
Abstract
With an anticipated increase in breast screening volume, provincial healthcare systems and health leaders must identify innovative technologies and care pathways that can alleviate the burden of an already resource-constrained healthcare system. The solution explored here utilizes vacuum-assisted technology that is clinically equivalent and a more cost-effective alternative care pathway, as successfully demonstrated in many other countries. This article reviews the clinical efficacy of Vacuum-Assisted Biopsy (VAB) and Vacuum-Assisted Excision (VAE) and calculates the potential Canadian direct cost savings by implementing VAE for the management of benign and high-risk breast lesions in place of Surgical Diagnostic Excision (SDE): calculated to be $1,607,769 to $11,341,107 (2025 CAD) annually in Canada, or $2,208 (2025 CAD) per-patient procedural savings from avoiding SDEs. Additional non-quantifiable patient benefits are also explored: avoiding unnecessary surgery; preventing the associated anxiety and time off work; and greater patient autonomy over their diagnosis journey, helping maintain their quality of life. Finally, barriers to adoption are identified, and an Implementation Leadership Action Plan is proposed, to help support the successful integration of this practice shift. The plan includes procedural reimbursement and policy changes, and multidisciplinary engagement targeting radiology, surgery, and pathology stakeholders.
Introduction
The aim of any cancer screening program is early detection prior to symptoms, enabling early treatment and more favourable prognosis. Screening mammography reduces advanced breast cancer incidence by 25% and decreases 10-year fatality rates by 41% among screened women aged 40-69 years.1-3 Younger women are more likely to develop aggressive breast cancers, contributing to a poorer prognosis. 4 A recent Canadian publication found an increase in breast cancer incidence rates in most age groups 20-54. 5 Many provinces have decreased their minimum screening age from 50 to 40, 6 aligned with recommendations in the United States (US). 7 This decrease in screening age is especially important for minority populations who are often diagnosed with breast cancer younger than white women—with a peak incidence in their mid-40s 8 —and are often diagnosed at more advanced stages of the disease. 9
Reducing the screening age leads to finding more and smaller lesions with mammography, enabling earlier intervention. However, screening can also result in overdiagnosis and overtreatment of benign lesions that might never develop into cancer. When implementing changes into a provincial health program, health leaders must balance screening age and frequency with resource availability and the probability of overdiagnosis and overtreatment. Breast cancer screening can cause anxiety for patients as they wait for results, repeat tests due to inconclusive findings, surgical referrals, preoperative appointments, and surgery (Schematic 1(A)).
10
Almost all Canadian provinces are already well behind their predefined time to diagnosis indicators: ≥ 90% diagnosed within 5 weeks when no biopsy is required and ≥ 90% diagnosed within 7 weeks, when a biopsy is required.
11
Care pathways are needed that can handle increased screening volumes and alleviate an already resource-constrained healthcare system.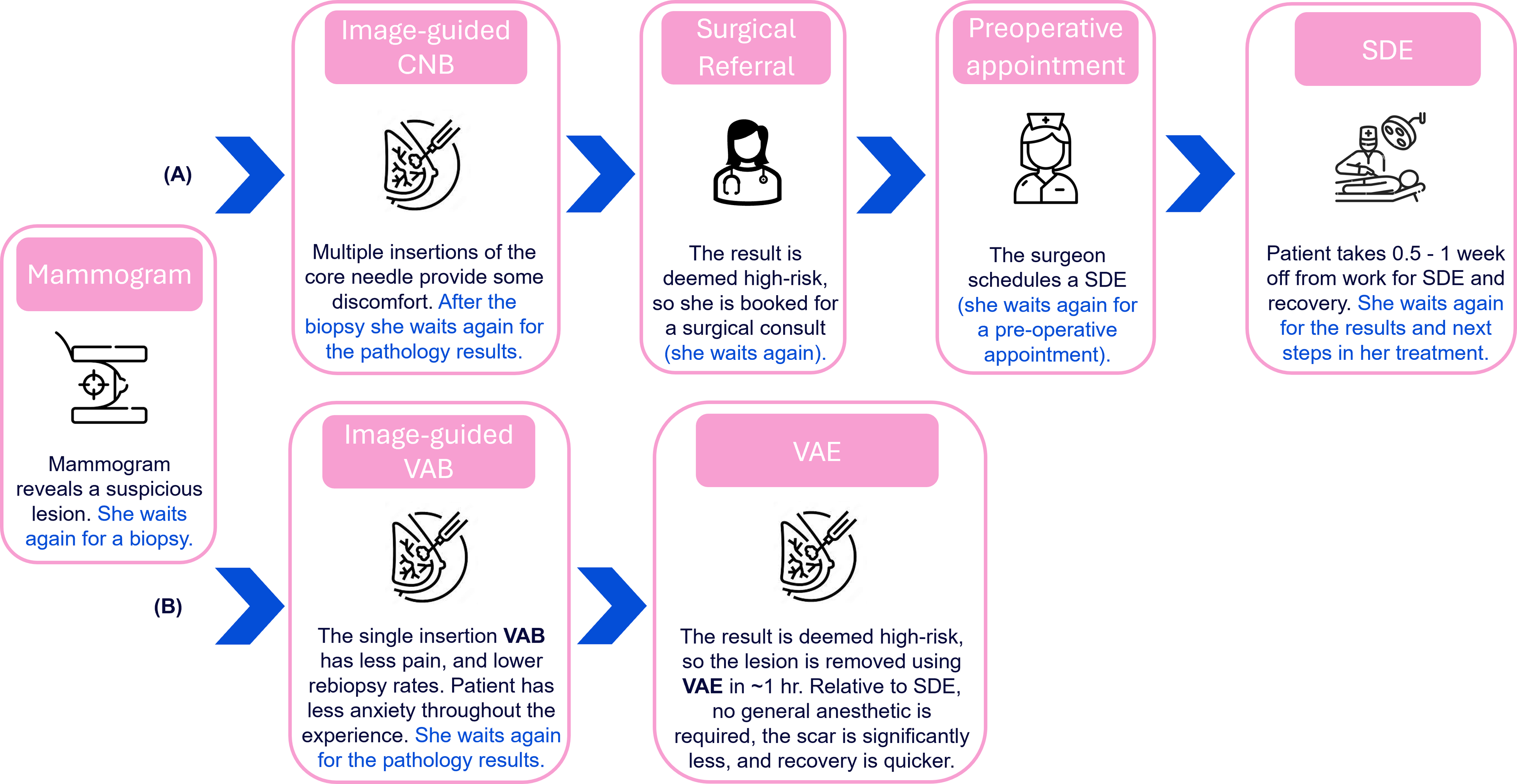
Provincial healthcare systems must more quickly adopt innovative, less invasive technologies that improve quality of life, especially for younger women entering the screening program, who have an increased risk of false positives. 12 This article explores an alternative breast care pathway using Vacuum-Assisted Biopsy (VAB) and Vacuum-Assisted Excision (VAE) to streamline patient care. It highlights potential economic savings to Canada, based on analyses performed in similar healthcare systems. 13 Finally, it proposes a leadership action plan to support health leaders in implementing this change effectively.
Innovative technologies and care pathways using vacuum-assisted technologies
Although VAB is standardized practice for certain types of lesions (e.g., for calcification-containing lesions without mass, and for MRI-guided biopsies),14,15 VAB still does not receive the appropriate level of reimbursement to compensate for its use. The goal of a biopsy in breast diagnosis is to obtain small cores of tissue for pathological evaluation, which can be achieved with VAB or without it (designated as Core Needle Biopsy or CNB). Ultrasound-guided CNB is one of the most-used procedures for breast cancer diagnosis due to its relatively quick, inexpensive nature and the availability of imaging technology in most imaging clinics.16,17
Although CNB is adequate in many cases, it does have limitations, particularly because it yields smaller specimens compared to VAB. This limitation necessitates multiple needle insertions for adequate sampling, which is uncomfortable for the patient, and can still result in undersampling of the lesion.18-20 In contrast, VAB uses vacuum suction and a cutting needle, which produces a more contiguous sample than CNB and typically requires only a single needle insertion.19-21 The sample size retrieved by VAB is larger in volume than that retrieved by CNB, resulting in better lesion characterization, less histological underestimation,21,22 a reduced likelihood of non-diagnostic or indeterminate findings, higher specificity, 23 and fewer repeat biopsies. 22 Furthermore, patients report less pain 24 and higher overall satisfaction with the procedure. 25
A 2023 retrospective analysis of over 31,000 breast cancer patients suggests VAB may be associated with improved survival outcomes compared to CNB in higher-stage breast cancers. 26 These findings remain controversial and require further validation through prospective studies.
High-Risk Lesions (HRLs) are findings of uncertain malignant potential that may be associated with elevated likelihood of cancer. These benign lesions carry an increased potential for harbouring undetected cancer cells, which typically can only be confirmed through Surgical Diagnostic Excision (SDE) following the initial biopsy. VAE can be leveraged to remove these lesions entirely or to obtain a large enough sample to replace or eliminate the need for SDE, 27 allowing many women to avoid surgery. 28 VAE is a minimally invasive procedure, which carries a lower risk of complications, a shorter recovery time, improved cosmetic outcomes, and less pain for the patient.29,30 The use of VAE for managing HRLs has been shown to be both clinically and cost-effective in many European countries.13,31
UK VAE experience
In the early 2000s, the UK National Health Service Breast Screening Programme assembled a multidisciplinary group of radiologists, surgeons, and pathologists, with the aims of reducing overtreatment and benign surgical biopsies, and maximizing preoperative diagnosis of cancer. 32 The group agreed that leveraging vacuum-assisted technologies for both diagnostic and excisional purposes would enable preoperative diagnosis, minimize risk of overtreatment, and allow for patient-centred care. Specifically, VAE was utilized to remove several HRLs (in Europe called B3), 32 replacing SDE, and shifting care from breast surgeon to radiologist. Traditionally, HRLs that have been diagnosed on initial (percutaneous) biopsy by the radiologist have been recommended for SDE, as they are upgraded to breast cancer in 5 to 25% of these surgeries, depending on the specific type of HRL.33-39
Following this shift in practice, several retrospective analyses have shown that breast surgery can be safely and cost-effectively avoided in select HRLs with and without atypia.13,31,34 A 2021 study 34 demonstrated that 73.8% of HRLs with atypia and 65.1% of HRLs with no atypia underwent VAE rather than surgery. More recently, McLachlan et al. 33 demonstrated that surgery was avoided in 79% of women with HRLs utilizing VAE, and only 5.1% were upgraded, suggesting that considerable time and resources could be saved avoiding SDE unlikely to change management. Aligned with the UK, International guidelines40,41 recommend VAE as an alternative to surgery and continue to expand the types of HRLs that are recommended for VAE, including Atypical Ductal Hyperplasia (ADH).
Applicability to Canada
Canadian physicians recently took a similar approach to that of the NHS, forming a multidisciplinary working group of radiologists, surgeons, and pathologists to review the latest evidence and provide recommendations for Canadian practice. 42 While they recognized VAE as an appropriate care option for several HRLs, their current guideline to obtain surgical consultation before proceeding with VAE may limit some of the potential time and resource efficiencies that this approach could otherwise offer. A more effective approach, consistent with European practice, would be to implement a multidisciplinary program that coordinates various patient options in a streamlined manner (Schematic 1(B)).
Convinced by the most recent European guidelines and data, health leaders at BC Cancer Vancouver Centre are taking a forward-looking approach and have begun offering VAE to patients and referring surgeons: a practice that will initially be done at a loss until reimbursement catches up to current-day practice and clinical efficacy.
Economic impact in Canada of utilizing vacuum-assisted technology
If all provinces expanded screening to include women aged 40-74, an estimated total of 2,058,796 women would attend screening annually.43-47 With a biopsy rate of 1.52% (based on British Columbia, Ontario, and Nova Scotia), this would result in approximately 30,210 biopsies per year.45-48 Yashima et al. 49 found that 4.82% of CNB and 2.36% of VAB require a rebiopsy—equating to 1,455 and 713 additional procedures, respectively. Using VAB in place of CNB could therefore reduce rebiopsies by 742, translating into potential annual savings of $739,025 (2025 CAD), based on a reduction in rebiopsy per-procedure cost of $996 (2025 CAD), which includes the cost of physician clinic visit, core needle biopsy, and pathology analysis50,51 (Schematic 2).
Shaaban et al. 52 also recommends using VAE to replace surgery as the standard of care for most HRLs, reporting that HRLs comprise 2.41-17% of breast lesions; a similar percentage of surgical procedures could be avoided by using VAE. Combined with Canadian screening data, this suggests that 728 to 5,136 surgical procedures could be avoided by utilizing VAE, translating to an estimated direct cost savings of $1,607,769 to $11,341,107 (2025 CAD) annually, based on costs of surgeon clinic visits, excisions, and pathology50,51 (Schematic 2). Although this excludes the added cost of a VAE procedure, per-patient procedural savings from avoiding SDE are estimated at $2,208 (2025 CAD).50,51 Costs are converted using the Consumer Price Index (CPI). 51
Internationally, greater per-patient savings of £1,510.75 ($3,252 [2025 CAD]) were reported in the United Kingdom when comparing VAE to SDE, even after factoring in the cost of VAE, based on an analysis of patient resource use from referral to discharge. 13 Similarly, a 2022 Dutch study reported total per-patient pathway savings—including follow-up activity—of €1,979 ($3,214 [2025 CAD]) when VAE was used instead of SDE for managing benign lesions and HRLs. 53 A large US 2020 database study demonstrated significantly lower procedural costs for ultrasound-guided VAE compared to open surgery: $1,750 USD ($1,963 [2025 CAD]) for benign and HRLs, and $2,250 USD ($2,523 [2025 CAD]) for HRLs only. 55 All costs are converted using purchasing power parity for health and CPI.51,56 A 2025 randomized controlled trial from Sweden showed that the total hospital procedural cost of VAE was estimated to be 60% lower than the cost of SDE (P < 0.001). 29
Indirect cost savings not captured in this economic analysis—but important for health leaders to consider—include unnecessary frustration and anxiety for the patients due to extended periods without conclusive outcomes and additional workload for the surgeon. If a patient with HRL is booked for surgical consultation, they often inaccurately believe they need surgery. They experience extended wait times to consult with a surgeon, as they are considered a lower priority than cancer patients. Then a surgeon will often spend more time consulting with these patients, due to surgical misconceptions and less-defined treatment pathways compared to confirmed cancer patients. Implementing an alternative VAE care pathway could alleviate the burden on surgical services and enhance patient care, allowing surgeons to spend more time in the operating room with cancer patients, rather than on consultations and surgeries for non-malignant cases.
Health leaders can support care models that deliver outcomes that matter to patients. VAE enhances quality of life by reducing repeat biopsies, surgical anxiety, and time away from work (Schematic 1(B)). As a minimally invasive outpatient procedure that is typically completed in under 1 hour with regional or local anaesthesia, 57 it removes patient risk associated with general anaesthesia. Cosmetically, VAE offers better results with minimal or no scarring compared to surgery 58 , aligning with system goals for patient-centred efficient care.
Forward-looking
As the role of VAE continues to expand, health leaders should be aware of additional clinical applications of VAE such as the removal of benign lesions at the patient’s request and the potential to remove small breast cancers. A 2021 meta-analysis 59 of 26 studies comprising 18,170 patients found VAE had a 93% complete resection rate for removal of benign breast masses. The authors concluded that VAE demonstrated favourable outcomes in terms of complete lesion removal and low complication rates. The efficacy of VAE to treat small breast cancers is currently under investigation, with many trials underway.60-62 The SMALL trial is a randomized controlled multi-centre Phase 3 trial that compares surgery with VAE for small screen-detected breast cancer. 62 If the removal of malignant lesions with VAE is proven efficacious, developing these new care pathways now for HRLs will significantly accelerate treatment for some cancer patients in the future.
Another advantage of vacuum-assisted technology is its environmental sustainability. Research presented at the European Congress of Radiology (ECR) 2025 showed VAE produces only 7.29 kg of CO2 emissions, compared to 29.56 kg from Magseed-guided surgical excision. While disposal costs of vacuum-assisted needles can be slightly higher than those of standard core needles, VAE procedures require less anaesthesia, fewer supplies, shorter hospital stays, and fewer pre/post-operative visits—making them a viable, sustainable alternative to surgery. 63
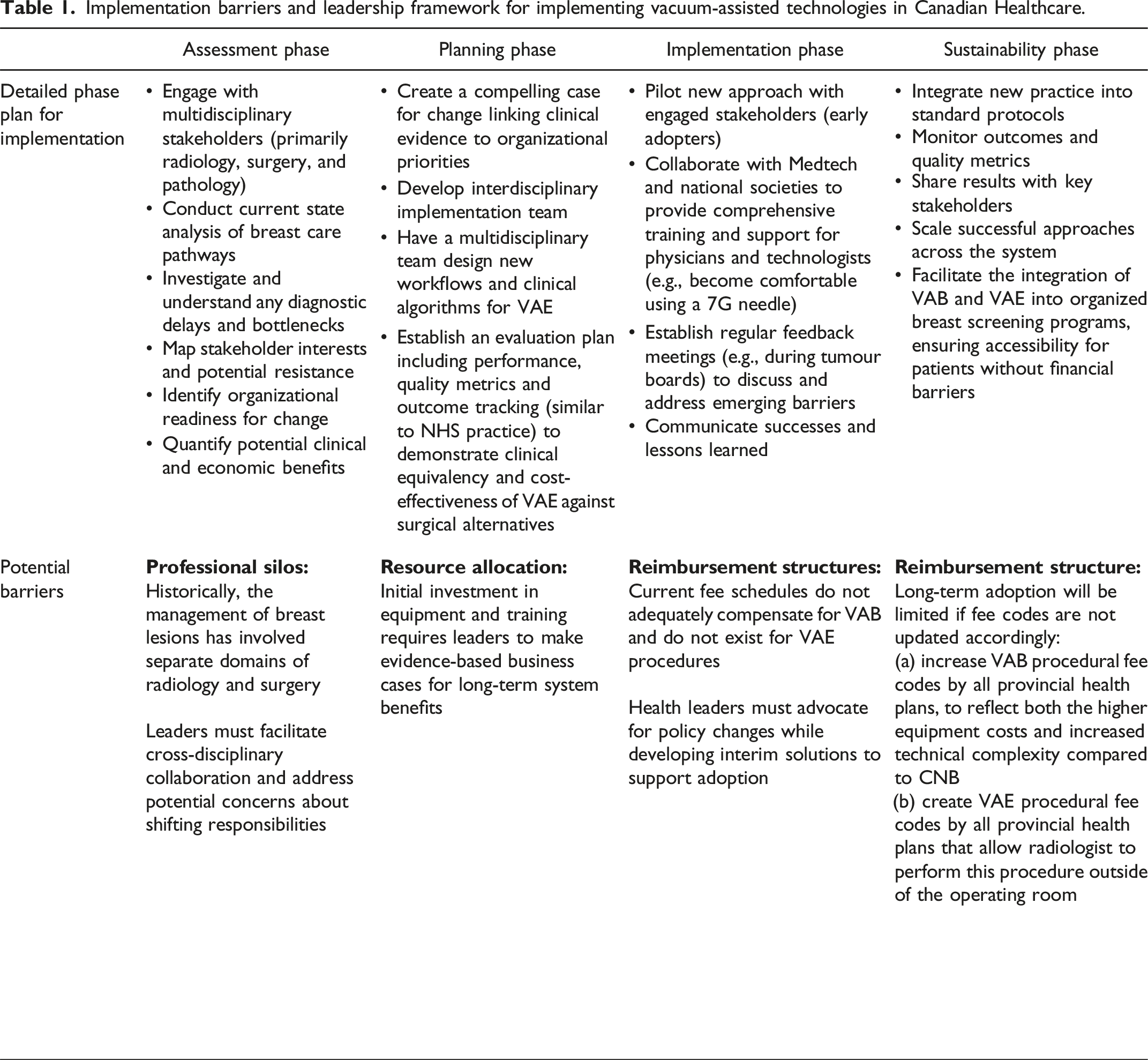
Implementation barriers and leadership framework for implementing vacuum-assisted technologies in Canadian Healthcare.
With growing awareness of the importance of women’s health, and its historic lack of attention, 64 it is time to support Canadian women. 11 Investments addressing the women’s health gap could add years to life and potentially boost the global economy by $1 trillion annually by 2040. 65 Patients’ voices matter. Like all patients, women want a say in their care. They should have access to a range of clinically appropriate options, allowing them to work with their care providers to determine their best pathway.
Take-home messages
The goal of breast imaging is to maximize diagnostic efficiency by ensuring accurate and timely detection while minimizing unnecessary procedures. This includes reducing SDEs, preventing overtreatment, and optimizing preoperative cancer diagnosis. Vacuum-assisted technology conserves healthcare resources while maintaining high-quality patient-centred care.30,31
European public healthcare systems, like ours, have shown that radiologists can manage HRLs using vacuum-assisted technologies, and that VAE is well-tolerated and cost-effective. However, broadscale adoption in Canada will require health leaders to support systematic changes in patient care pathways and appropriate reimbursement for VAB and VAE (Table 1). An estimate of Canadian women screeneda, biopsied,b and rebiopsied if all provinces screening programs began at age 40. Cost savings are also estimated for potential reductions in rebiopsy and surgical procedures by leveraging vacuum-assisted technology.c (a) Assumes the total Canadian women population 40-74 years of age is 8,715,065, which was calculated using 2024 population estimates from Statistics Canada and only includes the following provinces: Alberta, British Columbia, Manitoba, New Brunswick, Newfoundland & Labrador, Nova Scotia, Ontario, Prince Edward Island, Quebec, and Saskatchewan. Screened per year estimates use the screening participation rates for 50-74 years old in 2018-2019 for Alberta, Manitoba, New Brunswick, Newfoundland & Labrador, Prince Edward Island, Quebec, and Saskatchewan applied to the 40-74 years old population estimates from Statistics Canada. British Columbia screened per year numbers are reported for 2019. Ontario screened per year estimates come from the Ontario News Release in 2024 on projected screening numbers with lowering the age eligibility of mammograms to 40. Nova Scotia screened per year numbers are reported for 2021. (b) Province-specific core biopsy estimates were available for British Columbia, Ontario, and Nova Scotia. An average of the rates found in these three provinces was applied to population data from the other provinces for Canadian estimates of core biopsies performed annually. (c) Savings in rebiopsy costs are estimated using 2012 costs equalling $996 for CNB adjusted for inflation to 2025 values. Assumes VAE would be replacing a SDE and using 2012 costs equalling $2,208 adjusted for inflation to 2025 values.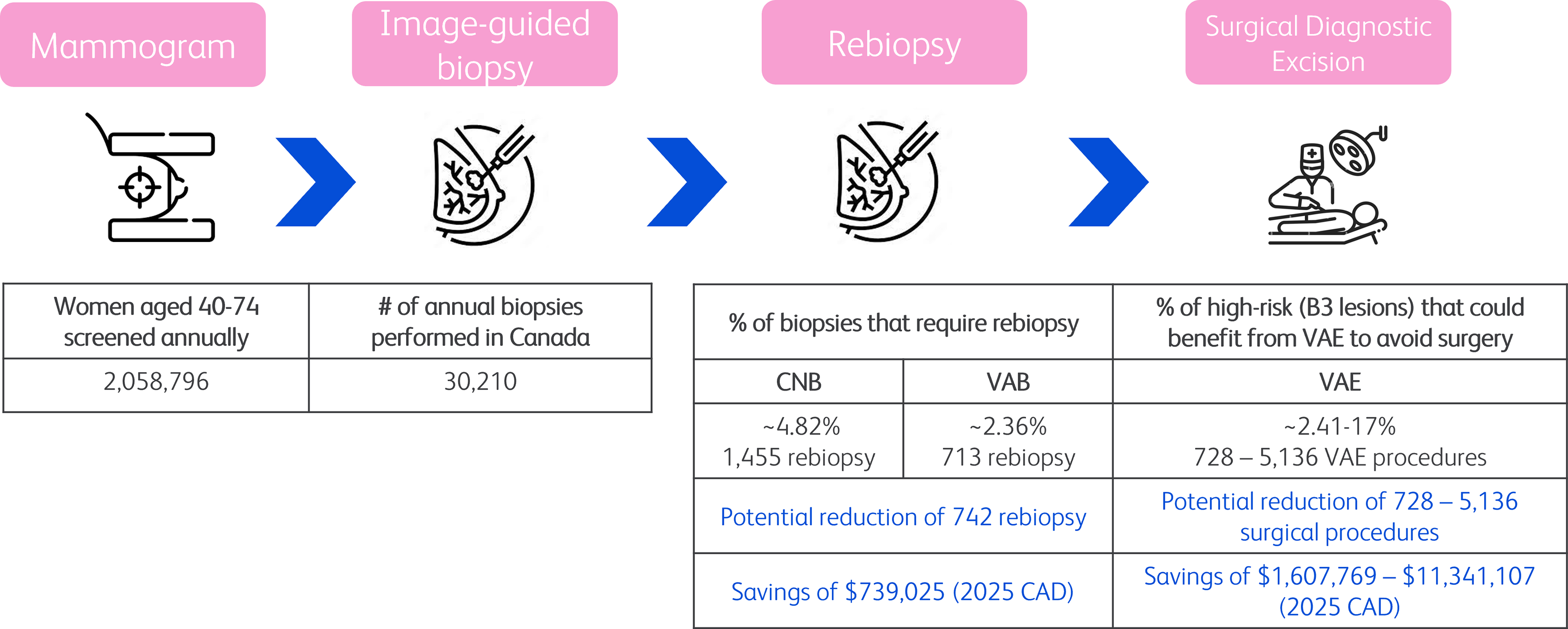
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional review board approval was not required.