
Abstract
Background
Nurses are regularly exposed to diverse potentially psychologically traumatic events (PPTEs) as a function of their work. Cumulative exposure to PPTEs can lead to clinically significant symptoms of mental disorders.
Purpose
We designed the current study to investigate the prevalence of different PPTEs among Canadian nurses and estimate the associations between diverse exposures and several mental disorders.
Methods
Canadian nurses (i.e., registered nurses, registered psychiatric nurses, licensed practical nurses, nurse practitioners) completed an online, self-reported survey. In total, 4067 participants (94.8% women) completed all relevant survey measures.
Results
Nurses reported exposures to several PPTE categories including severe human suffering, life threatening illness or injury, and physical assault, often 11 or more times. There were significant (p<.05) associations between diverse traumatic events and all mental disorders (i.e., Posttraumatic Stress Disorder, Major Depressive Disorder, Generalized Anxiety Disorder, Panic Disorder) except Alcohol Use Disorder.
Conclusions
The current findings suggest that Canadian nurses are substantially exposed to traumatic events, which vary by several sociodemographic categories. PPTE exposures were significantly associated with mental disorders; that is, if PPTEs were eliminated among Canadian nurses in the sample, symptoms would be reduced between 42.0% and 58.0%.
Keywords
Background and purpose
A potentially psychologically traumatic event (PPTE) occurs when an individual is directly or indirectly exposed to actual or threatened death, serious injury or sexual violence (American Psychiatric Association [APA], 2013; Canadian Institute for Public Safety Research and Treatment [CIPSRT], 2019). PPTEs are relatively common, with up to 90% of the North American population exposed to one or more PPTE within their lifetime (Van Ameringen et al., 2008). Exposure to PPTEs may result in the development of Posttraumatic Stress Disorder (PTSD; APA, 2013), or other mental disorders, such as Major Depressive Disorder (MDD), Generalized Anxiety Disorder (GAD), Panic Disorder (PD), or Alcohol Use Disorder (AUD; Nixon et al., 2004; O’Donnell et al., 2004; Perkonigg et al., 2000).
Individuals working in several types of occupations repeatedly face exposure to PPTEs. The Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5) criteria for PTSD was revised from the previous version to include exposure to cumulative PPTEs rather than a single, identifiable traumatic experience (APA, 2013). The change is particularly important for those exposed to multiple traumatic events as part of their jobs, such as public safety personnel (PSP) and nurses. Recent research (Carleton, Afifi, Taillieu, et al., 2019) has highlighted mental disorders and PPTE exposure within public safety personnel (PSP; e.g., communications officials, firefighters, paramedics, police). Canadian PSP have been estimated to have higher rates of mental disorders than the general population (i.e., 44.5% vs. 10.1%; (Carleton et al., 2018; Pearson et al., 2013). Repeated exposure to PPTEs has been associated with mental health disorders; accordingly, eliminating PPTE exposures for PSP might substantially reduce the number of positive screens for PTSD, MDD, GAD, PD, and Social Anxiety Disorder (SAD; Carleton, Afifi, Taillieu, et al., 2019). Nurses also regularly face high-stress situations and multiple exposures to PPTEs as part of their daily work activities. Consequently, researchers suggest that nurses may experience mental disorders (e.g., PTSD, MDD, GAD) at higher rates than the general population (Janda & Jandová, 2015; Laposa & Alden, 2003; Mealer et al., 2009; Tsaras et al., 2018; Van Ameringen et al., 2008).
Information regarding Canadian nurses’ mental health and associated factors, such as rates of PPTE exposure, remains scarce. The limited available research has reported the top five work-related stressors within Manitoba nurses as: (1) the death of a child, particularly when the child died from physical abuse; (2) violence at work; (3) treating patients that resemble family or friends; (4) death or injury of a patient after undertaking extraordinary efforts to save a life; and (5) heavy patient caseloads (Manitoba Nurses Union, 2015; Powell, 1996). Physical and emotional abuse, practice issues, conflict, and death of patients have also been identified as frequent types of PPTE experienced by nurses (Michael & Jenkins, 2001). Violence too is an identified specific risk factor for PTSD among a sample nurses, with 52% of participants reporting physical assault and 76% reporting verbal abuse from patients while at work (Manitoba Nurses Union, 2015). Emergency department nurses were more likely to report experiencing aggressive behaviour from patients than nurses from other departments (i.e., internal medicine, surgery, pediatrics, obstetrics/gynecology; Winstanley & Whittington, 2004).
Support for nurses following PPTEs appears highly variable across work environments (Doka et al., 1994; Happell, 2009). Mental health training for nurses has largely focused on the medical response, increasing skills and confidence for nurses working with patients diagnosed with mental health problems (Hemingway et al., 2014; Payne et al., 2002); however, almost no research has assessed the impact of mental health training on nurses, despite nurses reporting needs for training in how to cope with stress and burnout (Ford et al., 1997). Participating in critical incident stress debriefings and having routine structured debriefing meetings may help facilitate resilience among nurses and decrease the risk of PTSD (Jacobowitz, 2013). A study with Canadian emergency department nurses evidenced that 67% of participants reported inadequate support following a traumatic event at work and 20% reported considering leaving the profession because of the event (Laposa et al., 2003). Only 18% of participating nurses reported attending critical incident stress debriefing and no participants reported seeking outside help for their distress (Laposa et al., 2003). Identifying common and most distressing PPTEs experienced by nurses may provide valuable information for when to activate mental health resources.
We designed the current study, modelled after (Carleton, Afifi, Taillieu, et al., 2019), to (a) better understand the relative frequencies of exposure to PPTEs; (b) identify which PPTEs are most distressing; (c) assess for differences in rates of PPTEs between sociodemographic variables within nurses and nurse type; (d) assess for the relationship between PPTEs and positive screens for PTSD, MDD, GAD, PD, and AUD; and (e) assess the population attributable fractions associated with different PPTEs among Canadian nurses. The results will provide information that can inform supports, policies, and procedures for the mental health of nurses. The results will also contribute to understanding the experiences of Canadians working in potentially high-risk occupations, such as nursing.
Methods and procedures
Data and sample
Data were collected through a web-based, self-report survey between May and September 2019. The survey was available in English and French using validated measures that paralleled a previous survey of public safety personnel (Carleton et al., 2018). Occupation-specific revisions were made to the survey, in collaboration with the Canadian Federation of Nurses Unions (CFNU) executive team, to ensure all relevant nursing variables were included for the survey. The study was approved by the University of Regina Institutional Research Ethics Board (File #2019–052). The survey was distributed by CFNU to each of their member unions through emails, social media, and a video from CFNU President encouraging participation. Limited outreach was made to non-CFNU member nurse unions in British Columbia and Quebec, as well as nursing associations and colleges across Canada, all in order to encourage pan-Canadian participation. Interested participants were directed to a website with study details where they were issued a unique computer-generated random code to facilitate anonymous, nonduplicate entry into the survey. Participants provided informed consent before entering the survey. A total of 7358 participants (92.0% women) started the survey, and n = 4067 (94.8% women) completed the relevant measures on PPTE exposure and mental disorders.
Exposures to PPTE
Lifetime exposure to PPTEs was measured using the Life Events Checklist 5 (LEC-5) (Weathers et al., 2013). An exposure was recorded if participants indicated they had been directly exposed to, witnessed, or learned about a specific type of event. Changes to the wording of some items were made to reflect experience with the population. “Natural disaster” was revised to, “a life-threatening natural disaster;” and “transportation accident” was revised to, “a serious transportation accident.” In addition to the PPTE listed in the LEC-5, four events were included that may be specific to the nursing context (Manitoba Nurses Union, 2015): (1) the death of a child; (2) the death of an individual after extraordinary efforts were made to save their life; (3) the death of someone who reminded you of friends or family; and (4) exposure to life-threatening epidemic (e.g., SARS, Ebola). Participants who selected, “Any other very stressful event or experience,” were asked to provide details. Participants were then asked to choose the worst, most distressing event, or the event causing them the most difficulty currently.
Mental disorder symptoms
Well-validated tools were used for the purpose of screening for mental disorder symptoms. Screening is not diagnostic in itself, but would suggest to a mental health professional or physician that symptom criteria are met and follow up is recommended. The PTSD Checklist for DSM-5 (Weathers et al., 2013) was used to assess PTSD symptom severity over the past month, based on the trauma participants chose as the worst, most distressing event on the LEC-5. A positive screen required participants to meet the minimum criteria for each DSM-5 PTSD cluster and exceed a total score of 32 (Weathers et al., 2013). The 9-item Patient Health Questionnaire (Kroenke et al., 2001) was used to assess depression symptoms over the past 14 days. A total PHQ-9 score greater than 9 was indicative of a positive screen for Major Depressive Disorder (Manea et al., 2015). GAD symptoms over the past 14 days were assessed using the 7-item GAD scale (GAD-7) (Spitzer et al., 2006). A total GAD-7 score above 10 indicated a positive screen (Swinson, 2006). The PD Symptoms Severity Scale-Self-Report (PDSS-SR) (Shear et al., 1997) assessed PD symptoms over the past seven days, with a score greater than 7 suggesting a positive screen for PD (Shear et al., 1997). The Alcohol Use Disorders Identification Test (AUDIT) (Babor et al., 2001) was used to assess alcohol use over the past year. A total score above 15 indicated a positive screen for AUD (Babor et al., 2001)
Sociodemographic covariates
Sociodemographic covariates included gender (men or women), age (19 to 29 years, 30 to 39 years, 40 to 49 years, 50 to 59 years, or 60 years and older), marital status (married/common-law, remarried, separated/divorced/widowed, or single), work location (urban, rural, or First Nation/Inuit Community), total years of service (less than 1 year, 1 to under 5 years, 5 to under 10 years, 10 to under 20 years, or 20 years or more), job setting (home or community care, long-term residential care, acute care hospital, health centre, urgent care centre, or health clinic, public health/community health centre), and province of residence (Western Canada [British Columbia, Alberta, Manitoba], Eastern Canada [Ontario, Quebec], Atlantic Canada [Newfoundland & Labrador, New Brunswick, Prince Edward Island, Nova Scotia], and Northern Territories [Yukon, Northwest Territories, Nunavut]). Sociodemographic variables were used for across group comparisons (Table 2).
Statistical analyses
First, several cross tabulations with χ2 tests were conducted to examine the prevalence rates of PPTE exposures, the frequency of different PPTE exposures, and the worst PPTE exposures across nursing categories. Differences across nursing categories were assessed by changing reference groups in a series of logistic regressions. Differences in mean scores on the total number of different PPTE across nursing categories and sociodemographic covariates were computed using one-way analysis of variance (ANOVA) and an independent-samples t-test. The frequency of lifetime exposure was calculated for each PPTE for participants who reported having ever been exposed to each PPTE (i.e., 1 to 5 times, 6 to 10 times, 11 times or more).
Second, a series of multivariate logistic regression models were performed to test the association of each type of PPTE exposure with positive screenings of mental disorders. All models were adjusted for sociodemographic covariates (i.e., gender, age, province, work location, years of service, job setting) and nursing categories. Third, population attributable fractions (PAFs) were computed to estimate how much reduction might be seen in mental disorders if the PPTE exposure had not occurred (Brady, 1998; Last, 1986). The magnitude of PAF highly depends on the association between mental disorders and the PPTE exposure (Young, 2004). PAF have been used in different research fields to quantify the proportion of reduction in an outcome incidence (e.g., mental disorders, mental health service, childhood poisoning, death, and stroke) if a particular exposure is eliminated (Ahmed et al., 2011; Bolton & Robinson, 2010; Murakami et al., 2011; Sareen et al., 2008; Turner et al., 2017). PAFs were obtained from estimates derived from multivariate logistic regression models to estimate the magnitude of reductions in positive screenings of mental disorders if PPTE exposures were eliminated. All PAFs and 95% confidence intervals (CIs) were computed using the punaf module in Stata (Newson, 2013).
Results
Exposure frequencies to PPTEs
Table 1 includes exposure frequencies to PPTEs as self-reported by nurses. Significant differences were identified across many of the nursing category comparisons. The most commonly reported PPTE type across the nursing categories were physical assault (92.7%), the death of an individual after extraordinary efforts were made to save their life (88.9%), the death of someone who reminded you of friends or family (86.0%), sudden accidental death (81.9%), life threatening illness or injury (81.1%), and other unwanted or uncomfortable sexual experience (80.7%).
Prevalence of potentially traumatic exposure types across Canadian nursing categories.

1Not presented because of insufficient sample size (i.e., n < 10).
2Different lettered superscripts indicate nursing categories that differ from one another at p ≤ .05. Differences in prevalence estimates across categories were tested by changing the reference group in logistic regression models. Differences in mean scores across nursing categories were tested by changing the reference group in linear regression models.
*p ≤ .05; **p ≤ .01; ***p ≤ .001.
On average, participant nurses were exposed to 13.18 (SD = 4.35) out of 20 different types of PPTEs, with statistically significant mean differences in total number of PPTEs across nursing categories (Table 1). Nurse Practitioners (M = 14.60, SD = 4.16) and Registered Nurses (M = 13.30, SD = 4.29) reported the highest mean levels of different exposures; in contrast, Registered Psychiatric Nurses (M = 12.37, SD = 4.65), and Licensed Practical Nurses (M = 12.39, SD = 4.54) reported lower mean levels of different types of exposures. There were several statistically significant differences across nursing categories in terms of experiencing different types of PPTE exposures, indicating potentially important variability across nursing categories. For example, relative to other nursing categories, Nurse Practitioners were more commonly exposed to severe human suffering, sudden accidental death, the death of a child, and the death of an individual after extraordinary efforts were made to save their life. Despite differences between the nursing categories, the exposure prevalence of nurses to most PPTE types is substantial and concerning. Among the PPTEs, combat, captivity, and serious injury, harm, or death to someone else caused by the nurse were less frequently by participants.
The frequencies of exposure for each PPTE type are also provided in Table 1. The most frequently occurring PPTE across nursing participants was severe human suffering (i.e., 57.8% of nurses reported exposure 11 or more times). Other PPTEs that were experienced 11 or more times by participants included life threatening illness or injury (54.2%), physical assault (46.4%), and the death of an individual after extraordinary efforts were made to save their life (40.0%). In contrast, exposure to life threatening natural disaster was the least frequency occurred (i.e., 94.9% of participants reported the exposure occurred fewer than six times).
The total number of different types of PPTEs for different sociodemographic categories are presented in Table 2. There were statistically significant differences among different categories of sociodemographic variables (i.e., gender, age, province, work location, nurse type, years of service, and job setting), except for age groups, in terms of total number of different traumatic exposures. Men (M = 14.10, SD = 4.64) reported statistically significantly more exposure to PPTEs than women (M = 13.13, SD = 4.33). Participants from Western Canada reported experiencing statistically significantly more PPTEs (M = 13.42, SD = 4.27) than participants from Eastern (M = 12.91, SD = 4.63) and Atlantic Canada (M = 12.67, SD = 4.23). In terms of work location, participants working in First Nation/Inuit communities were exposed to more PPTEs events on average (M = 15.80, SD = 3.03) when compared to urban and rural work locations. Among different nurse types, Nurse Practitioners reported more PPTE exposures (M = 14.60, 4.16) than other categories. Participants working in a health centre, urgent care centre, or health clinic reported more frequent exposures to PPTEs (M = 14.08, SD = 4.23) in their job setting than participants in other categories.
Total number of different types of potentially traumatic exposure across Canadian nurses.
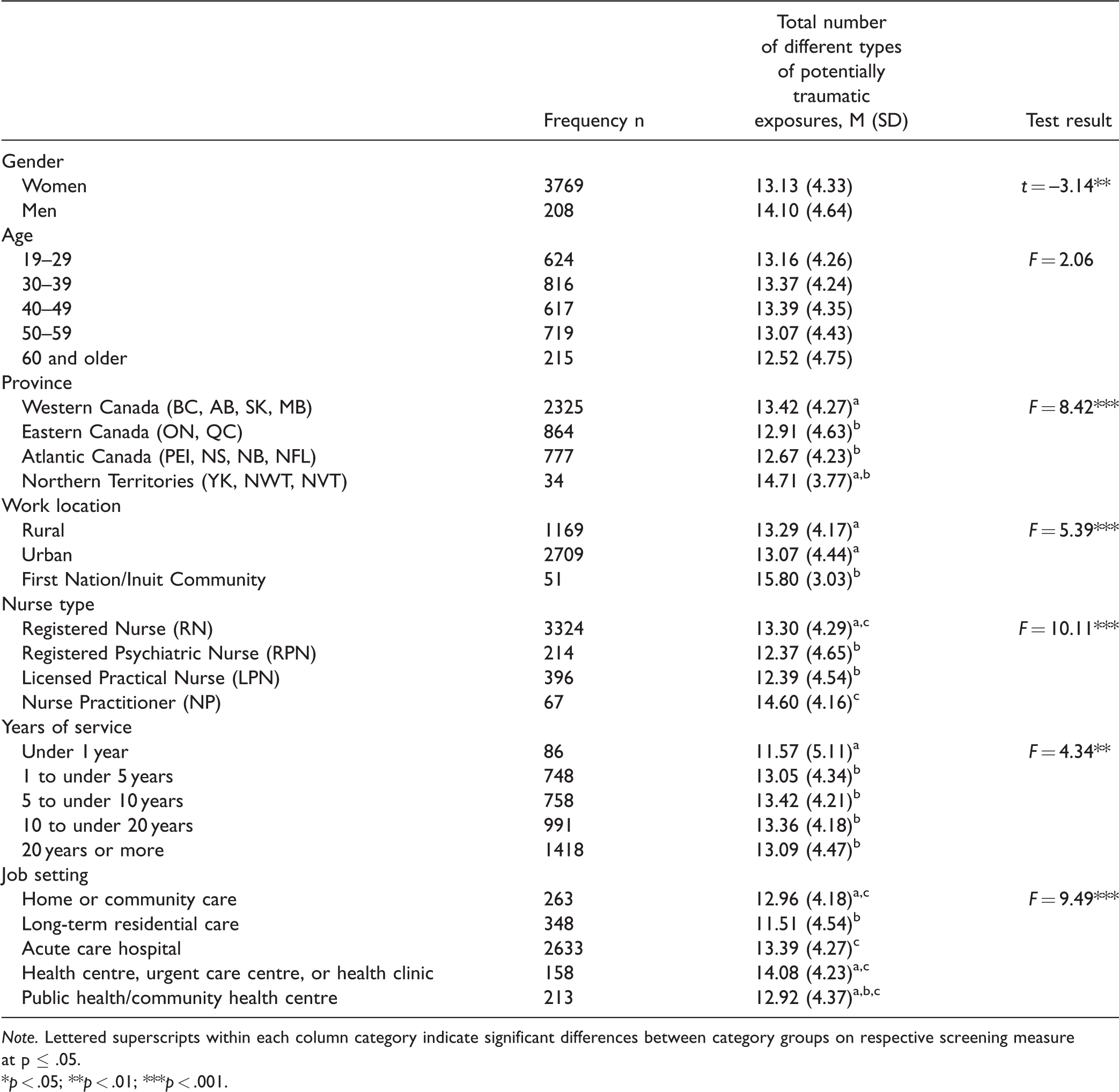
Note. Lettered superscripts within each column category indicate significant differences between category groups on respective screening measure at p ≤ .05.
*p < .05; **p < .01; ***p < .001.
Worst, most distressing PPTEs
The prevalence of each type of PPTE frequently identified as the worst event is provided in Table 3. Across the entire sample, the PPTEs most frequently identified as the worst event were physical assault (12.2%), followed by the death of a child (10.9%), and the death of an individual after extraordinary efforts were made to save their life (10.8%). The worst exposures reported by Registered Nurses were similar to the total sample. Licensed Practical Nurses reported physical assault, sexual assault, and transportation accidents as the worst exposures. Registered Psychiatric Nurses most frequently reported physical assault as the worst event, but identified sudden violent death and sexual assault as the worst events more frequently than other nursing categories; Registered Psychiatric Nurses less commonly reported the death of a child or the death of an individual after extraordinary efforts were made to save their life as the worst event. Worst exposures for the Nurse Practitioner participants could not be reported due to insufficient sample size for each type of PPTE.
Prevalence of worst potentially traumatic exposures across Canadian nursing categories.
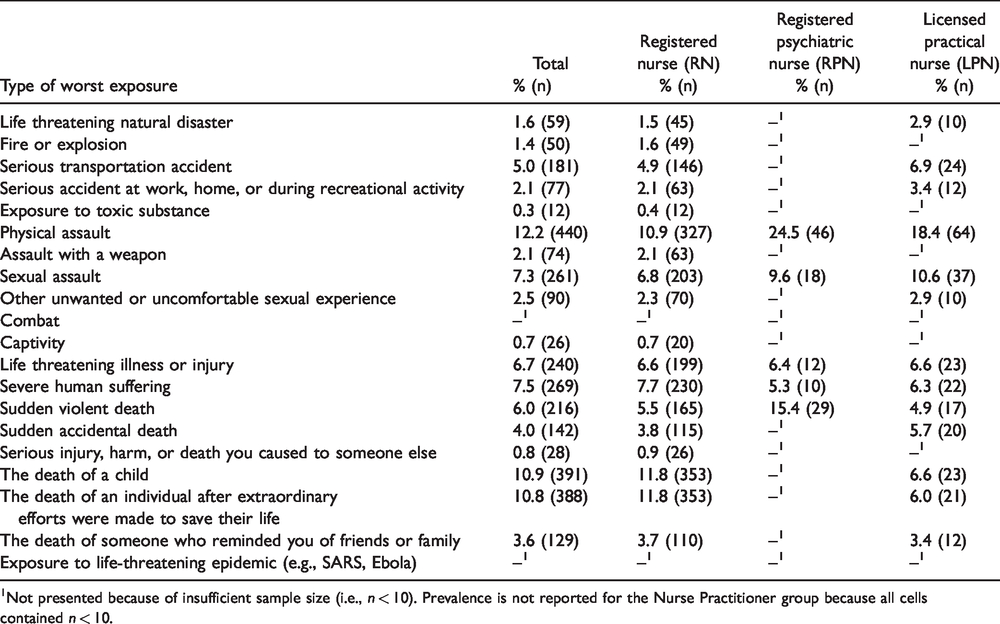
1Not presented because of insufficient sample size (i.e., n < 10). Prevalence is not reported for the Nurse Practitioner group because all cells contained n < 10.
PPTEs and positive screens for mental disorders
The relationships between PPTE and positive screens for mental disorders are presented in Table 4. All models were adjusted for sociodemographic covariates (i.e., gender, age, marital status, work location, years of service) and nurse type to obtain more reliable comparisons. The results indicated a significant association between PPTEs and increased odds of positive screens for several mental disorders. Fairly consistent patterns were found in the relationships between type of PPTE and positive screens of mental disorders except for alcohol use disorder.
Relationship between trauma exposures and positive screens for mental disorders across Canadian nursing categories.
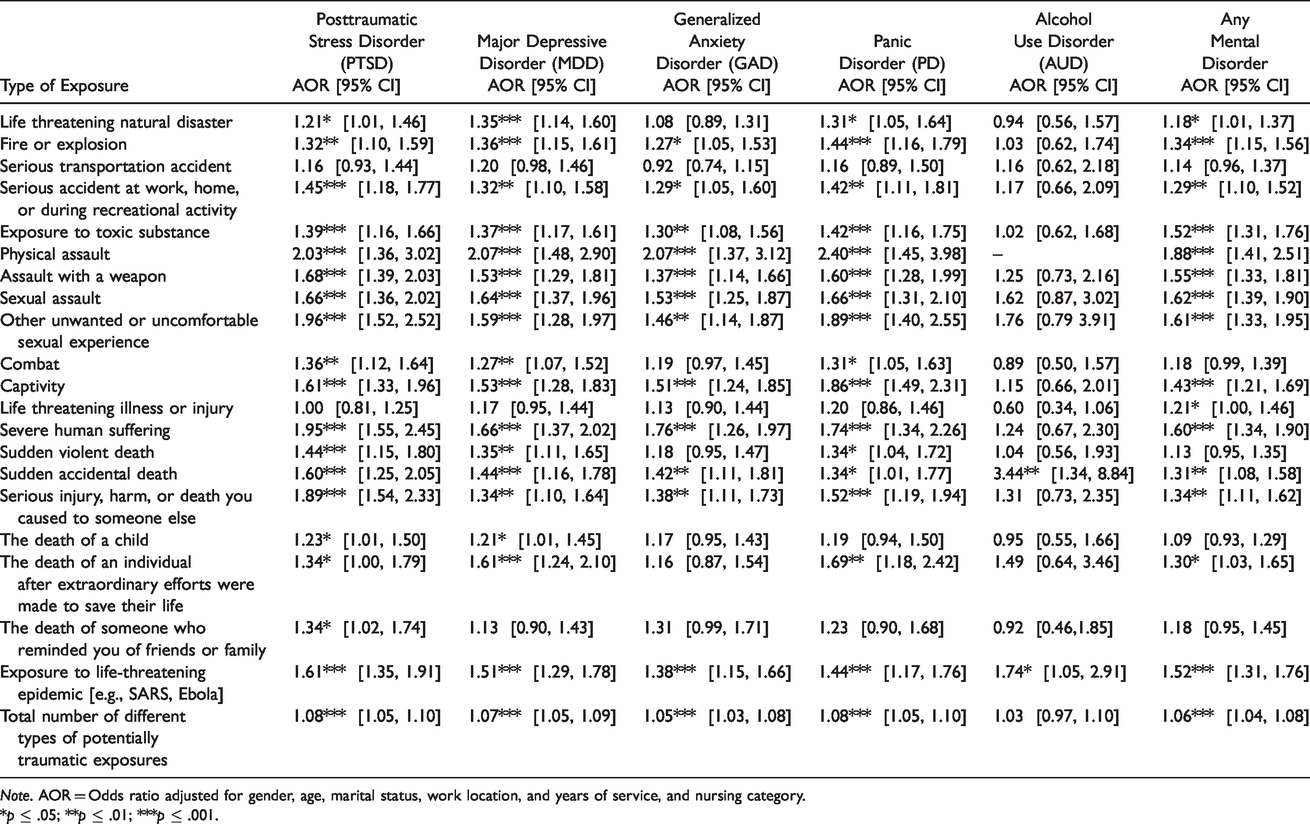
Note. AOR = Odds ratio adjusted for gender, age, marital status, work location, and years of service, and nursing category.
*p ≤ .05; **p ≤ .01; ***p ≤ .001.
Screening positively for PTSD was significantly associated with all PPTE types except for serious transportation accident and life threatening illness or injury (significant Adjusted Odds Ratios [AORs] = 1.21 to 2.03), suggesting participants reporting such PPTE exposures screened positively for PTSD significantly more frequently. Screening positively for MDD was statistically significantly associated with exposure to all PPTE types except for serious transportation accident, life threatening illness or injury, and the death of someone who reminded you of friends or family (significant AORs = 1.21–2.07). Screening positively for GAD was statistically significantly associated with exposure to several of PPTE (significant AORs = 1.27–2.07), except life threatening natural disaster, serious transportation accident, combat, life threatening illness or injury, sudden violent death, death of a child, death of an individual after extraordinary efforts were made to save their life, and the death of someone who reminded you of friends or family. Screening positively for PD was statistically significantly associated with most PPTE (significant AORs = 1.31–2.40), except serious transportation accident, life threatening illness or injury, the death of a child, and the death of someone who reminded you of friends or family. Screening positively for alcohol use disorder was only statistically significantly associated with two PPTE: sudden accidental death (AOR = 3.44) and exposure to life-threatening epidemic (e.g., SARS, Ebola; AOR = 1.74). Relative to other mental disorders, nurses who reported being exposed to different PPTE were not significantly likely to screen positive for alcohol use disorder.
Screening positively for any mental disorders was statistically significantly associated with all PPTE types except for serious transportation accident, combat, sudden violent death, the death of a child, and the death of someone who reminded you of friends or family (significant AORs =1.18 to 1.88). Looking at several dose-response relationships such as odds of positive screening for PTSD (AOR = 1.08, 95% CI [1.05, 1.10], p < .001), MDD (AOR = 1.07, 95% CI [1.05, 1.09], p < .001), GAD (AOR = 1.05, 95% CI [1.03, 1.08], p < .001), PD (AOR = 1.08, 95% CI [1.05, 1.10], p < .001), and any mental disorder (AOR = 1.06, 95% CI [1.04, 1.08], p < .001) indicated that the likelihood of a positive screen for each mental disorder increased as the total number of different PPTE types exposures increased. The results indicated that there was no dose-response relationship such that the odds of a positive screen for AUD did not change statistically significantly as the total number of exposures to different PPTE types increased (AOR = 1.03, 95% CI [0.97, 1.10], p > .05).
Population attributable fractions
The relationships between PAFs for different types of PPTE exposures and positive screenings for mental disorders are presented in Table 5. Some assumptions need to be considered when interpreting a PAF including (a) a causal relationship between an exposure and outcome, which cannot be assessed with cross-sectional data; and (b) population attributable fractions are affected by the prevalence of exposure in the population in such a way that higher prevalence leads to a higher population attributable fraction. The PAF in the current study provides a preliminary estimate of the proportion of an outcome (i.e., a positive screen for a mental disorder) that might be decreased if the exposure (i.e., a specific PPTE) never occurred. Such a result provides the opportunity to make theoretically relative comparisons of relationships between each PPTE type and each type of mental disorder. In the current study, the PAF were only calculated for the significant association between a positive screening for the mental disorder and exposure to the specific type of PPTE (see Table 4).
Population attributable fractions (PAF) for types of trauma exposures on positive screens for mental disorders across Canadian nurses.
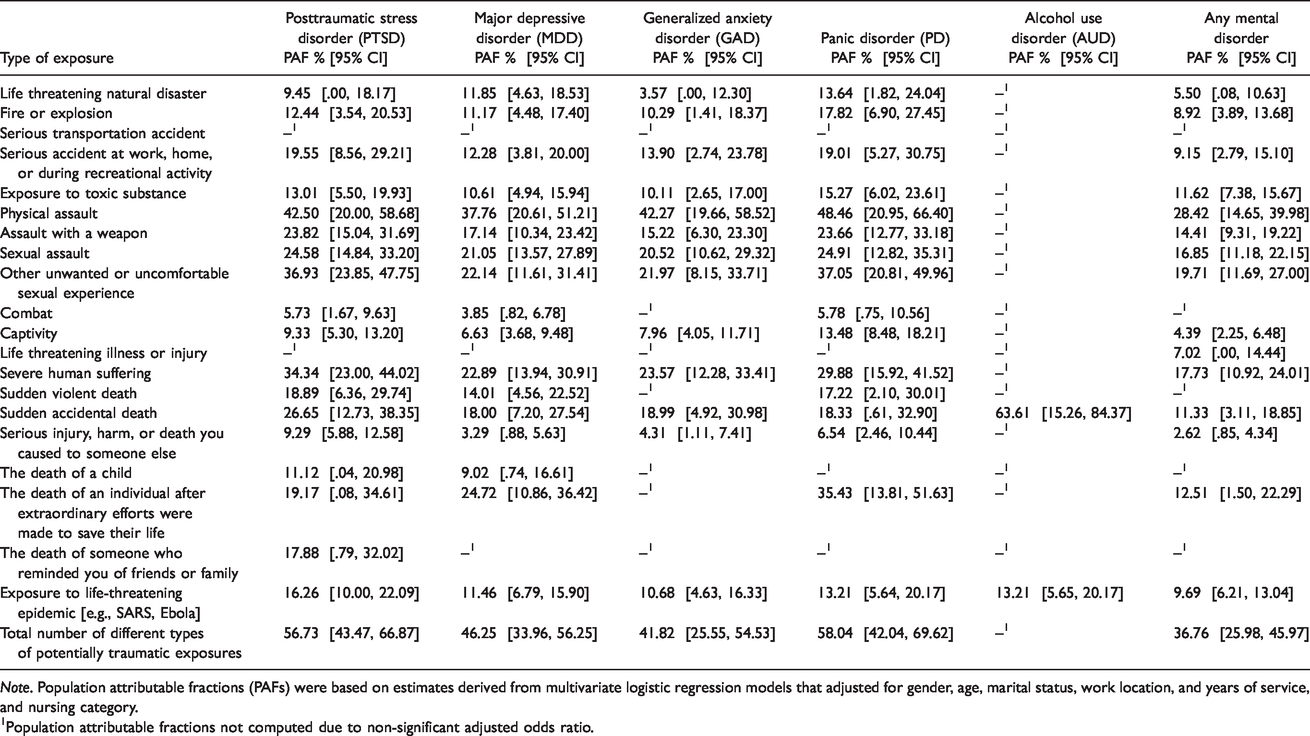
Note. Population attributable fractions (PAFs) were based on estimates derived from multivariate logistic regression models that adjusted for gender, age, marital status, work location, and years of service, and nursing category.
1Population attributable fractions not computed due to non-significant adjusted odds ratio.
The results indicate that eliminating all PPTE exposures in the nursing population might lead to estimated reductions in positive screens for PTSD of 56.7%, MDD of 46.2%, GAD of 41.8%, PD of 58.0%, and any mental disorder of 36.8% (see Table 5). Eliminating several specific PPTEs might have decreased positive screens of mental disorders. For example, eliminating exposure to physical assault might result in estimated reductions in positive screens for PTSD of 42.5%, for MDD of 37.8%, for GAD of 42.3%, and for PD of 48.5%. Similarly, eliminating exposure to other unwanted or uncomfortable sexual experience might reduce positive screens for PTSD of 36.9%, and for PD of 37.1%. If exposures to severe human suffering were eliminated for nurses, we might see reductions in positive screens for PTSD of 34.4%. Eliminating exposure to sudden accidental death might also result in estimated reductions in positive screens for alcohol use disorder of 63.6%.
Discussion
Results from the current study provide a better understanding of exposure patterns for PPTEs among Canadian nurses, identifies the potentially critical exposures, and examines associations between PPTE exposures and positive screens for different mental disorders. Substantial proportions of participants reported exposure to most of the measured PPTEs. Most of the nurses (i.e., 80%) reported being exposed to each of physical assault, the death of an individual after extraordinary efforts were made to save their life, the death of someone who reminded you of friends or family, sudden accidental death, life threatening illness or injury, and other unwanted or uncomfortable sexual experience, with many participants reporting exposure to some PPTEs 11 or more times. On average, participants reported experiencing 13.18 out of 20 different PPTEs. General population sample estimates indicate people are typically exposed to 3.3 unique PPTE (Kilpatrick et al., 2013), suggesting our current sample of nurses experienced PPTE much more frequently; however, direct comparisons cannot be made because of the addition of four nursing-specific events that were rated among the most frequent and the most distressing events. Nonetheless, the results support the notion that nurses are exposed to several different PPTE types more frequently than the general population.
The most frequent PPTE exposures and the PPTE selected as worst were consistent with responses from a sample of Manitoba nurses (Manitoba Nurses Union, 2015). Over half (52%) of the Manitoba sample reported being physically assaulted, 17% reported dealing with an individual who had a weapon, and 76% reported being verbally abused at work (Manitoba Nurses Union, 2015). Experiences of physical assault were reported by nearly half (46.4%) of the current nursing participants 11 or more times, suggesting that physical assault is very frequently experienced among Canadian nurses. Unlike other types of nurses, Nurse Practitioners reported the most frequent exposure to severe human suffering with 78% of Nurse Practitioners reporting exposure 11 or more times. Variation among nursing categories may be related to the nature of the occupation-specific duties (e.g., Registered Psychiatric Nurses working with psychiatric patients), work setting (e.g., acute care hospital or long-term care facility), or perhaps their training and preparation for their employment (e.g., Nurse Practitioners have university and post-graduate education, Registered Nurses have a university degree, Licensed Practical Nurses have a college diploma).
Sociodemographic groups experienced different total numbers of unique PPTE exposures. Statistically significant differences were also identified between nurses from different geographic regions, work locations, types, years of service, and job settings. There were no statistically significant differences between age groups, despite expectations that age would parallel years of service. Age and years of service has previously been identified as a risk factor for GAD and MDD symptoms in nurses, but PTSD may decrease over time (Mealer et al., 2009). Men, although underrepresented in the nursing profession (Brown & Jones, 2004), reported exposure to more PPTEs than women, which is consistent with some prior research indicating men experience more aggression in the nursing workplace than women (Andrews et al., 2012). Participants from Western Canada, participants working in First Nation/Inuit communities, Nurse Practitioners, and participants working in a health centre, urgent care centre, or health clinic all reported a higher total number of PPTE exposures than other groups. Future researchers should focus on better understanding why nurses within these categories reported more exposure to more PPTEs.
The current results also provide information about PPTE perceived as the worst or the most distressing for nurses. The three most distressing PPTE exposures identified by the current sample (i.e., physical assault, the death of a child, and the death of an individual after extraordinary efforts were made to save their life) have previously been identified as three of the top five stressors experienced by nurses (Manitoba Nurses Union, 2015). Given the overlap between frequency of events and level of distress caused by the event, and the consistency across two independent studies, each of the specific PPTE may well warrant providing the nurses who were exposed with appropriate resources to support their immediate and long-term mental health. The effectiveness of critical incident stress debriefing and critical incident stress management programs has been debatable (CIPSRT, 2016); nevertheless, identifying common stressors in the workplace, implementing stress management training programs, has been associated with fewer medication errors and malpractice claims (Jones et al., 1988), increased patient safety and patient satisfaction (Gärtner et al., 2010), and lower burnout and stress in healthcare environments (Duhoux et al., 2017). Mental health training programs have also contributed to fewer mental disorders among PSP (Carleton, Afifi, Turner, et al., 2019).
PTSD has traditionally been the mental disorder given the most attention following PPTE exposures (APA, 2013; Oliphant, 2016). The current results continue to support a link between PPTE exposure and PTSD. Exposure to almost all PPTEs was statistically significantly associated with increased odds ratios of positive screens for PTSD. Many PPTE exposure types were also associated with increased odds of screening positive for MDD, GAD, and PD among nurse participants, which suggests attention is needed for several disorders following PPTE exposures. Relatively few exposures (i.e., sudden accidental death and exposure to life-threatening epidemic [e.g., SARS, Ebola]) were statistically significantly associated with AUD. These findings are particularly noteworthy given the current COVID-19 pandemic and present exposure levels to life-threatening pandemic; suggesting the current crisis will negatively impact the mental health of nurses. In addition, the current results align with previous researchers highlighting the relationship between trauma exposure and mental disorder symptoms with PSP (Carleton, Afifi, Taillieu, et al., 2019). The largest odds ratios for positive screening for all mental disorders measured in the current study, except for AUD, were associated with physical assault. Other PPTEs rated as most distressing were also statistically significantly associated with positive screening for mental disorders. Specifically, the death of a child was statistically significantly associated with positive screening for PTSD and MDD and the death of an individual after extraordinary efforts were made to save their life was statistically significantly related to positive screening for PTSD, MDD, and PD.
Previous rates of mental disorders among nurses showing higher prevalence rates than the general population may be explained, at least in part, by repeated exposures to PPTEs (Janda & Jandová, 2015; Laposa & Alden, 2003; Mealer et al., 2009; Tsaras et al., 2018; Van Ameringen et al., 2008). The current results suggest a seemingly robust dose-response association. As the total number of exposures to different types of PPTEs increased, the odds of positive screening for PTSD, MDD, GAD, and PD also increased. There was no such relationship identified between positive screens for AUD and total number of PPTE exposures. The PAFs indicate that eliminating PPTE for nurses might reduce positive screenings for PTSD, MDD, GAD, and PD by almost half. The results also suggest exposure to physical assault, severe human suffering, and other unwanted or uncomfortable sexual experience may be considered particularly critical incidents, based on the PAFs. The incomplete relationship between positive screenings of mental disorders and PPTEs indicates that there are likely other important variables contributing to nurses’ mental health that warrant additional research attention (e.g., shift work, overtime, relationships with colleagues and supervisors, familial or other stressors outside of the workplace).
Limitations
Several limitations within the current study can provide direction for future studies of Canadian nurses. First, the study used a large, national, and diverse sample of Canadian nurses, but the current sample was not proportionally consistent with the distribution of Canadian nurses. Specifically, the sample included: 1) a larger proportion of Registered Nurses and smaller proportion of Licensed Practical Nurses; 2) larger proportions of nurses from Nova Scotia, Saskatchewan, and Alberta; 3) smaller proportions of nurses from Newfoundland, Ontario, and Quebec; and 4) overrepresentation of nurses practicing in rural areas relative to the general nursing population (Canadian Institute for Health Information, 2019). Second, the study was designed for anonymous, voluntary, self-selected participation. Participants who reported presently experiencing clinically significant stress may have opted not to complete the survey that was advertised as focused on stress in nursing. Further, such nurses may have been on leave or were too symptomatic to complete the lengthy survey. Third, the current data does not report specify how the participant experienced each PPTE (e.g., directly experienced, witnessed, or learned about the event) and what proportion of events were experienced before the participant’s nursing career started. Direct comparisons to reported frequency of PPTEs cannot be made to other populations because of the addition of four nursing-specific events, which also happened to be the PPTE selected by nursing participants as among the most frequently reported and the most distressing events. Finally, only a small number of mental disorders were included and screened for in the current study. Despite the inclusion of well-validated screening tools, additional research should broaden the scope of mental disorders assessed for and use clinical interviews for more reliable diagnosis.
Conclusion
The current results support the growing evidence that PPTE exposures can be significantly related to various mental disorders, including PTSD, MDD, GAD, PD, and AUD. The results are the first empirical evidence to provide better understanding of differences in patterns of PPTE exposure among diverse Canadian nurses. The current study adds to previous work (Carleton, Afifi, Taillieu, et al., 2019) emphasizing that the nature of one’s work increases exposure to PPTE and subsequently impacts the likelihood of screening positive for PTSD, MDD, GAD, and PD. There appears to be disparities between the PPTE perceived by nurses as the worst, most distressing events (i.e., physical assault, the death of a child, and the death of an individual after extraordinary efforts were made to save their life) and the PPTE more significantly associated with positive screens for mental disorders (i.e., physical assault, severe human suffering, and other unwanted or uncomfortable sexual experience); accordingly, the specific PPTE could be broadly considered as warranting additional resources for exposed nurses. Further research should investigate other external and internal factors contributing to the well-being of nurses.
Footnotes
Acknowledgments
The authors would like to acknowledge Carol Reichert and Linda Silas of CFNU for their assistance in the survey design, and the CFNU member unions who assisted with recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. CFNU had no influence on the outcome of the study results.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Andrea M. Stelnicki has received funding to support the current research in the form of postdoctoral funding from CFNU. R. Nicholas Carleton’s research is supported by the Canadian Institutes of Health Research (CIHR) through a New Investigator Award (FRN: 285489).