
Abstract
Purpose
Literature documenting mental health concerns among nurses is abundant, as is evidence that working conditions are a significant contributing factor. While conducting a study on the mental health experiences of seven professional cohorts in Canada, an unexpected finding was that for nurses struggling with their mental health, compassion profoundly shaped their experiences. This paper reports findings from a secondary analysis of the nursing cohort of this dataset to examine the role that compassion played in the experiences of nurses, their interprofessional relationships, and engagement with institutional policies and processes. Qualitative analysis of interviews with 52 nurses across Canada was conducted using interpretive description's inductive approach. Analysis was guided by the conceptual framework of Compassionate Communities.
Results
Compassion in the workplace impacted nurses’ experiences of mental health, the process of requesting a leave of absence, and negotiating return to work. Nurses described how practicing in uncompassionate environments prompted them to engage in presenteeism at the expense of their own wellbeing, often missing the signs of their distress. Seeking help was deemed more complicated than remaining at work; leave of absence and return to work processes were marked by uncompassionate responses from managers and institutional procedures. Nurses encountered stigma when disclosing a mental health concern, negatively impacting their professional identity and interprofessional relationships.
Conclusions
Implementing compassionate organizational practices and processes is instrumental in supporting nurses’ mental health experiences and supporting psychologically safe work environments. This paper adds to the literature on compassion, compassionate communities, and nurses’ mental health experiences.
Keywords
Introduction
Public health emergencies often bring increased attention to the wellbeing of health care workers (Chigwedere et al., 2021; Galanis et al., 2021; Kim et al., 2021). The COVID-19 pandemic starkly exemplified this, leading not only to a steep rise in psychological distress among healthcare workers (Stuijfzand et al., 2020), but also exposing the devastating impacts of chronic underfunding and resource scarcity on patient outcomes (Murray, 2023).
Concerns about healthcare professionals’ psychological distress predate the COVID-19 pandemic, with decades of research showing a clear link between challenging working conditions and healthcare workers’ mental health (Nolan & Smojkis, 2003; Sönmez et al., 2023). The nursing profession is characterized by high responsibility, demanding job roles, and occupational stress, coupled with low professional autonomy (McGrath et al., 2003). These factors, compounded by irregular scheduling, exhaustion, vicarious trauma, the emotional toll of caring work, and toxic work environments, place nurses at high risk of mental health concerns (Cares et al., 2015; Sönmez et al., 2023).
Similar to many countries, Canada is grappling with a chronic shortage of nurses (Ben-Ahmed & Bourgeault, 2022). There are multiple factors contributing to this shortage, notably not enough nursing school graduates to replenish workforce attrition. Currently, the most critical contributor to the nursing shortage is attrition, with nurses exiting the profession at alarming rates. As healthcare sector vacancies in Canada rise exponentially, implementing effective retention strategies for nurses across all career stages is critical to retain the current workforce (StatsCan, 2022, 2024).
In response to the skyrocketing rates of psychological distress among nurses in recent years (Akoo, McMillan et al., 2024; Havaei et al., 2023; McMillan et al., 2023; McMillan et al., 2021), Canadian researchers and policymakers turned their attention to psychological safety as a means of supporting nurses’ mental health and bolstering retention efforts (CIHR, 2022a, 2022b; CNA & CFNU, 2014; RNAO, 2017). Psychological safety in the workplace centres on interpersonal processes and strategies that sustain positive work environments, thereby reducing errors and enhancing overall safety (Edmondson, 1999; Newman et al., 2017), while promoting and preserving employee physical and mental well-being. While early work in psychological safety research emphasized learning and performance outcomes, psychological safety is now understood more broadly as it intersects with employee attitudes, ethical conduct, stress management, team conflict resolution, mitigating incivility and bullying, organizational commitment (Edmondson, 1999; Newman et al., 2017; Simpson et al., 2020; Wouters-Soomers et al., 2022), making mental health an important aspect of psychological safety.
In this paper we present findings from a secondary analysis of nursing-specific data drawn from a larger study that explored mental health experiences of seven professional cohorts in Canada. While qualitative results from the nursing data set have been published elsewhere (Akoo, McMillan et al., 2024; Akoo, Price et al., 2024; Bourgeault et al., 2022), a significant and unexpected finding was that for nurses struggling with their mental health, compassion (or a lack thereof) profoundly shaped experiences of struggle, the process of requesting a leave of absence and negotiating a return to work. This finding prompted a secondary analysis of the data to examine how compassion may support nurses’ mental health experiences in the workplace. The purpose of this paper is to report these secondary analysis findings, highlighting the role that compassion played in the experiences of nurses struggling with their mental health. The research question for this study was: What is the impact of compassion on nurses’ mental health and wellbeing, and its potential in fostering enhanced retention in the nursing workforce and return to work following a leave of absence? In that context, we examine the role of compassion in individual nurses’ experiences, interprofessional relationships and engagement with institutional policies and processes. In the discussion, we review the significance of these findings, and draw links between nurses’ mental health, broader psychological safety needs and compassionate communities.
Framework
A conceptual framework on Compassionate Communities was developed to guide the current analysis (Sofronas & McMillan, 2025). Compassion is the recognition of the suffering of another, and for nurses, this recognition comes with a moral and professional obligation to intervene to alleviate this suffering (Ferrell & Coyle, 2008; Schantz, 2007). Compassion is a core nursing principle most often understood as something nurses provide to patients in the context of care to relieve suffering, enhance therapeutic relationships and improve patient outcomes (Ferrell & Coyle, 2008; Schantz, 2007).
To practice compassionately, however, nurses need to work in spaces and places that consistently support, value, and enact the principles of compassion, both for patients and for employees. However, current literature suggests just the contrary: nurses work in environments that are uncompassionate and uncaring towards them (Abrams et al., 2024; Stacey, 2024). Uncompassionate work environments display repeated lack of acknowledgment from leadership for the difficult work experiences of employees, lack of empathy regarding the experience of trauma in the workplace, dismissal of ongoing workload issues, and a failure to recognize and address toxic work environments (Abrams et al., 2024; Stacey, 2024). As a result, nurses feel devalued, unsupported, and replaceable, leading to decreased organizational commitment and increased intent to leave (Abrams et al., 2024).
The analysis reported in this paper was guided by the Compassionate Communities framework to connect work environments and mental health experiences among nurses. Compassionate Communities are defined as moral communities that invest in and promote ethical behaviour from individuals and groups that make up such communities (Sofronas & McMillan, 2025). Compassionate Communities are built and sustained through compassion-focused education strategies, advocating for compassionate leadership practices, and implementing societal structures and/or policies that prevent or reduce suffering. In addition, Compassionate Communities actively promote health and wellbeing, community support and empowerment of community members in physical, social, organizational and living environments, as well as in infrastructure (Sofronas & McMillan, 2025; Vanderstichelen et al., 2022). The Compassionate Communities framework offers a philosophical shift in the construction of psychological safety, particularly in relation to employee mental health, and closely aligns with the goals of healthcare organizations and those of the nursing profession (Sofronas & McMillan, 2025).
The challenge of prioritizing compassion in healthcare environments amongst a variety of competing priorities is not new. Over 20 years ago, Nolan and Smojkis (2003) reflected on such challenges: “It seems that health care has become emotionally distant and the [nursing] profession's longstanding attachment to caring through interpersonal relationships has been overridden by a high technology, fast-track system of care management” (p.374). They argued that retaining the principles of caring required a heightened focus on the environments in which nurses work (Nolan & Smojkis, 2003).
Methods
Design
This study is a secondary analysis of interview data from the Healthy Professional Worker (HPW) partnership, a larger study examining the mental health experiences of seven Canadian professional cohorts. The HPW partnership was a multimethod study that included document analysis, stakeholder interviews, worker surveys, and interviews. Research ethics approval was obtained from the University of Ottawa Office of Research, Ethics, and Integrity (S-05-19-2508). Ethics approval was also obtained from 15 institutional review boards in Canada, due to the scope of the parent study.
Sample
The nursing cohort data consisted of 52 clinicians across Canada who agreed to participate in semi-structured interviews about their mental health in relation to their professional lives. Participants were recruited using crowdsourcing methods through partner organizations and social media. The sample (n = 52) consisted of 34 registered nurses, six licensed practical nurses, one registered psychiatric nurse, seven nurse practitioners, and five who chose not to disclose their professional affiliation. Most participants identified as female (n = 46), with seven males and no nonbinary or gender fluid individuals. A total of 38 participants reported having taken a leave of absence (LOA) for their mental health, one participant was prohibited from taking an LOA by their employer, and one participant declined to respond.
Data Collection
Interviews were conducted virtually in English and French between September 2020 and July 2021, and audio recorded for analysis. After collecting baseline demographic data, interview questions centred on nurses’ mental health challenges, the process of obtaining a leave of absence and return to work experiences (when applicable). Interview recordings were transcribed verbatim via otter.ai and verified by members of the research team for accuracy. Data was de-identified, and quotes used in publications were altered to protect participant anonymity while remaining faithful to the ideas and experiences articulated. Informed consent was sought verbally and in writing. Data for this study was collected during the COVID-19 pandemic, a crisis moment for health professions worldwide. Though study participants shared experiences of mental health struggles that most often predated COVID-19, the impact of the pandemic on nurses’ mental health across Canada and globally was significant, undoubtedly impacting participant responses.
An important finding suggested that compassion (or the lack thereof) was central to nurses’ experiences, and supported intent to return to work, subsequently impacting retention, despite compassion not bring central to the original research purpose or questions. This finding led to the current study.
Data Analysis
Data analysis was conducted using NVivo to help organize the large volume of data and catalogue themes. Interpretive description's inductive approach to analysis was used, wherein researchers reflectively examine data, drawing out meaningful themes and patterns related to the phenomenon of interest; the Compassionate communities framework served as a conceptual scaffold to guide the interpretive process (Sofronas & McMillan, 2025; Thorne, 2016). Each transcript was read once in its entirety to get an overview of the narrative. The principal researcher (MS) prepared a narrative summary of each interview, followed by a closer reading that noted significant words, phrases, and ideas articulated. We focused on the ways in which individual experiences were shaped by the workplace climate, specifically relating to compassion. Thematic analysis helped bring together common patterns and perspectives, paying special attention to locating the broader contexts of individual accounts (Braun & Clarke, 2006). This involved making explicit links between individual experiences and the presence or absence of structural and moral supports (e.g., compassionate leadership practices and policies) outlined by the framework (Sofronas & McMillan, 2025). Narrative syntheses were then prepared by the principal researcher, a postdoctoral fellow supervised by the senior author, bringing together overarching themes that emerged across interviews. Throughout the analytic process, the co-authors (who were familiar with the data from the original study) engaged in reflexive discussions about the significance and meaning of the data, and broader theoretical, practice, and policy implications.
Results
Nurse participants shared experiences of struggling with their mental health across seven dimensions, reflecting on the role of compassion. Thematic findings showcase how (1) nurses felt they were expected to practice in challenging settings that demanded their giving of compassion at the expense of their own wellbeing. Under these conditions, (2) nurses often missed the signs of their own distress, despite having extensive clinical expertise in assessing and caring for others. Participants reflected on (3) ‘the invisible labour of seeking care,’ with the burden of attending to their own mental health care set against engaging with presenteeism. Finally, (4) the impact of mental health stigma weighed heavily on their experience of distress and decision to seek help (or not), due to concerns about personal and professional consequences.
The challenging process of requesting a leave of absence (5) and the tumultuous experience of returning to work (6) exposed uncompassionate reactions from colleagues and managers, as well as inequitable institutional practices. Although much of the data reflected overwhelmingly negative experiences that lacked compassion, there were a few examples of positive experiences of asking for help, requesting leaves, and returning to work, whereby compassion was evident (7). These narratives were included to showcase the positive impact of compassion as it relates to nurses’ mental health experiences. Themes are displayed in Figure 1.
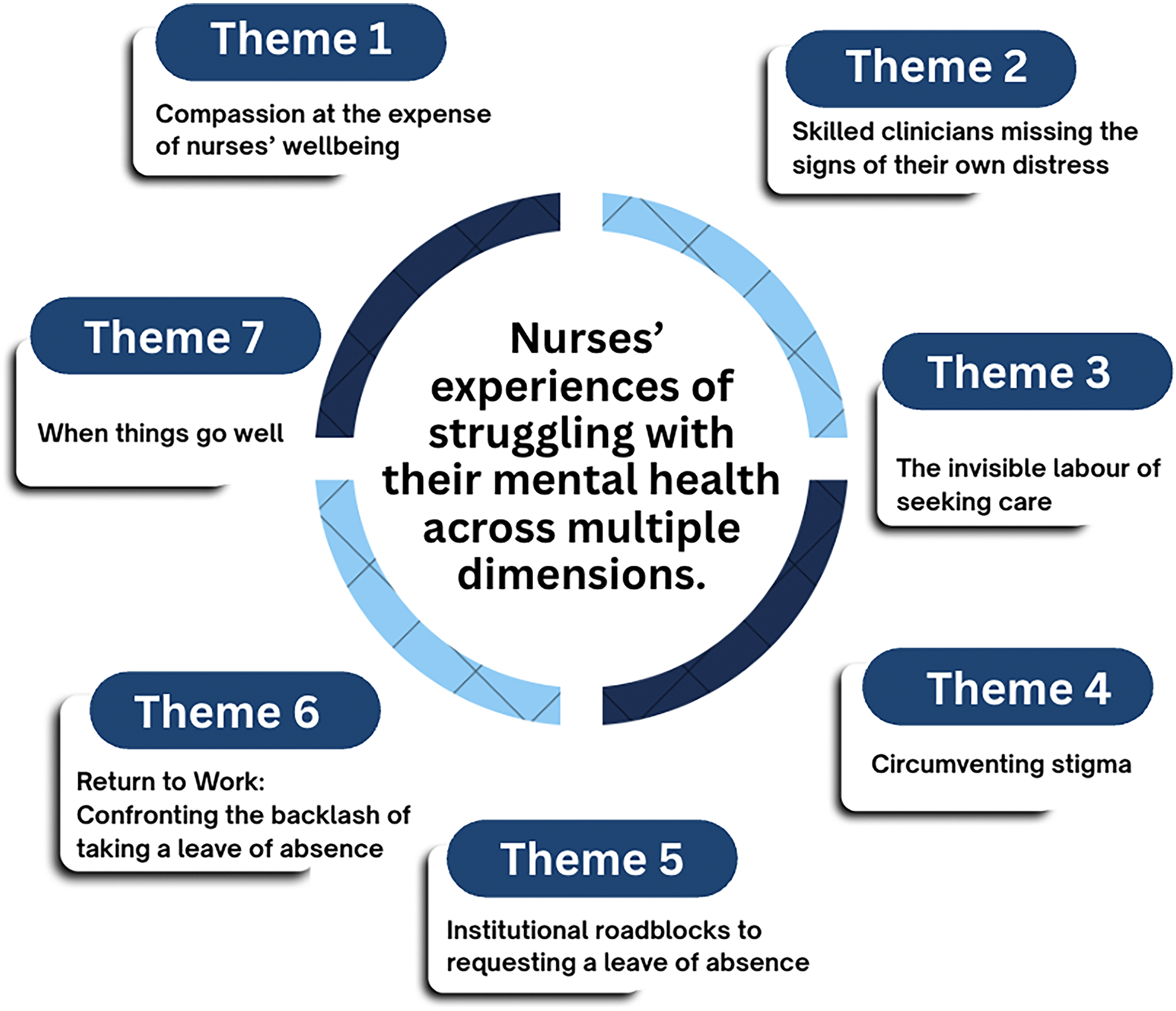
Thematic Findings.
Compassion at the Expense of Nurses’ Wellbeing
Nurse participants felt strongly that compassion was at the centre of their practice. However, the demands of caring amidst high workloads, chronic understaffing, low autonomy, and high risk of physical, emotional, and moral injury demonstrated to them a variety of ways in which compassion was not enacted towards nurses themselves. One participant highlighted the impossibility of such conditions: You’re supposed to provide care for other people, but you’re supposed to be infallible, and you’re human at the same time, which isn’t possible.
The following participants noted a lack of compassion for nurses from others, and from themselves: We’re a caring profession but when we need somebody to take care of us, it's really hard to find. We have to do it ourselves. I don’t know if it's in our makeup as nurses, but you give, give, give and you kind of put yourself on the back burner.
Many nurses felt that they were caring for others at the expense of their own health and wellbeing. They pushed themselves to work when they were exhausted and mentally unwell, due to staffing shortages that put their colleagues and patients at risk, as backfill for sick calls or leaves was rare. They were also swayed by ongoing expectations of self-sacrifice and the continuous giving of self that characterizes the nursing profession. For example, one participant stated: We feel such a responsibility to the people that we care for at work. I’m afraid that if I’m sick, if I’m not at work, then we’re going to be short. And then the ultimate end is that our patients will suffer.
The following participant reflected on the relational complexities at play when nurses contemplated a leave of absence to manage their mental health: I think it would be very hard to feel that you weren’t burdening other people. Depending on the length of a leave of absence, someone would replace me. I would be asking other people to take on my workload because I wasn’t there. I think it's hard to know that you’re doing that to your colleagues. I almost feel that someone would have to really point out how important it was that I get that time away, that I need it for my wellness because of the guilt or burden you would feel about leaving other people with your workload.
Another participant expressed feelings of guilt, whilst suggesting a relationship between guilt and blame in this context, where external blame reinforces internal guilt: There is a culture of guilt. You don't have the right to be sick; you have to be super-efficient all the time. If you ask for help, it's because you're not good, you're not managing your workload. There's a culture of blame: you’re the one who isn’t good enough, who's not a good nurse, who's not professionally competent.
Nurses made a connection between the pressures [both internal and external] to care for others at the expense of their own wellbeing, and the lack of support they received from their institutions in the context of their ongoing sacrifice of personal wellbeing: Since March [2020], no one came to see if we were OK. They [employers] didn’t offer debriefing when we encountered difficult situations. We were broken people holding up broken people; that's the culture of nursing. But having to hold everyone up, it took a toll on me.
Collectively, these quotes highlight numerous instances where the enactment of compassion towards nurses was either thwarted or simply absent. This was attributed to numerous sources, from nurses themselves and others in their units and departments, through to the level of the employer. Nurses also identified specific cultures within nursing and the institutions that employed them as contributing to this lack of compassion.
Skilled Clinicians Missing the Signs of Their own Distress
One repeating narrative in the interview data was how long it took for nurses to recognize that they were unwell. It was surprising how exceptionally skilled clinicians working across multiple specialities shared normalized experiences of either ignoring or altogether missing the signs of their own distress. Two examples are presented below: I had been feeling … not fantastic for about nine months. But I had been ignoring it because, well, everyone was having a hard time. It was the pandemic. I told myself, ‘Just push through it, that's what everyone's doing right now. I should be able to do the same thing.’ Somehow, things weren’t going well for me. I couldn’t say it will just work out. I had to see a therapist. And they told me: ‘I think you have anxiety and depression.’ That was a shocker to me. It took me a while to realise, yes, that could be true.
This finding presented a significant paradox, that while working in difficult conditions, caring professionals, highly trained to identify distress in others, had normalized feeling unwell and neglecting themselves in ways that led them to ignore what were in fact signs of distress.
The Invisible Labour of Seeking Care
For many nurses, the process of requesting a leave of absence was more cumbersome and complicated than remaining at work [presenteeism]. The following quotes suggest that procedural barriers and uncompassionate organizational cultures that did not support nurses in attending to their mental health posed significant barriers: I said, I can’t do this anymore and saw my doctor. I contacted my union, contacted HR [human resources]. But once again, it was entirely me getting connected to care. I told my doctor who to refer me to. In that state, I still had to run my care. Trying to take a leave of absence is the biggest barrier. Navigating, sitting down with a practitioner and establishing the steps that you have to go through to take a leave seemed more overwhelming than just coping at work.
Structures of support, such as employee assistance programs (EAP), had mixed results for participants. Nurses experienced long wait times for appointments, generic interventions that didn’t address the nature of their struggles, and a lack of integration with the health care system. One nurse recounted an interaction with a counsellor that was devoid of compassion and care, demonstrating a lack of understanding of the nurse's experience: I started out by contacting my EAP and was set up with a counsellor (…) and basically, they recommended a bunch of books and said, ‘Well, you’re a health professional, you know what you need to do,’ which was not helpful at all.
Another participant recounted an unhelpful exchange with an EAP counsellor, where self-care was recommended without consideration of the various structural antecedents shaping their poor mental health: At the beginning of the pandemic, I was on alert all the time, I was having panic attacks when I had never been anxious before. I called the [EAP] in tears and waited 3 weeks for an appointment. And it was not helpful at all, I felt like I [the counsellor] was reading me a self-care guide… She said, “you could go run in the stairs when you're feeling a little anxious at work.” I don't have time to run up the stairs! She said, “Take walks, eat right…” Well, that didn’t make sense.
Participant experiences draw attention to shortcomings of existing strategies to support nurses. Even when nurses sought support, they were tasked with solving seemingly structural problems to obtain supports, or received access to interventions that were not helpful, nor compassionate - which only intensified their struggle.
Circumventing Stigma
The ongoing stigma associated with mental health struggles was not lost on study participants, who reflected on how much easier the process of navigation would be if they suffered from a physical illness, something that was visible, with a measurable impact on their ability to practice nursing: If it was a physical injury, it would be so much more cut-and-dry and the manager would understand right away.
A nurse who suffered from mental illness and a respiratory condition reflected on how simple it was to request a leave for her respiratory condition, which contradicted her experiences navigating her mental health in the workplace: It seems more acceptable to be off [for physical illness], and the paperwork was a lot easier. All you had to do was look at my medical records. And you can see the number of times I was admitted or in the emergency room. That ended up being fairly easy, my respirologist ended up doing all the paperwork.
Stigma concerns were amplified for nurses practicing in rural or remote areas, as they had to seek care where they worked, often from colleagues, due to the scarcity of practitioners. One nurse went to great lengths to hide her mental illness with the support of a psychiatrist colleague who helped her access care while taking personal and professional risks to do so: When I went to see the psychiatrist, she did not chart anything. She didn’t make me part of her client base, she didn’t get paid, she didn’t bill for it. She did it on the down low so it would be kept confidential.
Another nurse practicing in a remote area joined a support group disguised as a clinician, with the endorsement of the group leaders, to access support without stigma: Probably the best thing I could have done for myself, what kept my head above water, was to take care of my own mental health by becoming…a disguised client. The group leads presented me as a clinician who was getting oriented to the group. But really, I was a client in that group to learn how to take care of myself.
Even nurses who worked within mental health care departments or facilities were not immune to stigma: As a mental health nurse, I was working with patients who were suicidal, depressed, in crisis. And I just had a constant fear that my team was going to think that I was incompetent. I couldn’t show weakness because of the area that I worked in, how could you work here if you’re that affected.
A few nurses requiring urgent care for their mental health recounted being admitted to the emergency departments where they worked. This created impossible tensions where they had to sacrifice their confidentiality and professional identity to receive life-saving care: They put me in the isolation room. I could hear them whispering and talking. And one of the physicians [caring for me] was someone I worked with so closely for years. And that was probably the hardest thing.
Another participant provided the following reflections: When I was diagnosed my physician hospitalized me on the unit where I used to work. Well, certainly, I almost left nursing! It was horrible. We’re not doing well there [with mental health stigma]. There's so much judgment.
Participants who took a leave of absence worried their credibility and professionalism would be impacted upon their return to work. In some cases, the discrimination was overt, but in others it was less clear, causing nurses to question their own capacity and clinical judgement: I was told to be in the office every day. My co-workers could work from home. I’m very micromanaged. I’m always on time, never missed a deadline. My cases are very thoroughly researched. There's no reason for me to be monitored [yet I am].
The fear of stigma, as well as the direct consequences of stigma shaped how these nurses experienced their mental health concerns, sought care, returned to work, and ultimately how they perceived themselves as nursing professionals. These themes are explored in the following sections.
Institutional Roadblocks to Requesting a Leave of Absence
The process of obtaining time off for reasons pertaining to mental health, from sick days to longer leaves, exposed nurses to uncompassionate institutional practices. This included interactions with direct supervisors, as well as navigating procedures to apply for a formal leave of absence. Nurses’ concerns about the consequences of asking for help were indeed realistic appraisals of the roadblocks present in institutional procedures. For many nurses, their first point of contact with their institution was their unit manager. Here, nurses were confronted with uncompassionate attitudes and behaviours that minimized and denied their distress: I initially approached my manager to look at options, because I was struggling with my mental health at work. I was told ‘you can’t be considered for any type of stress leave, because stress is such an umbrella term, anyone would be able to go on stress leave. You know, if that existed, anxiety and depression.’ It was a horrible two months of trying to prove myself, trying to get some form of income for missing work.
Another nurse received unsolicited advice from their manager that diminished their experience, suggesting that nurses lacked the capacity to cope: When I told my manager that I wasn’t coming back work, she said ‘just don’t let them prescribe these antidepressants. You need to just get out, you need to exercise, you need to just put this behind you and get on with life. You don’t want to become a zombie on pills.’ She said that she had lots of nurses that were off because they can’t handle life.
Many nurses encountered obstacles once they submitted paperwork requesting a leave, and were pressured to return to work: I put in my request for two weeks of leave, I just needed to figure things out. And I got a letter from management saying, ‘come back to work or give up your job.’ So, I resigned. As a full-time employee, there were processes in place. I was off for three months on stress leave, but after two weeks, I felt pressured to come back. I had to justify, every 2 weeks, why I still needed to be off. And I was extremely non-functional.
Institutional requirements necessitating a physician's note to justify an absence of more than a few days highlighted a lack of confidentiality in the treatment and safeguarding of nurses’ personal health information. This was particularly concerning for nurses working in rural or remote communities: I can’t take more than three days off in a row without a sick note. For mental health, I would have to get a note from my psychiatrist, which would cause stigma (…). Because the sick note doesn’t only go to my manager, it goes to the director, and it goes to human resources. It is seen by multiple people, and in a small town, it's known if you saw a psychiatrist, a surgeon or family doctor. And you don’t want to be the one who has issues.
Finally, forms for requesting medical leaves were disproportionately configured for physical illness, meaning they were difficult to complete when asking for a mental health leave: The forms are generic, functional disability forms, they don’t address the mental health aspect. When you start giving the information, it doesn’t fit into the box. And they ask for way too much personal information. If it's a physical ailment, Sure, I’ll provide the MRI, I’ll provide the surgical report. Not a problem. But with mental health, and especially when the workplace is the main focus of the [my] mental health issue, there's a real conflict there.
For participants, the interactions and processes associated with requesting a mental health leave served to diminish the validity of their health concerns and left them feeling vulnerable as their personal information was shared with multiple individuals at multiple levels of their workplace.
Return to Work: Confronting the Backlash of Taking a Leave of Absence
When leaves were approved, the struggle was not yet over. Returning to work after a mental health leave exposed nurses to questions about their professional competence and risked their career prospects. Nurses were also conflicted about having taken a leave while the healthcare system was so understaffed. Prioritizing their health meant their colleagues were given higher workloads to manage, which could create new workplace tensions: That first day I came back after my leave, my manager had me in tears in her office because she was telling me how hard my absence was on the rest of the team, and who had to do what to cover for me.
Blaming the chronic understaffing of the health care system on nurses who were off sick reinforced the trope of the self-sacrificing nurse, that self-sacrifice was expected to remedy system shortcomings such as understaffing. One nurse argued that their mental health diagnosis stigmatized them in ways that questioned their dependability and employability, positioning them as a risk to the workplace: There is an underlying belief, from an employer's perspective, that if you have a mental health challenge, you become more of a risk to not be able to do your job. And you are at risk of using more sick time than others. So, you’re not classified as a good employee. You’re an employee that they don’t want.
Finally, nurses worried whether their mental health leaves played a role in their career prospects long after their return: After my leave, I felt like I was being excluded permanently. Advancement opportunities, team leader, filling in for the head nurse… I had spoken with my manager about my desire to be in more of a leadership position. And they asked everybody except me when they were looking for someone to fill in while the manager was off. Nobody said it was because of my mental health. But with my work record, the projects that I had completed, my relationship with my co-workers, there really was no reason why I shouldn’t have been considered.
Another participant reflected on the longstanding legacy that taking a mental health leave left, even after the nurse had pursued employment at another healthcare institution, and tried to return to the site she had taken a leave from: I really enjoyed working there. And I’ve tried to go back, apply for openings that I’m very qualified for. And they don’t even call. I just feel like I’ve dug myself a hole there. Like I burned that bridge, I could never go back. And it's frustrating because I did nothing wrong to lose that job. But because of what I went through, they won’t even give me a chance. That's what it feels like when I’ve reached out. They’re so desperate for nurses and yet, I’ve applied and don’t get a call. I feel like there's this giant black mark on my file, saying don’t hire her because she can’t handle it.
Accounts of experiences returning to work show that taking a mental health leave often brought about new challenges and further stigmatization for nurses. When they returned to work, they faced backlash in multiple forms: blame for further contributing to understaffing, ostracization by colleagues, and persistent stigma impacting their professional identity and career advancement.
When Things Go Well
The data presented to this point predominantly chronicles negative experiences, which reflects the trajectory of most participants. Lack of compassion was readily apparent in participant experiences. However, a small number of participants reported positive experiences in requesting leaves and returning to work, and these accounts present persuasive arguments for harnessing compassion when navigating employee mental health experiences, notably when employees are struggling with their mental health. This theme is presented as a counter-narrative, one that serves to demonstrate the power of compassion in the context of caring for nurses. One nurse was concerned about asking for a mental health leave of absence, having to disclose the reason they needed time off, and how their manager would respond: I called my manager, because I didn’t want to write anything in an email, I didn’t want a paper trail or have something in my file. I explained what I could in a minimalistic kind of way. And she was very supportive right away. She said, I totally understand, how much time do you think you need? We settled on a three-week leave of absence. Then she just sent me the paperwork to fill out and send back to her. And thankfully, I got that time off with very little notice.
Two additional participants were concerned with the process of requesting a leave, which required disclosing a mental health diagnosis, being believed, and providing the documentation required by their employer. When the process was straightforward, non-judgmental, and compassionate, it was easy for them to focus on their recovery: When I had the relationship breakdown, I took six weeks off, a medical leave of absence supported by my family doctor. He diagnosed me with depression, provided treatment, a sick note, he reassessed me every two weeks, and at six weeks, I went back to work and that was fine. I called employee wellness. I was very honest with her, and she was very supportive. I told my manager that I needed some [psych] med adjustments [that would require time off], and I just felt very supported.
When employers advocated for nurses, facilitated human resources processes, and openly discussed options and employee benefits, this also made a substantive difference. For example, one participant was contract-based and not aware of their eligibility to request a leave, so they had planned to decline their next contract because they were struggling with their mental health, which would have made them ineligible for employee benefits. However, a compassionate interaction with their manager facilitated an alternative approach and a much better outcome: When my contract ended, I was going to be automatically recalled for the next contract. I knew that I wouldn’t be able to go back. But I didn’t want to say no because I would have lost my seniority. I contacted my manager and explained what was happening and asked for her help. And she advised me on what to do. She said, ‘accept the job and sign the contract saying, you’re going to do the job and then ask for the leave of absence.’ She really was key because I had no idea, and I was scared. If I hadn’t taken the job, I wouldn’t have access to [employee benefits], I wouldn’t have had anything that I needed.
In stark contrast to the predominantly negative experiences found in most of the data, a small number of participants reported positive interactions. Their stories serve as a powerful reminder of the transformative impact of compassion, advocacy, and empathy from leadership, which played a critical role in supporting nurses navigating their illness and recovery.
Discussion
Participants held compassion as a central tenet of excellent nursing practice, yet recounted working conditions that were wholly uncompassionate towards them. Despite holding compassion in high regard in their profession, nurses did not receive it from their colleagues or from their institutions when they needed it. The mismatch between what they provided for patients and the way their health concerns were perceived and managed in the workplace was a significant antecedent for what came next. Nurses continued to provide compassionate nursing care at their own expense, exemplified by missing the signs of their own distress, overwhelmed by the invisible labour involved in seeking care, and worried about the impact of mental health stigma on their professional lives. These narratives repeated themselves in the challenges of requesting a leave of absence and navigating their return to work, reflecting uncompassionate structural conditions in their workplaces.
The idea of ‘giving’ of oneself was not a source of concern for nurses; however, the expectation of excessive giving at the expense of their own wellbeing impacted their mental health. These findings align with research on compassion fatigue: that acting compassionately does not lead to compassion fatigue. Instead, it is a common occurrence in caring professions, linked to burnout and vicarious trauma, caused by repeated exposure to suffering, stressful work environments, chronic understaffing, and poor work-life balance (Sorenson et al., 2017; Wynn, 2020). Despite these insights, compassion fatigue continues to be erroneously presented as an individual problem, overriding structural and economic factors that create conditions that make compassion difficult to enact without personal cost (Brito-Pons & Librada-Flores, 2018). Study findings contribute to the literature on compassion, highlighting its necessity in the context of nurses’ mental health, and its limitations when understood solely as an individual virtue rather than a structural or institutional attribute.
Having learned not to expect compassion while suffering themselves, nurses in this study often missed signs of their own distress, viewed their needs as expendable, and worried about their professional futures instead of their current wellbeing. Considering the significant roadblocks nurses encountered when requesting and returning from a mental health leave, their delayed and reluctant requests for help are unsurprising. Although mental health concerns are well-documented among nurses, there remains a significant gap in evidence on how to best support nurses who request a leave for their mental health, and how to facilitate their return to work (Bourgeault et al., 2022; Covell et al., 2020). Findings showcasing positive experiences, albeit from a small minority of our sample, suggests that compassion played a significant role: participants who received compassion were able to focus on their recovery without worrying about cumbersome leave-related processes, stigma, or pressure to return to work prematurely. These participants, unlike those sharing negative experiences, also did not question their institutional commitment or consider leaving their workplace.
It is noteworthy that the examples of compassionate and uncompassionate interactions found in the data were almost exclusively situated within manager-nurse interactions. While promising scholarship exists on leadership practices that promote compassion in healthcare, serving to bridge these two concepts (Cho et al., 2023; de Zulueta, 2015; Kouta et al., 2022; Salminen-Tuomaala & Seppälä, 2023), these initiatives are often presented as person-dependent, rather than being built on sustainable institutional foundations and principles of healthy and psychologically safe work environments (Ahmed et al., 2024). This challenge was also reflected in study findings: examples where compassion was systematically embedded or operationalized in organizational structures or processes were not found in the data. Of note, nurse managers themselves also require compassion and institutional support to enact these principles. This is an area requiring further study.
Study findings prompted a deeper reflection on the areas of convergence and divergence between the concepts of compassionate communities and psychological safety. Both approaches share foundational principles of fostering empathy, connection, trust and belonging, while promoting openness to vulnerability, reducing stigma, and encouraging proactive support (Dumont et al., 2022; Ito et al., 2022; Quintiens et al., 2022). However, they also differ in some important respects. Psychological safety, a concept developed in organizational and management studies, primarily examines professional life, focusing on specific organizations and teams (Edmondson, 1999). Compassionate Communities, rooted in public health and palliative care, adopt a much broader scope, encompassing individuals, families, entire communities, and cities across both professional and civic realms (Kellehear, 2012). These differences are apparent in their definitions: compassionate communities view health and wellbeing as a shared responsibility beyond the formal health sector, requiring support from political structures, social services, community organizations, and work environments for prevention, health promotion, harm reduction, and early intervention (Kellehear, 2012; Sofronas & McMillan, 2025; WHO, 1986). In contrast, psychological safety emphasizes leadership behaviours and team dynamics that create positive work environments where employees feel safe to ask for help, receive feedback, report errors, and support psychological wellbeing, including mental health (Edmondson, 1999; Newman et al., 2017; Wouters-Soomers et al., 2022).
Despite their differing scopes, compassion is a critical element central to both compassionate communities and psychologically safe workplaces (Newman et al., 2017; Salminen-Tuomaala & Seppälä, 2023; Sofronas & McMillan, 2025; Wang et al., 2024; Wouters-Soomers et al., 2022). Study findings illuminate the importance of experiencing compassion not only for nurses’ mental health, but also for retention. For the nurses in this study, receiving compassion (or not receiving any) significantly shaped their experiences of mental health struggle, requesting a leave of absence, and returning to work. This aligns with existing literature: when compassion and psychological safety are prioritized, employees feel a sense of inclusivity and belonging, wellbeing becomes a collective responsibility, and stigma is reduced (Dumont et al., 2022).
Interventions promoting psychological safety are most effective when they embody principles of care and compassion in attending to employee needs (McMillan & Perron, 2020; Simpson et al., 2020). Compassionate communities, conversely, call for broader structural and policy changes that foster compassion by way of prioritizing equity, social justice, power-sharing, relationship building, mobilization, and empowerment, in addition to shifting management strategies and human resource approaches (Bakelants et al., 2023; Sofronas & McMillan, 2025; Vanderstichelen et al., 2022). Therefore, engaging with tenets of both psychological safety and compassionate communities can augment strategies to embed compassion into institutional norms, structures, and leadership practices, thereby buffering against poor mental health and supporting recovery (Brito-Pons & Librada-Flores, 2018; Nolan & Smojkis, 2003). This, in turn, can support staff retention and decrease absenteeism (Cho et al., 2023; Pressley & Garside, 2023).
Nursing is an inherently demanding profession, characterized by long hours, ethical tensions, and disproportionate responsibility for patient safety and wellbeing (Marufu et al., 2021; O'Brien-Pallas et al., 2010). The abundant literature documenting nurses’ mental health concerns and the exacerbating role of working conditions underscores this reality (Cares et al., 2015; Chigwedere et al., 2021; Galanis et al., 2021; Kim et al., 2021; McGrath et al., 2003; Nolan & Smojkis, 2003). It is therefore imperative that interventions addressing nurses’ declining mental health target systemic and organizational factors, rather than solely rehabilitating nurses to return to the same conditions that compromised their mental health and necessitated a subsequent leave of absence.
The sustainable infusion of compassion into institutional structures such as responsive and meaningful mental health supports, streamlined leave processes, and leadership that mobilizes compassionate responses, as opposed to stigmatizing responses when attending to nurses’ mental health struggles —cannot be entirely successfully without concurrently addressing underlying structural and organizational challenges like poor work environments and excessive workloads (Bourgeault et al., 2022; CIHR, 2022a, 2022b; CNA & CFNU, 2014; Heistad et al., 2022; RNAO, 2017) – which in and of themselves, would serve as a profound act of compassion towards nurses. Indeed, as Wang et al. (2024) attest, the relationship between compassionate behaviours and psychological safety is known to weaken under high workload demands. This collectively underscores the critical importance of embedding compassion at structural levels—into organizational practices and processes, a significant roadblock evident in our study findings.
This roadblock persists despite clear guidance from government and professional associations (CIHR, 2022a, 2022b; CNA & CFNU, 2014; RNAO, 2017). Our study identifies an important implementation gap: while the rhetoric of compassion and psychological safety is found at the policy level, it is lost in transit to the front lines. Identifying the institutional, relational, and procedural roadblocks is a necessary step towards supporting nurses’ mental health and creating and sustaining workplaces that are both compassionate and psychologically safe.
Conclusion
This study examined nurses’ experiences of mental health struggles, and the process of recognizing their own distress, navigating the invisible labour and institutional roadblocks in requesting a leave of absence, and negotiating stigma, and backlash with their return to work. This paper reports empirical findings on the role compassion played in these experiences, makes links to literature on compassionate communities and reflects on how compassion supports psychological safety in the workplace. Compassion is central to nursing practice and is associated with enhanced care and patient outcomes. However, compassion for nurses remains inconsistent, and in some cases, absent in the context of their work environments, particularly when they are struggling with their mental health. Compassion is notably absent in organizational cultures that continue to normalize nursing staff shortages and crushing workloads. Study findings highlight knowledge and policy gaps in implementing compassionate organizational processes; instead, compassion appears to be person-dependent, which translates into haphazard and micro-level implementation. Authors of this paper urge healthcare organizations to remain attentive to nurses’ experiences of mental health struggles, and to mobilize compassion as a framework to attend to the root workplace causes of nurses’ mental health struggles, and streamline workplace procedures to ensure nurses who need mental health support can access necessary care without excessive roadblocks, stigma, risks to confidentiality, and pressure to return to work before they are ready. Lastly, authors of this paper also urge organizations and policymakers to address the implementation gaps, procedural roadblocks, stigma, and backlash that study participants reported. We suggest looking to nurses as experts on compassion, seeking their input in designing psychologically safe workplaces that also serve to uphold central tenets of compassionate communities.
Footnotes
Acknowledgements
The authors are most grateful for the generosity of the nurses who participated in this study, and research assistants Chaman Akoo, Abby Ayoub, Kenchera Ingraham, Shamel Rolle Sands, and Mylene Shankland. The authors would also like to thank the two anonymous reviewers for their helpful comments.
CoI Declaration
None.
Ethical Approval and Informed Consent Statements
Research ethics approval was obtained from the University of Ottawa Office of Research, Ethics, and Integrity (S-05-19-2508). Ethics approval was also obtained from 15 institutional review boards in Canada, due to the scope of the parent study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Institute of Gender and Health, (grant number Catalyst Grant #492137).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
due to the sensitive nature of the questions asked in this study, respondents were assured that raw data would remain confidential and not be shared.