
Abstract
Background
Post-Traumatic Stress Disorder (PTSD) is a substantial problem for Veterans and active members of armed forces across the globe, resulting in debilitating mental and physical comorbidities. Evidence-based treatments have demonstrated some success; however, many Veterans remain symptomatic mandating the urgent need for innovative treatment strategies.
Purpose
The purpose of this study was to explore the lived experience of military Veterans with PTSD symptoms who participated in a therapeutic warm water immersion intervention aimed at reducing their symptoms.
Methods and Procedures
A standardized warm 33
Results
Five main themes explicated the participants’ experience: the rhythm of relaxed, embracing the properties of the water, the pain floats away, acclimatize to calmness, and a place to set your mind. Participants described a sense of relaxation, calmness, pain reduction, and a means to control intrusive thoughts. All indicated they would recommend the intervention and provided feedback on how to refine it.
Conclusions
As a component of a larger study, these qualitative findings revealed the potential for therapeutic effects of a novel water immersion intervention. The findings serve to inform revisions to the intervention for future research and practice. Immersion provides a fast-acting, non-stigmatizing adjunct therapy for Veterans who continue to experience symptoms during and after standard evidence-based treatment.
Background and purpose
Post-Traumatic Stress Disorder (PTSD) is a trauma and stressor-related mental health disorder that can develop in persons after experiencing or witnessing an actual or perceived traumatic threat. While exposure to the traumatic event can be direct or indirect, symptoms typically include 1) re-experiencing the event, including nightmares or flashbacks, 2) avoiding stimuli reminiscent of the trauma, 3) experiencing negative thoughts or affect and/or feelings of isolation, and 4) feeling hyper-aroused and reactive to stimuli (American Psychiatric Association, 2013). The trajectory of PTSD can change in frequency and intensity and may last a lifetime, often including complex and varied comorbid psychophysiological conditions.
Recent epidemiological studies demonstrate the impact of PTSD on individuals and society globally. The comorbidity of psychiatric conditions is significant as seen in worldwide samples and patterns in European and North American populations (Alonso et al., 2004; Galatzer-Levy et al., 2013; Koenen et al., 2017), with estimates for major depression approximating 48% of PTSD cases, and often associated with suicidal ideation (Cougle et al., 2009; Kessler et al., 2005). Some regional studies, such as one conducted in 7400 adults in England, revealed comorbidity reaching 78.5% (Qassem et al., 2021). Similarly, symptoms of anxiety disorders, alcohol dependance, and increased aggression and impulsivity co-exist and increase the burden of illness for PTSD patients and families, leading to poor quality of life and negative outcomes (Felson & Staff, 2010; Kessler et al., 2005; Modesto-Lowe et al., 2006; Pietrzak et al., 2011; Price & van Stolk-Cooke, 2015; Tull et al., 2007).
Compared to victims experiencing other types of trauma, military Veterans are at particularly high risk for developing PTSD (Brewin et al., 2000; Crum-Cianflone et al., 2014; U.S. Department of Veterans Affairs, 2023) revealing a substantial problem for Veterans and active members of armed forces across the globe including the United States (U.S.), Canada, the United Kingdom (U.K.), and Nigeria (Brunet et al., 2015; Nwoye & Nwek, 2024; Rona et al., 2009). While differences in prevalence exist based on sampling and measurement strategies, a recent meta-analysis of 32 articles focused on military persons from the U.S., U.K. Australia, the Netherlands, and Israel reports ranges of PTSD between 1.09–34.84% (Xue et al., 2015). In North America, both Canada and the U.S. report higher prevalence of mental health disorders, and PTSD in particular, among active and Veteran military compared to the general population. The Canadian Armed Forces Members and Veterans Mental Health Follow-up Survey (2019) revealed increases of PTSD over time, with 16.4% of surveyed Regular Force Veterans released between 1998 and 2015 reporting a diagnosis of PTSD and 44% experiencing anxiety or depressive symptoms (Statistics Canada, 2019; Van Til et al., 2017). In addition, the prevalence of diagnosed mental health disorders among Canadian active and Veteran military is significantly higher (44%) compared to the general population (10%) as reported by a national survey (Pearson et al., 2013). Similarly, seven percent of U.S. Veterans have a lifetime risk of developing PTSD with higher rates among those who served in Iraq (29%), the Persian Gulf War (21%), and Vietnam (10%) (U.S. Department of Veterans Affairs, 2023). For active and Veteran military, the occurrence of PTSD increases with the number and length of deployments and combat exposure (Brewin et al., 2000; Crum-Cianflone et al., 2014; U.S. Department of Veterans Affairs, 2023; Xue et al., 2015).
Similar to other populations of PTSD sufferers, military Veterans experience co-occurring psychological and physical conditions including comorbid depression (Rytwinski et al., 2013; Stander et al., 2014), with aggregate data suggesting a post-deployment prevalence rate of 13–18% in the U.S. (Lavelle et al., 2018). In addition, chronic pain is diagnosed in 6% of patients with PTSD (Shipherd et al., 2007) with the most common causes being musculoskeletal and connective tissue conditions (Gironda et al., 2006). For example, in U.K. Veterans, injured in combat with at least moderate pain, rates of PTSD, depression, and anxiety were four times higher when compared to those who experience mild or no pain (Vollert et al., 2024). Re-experiencing traumatic events, a classic symptom of PTSD, is associated with current pain (p = .008), and higher levels of pain severity (Powell et al., 2015). In one study, current and overall pain and pain disability were positively associated with the severity of re-experiencing symptoms, and with subjective reporting of depression, pessimism, and a lack of energy and motivation by 90% of these Veterans (Beckham et al., 1997).
Although there is ongoing debate regarding the most effective strategies for managing PTSD, evidence-based treatments have shown success. However, these strategies tend to be less effective in individuals exposed to combat, due to various complicating factors (Easterbrook et al., 2022). First, treatment dropout rates among Veteran and active military persons are higher than among the general populations and estimates of one out of four Veterans do not complete residential treatment (Smith et al., 2019). In addition, others do not seek treatment due to access and structural barriers, perceived experiences of stigma, and misconceptions regarding treatment (Smith et al., 2019; Sudom et al., 2012). U.S. military personnel returning from Iraq and Afghanistan reported fear of stigmatization as a major barrier to care even when experiencing significant symptoms of PTSD, Major Depressive Disorder (MDD) or Generalized Anxiety Disorder (GAD) (Hoge et al., 2004). Further complicating the situation, with PTSD and co-morbid depression, a delay in treatment, increases the burden of illness substantially (Brady et al., 2000; Campbell et al., 2007). The standard of care for uncomplicated mild to moderate MDD, is evidence-based psychotherapy or pharmacotherapy as recommended by the U.S. Veterans Administration (VA), while individual trauma focused psychotherapy (TFP) is the standard treatment for PTSD. There is also evidence indicating that eye movement desensitization and reprocessing (EMDR), a form of TFP, can effectively reduce the symptoms of PTSD (Every-Palmer et al., 2019; Wright et al., 2024). Pharmacotherapy is recommended when Veterans are unable or reluctant to engage in individualized therapy. Unfortunately, two-thirds (60–70%) of patients receiving cognitive processing therapy (CPT) or prolonged exposure therapy continue to have a diagnosis of PTSD after treatment. These troubling findings mandate an “urgent need for innovative treatment strategies” (Steenkamp et al., 2015, p. 498) that are easily accessible, non-stigmatizing, and result in successful outcomes.
Water immersion therapy
One treatment approach that may have positive therapeutic effects on PTSD and comorbid symptoms is water immersion therapy. An emerging body of evidence demonstrates the application of water immersion and other hydrotherapies have been used for mental relaxation, fatigue, quality of life, depression/stress (Han et al., 2014; Mizuno et al., 2010; Sa & Palmeira, 2015), relief of symptoms for musculoskeletal and neurological conditions and rehabilitation of acute sports injuries, (Bartels et al., 2016; Bidonde et al., 2014; Mehrholz et al., 2011; Verhagen et al., 2015), and childbirth related clinical practice (Benfield, 2002; Benfield, Heitkemper et al., 2018; Benfield, Hortobágyi et al., 2010).
The mind and body effects of immersion are fast acting and occur within 15–30 min (Benfield, Herman et al., 2001; Benfield, Hortobágyi et al., 2010; Johansen et al., 1997). Seminal studies reveal, the primary physiologic effect is a central blood volume increase and rapid suppression of vasopressin (AVP), (Epstein et al., 1981; Hammerum et al., 1998). The suppression of AVP is particularly salient because in male Veterans with PTSD, plasma AVP level is significantly elevated (2.72 + 1.22 pg/mL) when compared to trauma controls (1.73 + .78 pg/mL; p < .001). In addition, elevated plasma AVP levels are significantly correlated with avoidance symptoms (cluster C; r = .74; p = .001) on the Clinician Administered PTSD Scale, supporting a role for anxiety in PTSD pathology (de Kloet et al., 2008) and amplifying the effects of aggression and anxiety, particularly in intense situations (Carter, 2017). Also, plasma AVP levels are significantly elevated in suicide attempts by depressed individuals (Inder et al., 1997). A positive central plasma volume shift occurs as hydrostatic pressure pushes extracellular fluid into the intravascular space (Johansen et al., 1998). This effect is largely caused by blood from the abdomen, with blood dilution caused by fluid from the legs (Johansen et al., 1997). With increased water depth, venous return to the heart, as well as stroke volume and cardiac output are increased with an associated reduction in heart rate due to the stretching of baroreceptors in the aortic arch and the carotid sinuses (Farhi & Linnarsson, 1977; Risch, Koubenec, Beckmann et al., 1978; Risch, Koubenec, Gauer et al., 1978; Sheldahl et al., 1987).
We postulated that the vasopressin lowering effect of immersion might have a positive therapeutic effect on PTSD and comorbid symptoms. Additionally, previous studies revealing positive effects on mental relaxation, anxiety, and pain for various conditions suggest immersion benefits may be transferable to other populations. Temperature, water depth and immersion duration vary across studies. To our knowledge, the effects of warm water immersion have not been previously examined in military Veterans with PTSD.
Study purpose
The purpose of this study was to explore the lived experience of military Veterans with PTSD symptoms who participated in a therapeutic warm water immersion intervention aimed at reducing their symptoms. The current study is part of a larger feasibility pilot study that examines the psychophysiological effects of water immersion on military Veterans who experience symptoms of PTSD and potential comorbid depression, anxiety, and or pain. The long-term aim of the pilot study was to confirm interpretation and inform future intervention study designs for this population.
Methods and procedures
Study design
This study used a qualitative descriptive design informed by phenomenology to explore military Veterans’ contextualized lived experience of participating in a warm water immersion intervention. Qualitative descriptive design is useful when the study focus is primarily a clear description of a specific phenomenon from those experiencing it (Bradshaw et al., 2017; Sandelowski, 2010) and focuses on descriptions founded on data instead of theorical interpretation (Doyle et al., 2020; Kim et al., 2017). It's often used as a precursor to larger studies and commonly as the qualitative component of mixed-methods studies (Doyle et al., 2020), The foundation for this study is grounded in the overarching principles of naturalistic inquiry (Lincoln & Guba, 1985) informed by a phenomenological worldview with its focus on experience as it is subjectively lived and how people experience the world through their senses (Laverty, 2003 Smith, 2018; Van Manen, 1997).
Setting and sample
Our convenience sample consisted of military Veterans who have returned to university after active military service. Recruitment was conducted at a large public U.S. university ranked as a Top 15% “Veteran-Friendly” school. Inclusion criteria for study participation were previous or current military service, current enrollment as a university student, age 18–55 years, exposure to a traumatic event(s), and currently experiencing at least one or more of these symptoms: nightmares, flashbacks, avoiding situations that reminded them of that trauma, negative thoughts or mood, feelings of isolation or overreacting to situations, pain and or anxiety; and the ability to enter and exit the therapy pool without assistance. Student Veterans were excluded who self-reported current cardiac, pulmonary or kidney disease; uncontrolled diabetes; HIV; hepatitis; mental illness (except depression and anxiety); traumatic brain injury; morbid obesity; open wounds; fear of water; missing lower extremities; and presumptive or confirmed pregnancy. All consented participants completed the study. Data was collected from November 2022 through December 2023. Less than two weeks elapsed between signing the consent and completing the intervention and interview.
Protection of human subjects
The University of Nevada, Las Vegas Institutional Review Board approved this minimal risk study (#UNLV-20022096). The protocol was registered with ClinicalTrials.gov ID: NCT0530903. An email message, containing study information and researcher contact was sent to all student Veterans registered in the university's military and Veteran services center. Eligible participants were invited to an orientation to review study procedures, obtain informed consent, collect demographic information, and schedule the immersion intervention. In addition, a clinical psychologist or a board-certified psychiatric/mental health nurse practitioner administered three questionnaires to assess history of trauma, PTSD symptoms, depressive symptoms, and type of combat exposure. Mental health practitioners were specifically included in the research team and procedures were developed to be initiated if any participants experienced escalating symptoms. All participants were provided with a list of 24/7 emergency resources, URLs and phone numbers to contact for any escalation of PTSD or depressive symptoms. Data collection was completed with no participants experiencing distress or strong emotions. All data were de-identified using alphanumeric codes and maintained on a password protected drive.
Data collection procedures
Study participants were provided an individual date and time to take part in the immersion intervention and data collection, which was conducted at a recreational facility with a therapy pool approximately 30 feet away from a large lap pool. Upon arrival, each participant was met by the principal investigator and a registered nurse experienced in psychiatric nursing and qualitative research. Participants first rested for 10 min in a private office, then changed into swim wear and proceeded to the therapy pool for the immersion intervention. The pool remained at a thermoneutral temperature of 33
Participants were immersed to the chest in the pool for a total of 45 min and were asked to remain vertical during the first 10 min of the intervention to maximize hydrostatic pressure. They then assumed a variety of positions including floating with pool noodles under each arm, walking, or resting in the corner of the pool with their back against the wall. Participants were observed from a distance and checked for any negative effects including facial expressions, or signs of distress by the research team at 15- and 45-min of immersion.
Following the water immersion, each participant dressed and returned to a private office where they participated in a face-to-face audio recorded semi-structured interview with a research team-member. The interviews were facilitated by an interview guide developed by research team members with psychiatric expertise in PTSD and qualitative research, which focused on exploring participants’ overall perceptions of the immersion experience and its effect on their general well-being and symptoms. Interviews lasted between 15 and 26 min. A male psychiatric nurse and qualitative researcher in Veteran PTSD and member of the research team, conducted the interviews using a conversational tone, open-ended questions, active listening techniques, and remained sensitive to participant cues to guide the conversation. The interview was initiated using grand tour questions, such as “Tell me about your experience while immersed in the water” and “How did you feel?” Then, we proceeded to more directed questions related to symptoms and specific emotional and psychological responses to the immersion. They were also asked to expand on specific items from the surveys as applicable. At the conclusion, the participant was asked if they had any questions or if there is anything else they would like to add. They were provided with a list of 24/7 emergency resources, URLs and phone numbers to contact for any escalation of PTSD or depressive symptoms. Participants received $100 for completing the study. All interviews were transcribed by a HIPAA-compliant professional transcription service.
Data analysis
The goal of data analysis for this qualitative descriptive study was to report a comprehensive thematic summary for the findings which emerges beyond individual participant experiences through the development of interpreted common themes (Willis et al., 2016), while remaining close to the data (Sandelowski, 2010). An iterative analytic process was informed by Giorgi's (2009) phenomenologic approach that involved first reading and rereading the verbatim transcripts and listening to the audio recordings to gain a sense of the whole. Two researchers reviewed the transcripts and audio recordings to also determine accuracy. Next, the interviews were coded based on “meaning units” derived from the individual statements, remaining close to the data provided by the participants. The meaning units were then reviewed repeatedly and compared so that the researchers replaced overlapping meaning units by transforming them into the most suitable words to reflect an overall meaning. Common meaning units were then categorized into themes that represented patterns across interviews, at times using the language expressed by participants. This process was completed by manually tracing, identifying, and coding provisional themes and patterns. The draft thematic analysis was shared between all authors who evaluated and discussed variations in the thematic findings and process. A final consensus of synthesized essential themes was refined with associated exemplar quotes to reflect the student Veterans’ lived experience and perception of the water immersion intervention. Study rigor was maintained through several strategies. The researchers remained open to the uniqueness of individual participant experiences while minimizing bias or prejudice during the interview and analysis by practicing reflexivity with the goal of acknowledging possible biases and avoiding interpretation of data based on preconceived notions. Additionally, we iteratively reviewed and refined themes and patterns with the team members throughout the coding process, including the perspectives of clinical and mental health professionals experienced with Veterans and military members, and conducted member checking with two study participants to review the proposed findings and consider any further refinements.
Results
Sample demographics and characteristics
A purposive sample of 13 U.S. military Veterans representing the Air Force, Army, Marines and Navy participated in the study. Nine participants identified as male and four identified as female. The mean age was 31 years (range 23–45) and included White-non Hispanic (9) and Hispanic (4), married (7) and single/divorced (5) Veteran students. Ten of the 13 participants had been deployed and had combat exposure. The number of deployments ranged from one to five and 70% of the participants had been deployed between 1–3 years. Seven of the participants were accessing mental health care services and nine were taking psychiatric medications at the time of the study. Additionally, 12 participants scored above the diagnostic threshold of the PTSD Checklist for DSM-5 (PCL-5) for PTSD diagnosis (Weathers et al., 2013), and 12 had moderate or greater depression based on the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001).
Qualitative interview results
The study findings focused on the participants’ overall lived experience, thought processes and emotional responses during the intervention, perceived changes before and after the intervention including general well-being and symptoms (anxiety and pain), related past experiences, and intent to use similar interventions in the future. The full horizon of their experience was articulated as they talked about their past trauma, anticipated the future, and how they converged in the current water immersion experience. The participants’ focal language provided the foundation for the findings that described their perceptions and revealed five main themes: the rhythm of relaxed, embracing the properties of the water, the pain floats away, acclimatize to calmness, and a place to set your mind. A synopsis of the study findings is located in Table 1.
Thematic findings and exemplar quotes.
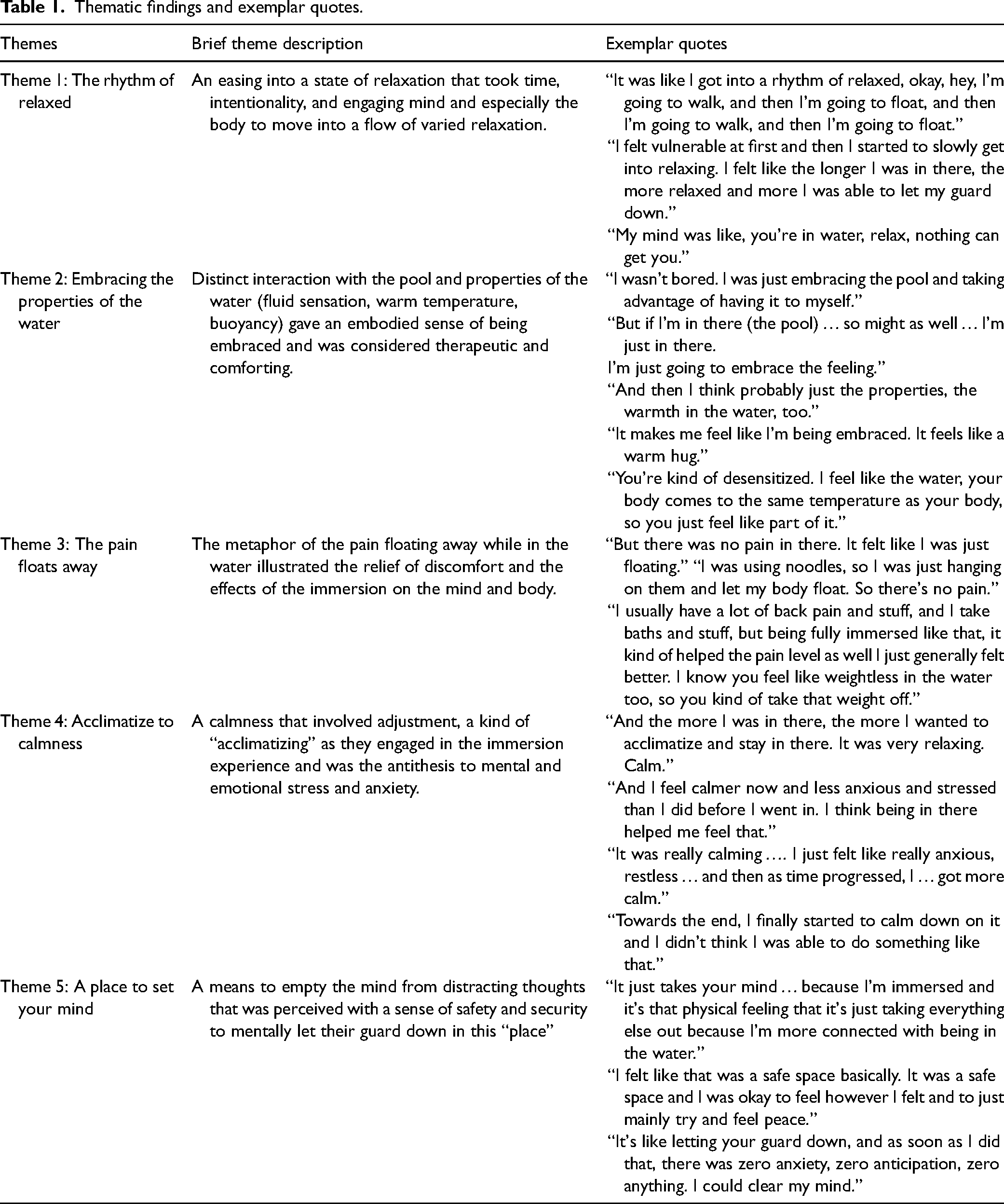
Theme 1: The rhythm of relaxed
Participants universally described an experience of relaxation when in the pool. There was an easing into a state of relaxation that took time and intentionality on the part of the participants. They described how they engaged their minds and their bodies to move into a relaxed state associated with being in the water and experienced a kind of “rhythm of relaxed.” There was also variation in this experience among the participants. Some indicated the rhythm continued even after getting out of the pool as they were still relaxed, while others experienced the anticipation of no longer being relaxed once the experience was over.
Participant 2 described their intentional focus and how the immersion experience involved engagement of their mind and bodies to move into the relaxed state: I was just rotating to see … But it was fine. It honestly actually kept me thinking, as I was walking, kind of pacing back and forth and kind of floating. I would close my eyes and pace when it was in front of me. And then when it was behind me, I kind of let my legs up a little bit more and float. So, I think the combination of it, too, it was like I got into a
While all participants described the experience in terms of relaxation, each had their own individual starting point and engaged their mind and body to get into the rhythm. At the beginning of the immersion experience, participants described a sense of anxiety and vulnerability associated with PTSD and eventually engaged themselves to find a relaxed state: Getting into the pool, I was a little anxious, just the normal being in a new area. I haven't been in here and I haven't spoken with you, so I get really anxious with new stuff like that right now. So, I was able to warm up a little bit, but once I got into the pool, I just completely, just relaxed from that. So, I just feel better overall, in general.” (P9) I felt vulnerable at first and then I started to slowly get into relaxing. I felt like the longer I was in there, the more relaxed and the more I was able to let my guard down.” (P3) So, I think that's how the water helped a lot because I don't know, in my mind, my mind was like, “You're in water, relax, nothing can get you. You can see everything. There's safety around you and you're safe. You're not going to drown. You're okay, you can finally relax.” I was like, okay. (P11)
Theme 2: Embracing the properties of the water
The participants’ immersion experience included a distinct interaction with the water that they described as embracing, like a warm blanket. The properties of the water – the fluidity that allowed a floating sensation, the warm temperature, and the sensation of weightlessness of their bodies were considered therapeutic and comforting. The general comforting sensation they experienced from the water was uniquely distinct, and they described how it was different from other types of comfort (such as sitting on a couch or lying in bed). The interaction with the water exemplified their embodied experience. They embraced the properties of the water and the pool: I wasn't bored. I was just embracing the pool and taking advantage of having it to myself. (P1) And I didn't feel like there was something else I could be doing. At the same time, like I was wasting my time. It felt like I was doing something, but the thing I was doing felt good to do and felt relaxing, if that makes sense. So, the difference between if I was just sitting here trying to relax here, I feel like I could be doing other things. But if I'm in there (the pool) I can't, so might as well … I'm just in there. I'm just going to embrace the feeling. (P5)
Participants also expressed the distinct nature of the water that provided a unique kind of comfort: It just felt like a warm blanket. There was a part there where I was just standing and just kind of enjoying the warmth, and then there was a part where I was kind of floating and enjoying the warmth and just the free float. I would say the warm water is a little more therapeutic than just relaxing on the couch, because I mean, water is almost like, it is going to sound weird but, it forms to your body, unlike a couch, it's like, yeah it's kind of, you're laying on a couch, but if the couch is uncomfortable, you're not going to be fully comfortable. (P4) And then I think probably just the properties, the warmth in the water, too. P2 It makes me feel like I'm being embraced. It feels like a warm hug. So being in there, it reminded me of that. And it's peaceful those moments alone. (P11) Because if I'm in bed, I don't really get that same, even though you're relaxed in bed too, you don't really get that same feeling. I think feeling, being in water, it's like, I don't know. It was very cozy. It was like being, I don't know. I don't know how to explain it. It just felt very, very light. (P11)
They also interacted with the water and described their embodied experience: The warmth of the pool just helped me forget everything going on in life, just being in the water, I don't know, I kind of felt one with the water, I guess, just kind of floating and just letting everything out. So, it was nice. (P9) Because I was in the water and my ears were in the water, so I was listening kind of like to the pool, if it makes sense. Again, it was some kind of mini-meditation for me in this case. If you have symptoms like depression, or anxiety, it brings you to, I don't want to say the different word, but it's bringing you to your better side where you start to feel better after being there in a while. And personally, for me, water always has beneficial effect, even whenever I feel super depressed or anything, I need to go to see water. For me, it's super helpful and always been, I would say. I think I'm not the only person that feels better near the water, so I think this experience would be very beneficial. (P14) It was very buoyant, so it felt almost as if I didn't feel anything. Kind of very neutral. It was like a weightless feeling. Both, (body or thoughts) actually. I see mostly physically, though, of course, because you're floating, you're not putting any effort into it. You're kind of desensitized. I feel like the water, your body comes to the same temperature, so you just feel like part of it. (P10)
Theme 3: The pain floats away
Relief of pain was part of the immersion experience as participants described the specific effects the floating sensation and the lack of pressure or weight had on their bodies. The metaphor of the pain floating away while in the water illustrated the relief of discomfort and the effects of the immersion on their minds and bodies. Something like this actually was really good for my mind and body. My back feels good, my body feels good, my mind feels good. But there was no pain in there. It felt like I was just floating. (P1) My body was very, very relaxed, especially I was using noodles, so I was just hanging on them and let my body float. So, there's no pain. (P14)
Additionally, the participants were able to compare their usual pain with the relief they experienced with the immersion: In the mornings I usually feel the most pain with my ankle, my back, my shoulders. I usually get flare-ups during that time. So, it was moderate. I'd say out of a 10, probably at a six or seven pain usually. It usually takes about two or three hours in the morning to kind of un-stiffen everything. But I feel like by the time I got done with the water, I feel pretty limber right now and my pain level is definitely not there right now. (P2) And then progressively kind of went towards like, oh, I'm just now noticing my leg doesn't hurt at this moment. So, it's like a euphoric kind of pain release. (P3)
The relief they experienced was directly related to the natural effects of the water: It (pain) more affects me when I'm moving around and being physically active affects me more. So, with that, I wasn't really doing that. And I have, like I said, some back and neck issues that's very mild that I didn't feel when I was in there because there's no pressure or weight on any of it. (P5) I usually have a lot of back pain and stuff, and I take baths and stuff, but being fully immersed like that, it kind of helped the pain level as well. I just generally felt better. I know you feel like weightless in the water too, so you kind of take that weight off. Everything kind of takes off. (P9)
Theme 4: Acclimatize to calmness
The participants experienced a calmness that involved adjustment on their part – a kind of “acclimatizing” as they engaged in the immersion experience. Some entered the water initially feeling stress and anxiousness and it took deliberate focus to “acclimatize to calmness”. While the experience involved the mind and body to be engaged, the theme acclimatize to calmness has a distinct focus different from the physical relaxation of theme 1. The calmness they described was the antithesis to their mental and emotional stress and anxiety. And the more I was in there, the more I wanted to acclimatize and stay in there. It was very relaxing. Calm. (P1) So, I kept shifting my arms back and forth just to keep my shoulders warm. But other than that, by the first 15 min I think I was pretty calm, very chill. And then I think by the last five minutes I was almost falling asleep in the water. (P2)
The participants described an experience of calm that overtook their stress and anxiousness. They talked about a sense of stress and anxiety that preceded that morning and the water immersion that led them to a calming experience. In nearly all cases, the calming experience took time and occurred throughout the immersion. I just felt very anxious last night and I was still feeling kind of anxious this morning and some stress. And I feel calmer now and less anxious and stressed than I did before I went in. I think being in there helped me feel that, but also, I was taking some time to think through some things. And I think that also helped, just the time in there. I definitely feel less anxious, less stressed, calmer now than before I went in. (P5) Towards the end, I finally started to calm down on it and I didn't think I was able to do something like that. I didn't think I was able to calm my mind down at all. P3 So, it took me a minute to kind of calm myself. That's why I was telling myself, “It's okay, you can relax. You don't have to be constantly brain working.” So, it was a little bit of an adjustment at first. That's why I was a little anxious in the beginning, but then I got used to it. I was like, “Oh, this is nice.” (P9) It was really calming. The first 15 min, it felt a little weird. A little restless. I don't know. I just felt like really anxious, restless. I was expecting something to happen, and then as time progressed, I got more calm. (P10)
Theme 5: A place to set your mind
During their time in the water, the participants experienced a “place to set their minds” – as some were able to “empty their minds” of any distracting thoughts. Some participants internalized their experience while others focused on nature as they looked out the windows and found a “safe space” mentally. This part of their immersion experience is particularly relevant as many indicated having unrelenting racing thoughts and intrusive memories as part of their PTSD symptomatology. So whatever kind of thoughts, because in my mind, I always have some kind of thoughts running around the head, and you can zone out and you're in the moment. So definitely helped to push away and block some of the unpleasant thoughts. (P14) Well, the more I paid attention (to outside stimuli), the more it pulled me away from what I was doing, and I wanted to use the water to the best of it, my message. Just thinking about nothing. I was almost meditating, I guess, I want to say after the 15 min, I really stopped thinking about everything. (P10)
The participants experienced a sense of safety and security to mentally let their guard down in this “place”: It's like if somebody left you in a room and said, “Just relax, I'll come in 20 min.” It's like letting your guard down, and as soon as I did that, there was zero anxiety, zero anticipation, zero anything. I could clear my mind. (P1) So, then I think that's how that helped because I wasn't too stressed or worried about anything. And it did help me refrain from thinking about bad things because I don't know, I felt like that was a safe space basically. It was a safe space and I was okay to feel however I felt and to just mainly try and feel peace.” (P11)
They also described various ways they found their “place”. Some allowed their minds to focus on pleasant external experiences while others internally emptied their thoughts. Then really, really try and set your mind in a place that it makes you happy, something that you look forward to a goal, and it's worth trying. (P3) Yeah, it just takes your mind. I don't know if it's just because I'm immersed and it's that physical feeling that it's just taking everything else out because I'm more connected with being in the water than I am with all the outside stuff. (P9) No, just almost empty minded in a way. I didn't really have any thoughts. I was just like watching the birds fly by, and the other side, I seen there was cars driving in distance, just taking into view. (P4) Empty my mind and then come back, check in with myself, see where I'm at, and then kind of repeat that cycle. (P7) Yeah, absolutely. Just not having to stress or think about bad things. It was a nice break for my brain. (P9)
Additional descriptive findings
The interviews also included questions specific to the water immersion process/logistics and if they would recommend this to their peers. All participants indicated they would recommend the immersion intervention to other Veterans. In addition, they provided feedback on the presence and proximity of the lifeguards and other individuals in the larger lap pool during their scheduled time, the length of time of the immersion experience, the water temperature and depth of their immersion, and sounds and noise within the environment. These findings can be used to inform the development of future immersion interventions.
Discussion
This study revealed the subjective perspectives of student military Veterans with PTSD symptoms who participated in a therapeutic warm water immersion intervention aimed at reducing their symptoms. The participants described their experience as a sense of relaxation, calm, pain relief, and mental rest with active engagement with the properties of the water and therapy pool. Consistent with qualitative research methodology, we returned to the literature to consider our thematic findings within the larger context of the scientific evidence. Other research reveals similar findings in various populations with diverse health conditions who participate in forms of hydrotherapy, such as warm water immersion.
Hydrotherapy, or the use of water for therapeutic purposes (An et al., 2019), is considered a naturopathic modality that dates back to ancient cultures (Bahadorfar, 2014) and is also referred to as water therapy, aquatic therapy, pool therapy, and balneotherapy (Geytenbeek, 2002). While the practice was used widely in many countries to maintain health and treat disease, attempts to substantiate scientific evidence have only developed since the mid-1980's (Mooventhan & Nivethitha, 2014). Importantly, little consistency exists across studies regarding the parameters of the immersion intervention, including water temperature and depth, intervention duration, pool size and shape, and the characteristics of the studied population and culture. In addition, the lack of consistency in research designs, instruments, and measured outcomes has presented challenges when comparing the results.
Nonetheless, studies have been conducted and synthesized in systematic reviews that demonstrate the benefits of hydrotherapy in populations with conditions such as Parkinson's, arthritis, stroke, dementia, multiple sclerosis, neuropathy, fibromyalgia, and cancer (Fujimoto et al., 2017; Herold et al., 2016; Mooventhan & Nivethitha, 2014). We found evidence similar to our thematic findings, which supports benefits in other populations that directly relate to PTSD symptoms such as pain reduction, muscle relaxation, mental relaxation, stimulation of sensory systems, increased pain threshold, suppression of sympathetic nervous system activity (Becker, 2004; Campion, 1995; Stan, 2012), reduced muscle tension, stress, anxiety, and pain (Al-Qubaeissy et al., 2012; Brown & Gerbarg, 2005; Cadmus et al., 2010; Konlian, 1999; Munguia-Izquierdo & Legaz-Arrese, 2008; Neville et al., 2013; Roehrs & Karst, 2004; Stroller et al., 2012; Tecic et al., 2012) along with increased comfort (Taşdemir & Efe, 2019).
Similar studies describe the important aspects of warm water immersion and its rapid effects on pain and anxiety relief during human labor at term gestation (Benfield, 2002; Benfield, Herman et al., 2001; Benfield, Hortobágyi et al., 2010). Notably, a qualitative study employing a design and intervention similar to the current study, i.e., a Giorgi-style thematic analysis of audio-taped conversations with New Zealand women who used an approximate water temperature of 35–37
Nonetheless, our study adds to this overall body of literature focused on the therapeutic effects of hydrotherapy in a unique population. The thematic findings of increased relaxation, sensation of calmness, mental rest, and the properties of the water closely align with the current research across varied populations and health conditions and contribute to the consistent findings regarding the use of water therapies.
Despite the growing body of evidence in other health conditions, few studies exist that focus on PTSD and the therapeutic effects of any type of hydrotherapy. A recent scoping review revealed a significant gap in research on the effects of aquatic therapy for persons with PTSD (Herold et al., 2016). After thoroughly reviewing 400 articles and systematic elimination based on specified parameters, 18 articles were reviewed fully and found that none of them directly examined the effects of aquatic therapy on PTSD. Similarly, we identified only one study which explored the effects of warm water therapy on PTSD symptoms in Veterans (Corcoran et al., 2014) and found it closely aligned with our study findings. Themes derived from the 15 participants included relaxation, self-reflection, body awareness, reduction of symptoms (including pain), letting go, and overall general satisfaction with the immersion intervention (Corcoran et al., 2014). Improvements in PTSD symptoms and mood were also found but were not consistent across their survey instruments (Corcoran et al., 2014). Our study supports these thematic findings overall, apart from the theme of self-reflection, which suggests further analysis may be warranted. The paucity of research on immersive water therapy and PTSD demonstrates a need to further develop studies that can provide evidence for best practice and protocol development.
A PTSD diagnosis is associated with significantly poorer quality of life and increased medical conditions and health symptoms (Pacella et al., 2013). In addition to psychotherapeutic interventions, complementary approaches including acupuncture, yoga, neurofeedback, transcranial magnetic stimulation, mindfulness, meditation, art, physical exercise, and pet therapy hold some promise for relief of PTSD symptoms; although there is a dearth of high-quality trials with rigorous control conditions and follow-up (Bisson et al., 2020; Kaplan et al., 2024; Leighton et al., 2024; Niles et al., 2023; Reyes, 2022; van de Kamp et al., 2023). Similarly, the lack of research focused on the effects of warm water immersion as an integrative treatment approach reflects a significant area for future investigation with the potential for quick, self-administered therapy.
Strengths and limitations
The strengths of this study primarily focus on the study design and careful protocol development. First, the interdisciplinary research team included health care providers trained in mental health and familiar with PTSD symptoms and treatments. Second, the current immersion intervention was guided by evidence from past studies conducted by the principal investigator examining the effects of immersion (Benfield, 2002; Benfield, Herman et al., 2001; Benfield, Hortobágyi et al., 2010). We consistently adhered to the parameters of the protocol requiring constant water temperature and ambient air temperature and minimized environmental distractions by having only one Veteran in the therapy pool during the intervention. Third, we followed provisions for qualitative rigor throughout the study and included member checking to ascertain participant feedback on the findings.
Limitations include our inability to completely control the environment and the potential effects of medications. Pharmacologics, including antidepressants, analgesics, and non-steroidal anti-inflammatories, were not controlled because of the difficulty recruiting participants without comorbid depression or pain. Although we arranged for a specific time with the community recreation center which was our intervention site, the therapy pool was located approximately 30 feet away from the large lap pool, and we were unable to control for noise or people using the lap pool. Lifeguards were required by the recreation center and they played music which may have also added distraction into the environment, although we asked that the volume be maintained at a low level. The water temperature was approximately 4 degrees cooler than immersion studies conducted in parturients, and it is unknown if a higher temperature might have increased pain relief in student Veterans. Many of these issues are a reflection of conducting research in a naturalistic setting that involves the participants in the lived world.
The use of a purposive sample limits the generalizability of our findings to all Veterans, although it was consistent with the qualitative research design and does provide a rich description of the participant's perspectives. In addition, the recruitment of Veterans with PTSD who were also students may result in findings that are more relevant for a subset of the overall Veteran population.
Study recommendations
Based on the study findings, several recommendations for future research can be implicated. The participants provided feedback regarding the logistics and details of the immersion intervention; several expressed feeling anxious and vulnerable initially at the start of the immersion, which aligns with a diagnosis of PTSD. Similarly, they indicated feeling a sense of safety was important. Modifications to the implementation that reduce the proximity and presence of others, such as lifeguards or individuals who may be perceived as threatening, along with the provision of a quieter setting, could contribute to creating a more comfortable environment. The timing of the immersion could be adjusted based on the participants’ description of the continuum of the experience – many indicating it took time to acclimate and relax. Increasing the sample size and diversity and expanding beyond student Veterans would provide a depth of understanding that could reflect a broader population of Veterans. Finally, as this paper reports the qualitative segment of a multi-methods study, development of a quantitative study that is informed by the qualitative findings and use of measurements that align with the thematic findings could progress the research on warm water immersion in PTSD.
Conclusions
In conclusion, these qualitative findings reveal the therapeutic effects of this novel warm water immersion intervention and serve to inform future research and practice. The intervention was not simply a passive experience for immersed participants letting the properties of the water calm them down. Rather, they took an active part to acclimatize to a state of calmness, thereby destressing themselves. Immersion is relatively easy to implement within the community and provides a fast-acting, non-stigmatizing adjunct therapy for student Veterans who continue to experience symptoms during and after standard evidence-based treatment. Physical pain acquired from active military service was reduced or relieved with warm water immersion. All participants said they would recommend the intervention to others.
Footnotes
Acknowledgments
We would like to thank the Centennial Hills YMCA, particularly Senior Aquatics Director, Amanda Layton and Director of Development, Jordan Sommaggio for their enthusiastic support of this study and their commitment to Veterans. A special thank you to Ross D. Bryant (U.S. Army Retired) Executive Director, Military & Veteran Services Center for his commitment to and support of our Veterans. With boundless gratitude, we thank the military Veterans who participated in this study for their service to our country, and their sacrifice and commitment to their fellow Veterans. We are deeply touched by them. With much appreciation, we thank SIGMA and the Western Institute of Nursing for the small research grant award which made this study possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by Sigma and the Western Institute of Nursing Small Grants award.
Study approval
This minimal risk study was approved by the University of Nevada, Las Vegas Institutional Review Board (#UNLV-20022096).
Informed consent
Written informed consent was reviewed and obtained.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Trial registration
ClinicalTrials.gov Identifier: NCT0530903.