
Abstract
Background
Interprofessional education strategies are becoming more prevalent as nursing schools integrate interprofessional practice activities into their curricula.
Purpose
This paper presents the results of a federally funded project to deliver online interprofessional education to nursing students on screening for alcohol and substance use in rural areas, in which their perceptions about interprofessional education were measured.
Methods
A quasi-experimental within-subjects repeated measures design was utilized. Students in the bachelor or associate degree program were recruited from two rural nursing schools. A demographic questionnaire, Alcohol and Alcohol Problems Questionnaire, Drug and Drug Problems Questionnaire, and Interprofessional Education Perception Scale were utilized. General linear modeling was used to determine changes in these measurements over time. Data collection was performed at pretraining, posttraining, and following an online interprofessional dialogue.
Results
The study consisted of 89 nursing students. The participants were 87% female (n = 77/89) and 91% white (n = 81/89); their mean age was 24.9 years (standard deviation = 10.36). Analysis of evaluation questionnaires demonstrated increased levels of confidence in working with patients who consume alcohol or other drugs and on certain aspects of interprofessional education.
Conclusion
Online interprofessional preservice education holds the potential to positively increase nursing students’ confidence in working with patients and to increase their interprofessional practice.
Keywords
Background and purpose
When health-care professionals are exposed to interprofessional education (IPE), they are more likely to work effectively in teams in clinical settings (World Health Organization [WHO], 1988, 2010), which can improve the continuity of care and allow for better patient outcomes (Meleis, 2016). IPE was initiated when WHO addressed the need for interprofessional collaborative health-care practice. IPE is a process that promotes learning about, from, and with other health-care professionals. Recent studies (Johnson et al., 2014; Reeves, Perrier, Goldman, Freeth, & Zwarnestein, 2013) demonstrate that the implementation of collaboration among health-care workers will result in the improvement of health outcomes and overall patient well-being. Moreover, similar studies (Kent et al., 2016; Lapkin, Levett-Jones, & Gilligan, 2013; O’Connell, Gill, Artar, Jones, & Vargas, 2002) suggest that requiring nursing, medicine, pharmacy, and other health professionals to learn about IPE will improve teamwork. Health-care professionals practice safely and effectively communicate with patients and interprofessional colleagues through the use of active listening, respect, and timeliness (Brock et al., 2013; Kligler et al., 2015).
Education in the health professions needs to be aligned with clinical practice requirements as the delivery of health care rapidly moves toward team integrated models (Meleis, 2016). Clinical leaders need to be aware of their responsibility in helping educators better prepare students for the realities of team-based practice (Meleis, 2016). Interprofessional collaborative practice is critically important to allowing U.S. health care to progress toward the triple aim of (1) better care for individuals, (2) better health for populations, and (3) lower health-care costs to meet Healthy People 2020 objectives (U.S. Department of Health and Human Services, 2011). Interprofessional collaborative practice occurs when health professional students develop core competencies through IPE education, including attention to the social determinants of health (Addy, Browne, Blake, & Bailey, 2015). Moreover, IPE experiences must dovetail with the creation of continuing education programs that contribute to interprofessional curricula from prelicensure through lifelong practice (Schmitt, Gilbert, Brandt, & Weinstein, 2013).
Not all health science students, including nursing students, have the opportunities to work with or observe teams engaged in collaborative interprofessional practice. Such opportunities depend on the clinical placement settings available, which results in variation in students’ observations of and participation in interprofessional practice. The observation of teams in action is not sufficient, as students need to become active members of interprofessional health-care teams to fully grasp collaborative interprofessional practice (Thistlethwaite et al., 2014). Without having clinical experiences that emphasize the importance of interprofessional teams, nursing students may lack an understanding of collaborative practice, resulting in students being ill-equipped to enter academic health centers (Chen, Delnat, & Gardner, 2015). Unfortunately, many nursing programs lack formal IPE opportunities that comprise intentional curricular approaches (Hudson, Sanders, & Pepper, 2013). Moving forward, nursing educators need to first provide students the opportunity to begin understanding their own professional roles and then gradually stream IPE into the curriculum as part of the student experience (Hudson et al., 2013).
In May 2011, a report by an expert panel of the Interprofessional Education Collaborative (IPEC) described core competencies for interprofessional collaboration. IPEC is an interprofessional initiative for health-care education that is under the leadership of the American Association of Colleges of Nursing, the American Association of Colleges of Osteopathic Medicine, the American Association of Colleges of Pharmacy, the American Dental Education Association, the Association of American Medical Colleges, and the Association of Schools of Public Health. The IPEC competencies consist of four domains: (1) values and ethics for interprofessional practice, (2) roles and responsibilities, (3) interprofessional communication, and (4) teams and teamwork. The IPEC report (Interprofessional Education Collaborative Expert Panel, 2011) also suggests that the process to acquire competence across these domains begins in admission to health-care professional programs, continues throughout training, and is carried into professional practice. The IPEC competencies provide a framework for assessing competency-based learning outcomes (Martinez, Pfeifle, & Ballard, 2013).
Likewise, the Canadian Interprofessional Health Collaborative states that Interprofessional Collaborative Practice (IPCP) is a participatory, collaborative, and coordinated team-based practice between health-care providers and patients. The six competency domains of Canadian IPCP are similar to the four competencies outlined in the American IPEC competencies, albeit they are divided into six rather than four domains. These six competencies include (1) role clarification, (2) team functioning, (3) patient/client/family/community-centered care, (4) collaborative leadership, (5) interprofessional communication, and (6) interprofessional conflict resolution (Canadian Interprofessional Health Collaborative, 2010). The competencies required for interprofessional collaboration are similar worldwide and do not vary according to the country.
Alcohol and other drug misuse remain a public health challenge. Harmful alcohol use alone accounted for over three million deaths worldwide in 2016 (World Health Organization, 2018). Also, over 200 health conditions such as liver disease, cardiovascular diseases, and tuberculosis are linked to risky alcohol consumption (World Health Organization, 2018). Drug overdoses have continued to rise steadily in the United States. The occurrence of drug overdose deaths represented a 9.6% increase from 2016 to 2017 and accounted for 70,237 deaths in 2017 (Centers for Disease Control and Prevention, 2018). Although harmful alcohol and drug use frequently presented in clinical setting and caused severe consequences, they often are unrecognized. Nurses and other health-care professionals have an essential role in identifying and intervening with patients who use alcohol through the evidence-based practice of Screening, Brief Intervention, and Referral to Treatment (SBIRT).
The purpose of this project is to explore the effect of an online IPE substance use screening program on nursing students’ perceptions about interprofessional practice and perceptions about working with patients who use/misuse alcohol and drugs.
Methods and procedures
Upon Institutional Review Board clearance from the University of Pittsburgh, a within-subjects repeated measure quasi-experimental design was performed on a sample of 89 nursing students. Students were recruited through their instructors from two rural nursing programs affiliated with the University of Pittsburgh.
Online IPE
The nursing students learned about IPE through 6 h of online modules. Nursing students learned IPE concepts from and with health providers from behavioral health and public health professionals. The online IPE had four components. First, IPE core competencies (values, roles, communications, and teamwork) of professions were reviewed. Second, four simulated patient case studies with the roles of nurse practitioners, behavioral health specialists, and public health providers were presented. Third, nursing students learned about substance use assessment in Screening, Brief Intervention, and Referral to Treatment (Gordon & Alford, 2012) with a team of professionals (nurse practitioner, behavioral health counselor, and public health provider coordinating care). Fourth, nursing students during the online interprofessional dialogue heard professionals (nurse practitioner, behavioral health counselor, and public health worker) discuss case management of patients with substance use emphasizing roles of the team members.
The online IPE program was evaluated at three time points: pretraining, posttraining, and postinterprofessional dialogues. The following instruments were utilized:
Demographic questionnaire
The demographic questionnaire was constructed by the study team to gather basic information about characteristics such as gender, age, and race of the nursing students.
Alcohol and Alcohol Problem Perceptions Questionnaire
The Alcohol and Alcohol Problem Perceptions Questionnaire (AAPPQ) is a 30-item questionnaire, measuring clinician perceptions about patients who use/misuse alcohol. The AAPPQ is comprised of two subscales: Role Security and Therapeutic Commitment. The Role Security subscale contains items that measure how adequate and appropriate one feels in the role of working with people who use/misuse alcohol. The Therapeutic Commitment subscale consists of items that measure the motivation and satisfaction in working with individuals who consume alcohol. Higher subscale scores indicate positive perceptions toward working with people who use/misuse alcohol. The AAPPQ integrates education/training, experience, and the work environment as support for the development of Role Security, which leads to an increase in Therapeutic Commitment. Original AAPPQ development by Cartwright and colleagues (Anderson & Clement, 1987; Gorman & Cartwright, 1991) and more recent application of AAPPQ in different clinical settings (Childers et al., 2012; Keurhorst et al., 2014; Puskar et al., 2013) have demonstrated adequate reliability and validity. The reliability for the AAPPQ individual subscales ranged from 0.69 to 0.90 when used for measurements of a sample similar to that of the present study (Puskar et al., 2013).
The Drug and Drug Problems Perception Questionnaire
The Drug and Drug Problems Perception Questionnaire (DDPPQ) measures professionals’ perceptions about drug use and consists of two subscales: Role Security and Therapeutic Commitment. It was intentionally constructed to contain items that are largely identical in structure to the AAPPQ (Watson, Maclaren, Shaw, & Nolan, 2003), although due to revisions over time, it contains 22 items compared with 30 on the AAPPQ. The DDPPQ has demonstrated adequate reliability among undergraduate students ranging from 0.64 to 0.93 (Puskar et al., 2013).
The Interprofessional Education Perception Scale
The IEPS, developed in response to the burgeoning field of IPE, is an 18-item measure comprised of four subscales: Competence and Autonomy, Perceived Need for Cooperation, Perception of Actual Cooperation, and Understanding Other’s Values. Higher subscale scores represent better perceptions toward interprofessional practice. Internal consistency of the scale is 0.80 (Luecht, Madsen, Taugher, & Petterson, 1990), and the reliability of individual subscales has ranged from 0.40 to 0.80. The IEPS is a tool that is frequently used to measure students’ perceptions of interprofessional practice and has been used in different countries: Australia (Hallam et al., 2016; Williams & Webb, 2013) and Canada (Solomon & Salfi, 2011; Tsang, Cheung, & Sakakibara, 2016).
The Statistical Package for the Social Science (version 22.0; SPSS Inc, Chicago, IL) was used for analyses. All statistical inferences were made based on a two-tailed alpha of 0.05. Descriptive statistics were used to describe the nursing student sample. The outcome variables were reasonably normally distributed, and no outliers were observed. There was an acceptable amount of missing data which was judged to be missing at random. Within-subjects repeated measures analysis of variance was utilized to compare mean scores on the three measures: the AAPPQ, DDPPQ, and IPES. Post hoc pairwise comparisons were performed with Bonferroni-adjusted significance level.
Results
The students were 87% female (n = 77/89) and 91% white (n = 81/89); their average age was 24.9 years (standard deviation = 10.36). Table 1 presents the changes in subscale scores of AAPPQ, DDPPQ, and IEPS over time. Overall, the online IPCP training was associated with improved perceptions toward working with patients who use/misuse alcohol and other drugs and toward IPE. Specifically, scores from the Role Security and Therapeutic Commitment subscales of the AAPPQ showed statistically significant increases (Role Security, F(2, 73) = 8.43, p < 0.05; Therapeutic Commitment, F(2, 73) = 7.97, p < 0.05) across the three time points, which were attributable to increases from pretraining to posttraining (Bonferroni-adjusted pairwise comparisons: Role Security, t(30) = 4.89, p = 0.015; Therapeutic Commitment, t(30) = 3.32, p = 0.006).
Measurement descriptives over time and comparison (N = 89).
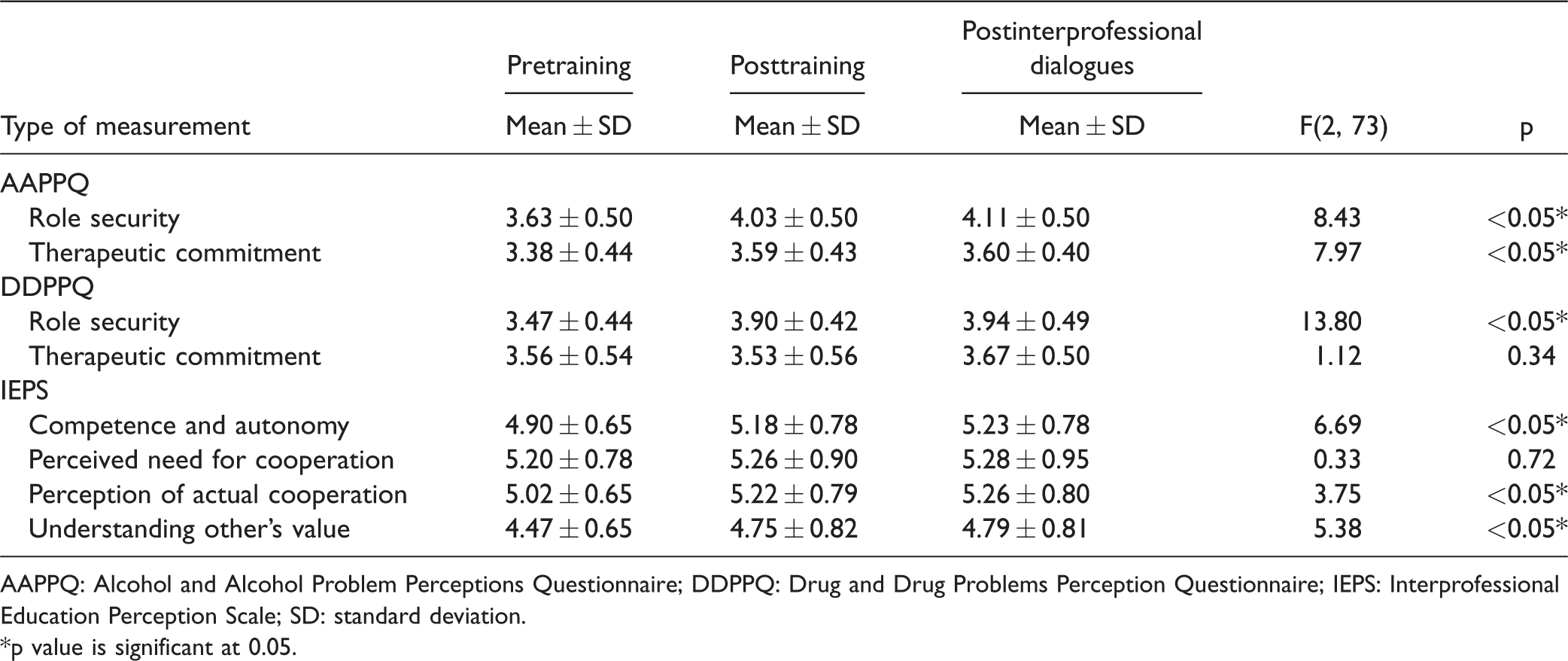
AAPPQ: Alcohol and Alcohol Problem Perceptions Questionnaire; DDPPQ: Drug and Drug Problems Perception Questionnaire; IEPS: Interprofessional Education Perception Scale; SD: standard deviation.
*p value is significant at 0.05.
In contrast, the Role Security but not Therapeutic Commitment subscale of the DDPPQ showed a statistically significant increase (respectively, F(2, 73) = 13.80, p < 0.05; F(2, 73) = 1.12, p = 0.34) over time. The difference in Role Security also was attributable to the increase from pretraining to posttraining (Bonferroni-adjusted pairwise comparison: t(30) = 4.81, p < 0.05).
Additionally, the following three subscales of the IEPS exhibited statistically significant increases from pre- to posttraining: Competence and Autonomy (F(2, 73) = 6.69, p < 0.05); Perception of Actual Cooperation (F(2, 73) = 3.75, p < 0.05); and Understanding Other’s Value (F(2, 73) = 5.38, p < 0.05). Similar to the above results, all differences were attributable to increases from pretraining to posttraining (Bonferroni-adjusted pairwise comparisons: Autonomy, t(30) = 3.91, p < 0.05; Actual Cooperation, t(30) = 2.31, p < 0.05; Value, t(30) = 2.17, p < 0.05). No significant changes in mean scores of these three IEPS subscales were observed from posttraining to postdialogues, indicating that the increases in mean scores from pre- to posttraining sustained through the postinterprofessional dialogues.
Discussion
This study examined the effect of an online IPE program on nursing students’ perceptions about interprofessional practice and perceptions about patients who use/misuse alcohol and drugs. After the online training program, nursing student scores on the role security, perceptions of competence and autonomy, actual cooperation, and understanding of other professionals’ value increased significantly and the increase sustained over time. These results are consistent with other studies in the literature. For example, Tanner, Wilhem, Rossie, and Metcalf (2012) examined pretest and posttest scores among health professional students in relationship to addiction education and SBIRT, revealing that medical students and nursing students had similarly low baseline scores on knowledge, confidence, and clinical performance, all of which improved posttraining (Tanner et al., 2012).
Substance misuse is a serious public health concern (Tanner et al., 2012). To prepare health professionals (especially professionals-in-training) to effectively implement SBIRT when encountering patients who misuse substances, barriers to learning and implementing these evidence-based interventions—specifically SBIRT—need to be addressed. Persons with substance use disorders are often stigmatized, and health-care professionals may have discomfort and lack the confidence to work with this population. Educating nursing students about SBIRT for patients with substance use disorders and the importance of integrating interprofessional collaboration is essential.
While our findings cannot be generalized globally, prior studies that compared IPE (Brault et al., 2016) and practice (Harris et al., 2016) in the United States and Canada indicated that active leadership involvement within academic and practice settings is crucial to interprofessional activities. Likewise, WHO examined cases of IPE and practice in Brazil, Canada, India, South Africa, and the United States and indicated that shared vision and linkage between academia and clinical sites can facilitate implementing IPE and collaborative practice (World Health Organization, 2013). Therefore, as more professionals are exposed to IPE and SBIRT, SBIRT can be further integrated into their interprofessional practice, thus promoting better patient outcomes in areas such as substance misuse. Integrating IPE into the undergraduate curricula and clinical rounds prepares students to effectively communicate with other professionals, further promoting quality care (Cartier, 2016).
Several limitations are acknowledged. First, while students’ perceptions about substance use and IPE improved with the educational training, the sample size was small. Second, transfer of students’ perceptions into clinical practice after graduation was not measured. Further longitudinal research with a larger sample is suggested to determine the effect of IPE on clinical practice change.
Conclusion
The perceptions of the students about IPE training and perceptions toward working with persons with substance use problems improved with the educational content. Overall, our results demonstrate that online IPE efforts have the potential to improve perceptions of interprofessional practice as well as perceptions about alcohol and drug use/misuse. If more nursing students embraced the importance of interprofessional practice as background for treating patients with substance use problems, students would be better equipped as practicing professionals to screen and address substance misuse before it progresses to dependence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported in part by funds from the Division of Nursing (DN), Bureau of Health Professions (BHPr), Health Resources and Services Administration (HRSA), and Department of Health and Human Services (DHHS) under cooperative agreement number UD7HP25060. The information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by, the DN, BHPr, HRSA, DHHS, or the U.S. Government.