
Abstract
This article showcases the high-quality, standardized, and national labour force and health-related data that can be leveraged for effective health workforce planning. It also underscores the importance of interoperability, the ability to integrate and harmonize data from multiple sources to optimize health workforce analysis. Using three case studies drawing on five Statistics Canada data sources, it examines persistent shortages of nurses and personal support workers and the impact of increased workload on their stress during the COVID-19 pandemic. This article also outlines how Statistics Canada data can inform planning by identifying unmet labour demand, work-related stress, and untapped labour resources, such as internationally educated healthcare professionals. It aims to guide health leaders in accessing and leveraging Statistics Canada data, including but not limited to those outlined here, to strategically address workforce and policy challenges in the health sector using an evidence-based approach.
Introduction
Leaders in health workforce planning, both academic and policy, have called for a strengthened federal role in contributing resources to coordinate the collection of accurate, standardized, and more comprehensive data on the health workforce.1,2 Statistics Canada, as the national statistical agency, ensures access to vital information, enabling a comprehensive national portrait across subject areas. This information supports analysis across health occupations and industries and is crucial for enabling more strategic planning for health workforce needs at all levels. While data from provincial and territorial health authorities or agencies may reflect jurisdiction-specific requirements or operational priorities, Statistics Canada collects and processes data that are nationally representative and standardized, a consistent approach to collection from organizations, households, and individuals. For instance, Statistics Canada uses standard classification systems like the North American Industry Classification System (NAICS) 3 and the National Occupational Classification (NOC), 4 to facilitate consistent analysis across statistical programs.
This article presents three case studies, derived from analytical products disseminated by Statistics Canada, that harnessed specific data sources to answer complex and timely questions about the health workforce. These case studies illustrate the types of health workforce data available from Statistics Canada as well as the interoperability of those data, specifically the ability to integrate and harmonize information across multiple sources. They also address key considerations when using such data and underscore the value of standardized concepts and classifications. Together, they demonstrate the potential of Statistics Canada data to enhance understanding of the health workforce in Canada.
Case Study 1: Examining Job Vacancy Dynamics in Health Occupations
Context and Research Objectives
Demand for healthcare continues to rise due to factors such as demographic shifts and an aging population, while supply-side challenges, driven by systemic issues and increased pressure on healthcare workers, are contributing to persistent gaps in meeting population health needs.5-7 In addition to examining healthcare employment data, understanding job vacancy trends, especially at a regional level, can shed light on pressure points within the healthcare system where unmet labour demand may result in stressful working conditions and turnover impacting patients’ access to timely care.1,8
Data and Key Measures
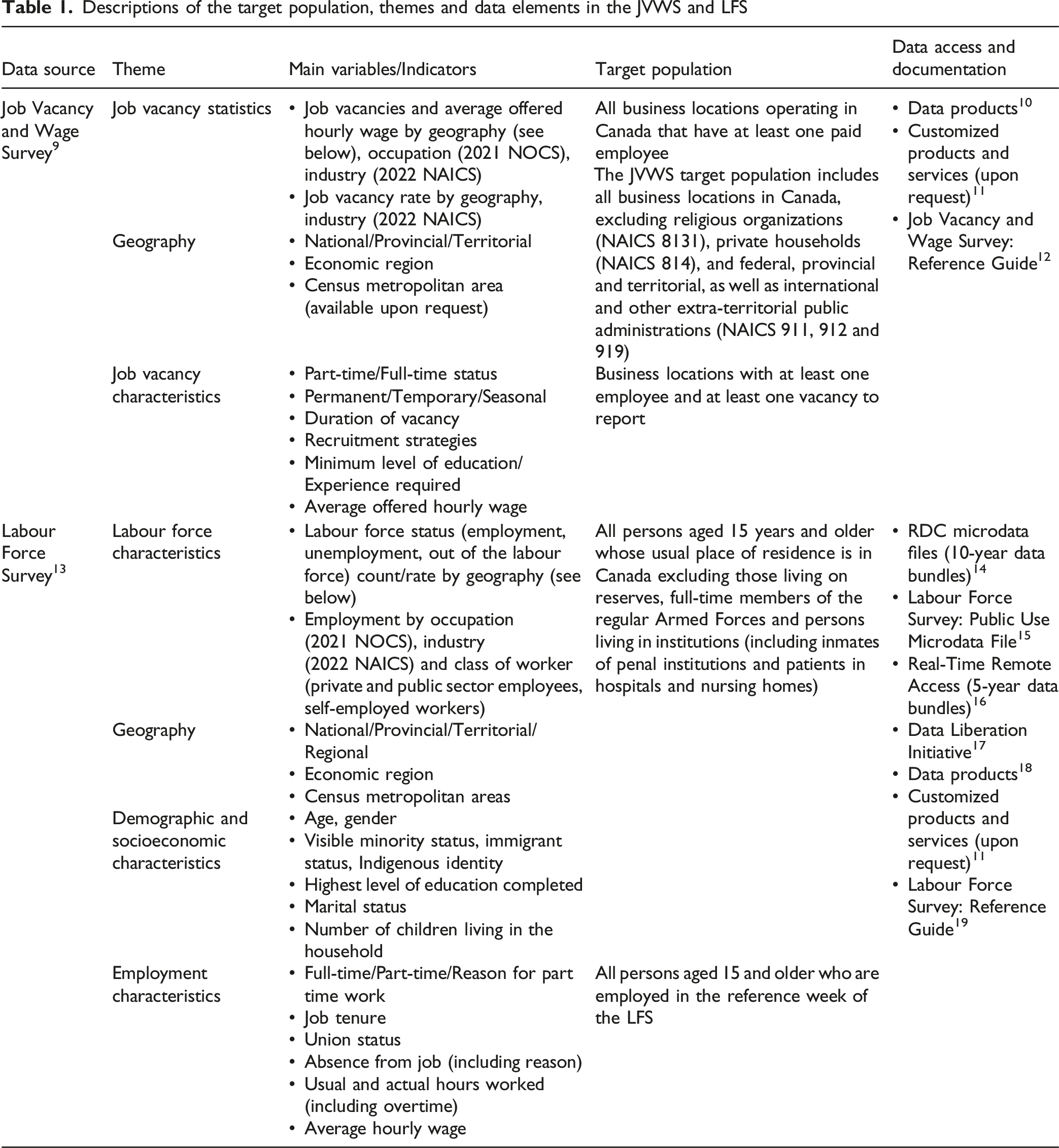
Descriptions of the target population, themes and data elements in the JVWS and LFS
Main Findings
The findings from the study Regional Dynamics of Vacancies in Health-Related Occupations in Canada showed that while employment in health-related occupations continued to grow steadily since 2016, job vacancy rates have risen sharply, from 2.1% in 2016 to 5.8% in 2024. In particular, vacancy rates for nurses and PSWs saw large increases between 2016 and 2024, especially among LPNs, with their 2024 vacancy rate more than five times higher than in 2016. This suggests that increased labour supply has not kept pace with rising demand.
In addition, unmet labour demand for health occupations was not evenly distributed across Canada. For example, vacancy rates for nurses and PSWs were highest in remote areas. While offered wages for nursing positions in remote areas tended to be slightly higher, these vacancies also remained open longer, pointing to persistent recruitment and retention challenges that cannot be explained by wages alone.
Moreover, vacancy trends differed by socioeconomic context where vacancy rates for PSWs and LPNs were lowest in high-poverty areas, whereas rates for registered nurses were highest in those same areas. This may be tied to local supply dynamics that could be explored further while leveraging the LFS and the JVWS to better understand the association between labour demand, geographic factors and material deprivation and marginalization at the regional level.
Value of and Key Considerations in Combining LFS and JVWS Data Sources
The combination of two data sources yielded new insights on job vacancies among selected health occupation groups. Differences in the coverage and classifications between the two surveys led to two main considerations.
To address this first consideration, employment counts from the LFS (Table 1), a monthly survey with information on labour force characteristics by occupation groups, were used to calculate the job vacancy rate, the number of vacant positions as a proportion of all positions (filled and unfilled), after aligning employment coverage with the JVWS, demonstrating interoperability between the two data sources.
The second consideration included defining PSWs in the data. The NOC provides a standardized and structured way of analyzing and reporting on occupational data. However, it may not always provide specificity for certain occupations based on considerations in the architecture and broader purpose of such a standard. Thus, users may need to consider groupings or exclusions to arrive at the required definition. In this case, the definition of PSWs required combining occupations described by two NOC codes, one for nurse aides, orderlies and patient service associates and the other for home support workers, caregivers, and related occupations, which is considered part of occupations in education, law and social, community and government services within the NOC. Industry-based exclusions to the latter were made to confine the analysis to the healthcare context.
Case Study 2: Understanding Canada’s Health Workforce – the Case of Internationally Educated Healthcare Professionals (IEHPs)
Context and Research Objectives
The integration of IEHPs into health occupations has received increasing interest amidst labour shortages in Canada’s health sector.20-24 However, previous research on IEHPs has largely been limited to specific occupations or jurisdictions in Canada1,25,26 preventing a broader picture of the labour outcomes and skill utilization of these workers. 27 Additionally, disaggregation of IEHPs across sociodemographic subgroups is needed,1,27,28 but is often restricted by data sources with small sample sizes for this population.
The study Characteristics and Labour Market Outcomes of Internationally Educated Health Care Professionals in Canada 29 illustrates how Canada’s Census of Population can address many of these limitations. The first objective of this study was to estimate the number of IEHPs in Canada and the provinces and territories and describe their sociodemographic characteristics. The second objective was to examine the labour outcomes of IEHPs, focusing on their employment in health occupations and the skill level requirements of their jobs.
Data and Key Measures
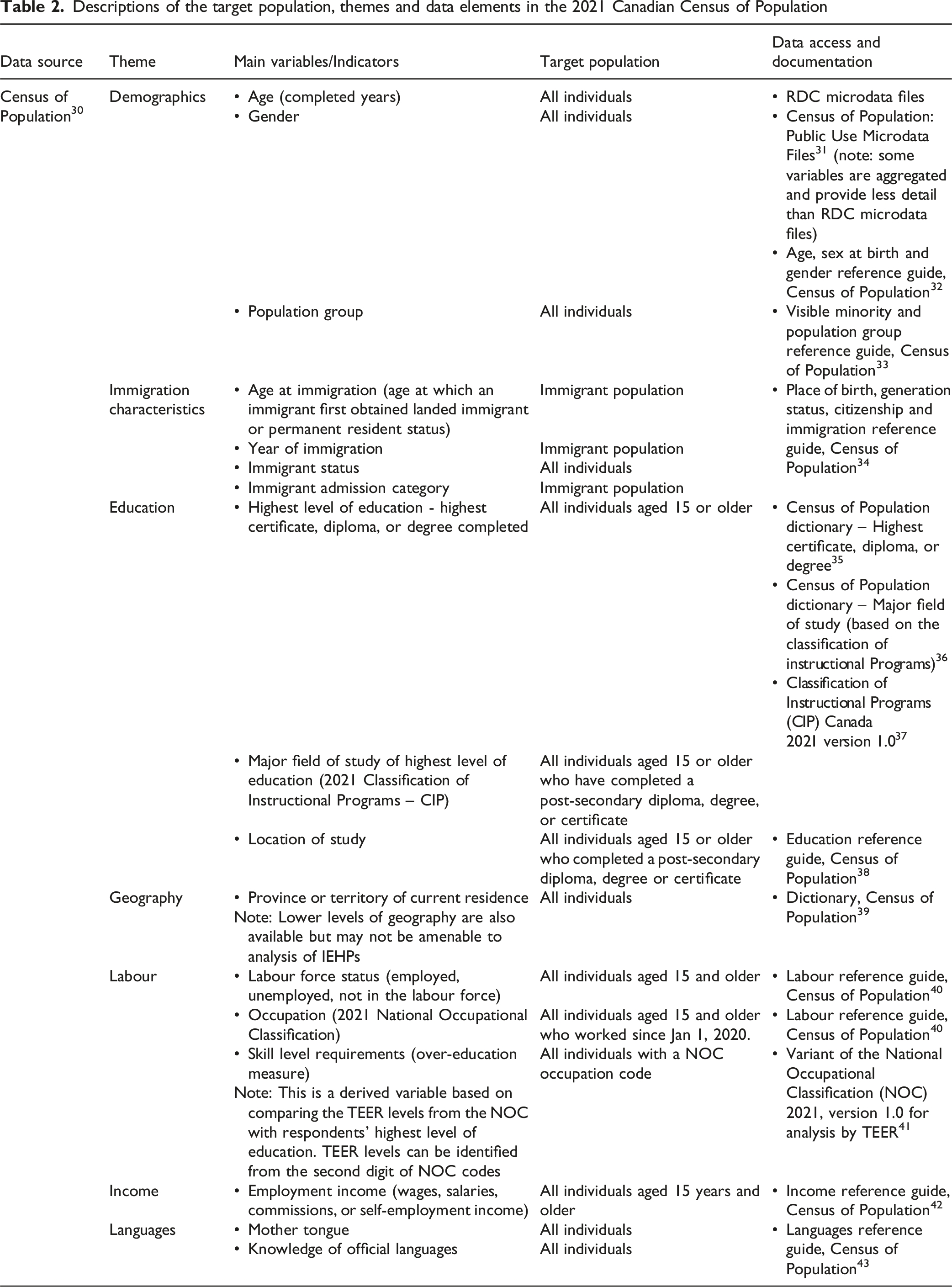
IEHPs were defined as individuals who are, or ever have been, landed immigrants or permanent residents, have a post-secondary certificate, diploma, or degree in a health field of study, and received this credential outside of Canada. The study used 2021 long-form Census of Population data, which contain the key pieces of information needed to identify IEHPs, based on a nationally representative sample.
Descriptions of the target population, themes and data elements in the 2021 Canadian Census of Population
Main Findings
The study estimated that Canada had just over 250,000 IEHPs aged 18 to 64 in 2021, with nearly half residing in Ontario. About one-third had studied nursing (33.0%) and over 1 in 10 had studied medicine (15.2%). IEHPs were primarily women (71.2%), and most received their education in an Asian country (62.7%). Nearly one-third of IEHPs were recent immigrants to Canada (32.1%), arriving between 2016 and 2021, and most entered Canada under the Federal Skilled Worker program (32.3%) or a provincial immigration program (20.1%). The majority of IEHPs reported a mother tongue in a non-official language, but proficiency in English (65.1%).
While over half of IEHPs in Canada worked in health occupations (57.7%), this varied across provinces and territories. Most IEHPs who had studied nursing or medicine were employed in a health occupation (68.7% and 66.9%, respectively). However, many IEHPs with a bachelor’s or higher degree who worked in the health sector had more education than required for their current position. Moreover, while men were less likely than women to be employed in health occupations generally, they were more likely than women to work in managerial or professional health occupations after controlling for other sociodemographic, education, and immigration characteristics. Period of immigration, immigrant admission category, region of education, population group, language, and education level were also associated with the labour outcomes of IEHPs in Canada.
Value of Census Data for Future Research on IEHPs
Canada’s Census of Population is collected every 5 years and uses standardized concepts for key variables, enabling researchers and policy-makers to monitor trends. However, structural changes to standardized classification systems may require the use of concordance tables 44 to compare results over time, and NOC groups may be too broad for some data users. 28 Overall, census data are advantageous to researchers examining IEHPs in Canada as they provide the demographic, immigration, and education information required to accurately identify this population. Additionally, the large, nationally representative sample permits both national and provincial/territorial estimates of IEHPs, and data disaggregation across different sociodemographic and occupational groups.
Case Study 3: Work and Life Stress and Mental Health Outcomes Among Nurses and PSWs During the Pandemic
Context and Research Objectives
Nurses and PSWs played a central role in Canada’s pandemic response. During the COVID-19 pandemic, these occupations were subject to increased workloads, redeployments, and exposure to health risks, while continuing to provide direct care.45,46 PSWs in particular faced unstable employment conditions and lower access to workplace protections.47,48 As the pandemic altered both work and home environments—especially for women—work-life boundaries became less distinct, and reported stress levels increased.49-52 Although prior studies show that nurses and PSWs report high self-perceived stress, even when job satisfaction is relatively high, 53 there has been limited analysis of how their experiences compare to other worker groups or how workplace and personal stressors jointly affect outcomes.
The study Work Stress, Life Stress and Mental Health among Nurses and Personal Support Workers (PSWs) during the Pandemic (2021-2022) intended to address this information gap. The research was driven by the following questions: How did work and life stress manifest among nurses and PSWs during the COVID-19 pandemic? How did these experiences compare to those of other workers? This study also sought to understand how job and personal life impacts intersect to shape stress levels.
Data and Key Measures
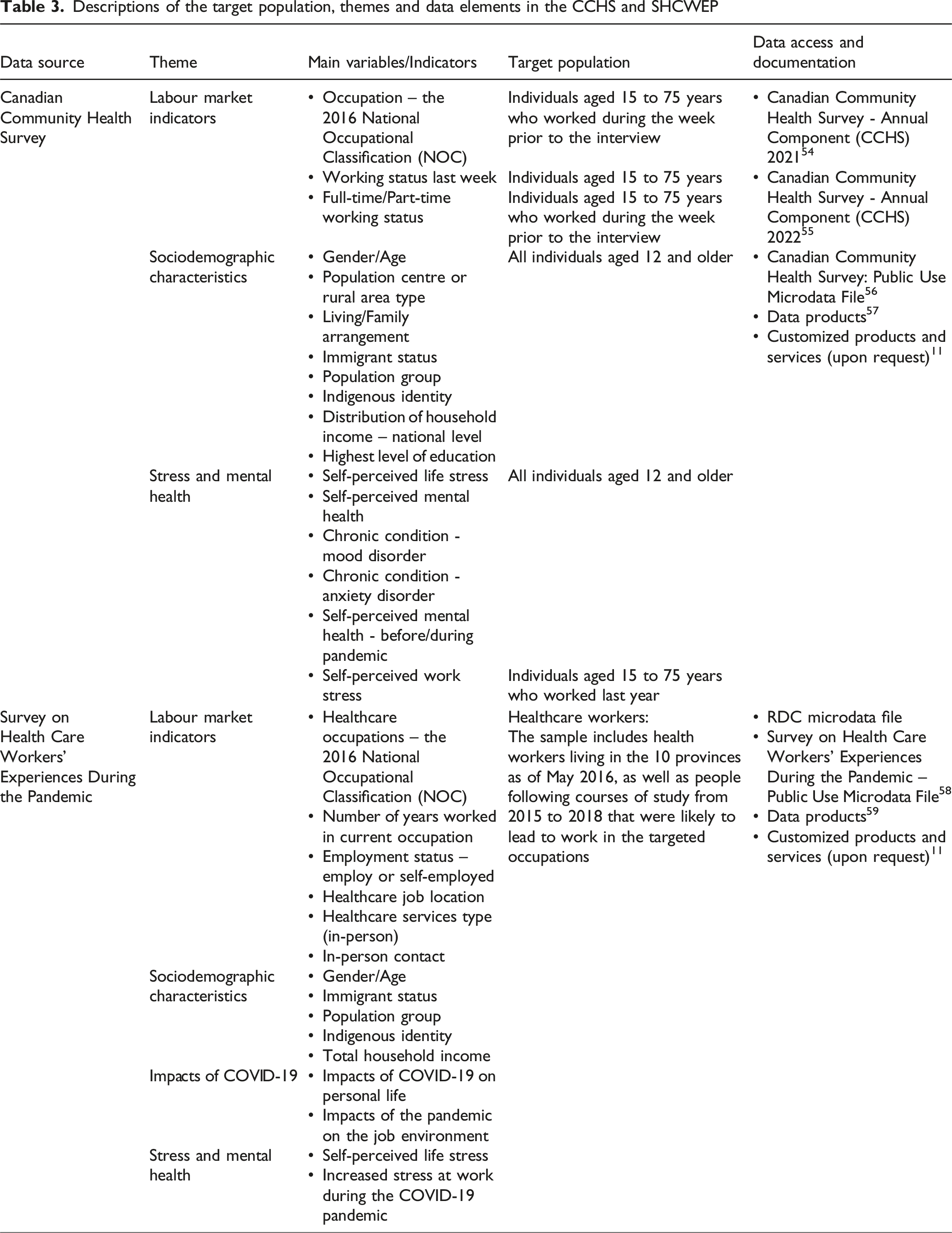
To answer the research questions, two key data sources were used (Table 3): (1) The Canadian Community Health Survey (CCHS) is a population-based, cross-sectional survey that collects information on health status, mental health, and work-related conditions among Canadians. Using data from the 2021 and 2022 cycles, which include self-reported measures of stress and mental health along with 4-digit occupational codes based on the 2016 NOC, stress levels among nurses and PSWs relative to other workers were examined. (2) The Survey on Health Care Workers’ Experiences During the Pandemic (SHCWEP) provides detailed, occupation-specific data on the experiences of healthcare workers during COVID-19. Conducted by Statistics Canada in 2022, SHCWEP collected information on stress, mental health, and the specific impacts of the pandemic on both job environments (e.g., increased workload, workplace conflict) and personal lives (e.g., caregiving responsibilities, financial strain). Based on this information, a measure of cumulative stressor impact across work and life domains (e.g., high-high, high-low) was constructed, enabling analysis of how these stressors intersect and contribute to reported stress levels. Descriptions of the target population, themes and data elements in the CCHS and SHCWEP
Main Findings
Life and work stress were not only more common among nurses and PSWs during the pandemic, but that the combination of job-related and personal life stressors created particularly high odds of reporting both high life and work stress. CCHS results showed that, after adjusting for relevant covariates, nurses were 3.2 times and PSWs 1.4 times more likely than other workers to report high work stress. SHCWEP findings further highlighted the cumulative effect of stressors. Among nurses, those experiencing high impact in both their job environment and personal life had 13 times higher odds of reporting high work stress compared to nurses with low impact in both domains. Among PSWs, the odds were 19 times higher for those with high impacts compared to those with low impacts. For life stress, the odds were 5 times higher for nurses and 6 times higher for PSWs when comparing individuals with high impacts to those with low impacts in both domains.
Value of and Considerations in Combining CCHS and SHCWEP Data Sources
Using population-based surveys in combination provided complementary insights into the health workforce. The main challenge in using these data sources is that while the CCHS allowed for broader occupational comparisons, it had a limited sample size for nurses and PSWs. In contrast, SHCWEP provided more detailed insights specific to healthcare workers but did not include other occupational groups. CCHS offered broad occupational comparisons, while SHCWEP captured stressors specific to nurses and PSWs. Together, they revealed how work and life stressors during the pandemic compounded to affect stress and mental health for those workers.
Conclusion
The health workforce is essential not only to the well-being of Canadians but also to the country’s social and economic sustainability. High-quality labour force statistics and health-related data, based on standardized concepts and classifications, are critical for providing consistent information on sociodemographic and employment characteristics, work location and activity across occupations. Such national data are vital for health leaders to inform decision-making aimed at enhancing health system sustainability and effectiveness across Canada.
This article presented three case studies to raise awareness of health workforce data available through Statistics Canada and to demonstrate how these data can be leveraged to produce nationally representative information across health occupations, sectors, and jurisdictions. They provided insight into issues such as job vacancies, stress, burnout, unpaid leave, changing job demands and mismatches between qualifications and job roles. Together, these analyses highlight the value of robust, nationally representative data in supporting evidence-based decision-making.
Underscored within these cases is the importance of considering data harmonization or alignment, particularly when certain variables are unavailable in one survey, but can be derived or matched from another. Additionally, when working with Statistics Canada data, it is essential to follow privacy and confidentiality requirements, which determine how data can be accessed and what can be reported, in line with the Statistics Act. 60
It should be noted that the availability and utility of national health workforce data available through Canada’s national statistical agency aligns with Health Workforce Canada’s (HWC) strategic plan61,62 which emphasizes the importance of improved access to high quality data. Recent tools such as HWC’s ‘Workforce in View’ dashboard,
63
developed by HWC with data from the Canadian Institute for Health Information (CIHI) and Statistics Canada, represent progress toward this broader goal of improving data access and usability. Indeed, an essential part of enabling health leaders and planners to better understand the scope, context and complexity of key health workforce issues lies in data. Statistics Canada data are collected, processed, and released in strict accordance with privacy and confidentiality guidelines. These safeguards ensure that information is handled in a fair and consistent manner, and that no individual, business or organization can be identified as per the Statistics Act.
60
Some surveys at Statistics Canada offer Public Use Microdata Files (PUMFs)
64
online that are free of charge to download and use. However, these datasets may be limited for some analyses as they contain a subset of variables from what the survey has to offer with some variables aggregated to protect confidentiality and for privacy concerns. For analyses or research that requires further nuance or disaggregation, accessing secure microdata from data sources such as those presented herein can be done through Research Data Centres (RDCs), housed on campuses across Canada.
65
RDCs can be accessed by academics, students, and government and private sector researchers. They offer a secure environment for researchers to analyze confidential data files. Researchers can gain access to RDC data through an application process.
66
More recently, in working with the Canadian Research Data Centre Network (CRDCN) and university partners, Statistics Canada has launched the virtual RDC (vRDC)
67
as a service. The vRDC is a networked IT platform that will provide new and improved remote options for accessing Statistics Canada microdata to researchers across Canada.Accessing Statistics Canada Microdata
Footnotes
Acknowledgements
We thank Isabelle Marchand, André Bernard, Li Xue, Dafna Kohen and Katie Scrim, at Statistics Canada, for their constructive feedback and helpful suggestions which greatly improved the manuscript.
Ethical Considerations
This manuscript uses secondary survey data, which is collected on a voluntary basis and requires participant approval for use, except in the case of the Census. The data is anonymized and adheres to the Statistics Act, which ensures the confidentiality of all individuals, households and businesses participation in Statistics Canada data collection efforts.
Author Contributions
Conceptualization: HM, KF, JP, TH; Writing original draft and preparation: KF, JP, HM, TH; Writing – review and editing: KF, JP, HM, TH. All authors have read and approved this version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.