
Abstract
Background
Mental workload is an important indicator of an individual's interaction with task demands. Care aides in long-term care (LTC) settings frequently report excessive demands imposed on their daily work due to challenging resident behaviours and organizational expectations. Understanding mental workload in these contexts is key to predicting staff strain and guiding support strategies.
Methods
Twenty-eight care aides from six LTC homes in New Brunswick, Canada, participated in a simulated care scenario involving common challenges encountered when completing resident care. Two physiological markers of mental workload, namely heart rate variability (HRV) and pupil dilation, were continuously measured across five experimental stages, each designed to elicit different cognitive and emotional demands. Hierarchical mixed-effects models assessed the impact of demographic variables and experimental stages on mental workload.
Results
Mental workload increased significantly, as indicated by decreased HRV and increased pupil diameter, when the care aide was required navigate impossible requests made by the resident. Contrary to expectations, resistance to care, verbal aggression, direct time pressure, and intervention by a supervisor did not significantly influence physiological correlates of mental workload.
Conclusion
These findings suggest that creative problem-solving, such as responding to impossible resident demands, may be more mentally taxing than expected stressors like aggression or time pressure. To manage mental workload, staff should be prepared and supported to adapt creatively under pressure. Further efforts should be made to understand the relationship between increased mental workload and cumulative stress in care aides.
Background & Purpose
Mental workload is traditionally conceptualized as a balance between the demands of a task and the cognitive resources available to meet those demands (Welford, 1978). More recent definitions describe it as a complex, individualized, and non-linear construct that emerges from the dynamic interplay between task demands and an individual's cognitive capacity at a given time (Jafari et al., 2019; Longo et al., 2022; Young et al., 2015). Mental workload is recognized as being closely linked to attentional processes and mental effort, both of which are essential for rapidly shifting focus, solving problems, and making decisions under pressure (Fikri et al., 2024; Teng et al., 2024). When mental workload becomes excessive, it can lead to cognitive overload, impairing work performance, decision-making, sustained attention, accuracy, and emotional regulation (Young et al., 2015).
In addition to cognitive impacts, high mental workload is associated with both physiological and psychological strain, including tachycardia, musculoskeletal injuries, increased stress, fatigue, and burnout (Charles & Nixon, 2019; Darvishi et al., 2016; Nino et al., 2020; Tao et al., 2019). Identifying tasks and activities that contribute to elevated mental workload is therefore essential for targeting areas in need of intervention, system redesign, or additional support to improve healthcare worker performance and well-being. This importance is reflected in the increasing scholarly interest in the mental workload of healthcare providers due to its significant implications for patient safety, care quality, and workforce sustainability (Poku et al., 2025; Yuan et al., 2023). Among healthcare professionals, nurses are particularly affected, as they routinely operate in cognitively demanding environments that require rapid decision-making, multitasking, and the management of emotionally and physically challenging situations (Gündüz and Öztürk, 2025; Shan et al., 2023). Recent studies highlight the substantial mental workload of nurses working in acute care settings. Gündüz and Öztürk (2025) conducted a descriptive-correlational study with acute care nurses in Turkey, revealing that over 95% of participants report high levels of mental workload, particularly in the emotional and cognitive domains. Their findings also demonstrate a strong association between elevated mental workload and burnout. Specifically, higher cognitive burden was linked to emotional exhaustion and depersonalization, emphasizing the critical need to address cognitive demands to support nurse well-being. Similarly, Moghadam et al. (2021) investigated mental workload among ICU nurses and found high levels of mental workload. Importantly, they identified a significant positive correlation between physical and mental workload, suggesting that physically demanding tasks may exacerbate cognitive strain. Together, these studies underscore the complex interplay between various workload factors in acute care nursing and the importance of comprehensive strategies to manage both physical and cognitive demands to improve nurse performance and reduce burnout risk.
Although mental workload has been studied in acute care settings, its exploration within long-term care (LTC) environments remains limited. A search of the literature located only one study examining mental workload in LTC staff. Ma et al. (2025) conducted a national survey of 1,601 LTC care aides in Japan and found high levels of self-reported mental workload. Given the unique staffing and care challenges in LTC (Boamah et al., 2025; Gopinathbirla & Shankardass, 2024), this single study points to a need to further explore how mental workload manifests in LTC. The majority of LTC care staff are unregulated female care aides with minimal formal qualifications, and their work is often prescribed into routine tasks under efficiency-driven management (Chamberlain et al., 2019; Squires et al., 2015). Their highly prescriptive work environment is thought to be deliberately structured to prioritize routinized care practices that maximize efficiency in work performance (Rodriquez, 2011). However, delivering consistent, high-quality care to LTC residents remains a persistent challenge. Contributing factors include time constraints driven by chronic staffing shortages (Berta et al., 2022), limited autonomy for care aides in decision-making (Banerjee et al., 2015), and the complex needs of residents—particularly those with significant behavioural and psychological symptoms of dementia which can disrupt workflow and slow the pace of care delivery (Jeon et al., 2012). These structural features suggest that LTC environments may impose distinct cognitive demands on staff and at times, place conflicting expectations – requiring staff to uphold both efficiency and individualized care. As a result, staff often face increasingly difficult and stressful working conditions. Such features underscore the urgency for targeted research to better understand and mitigate the mental workload of LTC staff, ensuring both caregiver well-being and quality resident care.
The study of mental workload serves three primary purposes: i. to quantify the transactions between individuals and a range of task demands, and ii. to predict human performance in different situations, specifically the resource depletion and effort required of staff to perform their duties under specific circumstances, and iii. to identify needed modifications to the work environment (Tao et al., 2019; Young et al., 2015). According to Tao et al. (2019) mental workload can be assessed using a variety of methods, including both objective and subjective approaches. Physiological measures provide the benefit of real-time, continuous, objective data, enabling researchers to monitor fluctuating mental workload without interrupting task performance. To reduce the effects of confounding physiological influences (ex. physical activity), two distinct biomarkers were employed in this study; heart rate variability (HRV) and pupil dilation. Both are reliable and non-invasive indicators of autonomic nervous system activity and found to be closely reflect cognitive effort (Ahlstrom & Friedman-Berg, 2006; Charles & Nixon, 2019; De Rivecourt et al., 2008; Taelman et al., 2011). Importantly, biomarker information helps quantify how individuals will respond under different work demands and stressors, allowing for the identification of situations that may lead to cognitive overload. Such data can then be used to support the design and modification of the work environments and processes to better align demands with the human capabilities, ultimately improving performance, safety, and well-being.
The aim of this study was to identify the levels of mental workload associated with a routine resident encounter in a simulated LTC environment by measuring participant HRV and pupil dilation. The simulated scenario was intentionally designed to reflect common challenges faced by staff in their daily work (Morris et al., 2025a)—such as managing responsive resident behaviours that hinder care delivery (e.g., confusion, fixation on unachievable tasks, and resistance to care) (Cloak et al., 2025; Seitz et al., 2010) —along with added pressures like time constraints, understaffing, and supervisory expectations (Chamberlain et al., 2017; Cooper et al., 2016; Costello et al., 2019). The scenario was centered around a bathing activity since bathing is one of the most commonly resisted care activities (Backhouse et al., 2020). We hypothesized that challenging working conditions imposed by residents who delay care, and supervisory and family expectations of care, and inability to follow prescribed practices would result in increased mental workload. In keeping with established and validated measures by others (Tao et al., 2019; Young et al., 2015), HRV and pupil dilation serve as a proxy to mental workload.
Methods & Procedures
Participants and Recruitment
Participants were 28 care aides recruited from six LTC homes in New Brunswick, Canada. Participants were recruited via posters, distributed to local LTC homes and via social media. Participants were offered a 50$ VISA gift card as a token of appreciation for their time. The first simulation was conducted on May 5, 2024 and the last simulation was conducted on August 21, 2024. Upon arrival participants were informed of study protocol, the voluntary nature of their participation, and their ability to withdraw from the study at any time without any repercussions. A member of the research team reviewed the consent form with all potential participants, obtaining written consent prior to initiating the study. This study was reviewed by the institutional ethics review board (REB #2023-064) prior to commencement.
Study Design and Procedure
Simulation was employed as a research methodology to systematically measure care aides’ responses which allowed the study to proceed without disrupting the lives of actual residents or relying on the unpredictability of an actual LTC clinical settings (Morris et al., 2025a). The study was conducted in a simulation laboratory designed to replicate a double-occupancy room in a LTC home, complete with functional bathroom, hospital bed, closet, and personal effects (Figure 1). A trained actor was hired to portray a resident with dementia. Practicing registered nurses (RN) assumed the role of the RN in the simulation, to ensure they were familiar with the role. A meticulously crafted script, developed with input from experts in simulation and gerontological nursing, ensured consistency between participants (Morris et al., 2025a). The actors engaged in several practice scenarios to ensure their behaviour was standardized.

Simulated Care Scenario Including Resident-Actor and Participant Outfitted with FirstBeat Bodyguard 3 Heart Rate Monitor (not Visible) and Pupil Core Googles Connected to Laptop in Backpack.
Participants were given the task to give a resident a bed bath before their family arrived. The simulation included six (S0 – S5) stages, 2 min each in duration (see Supplemental Material 1 for a more detailed description of each stage). Progression through the simulation was triggered by in-room cues—the sound of a cough played from a speaker from the other sleeping area—to standardize the experience and introduce the desired experimental variables reliably. Stage 0 acted as a control, while stages 1–5 each included one obstacle to completing the assigned activity, serving as a potential mental workload trigger. The control stage deliberately included talking and moving around so that it served as a realistic comparison for the activity the care aide would be engaged in during the scenario.
Physiological Parameter Measurements
The simulated resident rooms and adjoining hallways are fitted with hard-wired cameras utilizing SimCapture software (Laerdal Medical, United States). This allowed the audio and video recordings of the simulated care scenarios, which ensured that the timing for each new stage could be confirmed when compared with the physiological data. Mental workload was determined using the relative increase or decrease in the physiological markers throughout the scenario stages.
Heart Rate Variability (HRV)
HRV assesses the differences in time between the R-peaks of the heart beats. Typical root mean square of successive differences in R-peaks (RMSSD) range from 24.2–98.7 ms for healthy adult men and 21.5–87.0 ms for healthy adult women (Keet et al., 2013). In states of high mental workload, lower variability in the time interval between heartbeats (lower HRV) is commonly observed, reflecting reduced parasympathetic nervous system activity and increased cognitive or emotional strain (Laborde et al., 2017; Shaffer et al., 2014; Tao et al., 2019). HRV data were collected using the Firstbeat Bodyguard 3, a two-lead electrocardiograph (ECG) device worn by participants (Firstbeat Technologies Ltd, Jyväskylä, Finland). The device was affixed to the skin using adhesive electrodes, with one lead placed below the right clavicle and the other positioned on the left ribs. Upon detection of an electrical impulse, the device initiates ECG recording, capturing raw voltage signals in millivolts at a sampling rate of 256 Hz with 18-bit digital resolution.
Accelerometry
The FirstBeat Bodyguard 3 device also collected 16-bit, 3-dimmensional accelerometry data. Since HRV is significantly influenced by physical activity (Laborde et al., 2017), accelerometry data served the purpose of quantifying the amount of bodily movement the participant exhibited for use as a covariate in the HRV models.
Pupil Dilation
Pupil diameter normally ranges from 2 mm to 8 mm (Spector, 1990) and consistently increases when mental workload is high (Tao et al., 2019). To gather pupil dilation data, participants wore a Pupil Labs Core goggles during the simulations (Pupil Labs GmbH, Berlin, Germany). The goggles featured two infrared cameras directed at each eye and a wide-angle world-view (front-facing) camera. The eye cameras capture 192 px images sampled at 200 Hz with 0.60° accuracy (after calibration). The associated Pupil Capture software (Kassner et al., 2014) uses the camera images to create 3D models of pupil diameter, accounting for slippage of the goggles (Dierkes et al., 2019). The goggles were fitted to participants by adjusting the length of the camera arms until the camera feed displayed a clear image of the pupil. The cameras were calibrated to the eyeball size by asking participants to hold the eyes on a fixed point on the wall while moving the head in the largest range of motion possible without moving the eyes. The goggles must be connected via cable to a computer running Pupil Capture software during recording, so participants wore a small backpack that enabled them to carry a Dell 13-inch laptop on their back (Figure 1).
Data pre-Processing
Demographic categorical variables were collapsed into fewer categories to facilitate statistical analysis and ensure adequate group sizes for comparison. This was done by combining related categories (e.g college education and university education were combined to make a post-secondary education category, ages were grouped into wider categories)
One-minute samples of HRV, accelerometry and pupil dilation data were extracted from each experimental stage and the baseline period. The one-minute samples were extracted from the middle minute of each stage to avoid any delay in physiological response that might occur in the beginning of the stage (Jainta & Baccino, 2010; Laborde et al., 2017; Taelman et al., 2011), or habituation/resolution to the trigger that might occur near the end of the stage (Charles & Nixon, 2019). The ability to locate the middle minute of each stage was achieved using annotation on the SimCapture video marking the start and end of each experimental stage. After synchronization of the time-stamps, these start and end markers were applied to the HRV, accelerometry, and pupil dilation data as well.
All samples were baseline corrected by subtracting the baseline values from the values obtained in each experimental stage (Laborde et al., 2017; Mathôt et al., 2018). One participant was missing baseline pupil data, so the average baseline pupil diameter from all other participants was used in this single case.
Heart Rate Variability (HRV)
Extracted one-minute samples of ECG data were loaded into PhysioZoo Pulse (Behar et al., 2018) to conduct automatic detection of R-peaks and extraction of R-R intervals. The detected R-peaks were manually validated. The R-R intervals were further filtered using the default moving-average outlier detection in PhysioZoo to remove any ectopic beats that would bias the HRV estimates (Laborde et al., 2017). Root mean square of successive differences (RMSSD) in the R-R intervals was calculated for each one-minute sample. RMSSD has been shown to be a valid measurement even at short time-scales such as this (Shaffer et al., 2020; Tiwari et al., 2020).
Accelerometry
Accelerometry samples consisted of values indicating the position of the participant's body in the x, y and z planes. The sum of the absolute values from each plane were averaged to give an estimate of the amount of motion that occurred during the 1-min period.
Pupil Dilation
Prior to data extraction, settings in Pupil Capture (Kassner et al., 2014) were set to exclude samples where the model of pupil diameter had <60% confidence in order to avoid low quality data and bias from blinks. The average of the 3D estimate of pupil diameter was averaged across all extracted samples to obtain a pupil diameter for each experimental stage.
Statistical Analysis
All statistical analysis was conducted using linear mixed models produced with the lmerTest (Kuznetsova et al., 2017) package in R v4.1.3 (The R Foundation). HRV and pupil dilation data were modelled using hierarchical models. Both models included a random effect of participant ID to account for the within-subjects design and the HRV model included the accelerometry data as a covariate. The demographic variables were entered in step one of the hierarchy and the categorical stage variable with the control stage as the reference group was entered in step two. Chi-squared tests were used to determine differences between the model steps and t-values were used to assess the predictive value of each predictor.
Residuals of fixed and random effects were assessed using the Shapiro-Wilk normality test. The fixed-effect residuals of the HRV models showed deviations from normality but transformations did not provide an improvement, so the model was run with the untransformed data. No evidence of multicollinearity (assessed with VIF < 10), heterogeneity of regression slopes (assessed with non-significant interactions between grouping variable and covariate), or heterogeneity of variance (assessed with Levene's test) was found in any of the models, so assumptions were met. An alpha level of 0.05 was taken to be significant in all cases.
Results
Descriptive
Data was collected from 28 care aides from six LTC homes in New Brunswick, Canada, but due to equipment failure on some participants, usable HRV data was gathered form 24 participants and usable pupil dilation data was gathered from 21 participants. The sample was typical of national care aide populations (Estabrooks et al., 2015) with the majority of participants being female, between 35 and 59 years, with college diplomas (Table 1). The sample had worked in a LTC for an average of 7.3 years with 60.7% working fulltime and the remainder working part-time or casually.
Descriptive Statistics of Demographic, HRV, and Pupil Dilation Data.
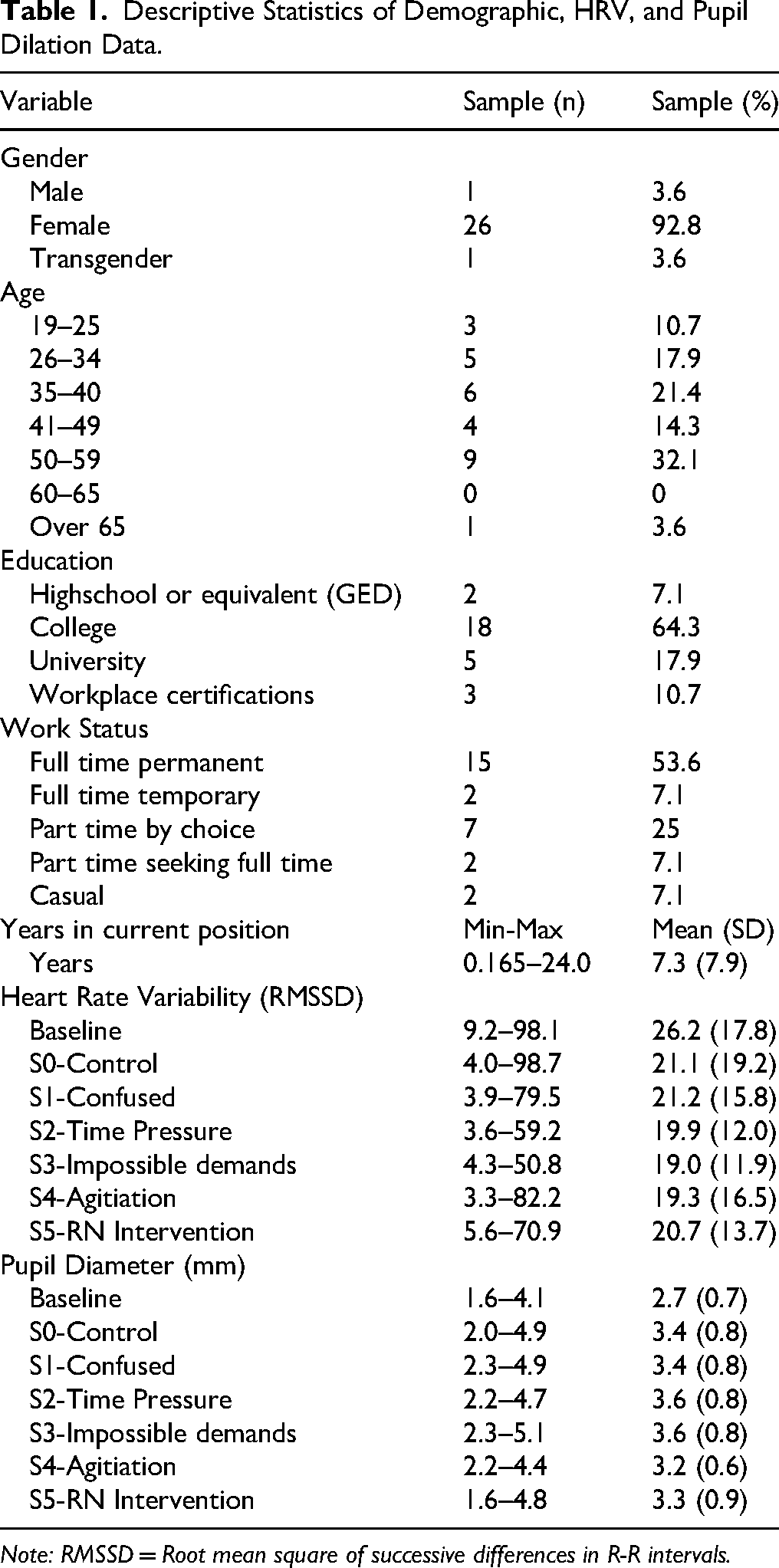
Note: RMSSD = Root mean square of successive differences in R-R intervals.
Physiological Data
Results from the hierarchical mixed-effects model indicate that the demographic variables did not significantly improve model fit for either HRV (χ²(5) = 5.906, p = 0.316) or pupil dilation (χ²(5) = 2.293, p = 0.807). This suggests that individual differences such as age, gender, or experience did not meaningfully influence these physiological markers in the context of this study. However, when the categorical ‘stages’ variable was added to the model, there was a significant improvement in fit for the pupil dilation model (χ²(5) = 27.869, p < 0.001), but not for the HRV model (χ²(5) = 9.258, p = 0.099) (Table 2). These findings indicate that different stages of the care interaction influenced pupillary dilation, confirming that pupil dilation is a sensitive measure of mental workload fluctuations in response to situational factors. In contrast, while the stage variable approached significance in the HRV model, it did not meet the conventional threshold (p < 0.05), implying that HRV may have been less responsive to these stage-based manipulations or that other unaccounted factors contributed to its variability.
Results of Hierarchical Mixed Models for Pupil Dilation Data.
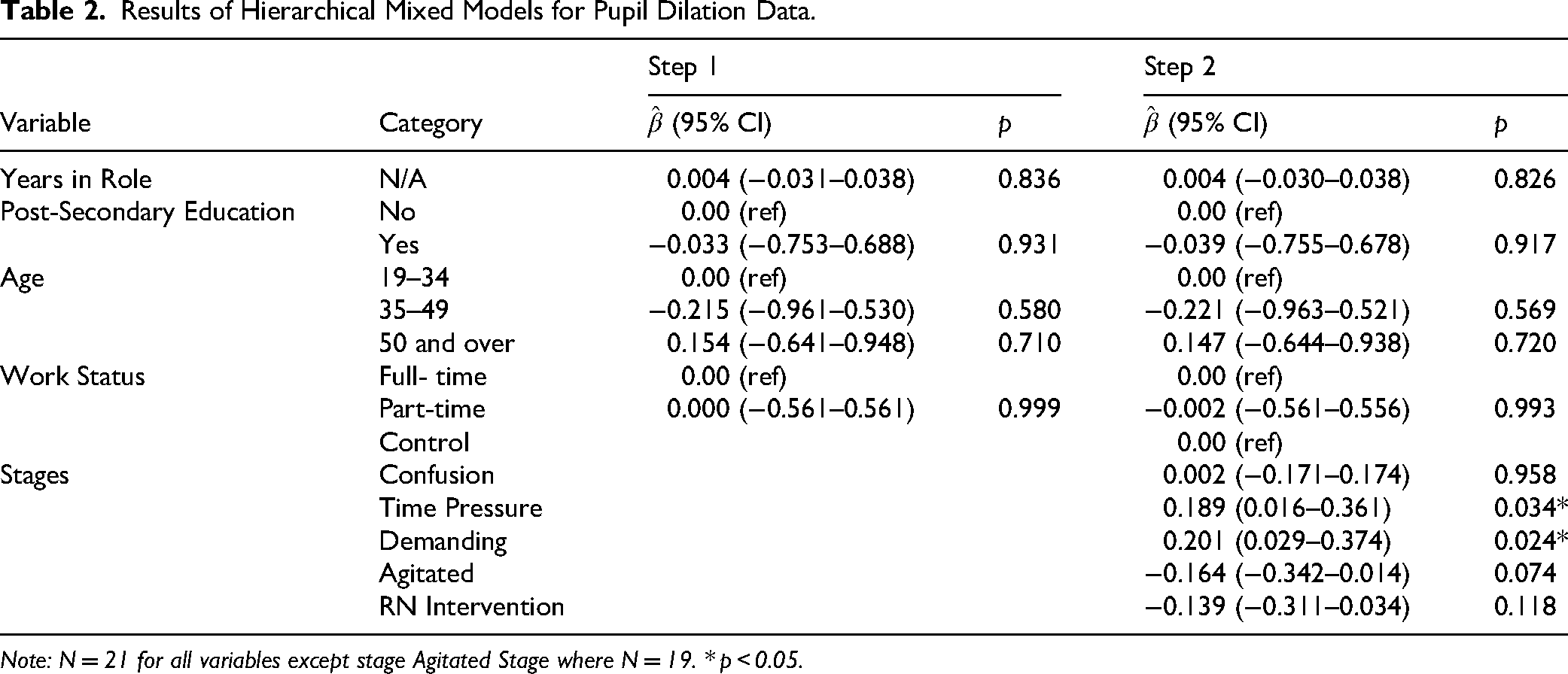
Note: N = 21 for all variables except stage Agitated Stage where N = 19. * p < 0.05.
Based on the contrast tests of each stage compared to the control, both models contained mixed results (Figures 2 and 3). In Stage 1, confusion that slowed the progression of care, there was no change in HRV (t = 0.256, p = 0.798) or pupil dilation (t = 0.018, p = 0.986) relative to the control. The time pressure trigger was introduced in Stage 2, when the RN informed the participant that the resident's family is “ten minutes away.” An increase in pupil dilation was observed (t = 2.150, p = 0.034) associated with the time pressure but no change was observed in HRV (t = −1.160, p = 0.249). Given that this significant difference was reliant on two outlier pupil dilation data points (Figure 3), and was not present in the HRV data, this cannot be concluded to be a change in mental workload relative to the control. Statistically significant results were identified when comparing the data from Stage 3 with the control. In Stage 3 the resident introduced an impossible demand by insisting that she only wanted to wear her black boots, which were not available in her closet. In the HRV model, RMSSD in Stage 3 was significantly lower than the control by an average of −3.71 ± 1.62 ms (18%) (t = −2.285, p = 0.024). In the pupil dilation model, pupil diameter increased in Stage 3 by 0.201 ± 0.088 mm (6%) (t = 2.288, p = 0.024), a significant difference compared to the control stage. In Stage 4 the resident became verbally and physically agitated, swinging a cane and screaming while the care aide attempted to wash her. Stage 4 elicited no significant change in the physiological variables (HRV: t = −1.146, p = 0.122; pupil dilation: t = −1.806, p = 0.074), but there was a near-significant decrease in pupil dilation in this stage compared to the control. The workplace hierarchy trigger was presented in Stage 5 when the RN intervened to take over the resident's care. No change in mental workload was observed in Stage 5 (HRV: t = −1.146, p = 0.254; pupil dilation: t = −1.578, p = 0.118). Note, however, that the most variability was observed in this stage.
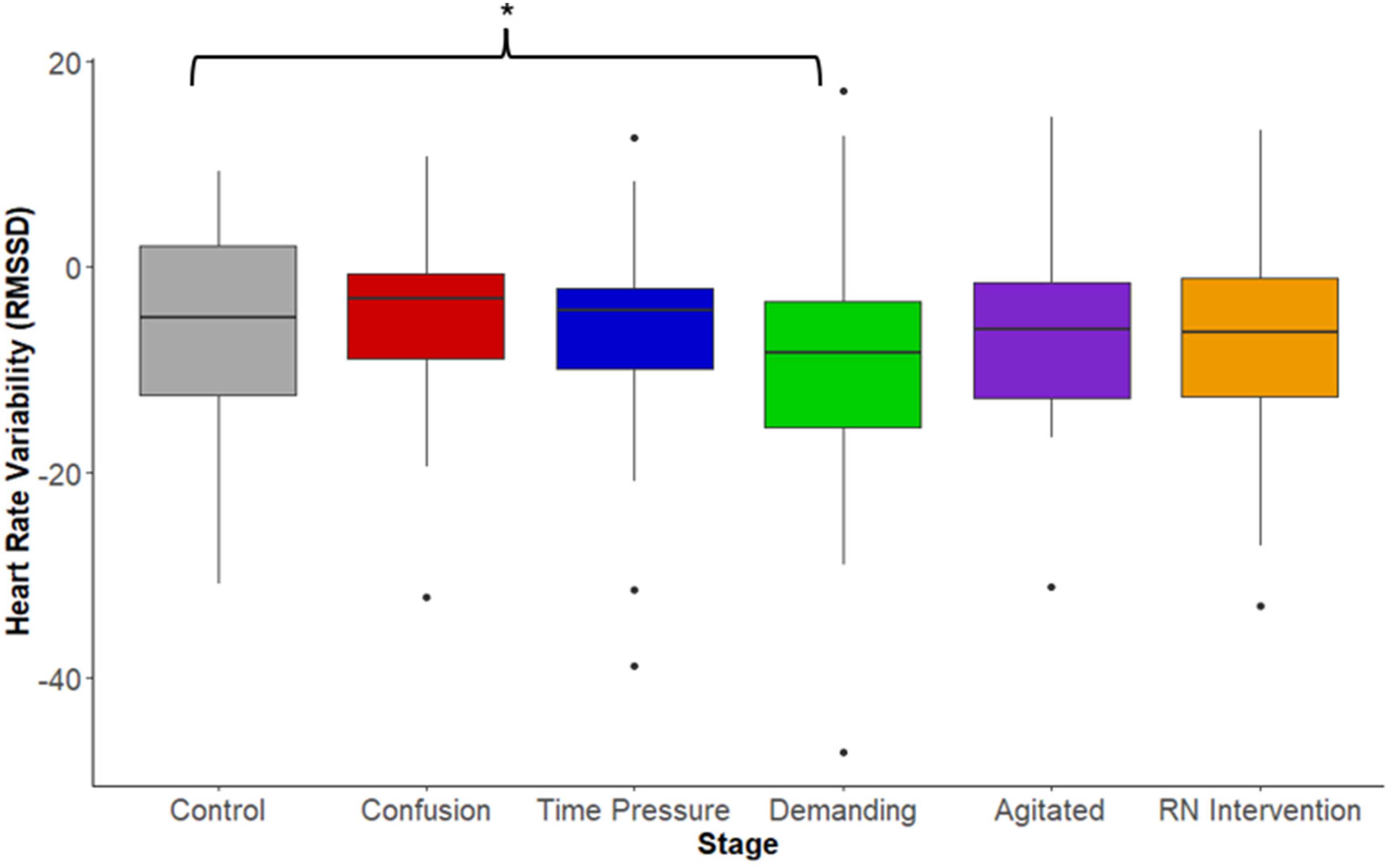
Baseline-Corrected Heart Rate Variability (RMSSD) by Experimental Stage. Note: Brackets indicate significant differences between stages. * p < 0.05. RMSSD = Root Mean Square of Successive Differences in R-R Intervals.
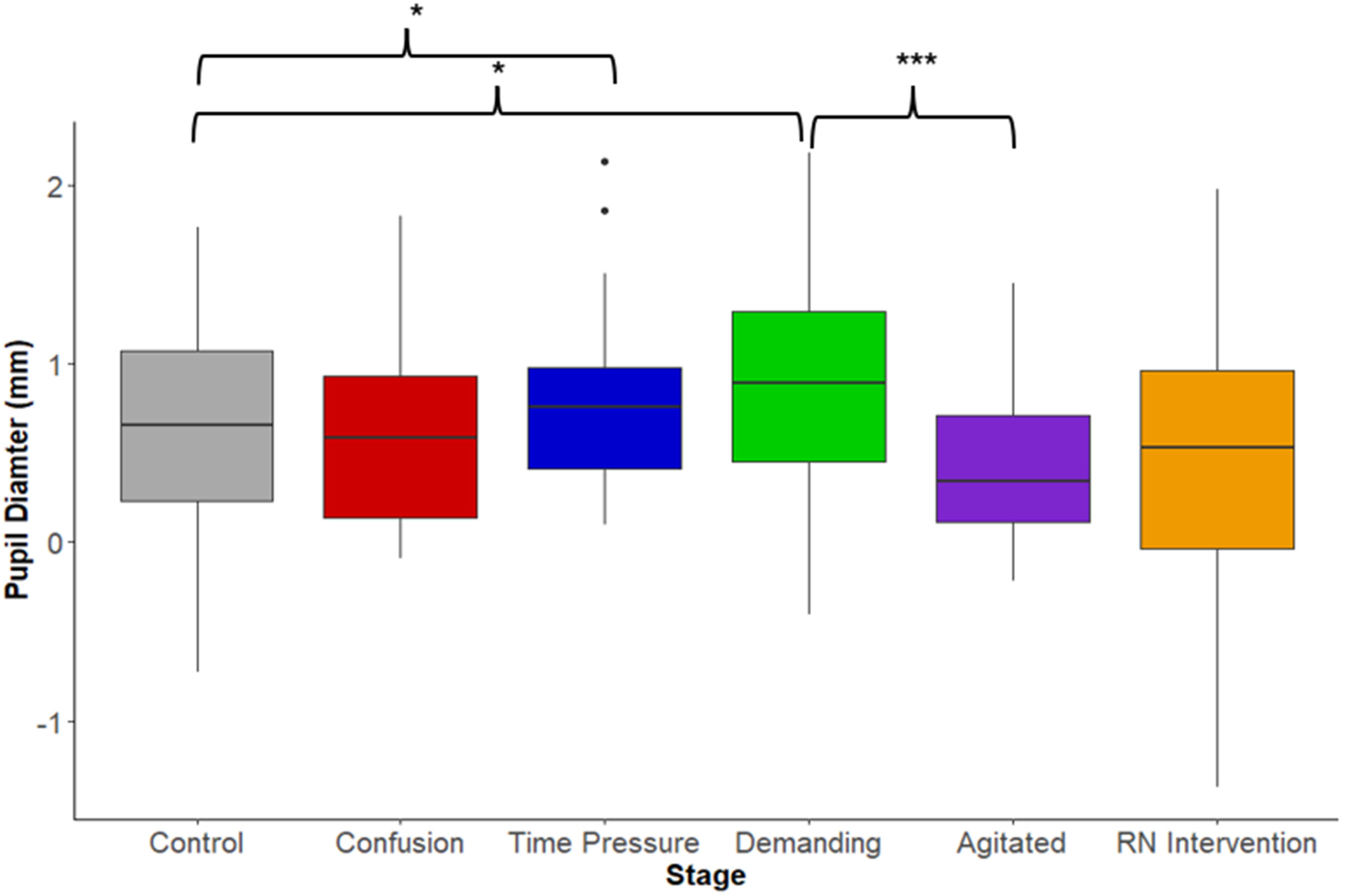
Baseline-Corrected Pupil Diameter by Experimental Stage. Note: Brackets indicate significant differences between stages. * p < 0.05, ***p < 0.001.
When comparing the three stages (1, 3, 4) that contained resident behaviours that delayed the progression of care to each other, mental workload appeared to be the lowest in Stage 4 (agitated resistance to care), as indicated by pupil dilation. Pupil dilation exhibited a significant decrease in Stage 4 compared to Stage 3 (t = 4.182, p < 0.001) and a near significant decrease in relation to Stage 1 (t = 1.937, p = 0.060) (Figure 3). However, when examining the HRV data, Stage 4 (agitated) did not differ significantly from either Stage 1 (confusion) (t = 1.383, p = 0.174) or Stage 3 (demanding) (t = −0.921, p = 0.363) (Figure 2).
Discussion
Care of people living with dementia is highly complex and, like much other work in nursing, it can be chaotic and fragmented (Surendran et al., 2024). Nursing today involves frequent disruptions and time pressures, which both contribute to an increased risk of near misses and adverse events (Jennings et al., 2022). Traditional metrics used to assess workload in healthcare—such as nurse-to-patient ratios or the number of technical tasks required in a shift—fail to capture the complexity of nursing workload (Havaei et al., 2025; Ivziku et al., 2022; Surendran et al., 2024). Research into physiological correlates of mental workload remains relatively novel, but the field is evolving rapidly as scholars refine measures to quantify this complex and abstract construct and explore the validity and reliability of these measures (Charles & Nixon, 2019; Kramer, 2020; Marinescu et al., 2018). Given the impossibility of stopping most healthcare encounters repeatedly to subjectively assess mental workload in real-time, measuring physiological correlates is a reasonable compliment (Charles & Nixon, 2019). Advances in wearable technology and sensor accuracy are enabling new forms of real-time, non-invasive monitoring of physiological correlates of mental workload that have not previously been possible (Giorgi et al., 2021; Umair et al., 2021).
This study contributes to the growing body of research investigating physiological correlates of mental workload. While subjective measures of mental strain collected from the same participants indicated high levels of strain experienced in the daily work of a LTC aide (Morris et al., 2025b), the magnitude of mental workload exhibited by the physiological indicators were less than that observed in another study involving a public speaking task (Pereira et al., 2017). The modest physiological changes observed in this study highlight the need for nuanced interpretation of the distinct factors that contribute to mental workload (Charles & Nixon, 2019; Surendran et al., 2024). The diverging trends in HRV and pupil dilation found in this study suggest that autonomic arousal (indexed by HRV) and cognitive effort (indexed by pupil dilation) reflect related but non-equivalent components of mental workload. This distinction is supported by emerging evidence that HRV and pupil dilation are governed by different, though interacting, branches of the nervous system. HRV is primarily a marker of parasympathetic nervous system activity—specifically, vagal tone—and reflects autonomic nervous system regulation of cardiovascular function (Laborde et al., 2017; Shaffer et al., 2014). According to emerging literature, it can serve as a sensitive indicator of emotional regulation in real-time (Bylsma et al., 2024). Pupil dilation is also regulated by the autonomic nervous system, but it is also modulated by central nervous system structures (Mahanama et al., 2022). According to emerging literature, it is an indicator that is most responsive to cognitive load and attentional engagement (Almukhtar et al., 2025; Krejtz et al., 2018; Wu et al., 2020). As such, HRV may more directly index emotional arousal, while pupil dilation may be more sensitive to cognitive effort. The divergent findings in our study reinforce the value of using multiple physiological indicators—not to derive a singular estimate of mental workload, but to capture its multidimensional expression (Vanneste et al., 2021).
Significant changes in physiological indicators of mental workload did not emerge during stages involving organizational expectations including time pressures and expression of workplace hierarchies. This finding is interesting in light of the consistent reports from care aides of these organizational expectations being a cause of stress, strain burnout (Booi et al., 2021; Duan et al., 2025; Page et al., 2024; Unger et al., 2022). This discrepancy highlights the complexity in the relationship between mental workload and larger well-being outcomes. While exposure to these pressures may have an impact on care aide well-being in LTC, this study suggests that the immediate effects on the demand/resource balance of mental workload (as measured by physiological correlates) are negligible. Time pressure and loss of control in a situation are often thought to increase mental workload (Galy et al., 2012; Syed et al., 2016), but acute strategies such as deferring decision-making responsibility to an authority figure (Gigerenzer & Gaissmaier, 2011) or desensitization to ever-present time pressure (Unger et al., 2022) may serve to mitigate the effects of these pressures on mental workload.
The presence of behavioural and psychological symptoms of dementia that delayed the progression of care also were associated with fewer changes in physiological indicators of mental workload than expected. The lack of physiological response to resident agitation is inconsistent with the literature about long-term psychosocial impacts of behavioural and psychological symptoms of dementia on direct care providers (Karlsen et al., 2023) and the literature focused on healthcare providers’ subjective experiences of verbal aggression (Featherstone et al., 2019; Xiao et al., 2021). In LTC settings, responsive behaviours such as verbal aggression and resistance to care are highly prevalent, particularly among residents living with dementia (Kwon & Lee, 2021). Similar to the organizational pressures, these stressors may be so common that they are processed as expected components of the job rather than as cognitively overwhelming demands, allowing the opportunity for desensitization or trained approaches to prevent acute autonomic reactions. The widespread use of de-escalation strategies observed during the simulations in this study—strategies such as redirection, offering choices, or allowing the resident to lead—further supports this interpretation (James et al., 2023). These techniques may be so well-practiced and embedded in the daily routines of care aides that they no longer require significant cognitive effort to deploy (Booi et al., 2021; Svendsen et al., 2017).
Significant increases in physiological indicators of mental workload emerged only when care aides were confronted with unresolvable resident demands—situations in which no standard response, de-escalation or deference strategy was available. This finding suggests that mental workload may rise most noticeably when routine strategies fail and creative problem-solving becomes necessary. This interpretation aligns in part with Van Acker et al.'s (2018) view that mental workload increases when task demands exceed available cognitive resources, but it may also highlight that significant changes in physiological markers of workload occur only when those demands are both excessive and novel. In these scenarios care aides may be required to step outside their familiar practices and engage in improvisational work that does not have a clear resolution. This creative cognitive effort may be a source of mental workload. To date, the literature has largely emphasized that creativity decreases as workload increases (Damadzic et al., 2022). However, these findings suggest a more complex relationship between the two, in which creativity is not diminished by high workload but may instead generate or coincide with it. This contributes to a growing body of research that explores the role of creativity in high-pressure work environments and examines how workers’ creative engagement may mediate the experience of mental workload (Chae & Park, 2023; Shao et al., 2019).
Limitations
This study has several limitations. Simulated care environments, while controlled, do not fully capture the complexity, unpredictability, or high-stakes nature of real-world clinical settings. Participant awareness of being observed and the absence of real relationships with the resident-actor may have influenced both behaviour and physiological responses (Fenske et al., 2013; Peabody et al., 2023). Light variability and visual fixation differences may have inadvertently introduced error into pupil dilation data (Bitkina et al., 2021), while HRV readings may have been affected by uncontrollable variables such as time of day or caffeine intake (Laborde et al., 2017). While every effort was made to encourage participants to avoid caffeine intake prior to the simulation, this was not always possible. The absence of performance or observational data also limits the interpretability of mental workload changes (Surendran et al., 2024). Future studies should prioritize in-situ research designs that combine physiological, subjective and task performance measures to better understand how mental workload manifests in complex care experiences.
Conclusion
This study used physiological indicators—heart rate variability and pupil dilation— as correlates to measure mental workload among care aides in a simulated LTC scenario. Findings showed that several commonly reported stressors including verbal aggression, time pressure, resident resistance, and workplace hierarchy did not influence physiological correlates of mental workload, suggesting that these routine stressors may be well-managed in the short-term through habituation and practiced coping strategies. In contrast, physiological markers rose significantly when care aides faced unresolvable resident demands, indicating that novel situations requiring creative problem-solving may be key drivers of elevated workload. This study also found divergence in physiological indicators at times, reinforcing the value of using multiple measures to capture the multidimensional nature of mental workload. Future research should link multiple physiological markers of mental workload with care quality outcomes and subjective measures, and explore how staff can be better supported to make creative decisions in their care of residents. These findings contribute to a growing body of evidence showing that mental workload in nursing is not solely driven by volume of tasks, but by the complexity and unpredictability of care interactions. Physiological evidence of mental workload offers a compelling, objective complement to existing self-report and observational data. It reinforces the urgency of investing in work environments that support care aides not only to perform tasks, but to adapt creatively and compassionately under pressure.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621251385021 - Supplemental material for Pressed for Time: Physiological Indicators of Care Aides’ Mental Workload in Response to Simulated Pressures in Long-Term Care Homes
Supplemental material, sj-docx-1-cjn-10.1177_08445621251385021 for Pressed for Time: Physiological Indicators of Care Aides’ Mental Workload in Response to Simulated Pressures in Long-Term Care Homes by Jennifer Moore, Patricia Morris, Rose McCloskey, Karen Furlong and Sue McNulty in Canadian Journal of Nursing Research
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New Frontiers Innovation Fund, NFRFR-2021-00186.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.