
Abstract
Ethical health data use in Canada is often reduced to compliance with privacy requirements, limiting its role in governance and decision-making. This article reframes ethical data use as a relational practice that supports trust, transparency, participation, and shared accountability across institutions, patients, and communities. Grounded in Principle 7 of the Pan-Canadian Health Data Charter, it examines tensions between risk-averse data protection and the need to enable responsible data use for care, research, and system improvement, arguing that this divide constrains both innovation and public benefit. Trust and social licence are positioned as foundational to participation, data quality, and legitimacy, underscoring the need to redistribute decision-making power to patients and communities. Relational governance offers a practical pathway to move beyond compliance and support ethical, effective, and publicly trusted health data use in Canada.
Introduction
The Pan-Canadian Health Data Charter established a common set of principles for health data in Canada, with Principle 7 upholding “The ethical use of health data to support decision-making, policies, programs, services, statistics, and research for better health outcomes, while respecting the importance of open science and being open-by-design.” 1 However, many decision-makers lack clear guidance on how to apply ethics in practice or view ethics from a compliance or privacy lens.
This article offers insights into ethical data use in health by grounding it in co-governance and relational practice. Relational governance emphasizes participation, transparency, and shared decision-making among institutions, patients, and communities. This approach broadens ethical data use beyond compliance, challenges ethical tokenism, and supports beneficial data use that earns the trust of Canadians and allows health data to flourish. 2 This article takes a pan-Canadian perspective, acknowledging that implementation needs will vary across provincial and territorial contexts.
The Data Divide
Canada’s current policy regime governing how, when, and under what conditions data can be used is increasingly out of step with the realities of modern health systems. It is largely built on a risk-based paradigm that emphasizes the reasons data should not be used. Absent is the acknowledgement that there are significant risks associated with the underuse of health data. This framework often prioritizes select perceived risks, particularly in the privacy domain, over the meaningful benefits that responsible data use can generate for patients, families, communities, and society.3,4 Ethical data use requires a balanced approach that carefully weighs both risks and benefits.
Efforts to advance data use for connected care, public health, innovation, open science, and research have often been in tension with privacy and policy approaches designed to safeguard sensitive information.3,4 These tensions continue to create barriers to balanced and responsible data stewardship. In practice, the debate has polarized around two competing positions. The first is focused on protecting data at all costs, while the other advocates for broad data access.3,4
Moving forward requires holding space for both the importance of mitigating conventionally prioritized data harms, alongside the societal value and patient benefits that responsible data use can generate. This shift is not only normative but functional, relational governance enables more legitimate, sustainable, and scalable data use by aligning decision-making with public expectations. These challenges reflect broader structural barriers, including fragmented governance, inconsistent standards, and limited mechanisms for public participation and accountability.1,3,4
Towards Ethical Action
Ethical use can be understood through the principles of autonomy, non-maleficence, beneficence, and justice, yet many health data decision-makers lack the tools to apply these principles in practice. For example, applying the autonomy principle would include creating real-time opportunities for individuals to make informed decisions about their own data and treating patients as data partners with meaningful opportunities to access, engage with, or share their own information. Restricting data autonomy out of fear often reflects paternalism rather than protection.
Operationalizing non-maleficence requires understanding potential harms from data use. Instead of a culture of caution, we shift towards a culture of safety that supports innovation and responsible data use through proactive risk management, transparency, and clear guidelines. After all, people using data will feel safe reporting concerns or trying new approaches within structured boundaries, when boundaries are clear. Applying non-maleficence would equally account for the ethical implications or harms relating to underuse, including missed opportunities for data use that drives improved care, system efficiency, and population health outcomes.
Applying beneficence requires maximizing the benefits of data use to improve health outcomes, enhance public good, and ensure benefits are shared equitably across patients and communities.
Lastly, from a justice perspective we would emphasize preventing unfair burden or exclusions in access, use, and sharing of health data, calling attention to potential inequalities, bias, or discrimination to ensure equitable outcomes. We would apply policies and practices to ensure marginalized or vulnerable groups are not disproportionately harmed by how data are collected, used, or governed.
Translating ethics into action will support leaders, policy-makers, data stewards, and data users in navigating complex data dilemmas. 8 Incremental changes to shift in this manner will support a data governance regime that is adaptive, participatory, transparent, and responsive, ensuring that decisions reflect the rights, interests, and well-being of all Canadians.
Social Licence for Data Use
Given public health functions as a system of cooperation, the ethical use of health data is foundational. Surveillance, prevention, outbreak response, and long-term planning depend on collective participation in a surveillance infrastructure shared across regional health authorities, provinces and territories, and federal partners. 9 When standards, practices, and legislation vary across the country, maintaining participation becomes a governance challenge, not simply a technical one.
When systems interoperate effectively, the benefits become tangible. Care is better coordinated across settings, duplicated tests can be reduced, and clinicians have more complete information when making decisions. 10 However, expanding access without accountability can create new governance risks, particularly where power imbalances exist or conflicts are not easily resolved. Increased technical access can interact with market dynamics, consolidation, and commercial incentives in ways that are not automatically aligned with public benefit.4,5 This is where social licence becomes a practical governance constraint. Canadian research shows that public support for health data use is conditional. The context in which data are used matters.11,12
Transparency makes decisions, processes, and outcomes visible, enabling accountability and reducing opportunities for hidden or unchecked authority.5,6 Relational practices, including dialogue, consultation, and stakeholder engagement, empower individuals to participate in decision-making. Together, these approaches shift power from centralized and hidden authority towards a broader set of stakeholders, fostering a culture of shared responsibility, trust, and vigilance. When deeply embedded in organizational culture, this combination not only discourages unethical behaviour but also strengthens the system’s capacity to detect and respond to potential misconduct, making ethical misconduct less likely to occur.
Openness and interoperability cannot be treated solely as a feature of technical infrastructure; it must also be embedded in governance, decision-making, and accountability structures. Canada’s Pan-Canadian Health Data Charter reflects this approach, situating open-by-design alongside commitments to ethical use, public inclusion, Indigenous data sovereignty, common standards, and harmonized governance. 1 Indigenous data governance also reinforces this perspective. For instance, the CARE Principles emphasize that data systems should be evaluated not only for accessibility and technical reuse but also for whether they create collective benefit, respect communities’ authority to control their data, and embed responsibility and ethical practice. 13
Although interoperability connects systems, it is relational governance that ensures that these connections remain stable, equitable, and ethically accountable under pressure. Open-by-design must therefore be paired with care-by-design, ensuring that ethical use is not merely aspirational, but actively operationalized.1,13 If people do not trust how data will be used, the social licence will be jeopardized and fail to materialize benefits from data in Canada.
Trust as Infrastructure
Trust is the foundation of any data ecosystem. It shapes participation, data completeness, and the legitimacy of data-driven decisions. Just as ethical principles guide our decision-making at the individual and societal level, trust guides the relationships and interactions that make ethical data use possible. Without trust, we risk reinforcing inequities or failing to serve those most affected. Conversely, when trust is intentionally cultivated, it becomes an enabling infrastructure for responsible, innovative, and socially valuable data use.5,7
Effective trust-building is cyclical and relational; beginning with listening to stakeholder expectations and understanding the interests of patients, communities, and the public. These expectations must then be embedded in policy, practice, and governance structures. In contexts involving Indigenous communities, this means building relationships that respect self-determination and cultural priorities, demonstrating that ethical governance is inseparable from relational accountability.13,14 The consequences of weak trust are structural and cumulative. Low trust reduces participation, which undermines data completeness and quality, producing less reliable decisions that disproportionately affect underserved populations.7,12 Trust is both a prerequisite for ethical data use and a measure of legitimacy. 15
By embedding trust as infrastructure, data systems can move from procedural compliance towards meaningful, value-driven governance. Through relational practices, we can uphold the rights, interests, and well-being of individuals, communities, and society at every stage.5,7
A Shift in Power
At a basic level, shifting power from institutions towards patients and communities is essential for ethical data use. The benefits of data cannot be fully realized if the people who contribute it and are most affected by data decisions have little influence over how it is used. Yet, “there is widespread recognition that standardizing approaches to data stewardship requires a shift in mindsets and collective culture. It will also require a redistribution of power, but it is less clear if that is widely accepted or understood.” 3
In conventional systems, decisions about how data are collected, used, and shared are made internally by institutions, often without meaningful input from those whose data are at stake.5,6 The culture of healthcare continues to reinforce institutional power concentrated within organizations. Shifting power towards patients and communities is essential to move towards a relational governance model focused on ethical legitimacy. Relational governance reorients this with shared decision-making authority with communities and proactively engaging patients and the public more broadly before decisions are made.
Data interoperability holds some promise of empowering patients with access, and the ability to manage or share their health information across different providers and systems. 10 However, the push for interoperability also exposes the structural realities of the health system. Historically, whether by design or default, data flows and control have primarily benefited institutions, clinicians, and centralized systems rather than patients.3,4
Interoperability and other optimized data uses in Canada cannot be realized through technology alone. Achieving ethical data use requires restructuring governance, redistributing power, and embedding relational practices that give patients genuine agency. Relational governance ensures that decisions are made with patients and communities, not just for them, embedding transparency, accountability, and co-design into every stage of the data lifecycle.3,6
Policy Recommendations
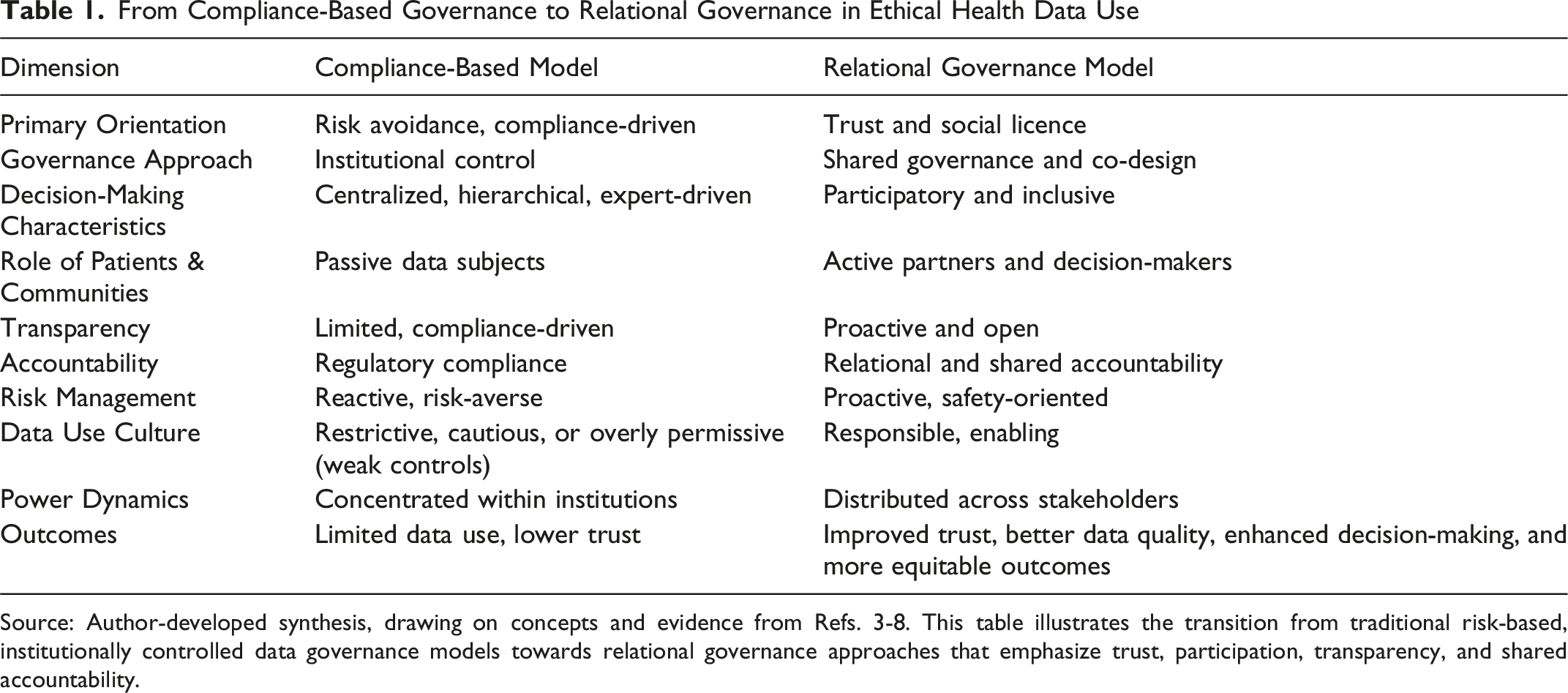
Adopting a human-focused policy perspective, the following recommendations aim to advance the spirit of the Pan-Canadian Health Data Charter, and support the shift towards relational governance outlined in Table 1.3,7,8 1. 2. 3. 4. a. Patient Care Metrics: data use leading to improved personalized treatment, faster diagnoses, and coordinated or connected care; b. Policy and Planning Metrics: data use enabling evidence-based decisions, resource allocation, and population health management; c. Research and Innovation Metrics: data use leading to innovations in care, treatment, and decision-making, including responsible Artificial Intelligence (AI); d. Operational Efficiency Metrics: data use reducing duplication, improving decision-making, and lowering costs; e. Societal Impact Metrics: data use supporting rapid public health response, promoting health equity, and enabling continuous system improvement. 5. 6. 7. 8. From Compliance-Based Governance to Relational Governance in Ethical Health Data Use Source: Author-developed synthesis, drawing on concepts and evidence from Refs. 3-8. This table illustrates the transition from traditional risk-based, institutionally controlled data governance models towards relational governance approaches that emphasize trust, participation, transparency, and shared accountability.
Limitations and Implementation Considerations
Implementation may be limited based on fragmented data systems, resource constraints, cultural differences, and varying legal frameworks across jurisdictions. As a conceptual paper, this work does not test the proposed governance model in practice. Future research should examine its real-world application and impact.
Conclusion
Public trust is cultivated not merely through meeting regulatory requirements but through demonstrating an ongoing commitment to ethical stewardship, openness, and shared purpose. When people see that data practices honour their dignity and advance collective benefit, confidence and a durable social licence emerge. 15
Ethical data use in Canada should ensure patients and community representatives participate in governance, decisions are transparent, and the benefits of data use are returned to the communities whose data made them possible. Embedding relational governance into health data systems is critical and creates the conditions for ethical and effective use of health data as outlined in Principle 7 of the Pan-Canadian Health Data Charter.1,3 Through participatory governance, transparency, and shared decision-making, healthcare leaders can move beyond fragmented data silos towards a trustworthy, resilient connected ecosystem worthy of public confidence.
Footnotes
Ethical Approval
Institutional review board approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.