guidelines were developed to ensure that radiation treatment programs keep patients informed by providing a wide range of educational resources and also keep them closely involved by working directly with them on the review and revision of the educational material content.
2. Patient communication and informed consent
The process of providing patients with sufficient and appropriate information allows them to confidently communicate with their healthcare provider and express informed preferences when providing consent. The UK’s Royal College of Radiologists 16 published a set of standards for patient consent, which are specific to radiology. In this document, the college recognizes the importance of fully involving patients in their treatment and care decisions. This process of involving patients in the decisions to be made and communicating information effectively is outlined as a key component of the consent process. Whenever possible, radiation oncologists must be completely satisfied that the patient is fully informed about the risks and benefits of treatment, has understood what is proposed, and has given voluntary consent.
The Royal Australian and New Zealand College of Radiologists’ (RANZCR) 17 have also published a set of standards that support this thorough consenting process. The RANZCR states that the practice of obtaining informed consent should be viewed as an ongoing one, whereby patients are repeatedly given the opportunity to have all their questions answered and that they fully understand the information provided to them. It is also recommended that informed consent be noted in patients’ charts or electronic records by the consenting physician at specific intervals in the care process prior to treatment.
In order to incorporate the various practices across the United Kingdom, Australia, and New Zealand, guidelines were developed as guidelines for successful patient engagement in communication and obtaining informed consent in radiation therapy programs. Guideline 3 involves patients by promising to work with them to ensure that all their concerns are directly reflected when treatment decisions are being made, while guideline 3 addresses the consult level of engagement by ensuring that they remain informed while listening to their specific concerns and treatment goals.
3. Disclosure of adverse events
As part of the effective communication process, it is important for the organization to implement a formal process for the disclosure of adverse events to patients and their families. The disclosure of adverse events is practiced in several healthcare programs within the United States and is also outlined in the national health policies in Canada, the United Kingdom, and Australia. A survey measuring 2,637 US and Canadian physician attitudes towards disclosure showed that 98% support disclosing adverse events to patients and 66% believe that disclosing a serious error reduces the risk of malpractice. 18,19
The Canadian Incident Analysis Framework encompasses a Patient/Family Perspectives section, which was written by members of the Patients for Patient Safety Canada, a patient-led program of the Canadian Patient Safety Institute (CPSI). These patients and families confirm that the open sharing of information with their healthcare provider helps to strengthen their trust in the care team and improves the safety and experience. The patients strongly believe that the principles of safety and patient-centred care are even more important when harm occurs or things do not go as expected. They believe that the disclosure, learning, and improvements made for the next patient are the most important part of the process. 20 In support of the views expressed by the CPSI, guideline was developed as a recommendation to ensure that the disclosure of adverse events is practiced by all radiation therapy programs. By involving and collaborating with the patient, the program can look to patients for support in formulating solutions and incorporating their advice and recommendations to prevent future events from occurring.
4. Patient feedback
There is a global trend that is moving towards detailed measurements of patients’ experiences and away from global satisfaction feedback. In the United Kingdom, the National Health Service (NHS) conducted a literature review that looked at user involvement in healthcare services. Ultimately, the active involvement of users through the collection of feedback and reviews is meant to develop a service in which “care is shaped around the convenience and concerns of patients.” 21 In their practice standards, RANZCR have also highlighted patient feedback as an essential indicator for the delivery of safe, quality care to radiation oncology patients.
There is also an increased importance being placed on the establishment of processes, which address patient feedback that arise from ethical issues. When these issues arise, healthcare professionals must resolve the conflicts while maintaining commitment to the organizational values. 22 Methods for addressing ethical issues may include supporting patients and families by means of patient advocacy and other formal support mechanisms.
For the successful quality monitoring and improvement in other jurisdictions, there is a heavy focus placed on the ability to obtain feedback directly from patients. In order to make these themes applicable to a Canadian radiation therapy program, guideline was developed. This guideline allows for a collaboration with the patient, where their specific feedback is incorporated into future decisions that the program makes.
5. Evaluation of services
To appropriately evaluate the efficacy of services related to patient engagement, it is recommended that healthcare programs have an effective process for monitoring and evaluating patient and family perspectives on the quality of services received. The UK’s Department of Health has recommended that healthcare programs have an effective process for monitoring and evaluating patient and family perspectives on the quality of services received. By having a process for obtaining evaluations, the program can successfully design new programs, facilities, or services that are centred around the needs of their users. 21
Although it is common for healthcare programs to collect service evaluations from their patients, the positive outcomes of collecting the feedback can be limited until the results are shared with other relevant members of the care team. In the United Kingdom, the United States, and some European countries, healthcare services have implemented programs that allow patient evaluations to be shared at a national level. The United States has implemented the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Benchmarking Database as a national database for surveys. It holds 11 years of data and helps policy-makers monitor the nations’ progress towards healthcare quality improvement. 23 In Canada, some healthcare programs also conduct CAHPS surveys. The data are collected, but there is no standardized system to compare quality of care between health services across the nation. 24
Based on these global practices and recommendations, guidelines were developed to ensure that radiation treatment programs have processes for monitoring patient perspectives on the quality of services and that the sharing and benchmarking of the evaluations are used as a key method for improving services. Certain guidelines allow for patients to collaborate with the program through the collection of advice that should subsequently lead to improvements in quality. Alternatively, some guidelines involve the patients by listening to their concerns about service quality and ensuring that they are provided with feedback on how their input contributed to the change.
6. Patient-reported outcomes
The interest and use of PROs has grown internationally in the United States, United Kingdom, and Australia. Reviews of the current state of PROs in clinical practice within the United States have shown that these interventions improve communication, diagnosis, and treatment. However, there are fewer results that report patient satisfaction or health status. 25 Likewise, it has been reported that 65% of studies found a difference in the process of care, but differences in outcomes were found in only 47% of studies. 26
According to Snyder et al., 27 a number of studies in the United Kingdom and United States have investigated the use of PROs in an oncology setting. It was most consistently found that there were benefits in communication and some benefits in treatment and outcomes. Routine assessments of health-related quality of life of patients with cancer had a positive impact on the communication between patient and doctor and also showed an improvement in emotional functioning when compared to those groups of patients who did not regularly complete PROs during their cancer care. 28 It was found that the use of the information obtained from these PROs is associated with a clinically significant improvement in the patient’s well-being.
It has been commonly suggested that these PROs are useful in facilitating the detection of physical or psychological problems, to monitor disease over time, and ultimately improve the delivery of personalized medical care. Based on the findings from these preliminary studies, guideline was developed to address the importance of PROs in radiation therapy service delivery. This specific guideline ensures that patients are consistently informed of the process of collecting PROs.
7. Barriers
Research has identified income, age, sex, education, and location of residence as contributing factors to access to cancer care. 29 Furthermore, due to the disparate Canadian population, ethnicity and culture have also been identified as potential barriers to cancer care access. From a healthcare professional’s point of view, the inability to effectively meet the language and cultural needs of those from a wide range of ethnic backgrounds may contribute to these barriers. 30 As such, those responsible for managing the treatment program have an ethical responsibility for making the service accessible to all who need it. This can be done by identifying and removing barriers that prevent clients, families, service providers, and referring organizations from accessing services.
The ability to provide accessible cancer care is of paramount importance, and addressing the barriers that prevent access is an essential component of patient-centred care. Guideline was developed as a guideline to help radiation therapy programs address barriers that may prevent access to their services. This guideline encourages collaboration between the program and the patient, as the barriers could not be addressed without the first-hand experience, advice, and recommendations of the patients.
8. Utilization rates
The radiation therapy utilization rate is a measure of the proportion of a population of patients with cancer who receive at least one course of radiation therapy within the first year of cancer diagnosis and can be an indirect measure of access to cancer care. It has been suggested that around 40% of patients with cancer should undergo radiation therapy, but there is a global shortfall in the actual delivery of radiotherapy. 31
Although it was initially thought in phase 1 that recording regional radiation therapy utilization rates was an important concept reflecting patient access, discussions among the patients and patient experts of phase 3 thought leader workshop revealed that it is not a direct relation to patient engagement. This section has been removed from the current state of the guideline document but continues to carry importance in the CPQR mandate.
Discussion
Patient engagement is critical to improving the quality of the patient’s cancer journey
A study by Gagliardi et al. 32 aimed to examine patient and physician opinions on patient participation on the selection of cancer care indicators in Canada. It was found that most patients and healthcare professionals have positive views on patient engagement and strongly believe that patients should be part of a committee or board where their feedback and opinions could be used to improve the care process. By directly involving patients in various aspects of service delivery, the quality of the service would undoubtedly meet the expectations of the general patient population. The need for this culture shift is evident in the current state analysis, as 97% of radiation therapy programs across Canada have reported that they do not have patient representation on quality assurance committees. Additionally, approximately half of the participating programs reported that they did not have active engagement activities at their centre. Ultimately, the patient’s active involvement in their cancer care journey and their knowledge, skills, and confidence in managing their health are critical in improving the quality of the patient’s cancer care journey. 4
Patient education leads to more informed decisions and can shape the experience of the patient
Educational resources offer decision support by providing evidence-based tools that can facilitate the process of making informed value-based decisions about treatment and disease management. Instead of being prescriptive, educational resources should help patients clarify their values and preferences while outlining the potential risks and benefits of alternative treatment options. 11 The materials should be available in various languages, literacy levels, and functional abilities, in order to accommodate the needs of the highly diverse Canadian population. By informing and involving patients in the development and revision of educational resources, the radiation program ensures that specific concerns and interests are reflected in the provision of patient education during the course of a patient’s radiation treatment.
Effective communication and informed consent helps patients feel involved and in control
Using a shared decision-making process, patients should be given an ongoing opportunity to have discussions with their doctor and make a free, voluntary decision about whether they will participate or continue to participate in the treatment or research. 33 Using a shared decision-making process allows patients to be active participants in their care and should be the goal of all physician–patient interaction. Within a radiation therapy setting, effective communication and informed consent through proper involvement and consultation respect the patient’s autonomy and protect them from any potential harm during treatment. The National Patient Engagement Survey, which showed that nearly 85% of informed consent is not documented across Canadian radiation therapy programs, demonstrates the importance of a culture shift.
The disclosure of adverse events can lead to more trusting relationships
The most beneficial outcome of effective patient-centred communication is the understanding of patients’ individual needs and values. This builds positive relationships that can allow for more honest discussions about the care process, especially when the discussion must involve disclosing adverse events. Research has shown a positive relationship between client satisfaction and how an adverse event is handled by an organization. If the adverse event is discussed with the patient in an open and timely manner, this may maintain the patient’s relationship with the organization, staff, and service providers. The open sharing of information between the patients and their healthcare provider, through direct involvement and collaboration, supports the patient-centred care culture and ensures that patients feel fully engaged in their care. Accreditation Canada’s Required Organizational Practices Handbook 2014 recommends that organizations implement a formal and open policy and process for the disclosure of adverse events to clients and families. With patient safety as a priority, it is also imperative for programs to inform and collaborate with their staff to implement corrective action, which can prevent repeated incidence.
Obtaining patient feedback provides an indication of patient expectations and the realities of the care received
To further support the patient safety culture, the process of obtaining patient feedback is viewed as an essential component of treatment quality, monitoring, and improvement and is being included in patient engagement practices around the globe. This can be achieved by the use of survey tools, focus groups, or other methodology. 11,34 Previous research has shown that there is an association between poor quality experience and poorer health outcomes, so it is becoming increasingly important to encourage patient feedback in healthcare settings. It has also been shown to stimulate quality improvement in the delivery of healthcare. 34 To ensure that valuable patient feedback does not get neglected, a quality monitoring and improvement process that allows for the acknowledgment and consideration of all feedback should be put in place at all radiation treatment programs. There needs to be a shift from generalized satisfaction feedback mechanisms to those that collaborate with the patient to ensure that their advice and recommendations are incorporated into program decisions. It is recommended that the feedback procedure is readily available and that the program staff regularly promote the process and ensure that it is easy to use.
The evaluation of services allows patients to provide recommendations for quality improvement
To support the patient feedback that is received, healthcare providers looking to enhance the care experience for patients can look to the service industry for guidance. In the service industry, a large emphasis has been placed on how the opinions of users can be translated into changes to goods and services. The concept of involving service users in change management is considered an essential component of maximizing customer loyalty and growth. The UK’s NHS uses focus groups to involve users and learn about the effectiveness of their services, enhance accountability, and improve public perceptions. 34 In the delivery of services, there is a general agreement that in order to meet the expectations and preferences of service users, it is important to ensure that 100% of users are given the opportunity to provide feedback. 34 Through the method of involvement and collaboration, those who use the services can provide the most valuable input when decisions are to be made about reconfiguration and development of the program. In a radiation therapy setting, the service users include the patients and their families. The national survey revealed that a large majority of Canadian radiation therapy programs already have processes in place to review and address patient feedback. Ideally, patients will have better health outcomes as a result of positive experiences during their radiation treatment journey. However, these positive experiences may not be possible without the continual improvement in high-quality services.
Patient-reported outcomes help programs understand the patient experience and determine the effectiveness of therapies
An additional form of feedback is a PRO. The use of PROs is growing in the healthcare sector and can be an important component of effective patient engagement. Patient-reported outcomes are outcomes that matter to the patient and are usually self-reported through questionnaires. 27 The Radiation Therapy Oncology Group (RTOG) was developed in order to host radiation oncology trials for patients with cancer between multidisciplinary groups. The RTOG has recognized the importance of PROs in evaluating the impact of cancer therapy on patients, especially in the case of clinical trials. Over the years, the RTOG studies that focus on PROs have helped develop clinical guidelines in radiotherapy treatment techniques. 35 Nationally, only 8% of radiation therapy programs have reported that PROs are collected from more than 50% of their patients. There is a clear requirement for guidance in introducing PROs as an essential tool in evaluating the quality of care, collecting data about experiences within cancer therapy, and to determine the effectiveness of various therapies in treating cancer and improving the quality of life of patients. Optimizing how patients feel should be a primary goal of all oncology practices and is therefore appropriate for the assessment of service quality. 5
Barriers reflect the public’s access to treatment facilities as well as the quality of care being received by current patients
Although collecting feedback may provide an accurate indication of the view of treated patients, the views of those who are unable to access required care may be missed. Accessible cancer care means that the service is readily available, and the people who are requiring the service are able to access it when needed. For radiation therapy, accessibility is particularly important due to the complex treatment process as well as the sensitivity in providing timely care. Despite these factors, access to care may be compromised by barriers that are under the team’s control (eg, hours of operation, physical or language barriers) or by barriers that are not (eg, transportation). From a patient engagement perspective, it is important for radiotherapy programs to collaborate with patients in order to be advised of the realistic barriers to access. These barriers reflect the access to treatment facilities as well as the quality of care.
A final version of the 12 patient engagement guidelines is currently available at http://www.cpqr.ca/wp-content/uploads/2013/09/PEG.2016.06.012.pdf. After distribution of these guidelines to centres across Canada, it is the hope of CPQR that the recommendations be used to transform current healthcare professional attitudes towards patient engagement activities. Ideally, CPQR would like to see the redistribution of the patient engagement survey used in phase 2 to reflect an increased level of patient engagement at a national level.
Conclusion
With a strong commitment to safety and quality in radiation treatment, the CPQR encourages patients and healthcare professionals to work as partners during the treatment and care process. In the current state, patients may not be given enough opportunities to be actively involved with their care. Additionally, programs may not have the dedicated resources to provide collaborative opportunities with patients. With specific training in engaging patients and support from the CPQR patient engagement guidance document, oncologists can start to recognize their responsibility to promote healthcare literacy and further involve patients and the public in the radiation treatment program improvement. At the same time, patients should be encouraged to raise their level of involvement and express their preferences more vocally.
The development of recommendations based on evidence-based research results along with input from patients and professionals is the first step towards implementing a national guideline. By providing radiation therapy programs with a tool to measure their level of patient engagement, their current state can be assessed and improvement opportunities can be identified. Ultimately, these guidelines can help provide fuel for the successful implementation of new patient engagement strategies and programs. This global shift in the culture of cancer care is what will allow the patient engagement initiative to move forward.
Footnotes
Acknowledgments
The authors would like to thank additional members of the CPQR Patient Engagement Working Group: Michel Milosevic and Eshwar Kumar. They also like to acknowledge the CQPR Patient Representatives: Ross MacDonald, Lianne Wilson, Leslie Hill, and Louise Bird for their valuable contributions to the development of the Patient Engagement Guidelines.