
Abstract
Introduction
Physical assaults perpetrated by patients in psychiatric hospitals against mental health staff (MHS) is a serious concern facing psychiatric hospitals. Assaulted staff reports physical and psychological trauma that affects their personal and professional lives. There is a dearth of literature exploring this phenomenon.
Purpose
To explore MHS perspectives of assault by psychiatric patients.
Methods
A transcendental phenomenological qualitative design was used to explore and analyze the perspectives of a purposeful sample of 120 MHS perspectives at an acute inpatient psychiatric hospital. Participants’ age ranged from 22 to 63 years (mean age = 32.4). Moustakas’ theoretical underpinnings guided the study.
Results
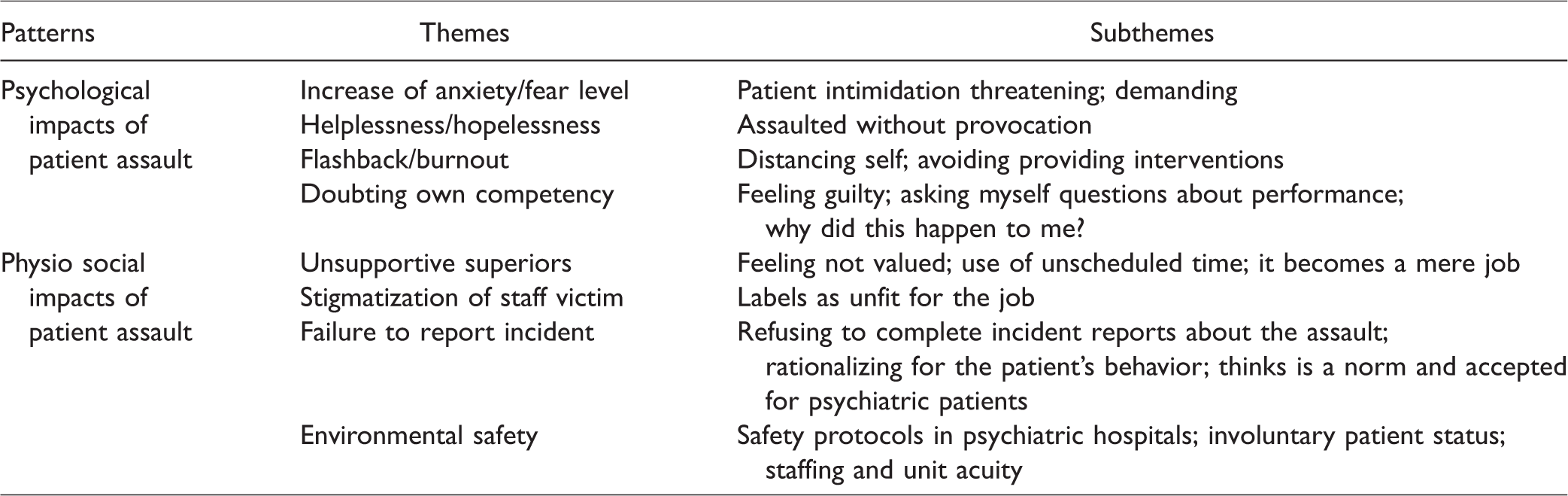
Two patterns, 8 themes, and 19 subthemes were identified: (a) Psychological impacts revealed four themes—increase of anxiety/fear level, helplessness and hopelessness, flashbacks/burnout, and doubting own competency. (b) Physiosocial impacts revealed four themes—unsupportive superiors, stigmatization of staff victim, failure to report the incident, and environmental safety.
Discussion
Participants verbalized that assaults by patients have instilled fear and trauma in them. Most of the assaults occurred when staff were performing their routine job functions and setting limits to patient’s behavior.
Conclusion
The study allowed MHS opportunities to narrate their lived experiences of being assaulted by patients and provided validation of their perspectives. Findings illuminated the phenomenon and may help to support policy changes in psychiatric hospitals.
Keywords
Introduction
Mental health staff (MHS) are faced with the possibility of encountering assaultive events during their day-to-day activities with psychiatric patients. Psychiatric patients’ assaults against staff are one of the greatest concerns facing inpatient psychiatric hospitals (Ezeobele, McBride, Engstrom, & Lane, 2019; Hackethal, 2016). Studies have shown that the assaulted staff experienced immediate physical and long-lasting psychological trauma, which may likely impact their professional and personal lives (Holleran & Mars, 2006; Jacobowitz, 2013; Jansen, Dassen, & Jebbink, 2005). Patient-on-staff assaults may occur in many forms and ranged from verbal assaults (bullying, cursing, threatening, and harassing) to unprovoked physical assaults. Verbal assaults are the most common form of workplace violence in healthcare settings (Anderson & West, 2011). In the past decade, the magnitude of assaults from patients has received both state and national attention in the medical literature (Ryan, Sparrow, Messick, Aaron, & Burnette, 2004).
The few studies that have examined the impact of assaults by patients against MHS have been alarming. Richter and Berger’s (2006) study identified that 70% of the staff assaulted were nurses, followed by social workers, physicians, and housekeeping staff. The assault data extracted from participating psychiatric inpatient hospitals from 2011 to 2013 National Database of Nursing Quality Indicators revealed that 5301 injurious assaults occurred. Of the total assaults, 3867 (70%) were classified as assaults against hospital staff. The overall rate of assaults by patients against hospital staff from this database was 0.55 assaults per 1000 patient days (Staggs, 2015).
Some studies have indicated that all direct care staff working in inpatient psychiatry hospitals are at higher risk for targeted assault by patients compared to other healthcare workers working in other settings (Kowalenko, Gates, Gillespie, Succop, & Mentzel, 2013; Phillips, 2016). Studies have also concluded that 69.5% of MHS have experienced physical assaults by patients which varied in severity (Hackethal, 2016; Kelly, Fenwick, Brekke, & Novaco, 2015). The U.S. Bureau of Labor Statistics Report (BLS) indicated that psychiatric assault incident rates were reported as 68.2% per 1000 patient days (BLS, 2015).
Background
In the psychiatric care setting, one study found that 62% of clinical staff were assaulted at least once with 28% reported being assaulted in the six months before the study (Caldwell, 1992). One research study had found 94% of psychiatric nurses had been assaulted at least once in their careers with 54% stating that they have been assaulted over 10 times (Jansen et al., 2005). Further research has indicated that 8 out of 10 nurses experienced some form of physical violence in the past 12 months. These findings represent physical assault only; threatening, intimidating, or verbal aggression are not represented and are often a prelude to physical assault (O’Connell, Young, Brooks, & Hutchings, 2000).
A review of a large international 424 studies reported an incident rate of over 32% of the patient against staff assaults in psychiatric hospitals (Bowers & Crowder, 2012). In acute psychiatric settings, 10% of the patients were responsible for 58% of assaultive incidents (Decaire, Bedard, Riendeau, & Forrest, 2006). Up to 70% of staff in forensic psychiatry have reported they were assaulted by patients (Kelly, Subica, Fulginiti, Brekke, & Novaco, 2015). Psychiatric aides and technicians were identified to experience higher rates of nonfatal occupational workplace injury and illness due to assault by patients (Longton, 2015). The report further explains that the incident rate of assault for psychiatric technicians (PTs) was 38 times higher than the national average for the nonlicensed staff working in nonpsychiatric hospitals (Longton, 2015).
Additionally, a study by Roy (2013) concluded that 69.5% of MHS had experienced patients’ assaults within the past 12 months. Some studies found that physicians at all levels were potentially exposed to workplace assault (Kowalenko et al., 2013; Phillips, 2016). The results from a study conducted in the United States on aggression and staff attitudes indicated that 13% participants reported they had experienced verbal abuse, 35% reported physical abuse, and 45% reported they had experienced both verbal and physical abuse (Ezeobele et al., 2019).
The majority of studies on staff perspectives of patient assaults were conducted in the United Kingdom, Switzerland, and Australia (Flannery, 2005; Kavanagh & Watters, 2010). There is a scarcity of studies exploring staff perspectives of experienced assaults. Most studies of assaults in inpatient psychiatric hospitals have been directed toward quantifying the problem through patient’s perspectives and less directed to understanding staff perspectives and the sources or the underlying risks (Conrad, Mulchandani, Sankaranarayanan, & Lewin, 2014; Phillips, 2016).
Purpose of study
Although there are various types of assaults, this study focused on MHS perspectives of physical assaults from patients. The increasing number of the patient-on-staff assaults that occurred at the study hospital in 2015 prompted the authors to conduct this study. The purpose of this qualitative transcendental phenomenological study was to explore MHS perspectives of assault experience and provide an opportunity for their voices to be heard. The authors of this study focused primarily on physical assaults. The authors defined physical assault from psychiatric patients to staff as punching, pushing, kicking, hitting, spitting on, and throwing items at staff.
Philosophical framework
Transcendental phenomenology as described by Moustakas (1994) and Moerer-Urdahl and Creswell(2004) and presented by Husserl’s (1970) ideas was the philosophical underpinnings that guided the study. It adheres to what can be discovered through reflection on subjective experiences and their objectives. It asserts that the only thing we are certain about is that which appears before us in our consciousness and guarantees its objectivity. To understand the objects that appear before us, we must return to the self and recognize ourselves in the experience that is being investigated. Transcendental phenomenology is a scientific study of the appearance of the phenomena as we see it or as they appear in our consciousness (Colazzi, 1978; Husserl, 1970).
Method and procedures
Research design
A qualitative transcendental phenomenological design as described by Moustakas (1994) using Husserl’s(1970) ideas was the most appropriate for the study. It commits itself to descriptions of experiences and absorbs the common meanings of the experience (Moustakas, 1994). The basic purpose of this design was to reduce the individual experience and obtain a description of the universal essence (Moustakas, 1994). Philosophically, phenomenology seeks to gather the essence of an experience consisting of what the experience was like and how the study group experienced it. It identifies the phenomenon of study, brackets the researchers’ personal experience, and data collection. Analyzed data are reduced to identify textural descriptions of the person’s experience to convey the true essence (Moustakas, 1994). Our goal was to capture an in-depth understanding of what the staff experienced after being assaulted by patients.
Study setting
The survey was administered at a 274-bed acute inpatient freestanding university teaching psychiatric hospital located in the southwestern United States. The patients served are categorized by Child/Adolescent and Adult Units. The average length of stay for patients is 7 to 10 days with 9000 annual patient admissions.
Recruitment and data collection
Institutional review board (IRB) approval for protection of human services (HSC-MS-16–0249, Reference Number 135128) and a site-specific letter approval were obtained before initiation of recruitment, data collection, and study. The target population of this study was the 280 direct MHS employed in this acute psychiatric inpatient hospital; a combination of physicians, registered nurses (RNs), social service (SS) staff, and PTs. Recruitment was conducted on the basis of self-selection and purposeful, based on individual willingness to participate. Inclusion criteria for participation in the study were the following: (a) staff must be employed at the study hospital with direct patient care contact, (b) assault occurrence must be within the preceding year 2015 prior to the study, and (c) assault must have occurred in the study hospital and not at any other psychiatric hospitals. Exclusion criteria: MHS were excluded if (a) the assault did not occur at the study hospital and (b) staff were not responsible for direct patient care.
Recruitment was conducted on the basis of self-selection and purposeful, based on individual willingness to participate. An online survey was chosen to (a) enable contact with every inpatient direct care staff via initial e-mail and (b) to ease the participant burden by using Qualtrics-based platform with a survey link embedded in the invitation e-mail (Kivits, 2005). This strategy maximized the final number of participants to the survey questions and ensured all representative staff was invited to participate. Participants were assured confidentiality during the consent process.
The data collection phase of study lasted 12 weeks during which participants completed online consent, demographic data, and survey questions (Bowden & Galinda-Gonzalez, 2015; Cilesiz, 2010). The invitation to participate was sent online to 280 MHS and, at two weeks intervals throughout the study period, to remind staff to volunteer and complete the survey. The computer was programmed and allowed staff to stop and return to the survey at any time and continued later at where they had stopped until completion. Once a participant has completed and submitted their responses, the system did not allow the participant to complete a second survey. A cover letter conveyed the study’s (a) purpose, (b) voluntary nature, (c) anonymity and confidentiality of responses, (d) no influence on staff participation, and (e) no special treatment for staff participation. Consent was implied with completion, and due to the anonymous participation, data were collected in the Qualtrics secured system. Surveys were collected anonymously to reduce the influence of desirability and to foster honest and confidential responses. The open-ended questions were focused on understanding the phenomenon (Creswell, 2012). The following open-ended questions were used to elicit narrative responses.
Describe your personal experience of patient assault in the past year. Describe any negative affects you encountered following an assaultive experience.
These questions were formulated from extensive literature reviews, based on Moustakas (1994) to provide detailed descriptions of participants’ experience. Open-ended questions were based on the intended purpose and their relationship to the study. The questions focused attention on data gathering that led to the narratives which provided thorough understanding of the experience (Creswell, 2012). The authors did not impart any personal experiences related to assault during the process to maintain truthfulness of the data collected.
Data analysis
A transcendental phenomenology data analysis was used to explore staff perspectives of patients’ assaults. Data analysis began after data collection and was an iterative process conducted by the authors through multiple reviews of the narratives, separately and collectively, to derive the reconciled segments of meanings, patterns, and themes that emerged from the analytic process. The authors read the narratives thoroughly to extract meaning, highlighted significant statements, and sentences or quotes to gain an understanding of the participants’ experience (Moustakas, 1994). It revealed participants’ insights and the essence of their lived experience of being assaulted. During the analytic process, the authors bracketed their own experience, remained reflective, and maintained objectivity with data interpretation.
The significant statements extracted were clustered into themes for the development of meanings which allowed the authors to review and synthesize the completed results. The essence focused on the common assault experience of the participants (Creswell, 2012) to provide insight into their perspectives of being assaulted in a psychiatric inpatient hospital. The Qualtrics program provided secured storage for the data and enabled the authors to manipulate the data and display the categories (Creswell, 2012). The most significant issue with the data was reading participants’ large narratives and deducing the information. The authors reached saturation after 120 narratives were reviewed. Saturation refers to the point in data collection where no new themes emerged (Mason, 2010).
All narratives were sorted according to the interview question, and the data were tracked for emerging patterns, themes, and subthemes. The identified themes described the perspective of how the participants experienced the phenomenon known as essential description (Creswell, 2012). The narratives were de-identified and stored in a secured Qualtrics system and transferred later to the Microsoft Excel program.
Results
One hundred and sixty-three MHS (77.6%) out of a total of 280 MHS of the study hospital consented to participate in the study. One hundred and twenty (73.6%) out of 163 who consented to participate in the study fully completed and submitted their responses. All participants were employed at the study hospital and had direct patient contact. However, the number of attrition was 43 (26%) and included 6 physicians, 10 RNs, 12 SS staff, and 15 PTs. The attrition was due to (a) staff did not meet the inclusion criteria, (b) some participants signed the informed consent but did not complete the survey questions, and (c) saturation point met.
The study sample was 120 (N = 120) which include (a) 18 physicians, (b) 70 RNs, (c) 12 SS staff, and (d) 20 PTs. The gender distribution of the sample was 46 males and 74 females; their age ranged from 22 to 63 years, a mean of 32.4. The mean age was calculated according to disciplines; it was noted that the mean age of physicians was 28.4 years, RNs was 32.11 years, SS staff was 35.67 years, and PTs was 33.79 years. Participants’ educational level varied from college credits to doctorate degrees and broken down as follows: 10 associate degree, 57 bachelor degree, 30 master’s degree, and 23 doctorates. The length of experience at the study hospital ranged from 1 to 30 years, a mean of 12.23 years. Each participant completed their narratives to the questions at an average time of 45 min. The researchers read the narratives very thoroughly to extract meanings of the participants’ experience. From the narratives provided by the participants, the authors identified 2 main patterns that revealed 8 themes and 19 subthemes (Table 1).
Patterns, themes, and subthemes representative of 120 mental health staff perspectives of patient’s assault.
Pattern #1: psychological impacts of patient assaults
The intrinsic factors of negative psychological experience to patient assault are frequently ignored, and the cognitive assessment of assaultive incidents negates the emotional response. In the present study, the psychological response was mostly universal for all the participants. However, few participants reported assaultive incidents as nonsignificant. The participants’ narratives were clustered into four themes: increased level of anxiety, powerlessness and helplessness, flashbacks, and doubting own competency.
Theme 1: increase of anxiety/fear
The frequent response was increased anxiety level and a significant factor for the participants.
Participant #4 describes the experience as: I was attacked three times by different patients … firstly … a patient threw a big plastic bottle at me as I was redirecting and setting limits with a patient … secondly … I was calming a patient who was attacked by another patient, the patient suddenly grabbed and pushed me down … thirdly, a psychotic patient who had already attacked multiple staff members also attacked me. I was out of work for a long time. I felt anxious upon returning to work and my anxiety level is always high; I always think of how to do my job without being assaulted. My anxiety level is high after I was assaulted by a patient unprovoked; I am now very careful when approaching a patient … and I try to distance myself from them for fear of being attacked again … I give them time, space, listen, and speak to the patient in a respectful manner.
Theme #2: powerlessness and helplessness
Many of the participants narrated powerlessness and helplessness as they were physically assaulted by the patients.
Participant #40 recounted, It is hard to understand what it was like on the day that I was assaulted. I felt very powerless as the patient assaulted me without provocation; this patient was bent on harming staff and he did injure several staff members during his rampage … it was very difficult for the staff to contain this patient even after a code was called. Our established staffing grid makes it very difficult to get enough help.
Theme # 3: flashbacks and burnout
Participants reported that the incident has affected their health, they continually experience flashbacks and burnout, and they are frequently drawn back into the traumatic experience. Participant #48 narrated, I feel like the assault is happening all over again, I have difficulty keeping my patients in close proximity because of constant bad memory. I have the belief that the assault may occur again and I do not want to re-experience this trauma and I am planning to quit this job … I cannot take the assault any more …
Theme #4: doubting own competency
Some participants narrated that patient assault led them to question their competency in working with psychiatric patients. Staff competency is evaluated formally in the classroom at the time of hire and during annual “Skills Lab.” Ongoing evaluation of staff competency is done on daily basis during staff tours of duty. The hospital ensures that staff meets competency requirements before performing assigned duties. One participant #36 reported: “You doubt your competency level and question what you did wrong to deserve this assault … I consistently apply all that was taught to me in training, this is a tough population to work with …”
Several participants did not narrate negative emotional responses after an assault. They did not consider patient assaultive incidents as important and rationalized that the patient’s behavior is part of the reason patient was admitted. Participant # 80 narrated: These patients are sick and I do not hold the assault against them or taking it personal … Aggression is part of working with psychiatric patients. I am here to help … I know they may be responding to internal stimuli that are commanding them to do what they did … some of the patients take street drugs that cause irrational behavior. It should be accepted as one of the behavioral patterns expected. I will not doubt my competency working with such patients. I will consider working with this particular patient again if assigned. It will help me to re-establish rapport …
Pattern 2: physiosocial impacts of patient’s assaults
The second interview question was set to describe the negative effects that staff encountered following the assault experience. Narratives were clustered into four themes: lack of support from superiors, stigmatization of staff victim, failure to report assault incident, and environmental safety.
Theme 1: impact related to unsupportive superiors
Some participants reported disappointment and dissatisfaction in the way assault incidents were handled by superiors. Participants’ reported that superiors see staff as the perpetrator of the assault and not as a victim. This perceived lack of support affects participants’ morale and team efforts. Participants reported that often times, team members may not intervene during patients’ aggressive episodes for fear of being blamed or stigmatized as “unfit” for the job and for any injury they sustained during the episode. Participants asserted that negative response from superiors was counterproductive.
Participant #5 reported: Our superiors always blame us for any injury we sustained from a patient assault, label us as “unfit” for the job and the perpetrator of the assault. This dampens our spirit, causes demotivation, low morale … and for many of us, the work becomes, “a mere job” and this behavior makes us want to quit … I do not want to be stigmatized and or labeled as an inept by my supervisor and coworkers … will rather call-in sick the next time I am scheduled to work …
Theme #2: impacts related to stigmatization of staff victim
Participants reported that when staff is physically assaulted by a patient, the staff is automatically stigmatized by superiors and sometimes, coworkers. The expectation for staff who work with the psychiatric patients is the ability to handle their behavioral situation, and getting injured is not acceptable. Participant #100, narrated: The myth regarding working in psychiatry is the expectation that staff who work with these patients have the ability to handle any aggressive situation. This results in staff believing that getting injured is normal and accepted. I have been assaulted three times by the patients. My superiors and some coworkers stigmatize me and consistently state that I am always getting assaulted by patients. Sometimes these coworkers resist me working with them and it makes it hard for me … and frustrates me.
Theme #3: impact related to failure to report assault incident
The participants reported that psychiatric patients might not be aware of their aggressive behavior, and the patients may be hearing internal voices commanding them to attack staff. They reported fear of retaliation and that they do not want the assault to be counted against them as a pattern.
Participant #19 narrated, I am reluctant to complete an assault incident report … I will not fill out assault paperwork. The patients are sick and may not know what they are doing … and this is a reason for their hospitalization … staff should be able to work with them and speak to them with compassion and respectful tone of voice. Moreover, the assault is counted against the staff and when you have more than one assault, it becomes a pattern.
Theme #4: impact related to environmental safety
Safety and the well-being of staff are compromised when staff experiences patient assault. The inpatient psychiatric hospital settings for patients provide a structured and supportive environment. Several participants reported an unsafe work environment, inconsistent staffing and the acuity of the unit with involuntary patients committed for treatment. Participants narrated that the safety of the patients and staff should be paramount in psychiatric hospitals. Participant #13 reported, My priority is safety for the patients, staff and others … a patient punched me on my nose and broke it … I bled profusely … and was sent out to a medical hospital via 911, I did not feel safe on the unit and had difficulty performing my job functions. I was referred to employee assistance program and it was very helpful … my family was very upset when they saw my broken nose and they want me to quit … and I am seriously thinking about quitting this job … it is very dangerous with these psychiatric patients … Staffing is very poor and inconsistent … due to core staff calling in sick and burnout … these patients are involuntary commitment and very sick … they also have a comorbid illness with their psychiatric illness … they are very demanding … patients focus on the staff for their admission into the hospital and consistently try to intimidate us … the patients demand discharge … and refuse to listen to any explanation from us … they instill fear on the staff … the patients demand a lot most of the time … and any delay in getting their needs met has resulted in patients’ assaultive behavior. This is what happened to me. I was trying to juggle my work and prioritize my assignments … the patient could not wait anymore and suddenly hit me …
Discussion
One hundred and twenty staff completed the study, and the results indicated that the majority of participants reported they had been assaulted by patients in the previous year. Most of the assaults occurred when the staff were either performing their routine job functions or setting limits to patient’s unacceptable behavior. The assaulted staff in the study reported negative psychological impacts are linked to anxiety, fear, helplessness, and powerlessness. These findings are supported by the findings from other studies (Flannery, 2005; Ryan, Sparrow, Messick, Aaron, & Burnette, 2004).
The participants’ narratives indicated that most of them have adapted to stressors of physical assault occurring with flexibility and with less traumatic stress reactions. A study has shown that whenever an assaulted staff is compelled to remember a traumatic event, it reinforces a recollection of fear and stress reactions because the body holds the story that words may not be able to express (Klein, 2015). MHS who experienced assault by patients in inpatient psychiatric hospitals may be compromised in their ability to care for the patients appropriately. Experiencing assault can promote fear of future assaults that enhance somatic symptoms and cause an intent to leave the organization in which the assault took place (Rogers & Kalloway, 1997). The study has identified that staff exposure to assaults by patients has resulted in decreased job satisfaction, occupational stress, and anxiety (Nijman, Bowers, Oud, & Jansen, 2005).
Participants stated patients might become assaultive due to multiple factors such as comorbidity or misconception of situations on the unit. The participants reported feelings of powerlessness and helplessness as they were being attacked by the patient. Several participants provided a rationale that psychiatric patients’ assaultive behaviors should be accepted as a social norm, stating that patient is admitted into a psychiatric hospital because of these behaviors. Our findings are supported by an earlier study by Snow (1994), whose findings indicated that the staff placed their safety at risk to help the patients. The participants also reinforced that many injuries caused by psychiatric patients are unintentional and unavoidable; therefore, they are able to accept them as routine psychiatric behaviors. Some of our study participants were not willing to brand patients due to their illness or impairment. This finding is supported by Occupational Safety and Health Administration (OSHA, 2015) study where patients were noted to be experiencing or responding to command auditory hallucinations, which is a false sensory perception (Townsend & Morgan, 2018).
The importance of environmental safety was resonated by all participants. They described environmental safety as keeping staff and patients safe to achieve positive clinical outcomes (Ekahau, 2015). The psychiatric unit environment integrally places staff at risk for workplace assault. The safety and the well-being of staff may be compromised when they experience being assaulted by patients. The inpatient psychiatric hospitals have been known to provide structured and supportive environment. The environmental practice including the structure, level of stimulation, patient autonomy, and safety provisions can impact the occurrence of assault (Hamrin, Iennaco, & Olsen, 2009). The environment has restrictions that often infringe on the patients’ rights or freedom, such as locked doors, and the patients are not allowed to leave the environment as they would like to. These are known universal patient safety guidelines in psychiatric hospitals. The enforcement of unit rules, denial of privileges, and the involuntary patient commitment status for treatment have positively correlated with assaults in psychiatric settings (Flannery, 2005).The structure of the environment plus inconsistent staffing has an impact on the propensity of assault in inpatient psychiatric hospitals (Johnson & Weichelt, 2004).
A major concern the participants reported was unsupportive superiors, and occasionally, peers stigmatize them for patient assault. Even though the staff was blamed for the injuries they had received from patient’s assault, the lack of support demotivates the innate urge to perform duties to full potential. The motivation is no longer present and the job becomes ‘a mere job’ for them. These findings are supported by Heponiemi, Kouvonen, Virtanen, Vanska, and Elovainio (2014); the study indicated that workplace assault is associated with increased rates of burnout, decreased quality of life, and poor job satisfaction.
Participants failed to report assault incidents for fear of stigmatization and retaliation from superiors and peers. This perceived fear prevents most staff from reporting patient assaults or talking about them. This finding is supported by previous studies which indicated that patients’ assaults are prone to underreporting because of the lack of faith in the reporting system and fear of retaliation by superiors (Anderson & West, 2011; OSHA, 2015; Richter & Berger, 2006; Ryan et al., 2004). Another study determined that 34% of clinical staff was physically assaulted, but less than 50% reported the incident (Privitera, Weisman, Cerulli, Xin, & Groman, 2005). Staff will rather use unscheduled time off than report the incident or to work the next time scheduled. Studies have linked unscheduled time off to affect clinical outcomes, the work team, and the organization (Charney & Shimer, 2007; Duclay, Hardouin, Sebille, Anthoine, & Moret, 2014).
Implications for practice
The findings of this study have important implications for MHS and psychiatric healthcare system. This study reinforces the call to listen to staff assault experience and the concerns they consistently encounter with psychiatric patients. To avoid being assaulted, MHS may be resistant to implement restrictions on patients. To prevent being assaulted, staff should be mindful of their communication techniques, both verbal and nonverbal, to use respectful tone while interacting with patients as one of the proactive interventions to decrease the incidents of patient initiated assaults. It is important for staff to recognize their own biases regarding psychiatric patients and know when to remove themselves from an aggressive patient’s situation by allowing another staff member to intervene with the patient. Staff traumatic experience from patients is likely to have negative impact on the hospital and may result in decreased job productivity and citizenship behavior.
Patient assault in psychiatric hospitals is pervasive and persistent problem that has been either tolerated or largely ignored by healthcare organizations (Phillips, 2016). The responses from the participants served as a guide for better understanding some of their experiences during and after being assaulted by a patient. It is important for superiors to listen actively to the staff who have been assaulted, provide honest support, and be open to suggestions for prevention of reoccurrences.
Providing assaulted staff scheduled time off will allow the person time to review and assess the event that led to the assaultive incident as well as to examine their feelings and concerns. Varieties of social, cultural, and economic changes in the delivery of psychiatric care may be direct contributors to the reports of increase rate of assaults toward staff (Shi et al., 2015). In some cases, when staff exhibit an attitude of politeness, respect, and compassion, it decreases assaults (Duxbury, Hahn, Needham, & Pulsford, 2008; Ezeobele, Malecha, Mock, Mackey-Godine, & Hughes, 2014; McCann, Baird, & Muir-Cochrane, 2014; Meyer, 2014; Peplau, 1964; Sharac et al., 2010). The foundational keys in delivery of psychiatric care by direct care staff is the use of respectful tone of voice and therapeutic communication techniques as interventions to decrease and prevent some patient against staff assaults (Peplau, 1964). Effective communication skill is the cornerstone of psychiatric care practice. Inappropriate communication techniques between staff and the patients have resulted in assaultive behaviors from the patients (Ezeobele et al., 2014).
Limitations/potential difficulties
The study was conducted in one single location which limits generalization of the findings. The method used for recruitment in this study may be subject to sampling bias. The participants may be aware of researchers’ interest, which could have affected their narratives in a way they thought would be desirable. The interview questions were developed by the authors specifically for the present study and have not been tested. Additionally, the online data collection method may be a limitation as there were no face-to-face interviews conducted. Future studies to employ appropriate methodologies to investigate the factors involved in patient initiated assaults are needed.
Conclusion
The findings from this study have provided important confirmation of the perspectives of staff of their physical assault experience. The narratives provided are valuable first steps in the process of understanding the phenomenon that is increasingly occurring in psychiatric inpatient hospitals. Our findings illuminate the importance of staff narratives and validate the need for enhancement of these concerns. Findings may be used as guidelines to support policy changes in psychiatric hospitals. This study has provided insight into the need for superiors to understand the assaulted staff experience. Superiors’ support to the assaulted staff is empowering and motivating and leads to a greater sense of self-direction and control. It is likely to contribute to staff quick recovery and connectedness. It is imperative to recognize that any patient-on-staff assault will not only affect the staff victim but will also affect their work team.
Footnotes
Acknowledgments
The authors express sincere thanks to the psychiatrists, psychiatry residents, nurses, social service staff, and psychiatric technicians at the hospital. Participants in this study illuminated their assaultive experiences. Study provided an avenue to express their experience. Findings will be used to support any policy changes necessary and for staff training.
The authors express our heartfelt appreciation and gratitude to various departments—nursing, medical, and social service that participated in our study. A special “thank you” to the Information Technology Department, Carina Ayers, Assistant Director, who added the survey into the online system and ensured that e-mails were distributed automatically, reminding and encouraging staff to complete the survey if they have not completed the survey.
The authors also appreciate the support from the Chief Executive Officer, Dr. Jair C. Soares, MD; Chief Operating Officer, Mr. Stephen Glazier; and the Chief Nursing Officer, Mrs. Elizabeth Maree, MSN, RN for supporting them in their study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The approval to conduct this study was obtained from the study hospital Research Committee and the University IRB, Committee for Protection of Human Services (HSC-MS-16–0249, Reference Number 135128), before recruitment and data collection began to ensure ethical protection of human subjects participating in the study. Confidentiality was ensured and implemented throughout by anonymity and de-identification of participants’ data collected electronically via a secured Qualtrics system (Qualtrics, Provo, UT).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.