
Abstract
Scalable, interprofessional care models are needed to support chronic disease management and improve access to speciality services. A community hospital heart function clinic expanded from a single-site, nurse practitioner–led model to a two-site interprofessional program over 4 years. The objective was to examine program growth, service utilization, and operational strategies supporting sustainable expansion. A retrospective review assessed annual encounters, visit types, and provider activity across nursing, pharmacy, supportive cardiology, and community partnerships. The Consolidated Framework for Implementation Research guided analysis of implementation and scalability. Annual encounters increased from 1,562 to 4,623, with unique patients rising from 566 to 854. Registered Nurse telephone follow-ups expanded substantially, with additional growth in Nurse Practitioner and pharmacy visits. The second site accounted for nearly 10% of visits, improving regional access. Interprofessional collaboration and distributed care supported sustainable growth and improved access to specialized heart failure services.
Introduction
Heart Failure (HF) is a leading cause of morbidity, mortality, and health system utilization in Canada. Provincially, HF accounts for substantial emergency department use and hospital admissions, with many patients experiencing repeat exacerbations and progressive functional decline.1-4 This burden is particularly pronounced in regional and rural areas, where older, multimorbid populations have limited access to specialized cardiac services and to the optimization of Guideline-Directed Medical Therapy (GDMT).5-8 These gaps highlight the need for locally delivered chronic disease management models that minimize regional travel burdens, prevent diagnostic delays, and enable early medication titration closer to home.
Heart Function Clinics (HFCs) provide an important avenue for delivering interprofessional HF care, improving access and supporting community-based HF management.9-11 As healthcare complexity has increased, care delivery has shifted away from isolated professional silos toward interprofessional collaboration, defined as the integrative cooperation among healthcare professionals with complementary competencies working together to deliver patient-centred care. 12 In HF management, Nurse Practitioner (NP)-led interprofessional teams represent an effective model for supporting medication optimization, continuity of care, and longitudinal disease management.13-15
This article describes the development and growth of a hospital-based HFC over an 18-month period, focusing on changes in clinical activity, referral patterns, care-delivery processes, and implementation factors that supported successful scale up.
Setting and Context
In response to the increasing prevalence of HF, a regional community hospital expanded its HFC model from a single-site, NP-led clinic to a coordinated two-site program with interprofessional support and integrated community care pathways. The HFC serves a mixed urban-rural population with high rates of chronic cardiovascular disease and limited local access to specialized cardiac care. At the outset, the clinic operated with a single NP at one site, providing approximately 75 patient visits per month. Care focused primarily on symptomatic management and follow-up for patients recently hospitalized with HF.
Increasing HF admissions and repeat emergency department presentations highlighted gaps in early intervention and follow-up, prompting clinic expansion. Concurrently, provincial and organizational priorities emphasized integrated, team-based approaches.2,16,17 Expansion included adding an NP lead. External, community-based cardiologists provided consultative oversight for complex diagnostic and therapeutic decisions, while longitudinal management remained primarily NP-led. Pharmacy services were embedded to support medication optimization. A supportive cardiology stream, grounded in palliative care principles, was incorporated to address symptom burden, goals of care, and advanced care planning for patients with end-stage HF.
To extend care beyond the clinic walls, partnerships were established with home and community care providers and community paramedicine programs. These collaborations enabled home-based monitoring, symptom assessment, escalation support, and rapid follow-up during periods of clinical instability. Together, these components formed a coordinated care model.
Methods
A retrospective review of administrative and clinical data of the HFC was conducted to describe program growth, service utilization, and outcomes. The analysis covered January 2022 through May 2025, with particular emphasis on the 18-month accelerated growth phase beginning in September 2023. The evaluation focused on clinic capacity, referral patterns, and system-level outcomes related to the delivery of HF care in a regional setting.
Data Sources and Extraction
Data were extracted from internal scheduling systems, Electronic Medical Record (EMR) documentation, and referral and encounter records. These sources provided information on visit volume and distribution, referral origin and type, diagnostic and treatment encounters, and hospital utilization metrics. Pharmacy involvement was identified through medication management notes and associated EMR tasks.
Outcome Measures
Outcomes were grouped into three categories. “Clinic Activity and Utilization” included the number of unique patients, the total number of visits stratified by type (in-person, virtual; clinician type), and patterns of follow-up frequency. “Referral Patterns” captured volume and direction of referrals to Home and Community Care, Community Paramedicine, and Pharmacy Services. “System-Level Outcomes” included length of stay for HF admissions, HF-related emergency department visits, and 30-day readmissions when available.
Analysis
Trends in clinic activity, referral patterns, and service utilization were summarized using descriptive statistics. Metrics such as patient volume, visit types, and interprofessional engagement were examined to characterize changes over time. Descriptive statistics were used exclusively to characterize clinic functions and operational patterns during the implementation and expansion of the HFC.
Implementation Framework
The Consolidated Framework for Implementation Research (CFIR), a comprehensive framework for evaluating complex interventions, guided the interpretation of findings. 18 The CFIR domains were applied to examine implementation processes and interprofessional collaboration. 19 This framework supported the systematic analysis of organizational, provider, and external factors that shape the growth, sustainability, and scalability of the HFC.
Ethics and Data Privacy
This project was undertaken as a retrospective program evaluation and quality improvement initiative. No patient identifiers were collected, and all data were analyzed in aggregate. This project was classified as a quality improvement and program evaluation initiative and was exempt from formal Research Ethics Board review in accordance with institutional policy.
Results
Growth in Clinic Volume and Patient Encounters
Over the 4-year period under review, the HFC demonstrated substantial growth in patient volume, visit volume, and clinical complexity. Annual patient encounters increased from 1,562 visits in 2022 to 4623 visits in 2025—nearly a threefold rise. The number of unique patients followed each year also grew steadily, from 566 in 2022 to 854 in 2025. This growth occurred alongside the transition from a single-site, NP-led clinic to a two-site interprofessional program with consistent access to nursing, pharmacy, and supportive cardiology services.
Shifts in Provider Activity and Interprofessional Integration
Provider activity patterns illustrate the extent of interprofessional expansion (Figure 1). Nurse Practitioner visits increased from 1558 in 2022 to 2082 in 2025, with NPs primarily providing in-person, comprehensive patient assessments. The most significant operational shift occurred with the addition of a full-time Registered Nurse (RN), whose annual visits increased from 616 in 2023 to 2254 in 2025, surpassing NP visit volumes by 2024. The RN conducted structured telephone follow-up visits under the NP’s direction, focused on symptom monitoring, patient education, and medication adjustment. Pharmacy visits increased from 109 in 2024 to 267 in 2025. Outpatient HFC volumes and appointments per year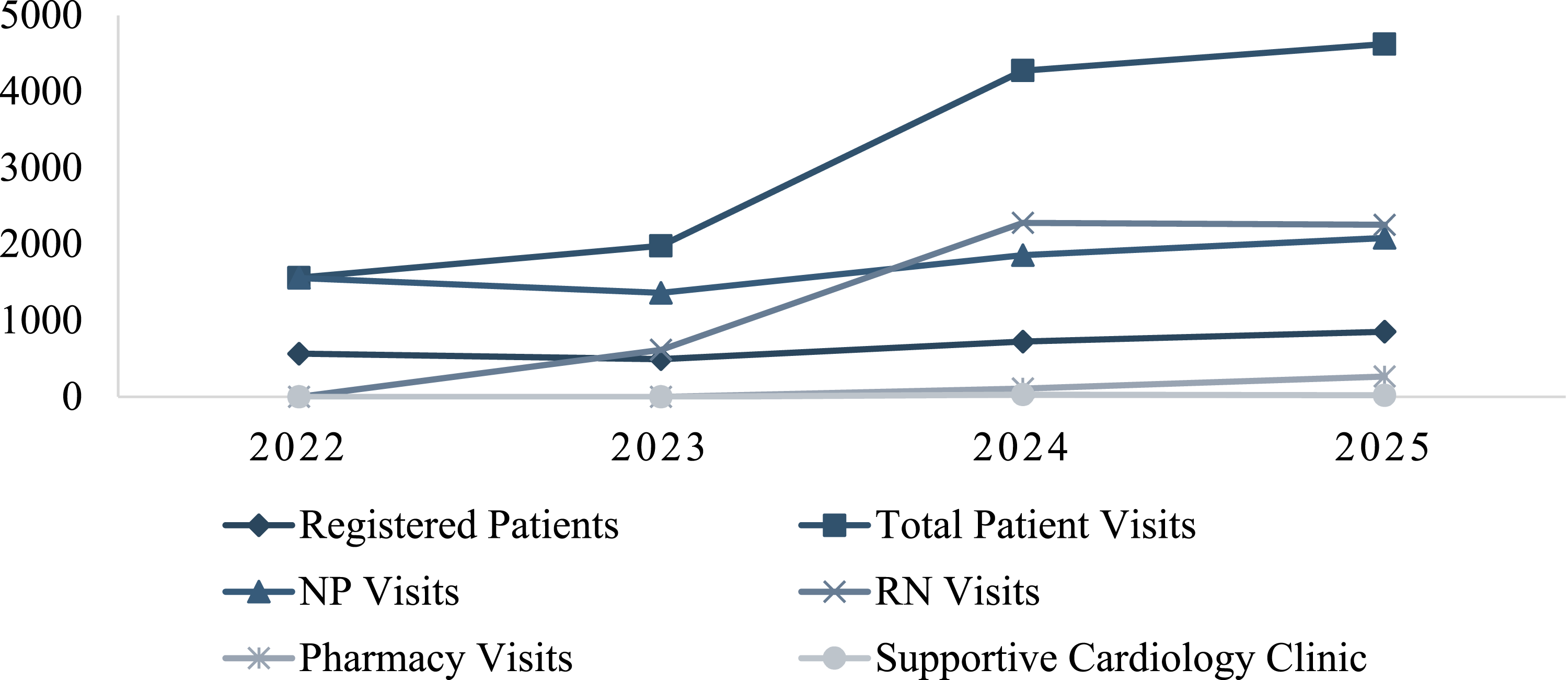
Regional Access Across Two Sites
Annual visits at the leading site increased from 1,538 in 2022 to 4,168 in 2025, while visits at the satellite site rose from 24 to 455 over the same period (Figure 2). By 2025, the satellite site accounted for nearly 10% of the clinic’s total number of visits. In-person visits remained the dominant modality, reaching 4,168 in 2025, while telephone encounters increased to 2,467, reflecting the growing role of remote management in chronic disease care.20-22 Outpatient HFC visits according to site and modality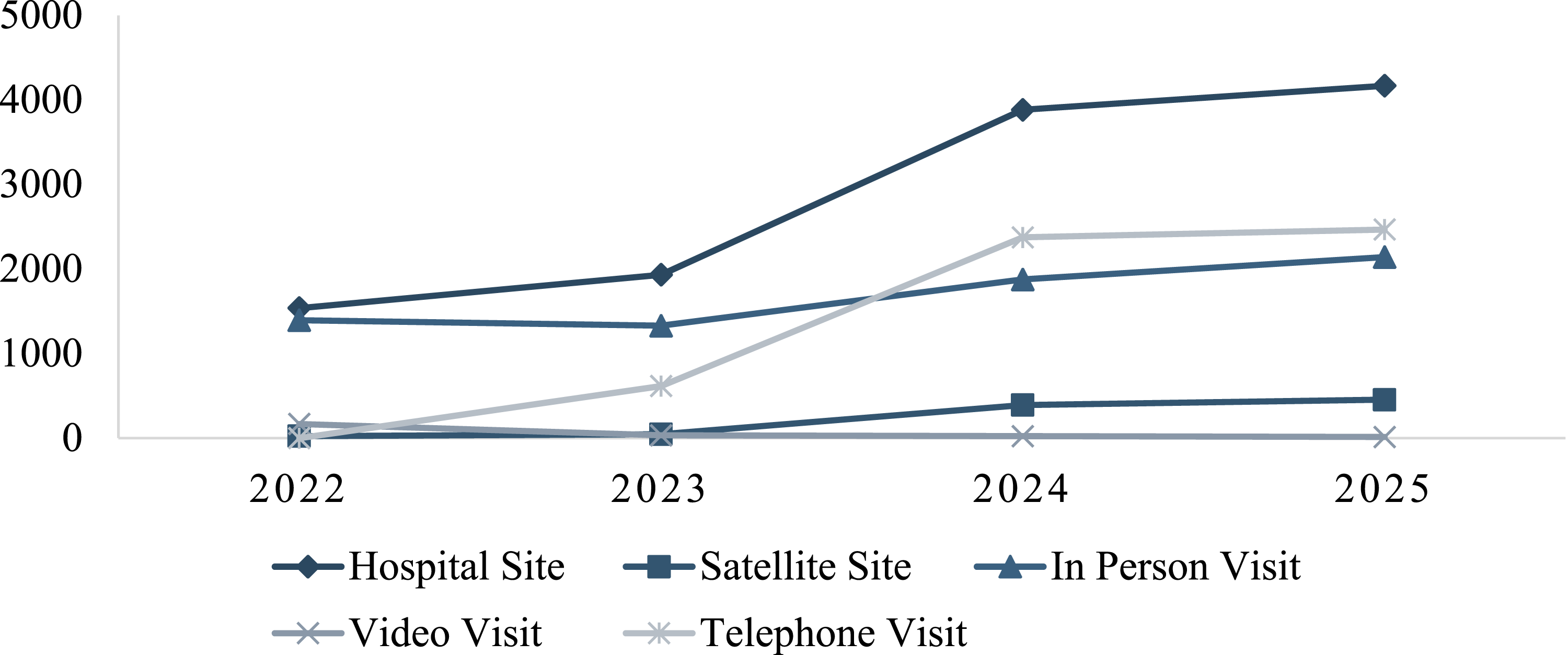
System-Level Outcomes: HF Inpatient Discharges, Length of Stay, and Readmissions
System-level outcomes differed between the all-comer HF cohort and patients seen in the HFC. Among all-comer HF discharges, annual hospitalizations decreased from 296 in 2022 to 180 in 2025, while HF discharges among HFC-known patients increased from 94 to 155 over the same period. Length of stay remained similar between HFC and all-comer cohorts across the investigated period.
Readmission outcomes are shown in Figure 3. In 2022 and 2023, HFC patients had lower 30-day readmission counts than the all-comer cohort (10 vs. 17 in 2022; 11 vs. 18 in 2023). In 2024 and 2025, 30-day readmissions were higher among HFC patients (22 and 13) compared with the all-comer cohort (12 and 8). Ninety-day readmission counts were lower for HFC patients in 2022 and 2023, increased in 2024 (45 vs. 24), and were similar between cohorts in 2025 (15 vs. 12). Thirty-day and ninety-day inpatient readmissions by cohort, 2022-2025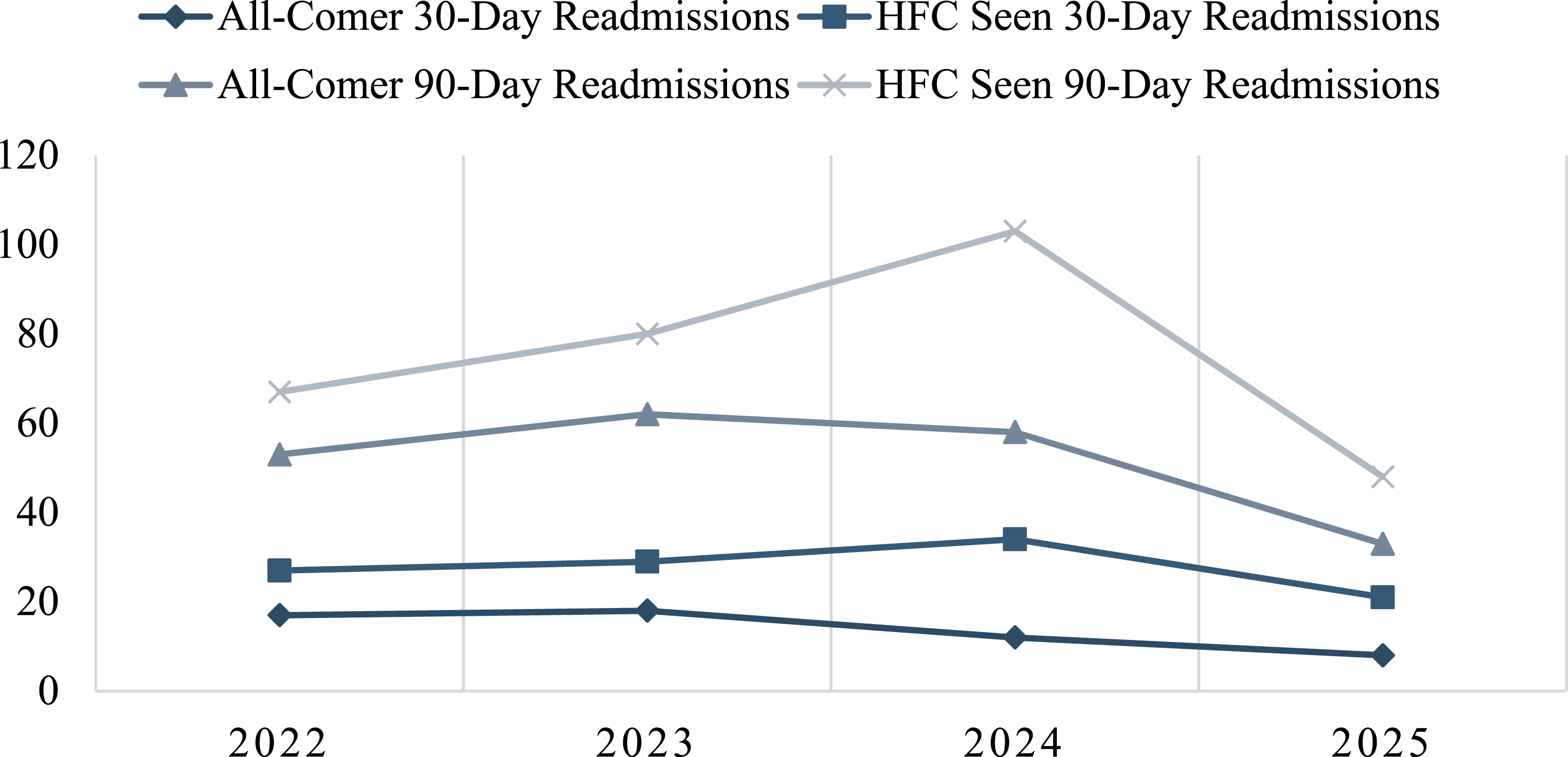
Interprofessional Care Pathways and Documentation Limitations
Home IV furosemide administration, home and community care referrals, and community paramedicine involvement were frequently identified during chart review but were not consistently captured in structured EMR fields. Community-based pathways commonly involved shared follow-up between the HFC, homecare nursing, and community paramedics to support monitoring and escalation management outside hospital settings. Consequently, these activities were not reliably retrievable through data extracts, resulting in underrepresentation of cross-sector care coordination volume.
Discussion
The expansion of the HFC demonstrates how an NP-led community HF model can be operationalized and expanded within a regional health system. Using the CFIR 18 as a guide, several key factors contributed to the successful development and sustainability of this model.
Intervention Characteristics
The HFC care model was designed to scale longitudinal HF management across varying levels of complexity through NP-led assessment, GDMT optimization, symptom monitoring, and rapid follow-up during periods of instability. The model incorporated multiple video modalities, including in-person, telephone, or videoconferencing, allowing patients to receive ongoing management without relying exclusively on hospital clinic-based encounters.
A major operational evolution during expansion was the transition of internal roles from paired care to autonomous, differentiated pathways. Initially, pharmacists attended paired visits alongside the NP, a resource-intensive approach vulnerable to scheduling constraints. Shifting pharmacy to an independent consultation track optimized workforce capacity. This structural evolution aligns with contemporary interprofessional collaboration literature, which demonstrates that transitioning from parallel practice to distinct scopes maximizes clinic throughput. 23 Pharmacists independently conduct assessments for newly referred patients to support HF education, medication reconciliation, GDMT counselling, collaborative treatment decision-making, and dynamically re-engage patients during periods of therapeutic change without tethering the pharmacist to the NP’s schedule.
Similarly, supportive cardiology services evolved from a joint-consult model to a co-located pathway operating in parallel with routine HFC care. The literature on clinical co-location demonstrates that physical proximity and shared infrastructure foster implicit trust and organic communication, without the administrative friction of external referrals.24,25 The monthly clinic, staffed by a palliative care physician, addresses symptom burden, quality of life, advanced care planning, and complex decision-making while maintaining structural continuity through shared clinical records.
Inner Setting
Program success was anchored in organizational alignment and leadership endorsement. The NP-led framework provided operational stability independent of physician resources. Monthly team education sessions supported role clarity and shared approaches across disciplines, mitigating individual role ambiguity that frequently challenges team-based care. 12 CFIR highlights that scaling capacity requires adjusting available resources and aligning work infrastructure to shifting clinical demands. 18 This was operationalized by adding a full-time RN to handle telephone-based symptom monitoring, complementing the NP’s comprehensive in-person assessments. Interprofessional literature emphasizes that sustainable scaling relies on deliberate task distribution; by shifting routine, high-volume monitoring to structured RN telephone protocols, the clinic preserved the advanced scope of the NP for complex cases.26-28 This internal collaboration may explain how encounters tripled without expanding physical infrastructure.
Outer Setting
Provincial performance expectations and regional disparities were critical structural catalysts for program growth. Expansion was driven largely by provincial mandates that enhanced cardiac quality standards and required access to specialized, interprofessional HF teams.2,17 These external pressures intersected directly with local system gaps, as regional and rural patients faced severe travel burdens and fragmented care pathways to access specialized cardiac care. In response, clinic leadership leveraged the partnerships and connections to link hospital-based operations with paramedic services and homecare networks. Local leadership converted high-level policy pressure into connected, inter-organizational networks that aligned regional delivery with provincial quality standards.
Implementation Process
Growth was phased and operationalized several CFIR constructs. The model utilized Tailoring Strategies to introduce staffing components progressively, such as an RN role and embedded pharmacy support, in response to clinical demand and capacity constraints. This growth was achieved through iterative Plan-Do-Study-Act cycles, 29 emphasizing localized learning over rapid structural change to maintain service quality. To support this workflow, cross-provider coordination relied on direct communication and collaborative care planning with regular team sessions to support role clarity and clinical consistency. The increase in NP in-person visits alongside RN telephone encounters demonstrates that the clinic optimized task distribution while maintaining comprehensive care.
Interprofessional Collaboration
Core clinic operations succeeded through clear role differentiation: cardiologists maintained diagnostic oversight; NPs continued workup and treatment; the RN managed telephone triage; pharmacists titrated complex regimens; and supportive cardiology addressed quality-of-life trajectories. The internal alignment expanded capacity without a proportional reliance on additional resources. Regular interdisciplinary communication, co-location of services, and collaborative care planning supported continuity across these pathways while allowing each discipline to function with increasing autonomy as the clinic matured. The substantial increase in RN follow-up encounters and pharmacy involvement proves that internal role differentiation enabled the clinic to expand capacity without expanding physical NP slots.
With this internal infrastructure established, collaboration with community-based partners, such as homecare nursing and community paramedicine, expanded to serve as a clinical support and safety net rather than replacing core clinic functions. While interprofessional collaboration literature notes that cross-sector boundaries often fragment care, this model implemented formal structural facilitators to bridge hospital and municipal services. 30 Communication relied on integrated tools: asynchronous e-consults, shared EMR documentation, and direct telephone lines. Clinical deterioration flagged during an internal RN phone check could trigger immediate, direct-dial deployment of community paramedicine for in-home diagnostics and virtual consultations. These formalized pathways allowed patients to be co-managed at home while maintaining central clinical governance within the HFC.
Limitations
The descriptive design did not allow evaluation of causal relationships between clinic expansion and clinical outcomes. Referrals to home care and community paramedicine were frequently documented as free-text entries rather than standardized orders, underestimating their involvement. Pharmacy integration was also inconsistently captured prior to the introduction of formal scheduling workflows. While the findings describe trends in clinic growth and interprofessional engagement, they may not fully reflect the extent or impact of the expanded model. Addressing these gaps through standardized EMR workflows and structured data capture will be essential to support future evaluation, quality improvement, and health system planning.
Recommendations for Health Leaders
This evaluation supports a strategic shift toward scalable, community-based HF care models anchored by strong internal clinic frameworks. To optimize sustainable scaling, health leaders should consider the following: • Prioritize NP-led Models: Expand NP-led clinics to meet quality mandates. Utilizing NPs as clinical leaders ensures pragmatic stability independent of physician capacity, allowing cardiologists to focus on high-complexity consultative oversight. • Maximize Internal Interprofessional Scope and Co-Location: Rather than relying on resource-intensive paired-visit models, leaders should transition internal clinic roles to autonomous, parallel pathways. • Position Community Partnership as a Strategic Safety Net: Establish formalized, cross-sector pathways with homecare and community paramedicine to serve as a rapid-response backdrop during acute exacerbations. Using direct-dial protocols and virtual consultation links the community to HFC services, allowing complex patients to be managed at home while maintaining central clinical governance within the core clinic team. • Invest in Standardized Data Infrastructure: Overcome the communication barriers of fragmented health networks by implementing standardized EMR workflows.
Conclusion
The expansion of the HFC demonstrates that an NP-led, interprofessional model can scale sustainably to meet rising HF demands. By transitioning to autonomous, parallel workflows among providers, the program successfully expanded to two sites while maintaining continuity of care. Grounded in CFIR and interprofessional collaboration principles, this model offers a transferable framework for health leaders aiming to scale up HF ambulatory care models.
Footnotes
Ethical Approval
This project was conducted as a retrospective quality improvement and program evaluation initiative. In accordance with institutional policy, formal research ethics board approval and individual informed consent were not required. Data were analyzed in aggregate and reported in de-identified form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employed by the Royal Victoria Regional Health Centre and hold clinical and operational leadership roles within the Heart Function Clinic and associated programs described in this manuscript. These affiliations represent non-financial interests related to program implementation and evaluation. The authors report no grants, consulting fees, stock ownership, patents, or other financial interests related to this work.
Data Availability Statement
Data are available from the authors upon reasonable request, subject to institutional privacy requirements.