
Abstract
Canada’s opioid crisis is a public health emergency that disproportionately affects people who use drugs alone at home, requiring the mobilization of health systems to implement timely, effective, and innovative programs. The purpose of this review is to provide a synthesis of recent literature relating to technology-enabled harm reduction strategies. The results of the literature review are corroborated with key informants, including family members of people who use drugs and policy-makers in the area of opioid use. Based on this, it is recommended that technology-enabled support programs for people who use drugs at home must deliver support at whatever point the person is along their drug use continuum, must transfer frontline relational skills, must be co-developed with community members and service providers, and must deliver predictable and reliable services that are safe from stigma.
Introduction
Canada is facing a national opioid crisis which has required mobilization of the healthcare system to overcome the crisis through national and provincial strategies, including the Canadian Drugs and Substances Strategy. 1 It is a problem gradually spreading across the country and a public health emergency has been declared in multiple jurisdictions, including the Okanagan area of British Columbia. Technology-enabled interventions provide an unprecedented opportunity, especially in remote communities and for people who want to preserve anonymity. This article provides a summary of literature complemented by key informant consultation to inform the development of technology-enabled programs and activities by healthcare leaders.
Methods
This synthesis consists of two sources of information that were used to develop key themes. First, a literature review focused on People Who Use Drugs (PWUD) or similar populations, specifically PWUD at home. Literature review topics that drove the search included:
Effective continuity of care and patient engagement;
Attachment styles and relationship-centred care in relation to harm reduction and opioid use;
Harm reduction and addiction programs; and
Effective relationship-building methods through technology, especially in hard-to-reach populations (both medical and non-medical literature and across urban and rural settings).
The literature searches consisted of acquisition of already widely used and regarded literature on harm reduction and relationship-centred care from personal bibliographies and contacts, as well as more formalized database searches (PubMed, Embase, Web of Science, CINAHL, and PsycINFO) and citation searching of retrieved articles, as appropriate. Librarians at the University of Saskatchewan and Alberta Health partially supported the searches by ensuring that keywords and combinations of searches were comprehensive. Published literature reviews and meta-analyses were selected and reviewed according to relevant content and methodological rigour. Overall, the literature relating to technology use by PWUD at home to seek support was sparse. For example, we were not able to find any relevant literature on the appropriateness of various informatics platform solutions to this population. Key articles are presented below.
Next, key informants were purposefully selected for semi-structured interview consultations. As the project was a collaboration with British Columbia’s Interior Health Authority, the proposed consultation received A pRoject Ethics Community Consensus Initiative 2 review prior to proceeding. We began with a wide-range identification of local (Kelowna area) and provincial stakeholders via existing networks and word of mouth. Informants included former PWUD, family members of PWUD, frontline service providers, and local/provincial leaders with portfolios relevant to the PWUD file. Information was sought out over a course of nine interviews and consulting sessions. In total, interviews were conducted with seven individuals and one stakeholder group. Data collection sessions were moderated by two or three research group members and audio-recorded with consent where feasible. Questions explored whether a technology-based program would meet the needs of PWUD, how PWUD would access such a program, the ideal staffing model, and program inputs and outcomes to be considered. Recordings and field notes were reviewed by all team members. Emerging themes from basic content analysis were collated and agreed upon by all team members.
Findings
Rationale for a harm reduction approach
The harm reduction approach is based on values of self-determination, inclusion, freedom from harm, and the promotion of public health. It is grassroots-driven, humanistic movement that grew out of a compassionate approach to a public health crisis associated with active injection drug use. 3 The main idea of this approach is to work with PWUD toward self-selected health goals, along a continuum ranging from safer use to abstinence. It has been shown to be effective, as people at risk of harm develop innovative and practical ways to reduce risk in partnership with frontline nurses, social workers, and outreach workers. Further, healthcare providers engaged in harm reduction practice transition from a solution orientation to a harm reduction orientation, from stigmatizing patients to recognizing their moral worth, and from assigning blame to supporting autonomy. 4
The harm reduction approach has given rise to various Safe Environment Interventions (SEIs), including syringe exchange programs, supervised consumption sites, and peer-based harm reduction interventions. The impact of Supervised Injection Sites (SIS) has been recently systematically reviewed. Potier et al. synthesized evidence of harms and benefits of supervised injection services. In total, 618 articles were identified, of which 75 met the evaluation criteria and were used in the review. The literature represents mainly a Canadian (Vancouver, British Columbia) environment due to rigour of inclusion criteria. 5 A notable finding was that implementation of SIS led to a substantial (35%) decrease in the number of lethal overdoses in the vicinity of such services; between 2 and 12 overdose deaths were avoided each year. More importantly, there were no reported deaths by overdose within an SIS, nor were increases in drug use, trafficking, or crime observed. Yet, there was an increase in referral to addiction treatment centre, initiation of detoxification program, and opiate agonist therapy. 5
The use of SEI as a means of reducing drug and health harms is also favourably perceived by PWUD. A meta-synthesis of 29 articles representing an aggregate of over 800 participants’ viewpoints was conducted to develop a comprehensive understanding of SEI. 6 These articles also represent a mainly Vancouver-based respondent sample, as majority of included studies were also conducted in Vancouver. The analysis shows that PWUD view SEIs as:
A physical and social environment to escape everyday and structural violence. By providing refuge from street-based violence, in particular violence arising from drug law enforcement. By contextualizing the understanding of “safety.” Participants indicated that these interventions provided environmental support that did not promote the risk of physical violence and provided an alternative to public consumption settings. Safe environment interventions provided an environment free from stigma, discrimination, and judgement.
An enabler of safer drug use practices. By reshaping the social and environmental contexts into safer practices. By situating safer consumption, mainly by reducing rushed injections and syringe sharing. It is important to note that these interventions provide perceived control over the consumption process, such as easing access to equipment and space to inject. As well, these interventions minimize barriers provided by social, structural, and spatial constitutions of their environment.
6
McNeil and Small further highlight that participants indicated that the SEIs facilitated their access to other services, such as food, shelter, social services, and healthcare. One of the key themes emerging from participants’ perspectives was the emergence and importance of trust between them and the program staff. This was particularly the case when the SEIs were integrated with the healthcare and social services systems. In fact, although participants often associated entering the healthcare system with negative experiences, they were more likely to access care when encouraged by a staff member from the SEI services with whom they had a trusting relationship. 7
Importance of relationships for PWUD
There is robust evidence that strong social support is associated with a higher likelihood of drug use cessation, suggesting that a relational practice approach is particularly salient for PWUD. 7 Relationship-centred care is associated with improved health and health service outcomes. Existing direct empirical evidence on relational care of PWUD specifically suggests that PWUD endorse the professional-patient relationship as central to effective care and positive patient experience. Healthy professional-patient relationships with PWUD are characterized by non-discrimination, empathy, open communication, shared decision-making, and trust. 8,9 The four core principles of relationship-centred care are as follows:
Healthcare relationships should be authentic, acknowledging each agent’s personhood;
Affect and emotion are critical to healthcare relationships;
Healthcare relationships involve reciprocity; and
Creating and sustaining relationships in healthcare holds moral value and transcends fiduciary duty. 10
Use of technology in harm reduction
Given system constraints and variable PWUD preferences for care, traditional face-to-face approaches for engaging with PWUD are not always feasible. This is particularly true in geographically isolated communities and with people with limited mobility and/or access to transportation. 11 To increase the impact of services while reducing the cost, the use of web-based interventions has recently increased in popularity. These approaches reduce geographical and resource constraints associated with the person-to-person support and increase the reach in remote communities. As well, web-based interventions provide a higher degree of anonymity for PWUD who are often targets of stigmatization.
As indicated in a review of 74 publications by Paul et al. to determine the effectiveness of web-based intervention and support for patients, as many as 80% of people who have access to the Internet search for health information on-line. Moreover, web-based information and support tools are effective in increasing patients’ knowledge and selected health behaviour outcomes, especially for chronic illnesses. 11 Similarly, web-based programs are effective in attracting younger users into tobacco treatment programs. Although attrition rates varied across studies, attrition rates from web-based programs were overall similar to those seen in person-to-person treatment programs and were further reduced when there was direct contact between a therapist and a program participant. 11
Although there is limited research on the efficacy of web-based approaches in improving psychosocial outcomes of patients with common chronic conditions, most studies included in the Paul et al. review focussed on mental illness. Twenty of 36 Effective Practice and Organisation of Care studies showed a significant positive effect on psychosocial outcomes, favouring web-based intervention; little effect was noted for depression specifically. With the lack of research in the area, it is difficult to establish the efficacy of web-based approaches for cost-effectiveness, especially when compared to existing harm reduction programs.
The Internet is a widely used resource for PWUD and continues to be a growing medium for the purchase of illegal drugs and for peer-to-peer sharing of information. Most information sought out by PWUD relates to drug types, effective use, and safety. 12 The use of web-based programs also provides an opportunity to advance harm reduction activities by providing real-time evaluation of emerging drug trends and epidemiological studies. 13 For example, in July 2014, the use of tramadol showed increased page traffic over hydrocodone. Although there may be several reasons for this increased interest (eg, US legal rescheduling of tramadol, media attention), these web sites also served to gauge the reaction to ongoing large-scale initiatives, such as policy action and provided an epidemiological assessment reflective of current trends. Thus, web-based programs provide an opportunity; changes in web traffic and new forum queries can reflect public interest in various drugs and can be used as a tool for rapid identification of new and emerging drug use patterns. The information obtained from web sites can also shape the way PWUD accessing the site use psychoactive substances and modify their behaviour based on provided safety information. 13
The “darknet” is a system of relays and encryption protocols that disguise the origin, content, and destination of Internet traffic. 12 Information on drugs amounts to approximately 70% of listings on one of the more popular darknet sites. Using forum threads and analysis, Bancroft analysed the use of cryptomarkets (exchange of digital encrypted assets) to determine the type of knowledge and discourses used by PWUD. The results indicated that the cryptomarkets provide an infrastructure for a community that supported exchange of information and product and risk reduction activities. The exchanges drew on knowledge from PWUD, vendors, and professionals interested in cultural normalisation/pathologization, chemical potency, legal/policy, and market. Site users indicated their adaptation of many harm reduction practices and promoted a responsible use orientation which included taking responsibility for their own harm reduction. 12
There are also several mainstream on-line resources for PWUD. These forums are used by PWUD worldwide and often provide an information source to learn about novel substances. A systematic examination of 13,082 posts from 60 threads of discussion on such popular forums was conducted by Soussan and Kjellgren. 14 The analysis revealed four major themes relating to the information site users are seeking:
Uncovering the substance facts. Substance identification, pharmacology, and assessment for purity, legal status, and acquisition;
Dosage and administration. Administration techniques, dose recommendations, technical talk about equipment, and preferred setting for drug use;
Subjectively experienced effects. Self-reported experiences with many different aspects of intoxication depicted in great detail including positive and negative experiences; and
Support and safety. Efforts of communities to prevent and minimize harm by sharing information about potential risks of harmful effects or contraindications of a substance; As well, on-line support and guidance provided to intoxicated persons who experienced bad or fearful reactions.
14
Recommendations for program design to reach PWUD alone at home
The above literature was used to develop a logic model (Figure 1), wherein the opioid crisis response is reoriented to include targeted programming for PWUD who remain relatively hidden, such as those who use alone at home. Preliminary suggestions for targeted programming, developed from the preceding review, were shared with key informants for feedback.
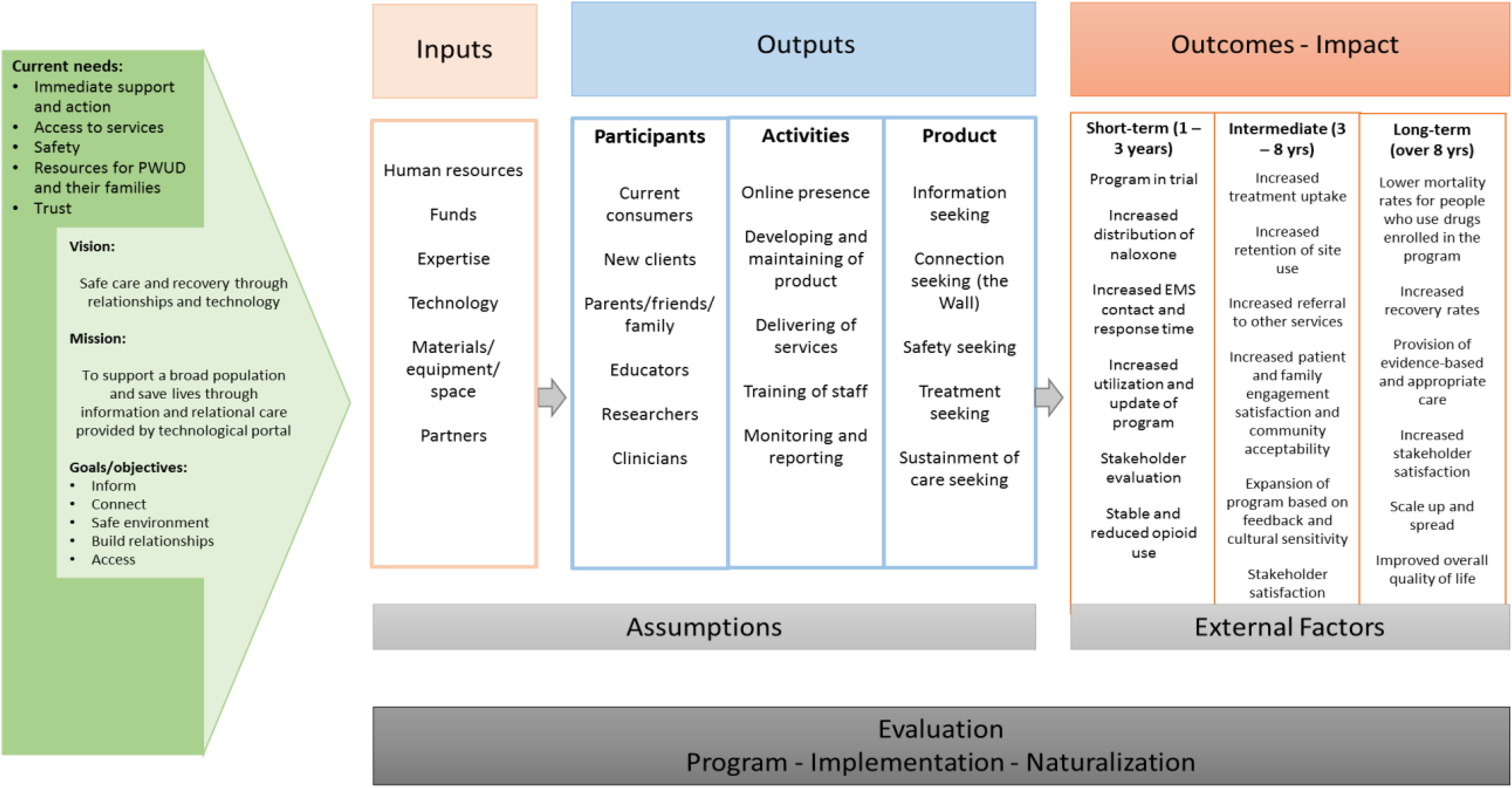
Overview of the program logic model.
Key informants emphasized that PWUD need to see themselves in programs designed to meet their needs. For those who use alone at home, this can be accomplished using on-line media. People who use drugs may seek on-line resources out in times of crisis, providing a small window of opportunity, potentially requiring 24/7 support. Surges in demand are anticipated, for example, at the beginning and end of workdays. On-line harm reduction programs need to engage a wide range of people and contain the following program components:
Support PWUD at whatever point they are situated along a drug use continuum;
Involve the transfer of a relational skill set from frontline workers through technology;
Provide up-to-date information on harm reduction, treatment options, and other topics of interest;
Provide peer support via forums maintained and monitored by staff with lived experience;
Link PWUD to on-line supervised consumption options and/or a physical location for safer consumption, including connection to naloxone kits;
Include a sound implementation strategy for the program to ensure all technology components used to deliver the services are highly reliable, available (24 × 7 × 365), well supported, and regularly updated;
Create an easy-to-navigate on-line interface and services that are co-developed with community members and service providers and accessible by various hardware options, for example, mobile phones;
Develop appropriate downtime procedures that continue to support users, should an outage impact the service; and
Connect technology-enabled services to local mental health/crisis response services.
Conclusion
Throughout Canada the focus of interventions to date to reduce opioid overdose has been on the street-entrenched population. However, programs have had an unclear reach into the “hidden” at-home population where the statistics demonstrate an ongoing unmet need. The health system needs to act swiftly, yet thoughtfully, to prevent overdose and reduce mortality if overdose occurs. Existing literature and key informant consultation can inform service providers tasked with addressing opioid overdose and its impact on public health and health systems.
Footnotes
Acknowledgements
The authors would like to acknowledge the following people for their support throughout the project: Devidas Menon, PhD, and Stephanie Montesanti, PhD, for providing us with the needed guidance in focusing, revising, and publishing this manuscript; Susan Brown for her support and sponsorship of the project; and Dr. Douglas Kingsford and Dr. Silvina Mema for informing the content. Finally, authors would like to acknowledge the Fellowship for Health System Improvement program and organizers for an opportunity for our team to come together and guidance we have received along the way.