
Abstract
The use of Robotic-Assisted Surgery (RAS) in Canada continues to grow and evolve, demonstrating improvements in patient and clinical outcomes across a wide range of surgical procedures. Global studies show how implementing a RAS program can also increase hospital capacity, drive benefits in health human resources, and improve overall health system efficiency. Despite the evidence of these positive results, Canada lags behind other developed nations in adopting RAS. Drawing on the experience of surgeons and health leaders from across Canada, this article focuses on the benefits of adopting RAS and discusses the challenges organizations face in successfully funding and implementing RAS programs. This includes the innovative approaches health leaders are taking to support equitable access to RAS for patients and offers evidence-informed strategies that can help unlock the full potential of RAS—beyond the operating room—to improve overall quality of care and the sustainability of the Canadian healthcare system.
Introduction
In keeping step with the rapid growth of innovation in health technology, medical communities world-wide are adopting robotic-assisted surgery, or RAS. Soft-tissue RAS is used across a broad range of surgical specialties including urology, gynecology, thoracic, cardiac, head and neck, and general surgery. Compared to open surgery, the clinical benefits of Minimally Invasive Surgery (MIS)—which includes both traditional laparoscopic surgery and RAS—are well understood and widely acknowledged.1-5
Evidence consistently demonstrates that RAS further improves MIS rates beyond what can be achieved through traditional laparoscopic surgery alone.6,7 These types of findings, combined with ongoing innovations in RAS, continue to emphasize the potential of robotics to drive improvements in patient outcomes, and are further driving the adoption of RAS globally.
The advantages of RAS for surgeons are obvious: improved dexterity, greater precision, enhanced vision, and improved ergonomics. “Surgery is considered one of the most resource-intensive areas of healthcare” 6 and the clinical value of RAS continues to be shown beyond the operating room through a variety of indicators such as Length of Stay (LOS) and improved rates of Same-Day Discharge (SDD), complications, and readmissions. However, these conventional indicators generally fall short of measuring the far-reaching impacts of RAS on health systems. The improved outcomes associated with RAS, 6 coupled with its technical features, 8 can also be linked to operational efficiencies and cost savings in the hospital and across the system.2-28
As RAS programs in Canada continue to mature, a growing body of evidence is revealing the many impacts and benefits of RAS. Outside the hospital setting, we are starting to understand the nature and diversity of RAS outcomes in areas such as patient recovery, patient well-being, system capacity and resiliency, training and education, hospital efficiency, and health human resources. We are also learning about the Canadian-specific barriers and facilitators associated with equitable access to RAS, including those related to procurement, adoption, and implementation, and how these factors affect decision-making.
Discussion
RAS in Canada
The United States, the United Kingdom and Australia have adopted RAS more quickly than Canada.29,30 In much of Western Europe and the United States, MIS accounts for more than 70% of all surgical procedures. 29 Over the past decade the adoption of minimally invasive robotic-assisted surgery in Canada has grown slowly, driven mostly by urology and gynecologic-oncology procedures. 31 The potential to leverage RAS to drive improved outcomes in thoracic and general surgery has yet to be fully optimized in Canada. 31
As of February 2025, there were 39 Canadian sites performing RAS with the da Vinci robotic surgical system (Figure 1). Of these programs, seven hospitals have more than one da Vinci system. In 2024, four Canadian academic hospitals introduced da Vinci RAS programs: the Montreal General Hospital (Quebec); Sunnybrook Health Sciences Centre (Ontario); Thunder Bay Regional Health Sciences Centre (Ontario); and Winnipeg’s Health Sciences Centre (Manitoba).
31
da Vinci RAS programs in Canada.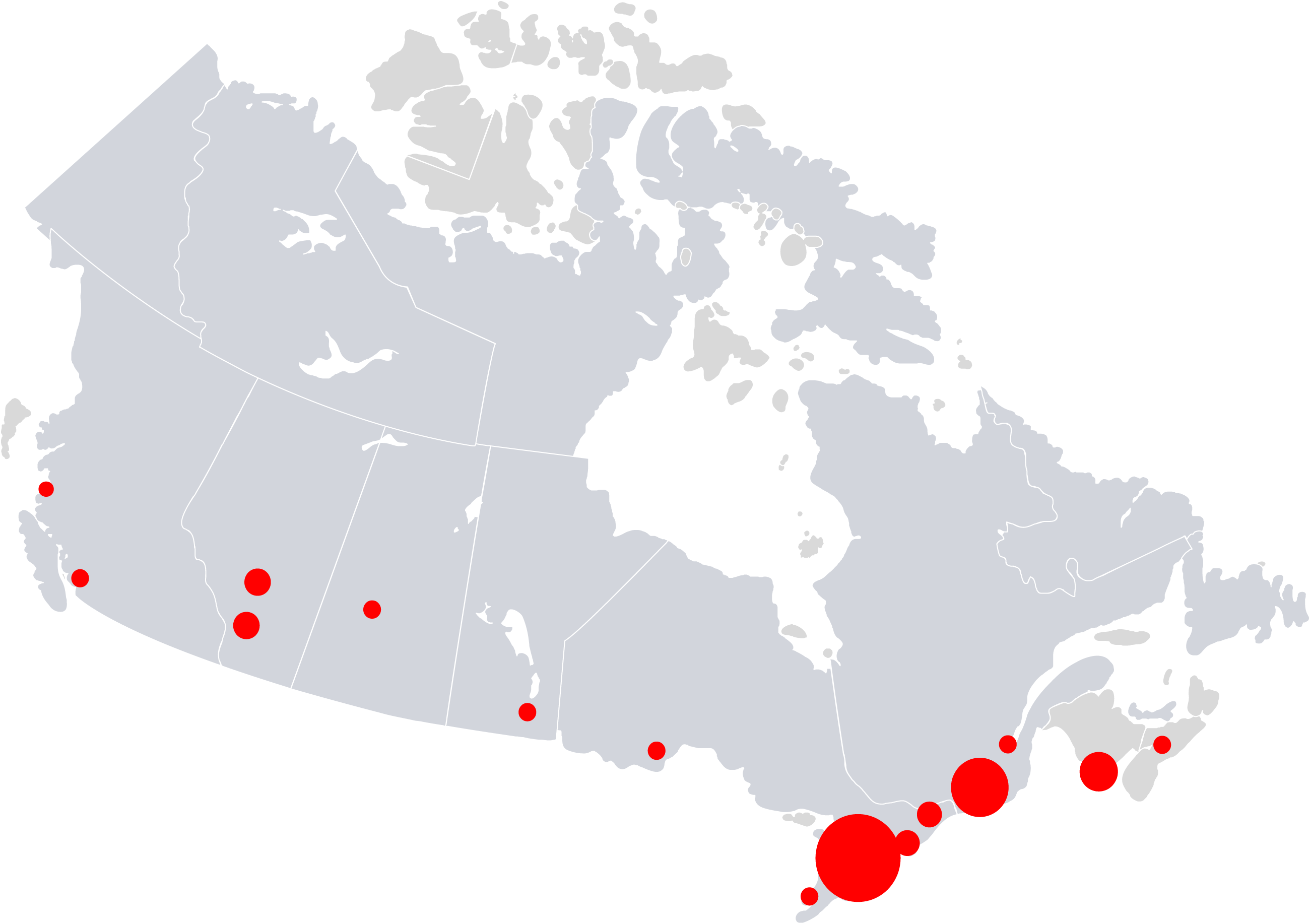
Clinical benefits
Global evidence confirms that RAS enables higher rates of MIS and leads to improvements across a wide range of clinical and perioperative outcomes.
6
Surgeons report that RAS helps them access the target anatomy and perform precise movements in ways that wouldn’t be physically possible with traditional laparoscopic surgery. The improved dexterity and visualization with RAS may allow surgeons to take on more challenging cases that would have been performed by laparotomy or converted to open surgery prior to the introduction of robotics, even in patients with a high body mass index and in the elderly.32-43 Compared to laparoscopy and open surgery, RAS can result in fewer blood transfusions, lower rates of 30-day complications, and fewer 30-day readmissions.
6
Reductions in the number of complications and decreased length of stay are helping hospitals increase capacity, achieve efficiencies, and expand into other clinical service lines (Figure 2). Clinical value of robotic‐assisted surgery. Results are based on The COMPARE Study – a meta-analysis of peer‐reviewed literature covering period 2010-2022 for robotic‐assisted procedures completed with the da Vinci® Surgical System.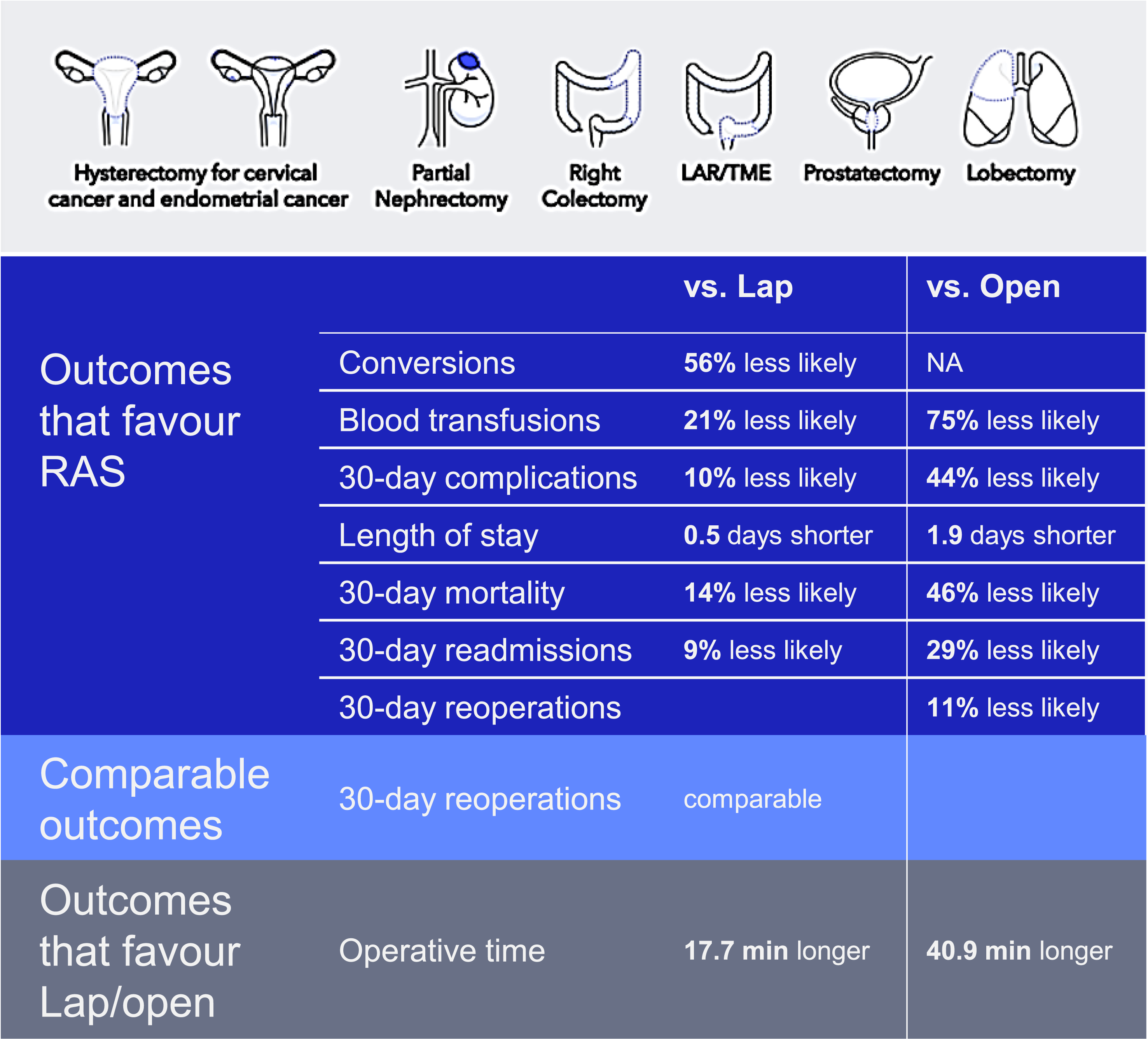
The Canadian evidence base for RAS is growing, and the outcomes are impressive. • In gynecology, Quebec surgeon researchers report robotic hysterectomy, compared to open surgery, was associated with fewer complications, less postoperative analgesic use, and faster recovery, without compromising recurrence rates or survival.
25
• In colorectal cancer, an Ontario study demonstrated that RAS reduced rates of conversion and increased overall MIS rates from 47% to 85%. RAS also reduced LOS and emergency department visits.
20
• Robotic lung resection is associated with a lower rate of conversion to thoracotomy, reduced LOS, and a lower rate of respiratory failure. Patients are more likely to be discharged to home compared to patients undergoing Video-Assisted Thoracic Surgery (VATS).
35
• In kidney cancer, a national study reported that robotic surgery was associated with increased use of partial nephrectomy and minimally invasive partial nephrectomy.
44
“Robotic partial nephrectomies reduced major complications and decreased LOS by half compared to open surgery. Partial nephrectomies preserve kidney function, lowering the risk of cardiovascular events, and make patient’s health better in the mid- and long term.” – Dr. Ricardo Rendon, Queen Elizabeth II Hospital, Nova Scotia Health
RAS: A value proposition for health leaders
Several Canadian sites are taking innovative approaches to optimizing their RAS programs and seeing notable results in diverse areas. • At Centre Hospitalier Universitaire in Québec (CHU), they are taking a transdisciplinary and collaborative approach to implementing RAS. Surgeons from several specialities, as well as medical directors, are included in all aspects of RAS program development, from initial design to establishing criteria, setting and measuring indicators, assessing cost, and evaluating outcomes. The team meets once a year to exchange information from across the CHU network and to plan ways to optimize RAS, including potentially expanding to new sites and specialities. • Horizon Health Network (Horizon) in New Brunswick has allocated robotic Operating Room (OR) time to urology and thoracic specialities. The learning curve for the RAS technology meant that procedures initially took longer, but by four months after implementation, robotic partial nephrectomies were 50% faster than laparoscopic. Reduced procedure duration, combined with efficiencies like reduced LOS, has allowed Horizon to add cases and repurpose 14 surgical beds, reassigning them to create 24 family medicine beds.
68
• Lois Hole Women’s Hospital in Edmonton, Alberta, achieved a 78.3% same-day discharge rate in patients with endometrial cancer undergoing robotic hysterectomy, without compromising patient satisfaction (98.2%) or impacting rates of readmission or presentations to the emergency department.
45
• At St. Joseph’s Health Centre Hamilton in Ontario, 60% of patients undergoing robotic prostatectomy are now discharged the same day, improving LOS rates.
46
“Robotic thoracic has dramatically changed our number of days in step-down units. So it opens up critical care beds for other services that may need it.” – Dr. Bobby Shayegan, St. Joseph’s Healthcare Hamilton
Benefits for patients
Value-based healthcare provides a balance between improving patient health outcomes and controlling costs. When it comes to considering the adoption of innovations like RAS, the shift to a value-based healthcare model gives health leaders license to look beyond short-term costs and focus on the innovation’s impact on quality of patient care.
Comparing RAS to laparoscopic or open surgeries, studies demonstrate benefits of RAS for patients across multiple procedures, including:
RAS may avoid delayed discharges and patient deconditioning. Shorter hospital stays can reduce the risk of hospital-acquired infections and help prevent the physical and mental decline that patients can experience due to even short hospital stays, especially for the elderly.61-65 Further downstream, recovering at home can mean less stress and anxiety for patients and improved well-being and recovery. Faster recovery may reduce patients’ need for home care services, nursing care, and visits from personal support workers. This could result in cost savings and improved efficiencies across the system.
A notable example of the benefits of RAS for patients can be found at St. Joseph’s Health Centre Hamilton in Ontario, the largest robotic thoracic surgery site in Canada. Their surgeons perform minimally invasive robotic lobectomy and have now implemented a robotic segmentectomy program, enabling a more precise and lung-preserving approach for early-stage lung cancer, with goals of improving patient outcomes and recovery.
31
“The recovery for a robotic versus open prostatectomy is dramatically different, particularly in terms of pain and length of catheterization. In thoracics, the incremental value for patients is significant. Robotic thoracic surgery reduces the volume of the lung that’s removed for a small lesion. With a segmental or sub-segmental resection, patients retain a lot of their lung tissue. Patients’ recovery is dramatically different.” – Dr. Bobby Shayegan, St. Joseph’s Healthcare Hamilton
Health human resources
Resource allocation
Approximately 40% of hospital spending is attributable to nursing care and support services in inpatient settings. 66 Improvements to SDD and LOS can translate to more efficient human resource allocation across all disciplines and services, including medical professionals, personal care attendants, patient care aides, food services, orderlies, and housekeeping.
The da Vinci RAS system allows the surgeon to precisely control four robotic arms, increasing surgeons’ ability to perform more of the surgery on their own. Surgeon autonomy means hospitals can introduce new staffing models based on case complexity. Some health systems are optimizing existing OR staff by scheduling da Vinci surgeries early in the day to maximize day-shift staff (front-loading) and by introducing “flip rooms”—alternating one surgeon who operates between two rooms, with two separate OR teams. 67
Workflow and efficiency
A structured implementation and governance framework can help RAS programs achieve improvements and realize efficiencies by redistributing hospital resources.
For example, when implementing a RAS program, hospitals generally choose to limit RAS access to a select few surgeons. Providing consistent access helps surgeons overcome the learning curve more quickly and bring them to full practice sooner. Having a dedicated robotic OR in place when the program is first implemented is an important strategy to support the success of RAS implementation. A dedicated OR may enable efficiencies, such as faster docking and faster turnover of the OR.
Typically, staffing for open or laparoscopic surgeries involves the primary surgeon, first assistant, scrub technician, and a circulator nurse. With RAS, staffing in the OR can be re-organized. A 2023 analysis of open versus robot-assisted partial nephrectomies revealed that the median total nursing times were significantly lower after adopting robotic surgery. The authors concluded that this “led to a measurable relief for the nursing staff and clearly represents a previously unknown cost-saving mechanism.” 14
Key performance indicators being monitored by Horizon show that introducing RAS has led to many improvements. 68 For example, robotic partial nephrectomies are 50% faster than laparoscopic, and embolization—common with open and laparoscopic procedures—did not occur with robotic procedures. Other benefits include fewer readmissions and averting narcotic/opioids post-operatively. After launching RAS, Horizon has achieved a zero-complication rate on robotic partial nephrectomies and is now considering discharging these patients sooner than the current two-day stay. 68
RAS is shown to increase rates of SDD in prostatectomy and hysterectomy.45,46,69,70 At Horizon, robotic prostatectomy cases may be discharged home directly from the post-anesthesia care unit, avoiding an inpatient stay and creating capacity for additional surgeries. As an added benefit, simplifying admission procedures for short-stay robotic prostatectomy cases at Horizon has reduced paperwork by 75% for these procedures and lessened the administrative burden for staff.
68
“From an optimization point of view, we really try to focus on those surgeries that have a clear patient benefit. In doing that, you’re not losing that efficiency that you've gained: it’s that you’re being selective on the cases you’re choosing to be done on the robot.” – Amy McCavour, Horizon Health Network
Attracting and retaining surgeons
Globally, RAS is now a routine part of training for many surgeons.71-75 The largest surgical residency programs in the United States use da Vinci robotic surgical systems in specialities including urology, gynecology, general surgery, thoracic, and head and neck.76,77
Many health leaders in Canada are actively working to acquire additional systems to expand RAS to more patients and across more procedure types. However, hospitals are challenged by how to provide consistent access to RAS when they have more surgeons than available technology. While waiting to acquire RAS technology, hospitals are unable to provide access to additional surgeons without compromising or reducing access for those surgeons already performing RAS (Figure 3). Growth in number of surgeons performing da Vinci RAS in Canada.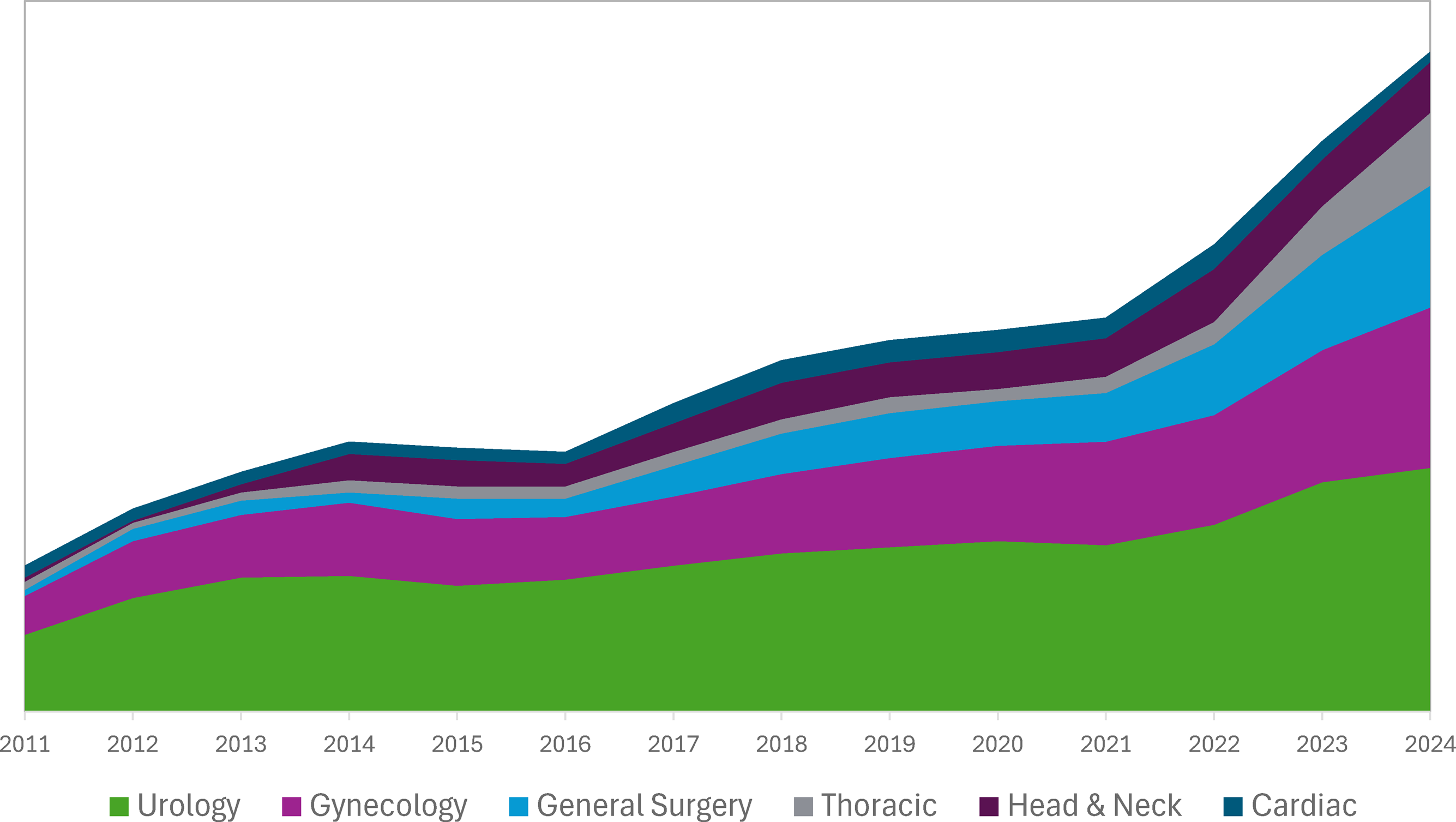
The lack of access to RAS OR time creates cascading problems related to training, recruitment, and retention of surgeons. Most surgical residents believe RAS is a required skill set and seek out residency programs offering RAS. 78 However, given the limited access to RAS in Canadian programs, some physicians may choose to pursue surgical residency or fellowship programs outside the country. After completing their training, surgeons trained in RAS will likely endeavour to practice at hospitals where they can use their RAS training regularly, but may not be able to use their RAS skills due to lack of availability of RAS systems or RAS OR time. Some RAS-trained surgeons are leaving for hospitals that have more access to RAS—even looking to the United States—and Canada is missing out on talent, capacity, and surgeon mentorship across the system.
L’Hôtel-Dieu de Québec, an organization of the CHU in Québec City, is taking a proactive approach. Some of their surgeons leave Québec or Canada to pursue a fellowship in RAS. When they return, surgeons participate in a CHU hospital-based program that includes a gradual approach to performing RAS surgeries along with peer evaluation from RAS-trained surgeons. In keeping with its organizational values, CHU has established a risk management strategy as part of the program to maintain high quality and safety standards. CHU’s multi-faceted, collaborative RAS program is resulting in effective teamwork, efficient mobilization of knowledge, improved surgeon engagement and retention, and an increase in surgical capacity. “We have comprehensive training for new surgeons who want to use robots. First, they observe other RAS surgeries here, even those outside their speciality or domain, and then we send our surgeons to be trained elsewhere—in Canada, the United States or France. When they come back to CHU they are not only fully trained, but also open and eager to teach their peers.” – Martin Beaumont, CHU de Québec
Surgeon ergonomics and career longevity
Evidence is showing the positive impact of RAS ergonomics on surgeons’ career longevity.79-83 Compared to open and laparoscopic, robotic surgery is linked to decreased feelings of burnout. 80 Performing traditional laparoscopic surgery involves standing and staying in uncomfortable postures for extended periods of time. Approximately 87% of laparoscopic surgeons have reported physical symptoms or discomfort in the neck, shoulders, back, knees, ankles, and feet.84,85 Studies show the prevalence of neuromusculoskeletal disorders is significantly lower in surgeons who perform RAS compared to other surgical modalities.79-83
To alleviate the pain and stress that results from performing surgery, surgeons may consider treatments and strategies that include pain medication, physiotherapy, practice modifications, a leave of absence, and even early retirement. 81 Improved ergonomics associated with RAS may reduce the risk of surgeons’ work-related injuries and burnout, potentially avoiding surgeon early retirement due to health reasons.79-81
Health equity
Challenges: Access to care
RAS is considered highly specialized and is often concentrated in larger urban and academic centres. Although RAS is emerging as a standard of care for select procedures in some provinces, access to RAS is not equal across the country. 31 For rural-based patients who need to travel far from home to benefit from the substantial advantages of robotic surgery, disparity in access is a very real barrier.
Travel burden relates directly to health equity. A 2024 analysis from the Canadian Institute for Health Information 86 shows that 51.3% of rural or remote patients experience a high or very high travel burden for advanced care requiring complex surgical interventions such as RAS. Patients travelling far from home to receive specialized care must deal with the logistics, time, and cost of transportation and accommodation for themselves and their caregivers, at a time when they may be particularly vulnerable. As well, some hospitals use an alternative care pathway for patients needing to travel long distances for RAS. This may mean higher direct costs due to overnight stays versus a same-day discharge pathway that might be available to local residents.
Tackling the equitable access issue
Digital innovations such as tele-mentoring and remote access can help overcome systemic and structural barriers to MIS across Canada. 87 The technology can support surgeons in rural regions to train and collaborate with more experienced surgeons, enabling the introduction of RAS in new settings and increasing access for patients.88,89
Alberta Health Services (AHS) has developed a novel approach to the RAS equity challenge. Allocation decisions go beyond considering how many people live where: it’s about planning the efficient distribution of resources related to medical needs and wants. AHS has 16 major hospitals—most of which are in urban centres—that do 93% of their surgical volumes. Patient and provider data is collected from those 16 sites to determine how the clinical and program outcomes for RAS compare to open and other MIS approaches. AHS strategic planning and decision-making considers: • What procedures are being done? Which surgical modalities are being used, and for which patients? • Is RAS used for the right procedures and patients? • What is the corresponding clinical pathway and what are the clinical outcomes? • Is RAS being used to its optimum capacity? • Should RAS be concentrated at a major urban hospital? Can some RAS procedures be safely delivered closer to home for rural patients? • What are the requirements for clinical and operational teams to implement and sustain a high-quality RAS program? • What is the minimum access to RAS required for surgeons to maintain standards of quality and safety?
Once procedure types and volumes have been analyzed, AHS leaders examine various operational considerations such as the physical OR space, sterile reprocessing, and workforce. AHS uses a layered governance model to integrate information, facilitate collaboration, and distribute decision-making across the levels of site, zone, and province. This holistic and evidence-informed approach helps AHS plan the appropriate expansion of services and determine where and how to introduce new RAS programs.
Challenges: Access to funding
Traditionally, Canadian hospitals partner with hospital foundations to fundraise for high-value, innovative capital items like robotic surgical systems. Large high-profile academic-affiliated hospitals have access to a variety of foundation, charitable, and philanthropic avenues to support the adoption of innovation, while smaller or rural facilities may lack these supports—further demonstrating and reinforcing inequity in access to specialized care like RAS. “Funding robotic surgery through foundations has to become, at some point, a thing of the past. RAS is no longer an innovation; it’s a standard of care.” – Dr. Ricardo Rendon, Queen Elizabeth II Hospital
A Canadian perspective, an innovative solution
Given all these parameters, experts agree a fresh approach is required to support the adoption of technology that can bring meaningful benefits to patients. Health professionals no longer consider RAS an optional “nice to have,” but rather, a necessary tool for providing high-quality surgical care. Canadian health leaders are urged to investigate and recognize the far-reaching benefits of RAS and adopt it as a standard of surgical care, as other jurisdictions have done.
Systems-thinking requires health leaders to challenge the status quo and look beyond traditional metrics and budget silos to embrace an integrated, systems approach to evaluation, strategy, and expansion. Historically, the adoption of innovation has centred on capital acquisition, disconnected from administration and operations. Taking a value-based healthcare approach to the adoption and expansion of RAS requires a shift to how health systems acquire the technology and how they can redistribute operating funds to facilitate the adoption of RAS technology that improves the quality of surgical care.
Ontario and Quebec are paving the way. Both provinces have introduced supplemental funding for select RAS procedures, supporting their hospitals that have chosen to adopt RAS technology to drive change and improve patient outcomes.90,91
Intuitive Surgical Inc. (Intuitive) offers an innovative, usage-based funding model that allows hospitals to acquire da Vinci RAS systems without having to pay the full cost of the RAS technology up front. Instead of the traditional method of procurement through capital purchase, hospitals can acquire and sustain RAS technology through a usage-based “pay as you go” funding arrangement. The cost of RAS technology can be covered by an organization’s operating budget, without having to rely on foundation funding.
The usage-based model is fiscally responsible and allows hospitals to minimize up-front costs and manage cash flow effectively when acquiring RAS technology. Depending on the provincial funding model, this usage-based funding arrangement is potentially cost-neutral for operational budgets. Additionally, the model enables hospitals to keep pace with rapid technology innovations and easily upgrade to new technology to avoid technology obsolescence. Intuitive’s funding model includes training and proctoring costs and is tailored to hospitals and hospital networks that have identified RAS as a strategic initiative. “You can’t necessarily say that all robotic systems are created equal just because they do robotic surgery. It's not generically about RAS; the majority of the evidence comes from the da Vinci system, which is the most mature, the most well published, and with the deepest set of literature. My surgeons like to work with those that are consistently innovating and have the tools available.” – Dr. Tara Klassen, Alberta Health Services
Conclusion
Increasing value requires improving quality and/or decreasing costs. Health leaders are discovering that RAS, when compared to open and laparoscopic surgeries, can improve outcomes, quality, and efficiency. Despite higher costs of robotic consumables, improved outcomes associated with RAS procedures can increase capacity, decrease length of stay, and reduce complications. 6 The efficiencies generated from improved outcomes can offset the costs of introducing or expanding a RAS program—a crucial consideration for those working within Canada’s publicly funded healthcare system.
With RAS, surgical staff are practicing to a high professional level and continually enhancing skills. Well-rounded RAS training programs can foster increased engagement, higher job satisfaction, collaborative teamwork, and sustained knowledge mobilization.
The adjustments to staffing models afforded by RAS can support the efficient redeployment of health human resources to other needs within the hospital and throughout the system.
Health leaders in Canada, including those in Alberta, New Brunswick, and Quebec, are using innovative approaches to expand existing RAS programs and introduce new RAS programs. When adopted and supported by leadership, business model innovations—like Intuitive’s funding model for RAS programs—can help tackle the root causes of inefficiency, introduce sustainable change, and enhance value for all stakeholders.
Patients and the health system can benefit when high-quality RAS is delivered, especially when it’s available closer to home. With Intuitive’s innovative “pay as you go” funding model, health leaders can explore options for acquiring state-of-the-art robotic-assisted surgery systems regardless of location and deploy RAS to deliver better value, improve the quality of care, and expand access to minimally invasive surgery for patients. “Introducing robotics needs to be cross-functional. We want the urologist to share their experience with the general surgeon and the gynecologist. Adopting and sharing best practices is definitely an important element, not only from a clinical perspective, but also from a managerial approach. I believe there is a great opportunity here to set up a RAS community of practice to share knowledge, optimize the use of robotic surgery, and create more value for our patients.” – Martin Beaumont, CHU de Québec
Intuitive Surgical Inc. is a pioneer in RAS and maker of da Vinci surgical systems. Since 1995, more than 66,000 surgeons around the world have been trained on da Vinci systems, with more than 16 million surgical procedures completed. 31
Visit Intuitive Surgical for more information on da Vinci robotic-assisted surgery technology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional review board approval was not required.