
Abstract
Background
Artificial intelligence (AI) continues to emerge into nursing practice with much of the AI research being conducted in the acute care sector. Community health nurses (CHNs) have distinct skills and knowledge focusing on helping clients to live well in the community. Community practice is an essential part of healthcare yet often overlooked, creating a knowledge gap. This research aims to understand CHNs’ knowledge and perceptions of AI to inform future practice.
Method
An explanatory sequential mixed methods design was conducted, a cross-sectional survey followed by focus groups to combine both sets of results for a comprehensive perspective.
Results
There were 228 survey respondents and 27 participants forming 8 focus groups. The survey revealed professional concerns: AI giving a wrong recommendation (77.7%) or if a correct recommendation was dismissed (73.8%) with focus groups explaining they knew their responsibility in decision-making, their concerns focused on accepting AI recommendations blindly or using recommendations to assist with decision-making. Overall CHNs felt AI applications had usefulness (68.8%-88%), the focus groups further explained clinical relevance, user friendly and time efficiency were factors that would determine usefulness.
Conclusions
Dedicated time for AI education for CHNs is needed to address how recommendations are generated and the significance to give to AI recommendations. Clear policies and guidelines need to be established to inform CHNs use of AI. Success of AI in CHNs practice is dependent on applications that do not add time to their busy schedules.
Keywords
Background and Purpose
Artificial intelligence (AI) continues to emerge into nursing practice. The common notion supporting the emergence of AI is its potential to improve healthcare (Henderson et al., 2022; Sharma et al., 2021; World Health Organisation (WHO, 2024)) in both clinical decision-making and system efficiencies (Henderson et al., 2022; Stead, 2018). AI is a broad term referring to computer systems that use algorithms to analyze data, recognize patterns, and generate predictions or recommendations that assist clinical care or health system decision-making, without being explicitly programmed for each task (WHO, 2024).
Several studies examined healthcare professionals’ reported knowledge and familiarity with AI and their perspective of artificial intelligence. The studies included nurses (Alruwaili et al., 2024; Swan, 2021), nursing students (Kwak et al., 2022), radiologists (Botwe et al., 2021; Coakley et al., 2022), physicians (Oh et al., 2019), medical students (Mehta et al., 2021), healthcare professionals inclusive of nurses (Abdullah & Fakieh, 2020; Castagno & Khalifa, 2020). These papers reported various levels of AI knowledge for nurses and other healthcare professionals such as moderate knowledge, (Abdullah & Fakieh, 2020; Alruwaili et al., 2024), fair to no knowledge (Swan, 2021), or not good familiarity with AI (Oh et al., 2019) but acknowledged that respondents understood general terms, i.e., AI rather than specific terms such as, machine learning or deep learning (Coakley et al., 2022; Mehta et al., 2021; Swan, 2021). Nurses and other healthcare professionals were willing to integrate AI into practice (Alruwaili et al., 2024; Botwe et al., 2021; Coakley et al., 2022) perceiving it would be useful (Castagno & Khalifa, 2020; Mehta et al., 2021; Oh et al., 2019; Swan, 2021). However, nurses along with other professionals had concerns about errors introduced by AI (Alruwaili et al., 2024; Botwe et al., 2021; Oh et al., 2019), privacy (Castagno & Khalifa, 2020) and ethics (Coakley et al., 2022; Mehta et al., 2021). None of these studies focused exclusively on registered nurses who practice in the community sector and their perceptions of AI in their practice setting.
Most of the AI research is conducted in hospital settings (Loftus et al., 2024; Seibert et al., 2021; von Gerich et al., 2022) yet community health nursing is different from hospital nursing. Community registered nurses are a smaller group (32,074, 16.6%) compared to hospital nurses (129,932, 67.3%) (Canadian Institute for Health Information (CIHI, 2024)). Community healthcare services are not included in Canada's universal healthcare (Martin et al., 2018) so services can vary from province to province and territories (Health Canada, 2016). Community health nurses (CHNs) are registered nurses with specialized nursing knowledge, skills and competencies (Canadian Nursing Association (CNA, n.d.)), who are employed in a variety of roles (e.g., public health, home care) and provide a range of essential services from well-baby to palliative care to help keep clients in the community (Community Health Nurses Canada (CHNC, 2019)). CHNs have more autonomy in their practice providing services to the clients in various places (e.g., homes, schools) (CHNC, 2019; dit Dariel et al., 2013; Sockolow et al., 2021 ). As well, CHNs’ clients have less nursing oversight compared to in hospital (Topaz et al., 2020). Therefore, CHNs have differences in their knowledge and skills, their practice focus, and their practice settings. These differences along with AI research more commonly occurring in hospitals creates the potential that AI may not be designed to best serve CHNs who work in community practice (Barda et al., 2020; Shang, 2021; Stead, 2018). The purpose of this study was to gain a comprehensive understanding of CHNs’ perception of AI and its potential effects on their practice. The research questions were: 1) What knowledge and perceptions do CHNs have about artificial intelligence emerging into their practice? 2) How do CHNs’ perceptions and experiences further expand our understanding of the survey results? 3) How does this inform future practice for CHNs with the emergence of AI into their practice?
Methods and Procedures
Design
An explanatory sequential mixed method design, a quantitative survey followed by a qualitative study using focus groups, was conducted to gain a comprehensive understanding of CHNs’ perceptions of AI emerging in practice, their thoughts on how they could be involved, and the importance of involvement in AI emerging into their community practice (Creswell, 2022). Each research method, quantitative and qualitative was considered equal, the strength of this approach is considering the results and findings together, to draw meta-inferences to answer the research questions (Creswell, 2022). Integration of the two methods was facilitated by connecting the samples, the qualitative sample was created from the quantitative sample, and by using the quantitative results to inform the interview guide for the focus groups to examine survey results. (Creswell & Plano Clark, 2018; Fetters et al., 2013; McCrudden & McTigue, 2019; Nowell et al., 2025; Othman et al., 2020; Younas & Durante, 2023). Ethics approval was granted by Research Ethics Board, University of Northern British Columbia for quantitative (6009080) and qualitative (6009311) phases. All data were captured, stored and analyzed on secure university servers.
The underlying philosophical assumptions addressed ontology, epistemology and axiology based on a commonly used world view, pragmatism (Creswell & Plano Clark, 2018). The research was built on the belief that nurses will hold their own knowledge (ontology) from their formal nursing education, their personal and professional experiences, learning gained by providing nursing services in their specific practice area, supporting the assumption community nurses would have multiple realities (Creswell & Plano Clark, 2018; Dolan et al., 2023) regarding perceptions of AI, community practice and how to be better involved. The next assumption, epistemology, focused on how we could capture the nurses’ knowledge and perceptions to answer the research questions. Thereby using quantitative and qualitative methods offered two ways to address the research questions (Creswell & Plano Clark, 2018). The qualitative method used Thorne's (2016) interpretive description, a clinical approach, to expand practice knowledge (i.e., CHNs’ perceptions of AI) and is considered congruent with pragmatism (Dolan et al., 2023). The explanatory sequential method chosen used the quantitative phase to describe ‘what’ the baseline of the nurses’ knowledge and perceptions of AI were, and the qualitative phase to help understand ‘why’ and possible solutions (Creswell & Plano Clark, 2018). The key elements for integration were connecting and then explaining (Creswell & Plano Clark, 2018; Fetters et al., 2013). Joint displays were used to visualize the results to determine meta-inferences to further explain the research questions (Creswell & Plano Clark, 2018; Fetters et al., 2013; Guetterman et al., 2015; Younas & Durante, 2023).
Specific description of methods and results are presented in the order the research was completed. The quantitative phase has been published (Henderson Betkus et al., 2026).
Quantitative Phase. National Cross-Sectional Survey
Survey Tool for Data Collection
A cross-sectional online survey was used for data collection. It was developed by using an existing survey that was purposively designed for nurses, with permission (email Beth Ann Swan, November 30, 2022), as the core structure. It was further adapted for a Canadian audience, specifically CHNs. Some additional questions were added or adapted from other existing published surveys (Esmaeilzadeh, 2020; Schepman & Rodway, 2020) or crafted by the first author to address pertinent areas for community practice. The adapted survey was not piloted; it was reviewed for content and clarity by a retired Canadian public health nursing manager who had 35 plus years’ experience in public health nursing both in direct care and in management. The English only survey (Supplemental file) was recreated to an online format using SurveyMonkey (SurveyMonkey, 2023).
Survey Recruiting Participants
National nursing organizations (e.g., Canadian Nursing Informatics Association, Community Health Nurses Canada) and individual provincial and territorial nursing associations or licensing colleges were approached to circulate invitations containing an embedded survey link. The invitations were extended by these third-party entities through email or routinely presented (e.g., monthly) to their members by broadcast message, newsletters, or social media throughout the survey period. The online survey included a cover letter providing the information for the informed consent. The inclusion criteria specified that participants had to be registered nurses licenced in Canada, providing community care, either direct care (e.g., public health, home health) or at some other level with a focus on community care (e.g., management, researcher, educator). If respondents satisfied the inclusion criteria, they could move to providing consent and access to the survey. Prior to signing off, respondents were asked to indicate their interest in further research by supplying their email address. The survey was live from April 24 to July 30, 2023.
Survey Data Analysis
The survey data were transferred to IBM SPSS Statistics (Version 29). Both descriptive and inferential statistics were used. The Chi-square test of independence was used to determine an association between the nurses’ reported knowledge of AI and their perceptions of the effects of AI (Pallant, 2020). Their reported level of knowledge was grouped as ‘good’ or ‘not good’ AI knowledge.
Qualitative Phase. Focus Groups
Focus Groups Recruiting Participants
The defining criteria for purposive was the previous participation in the survey to maintain an explanatory sequential design. The sample was created from a subset of survey respondents who had indicated interest in further research by providing their email address. These respondents were sent an enquiry email with one follow up email to determine if they were still interested in participating in the qualitative phase. Each respondent that returned an affirmative reply received a formal invitation with an informed consent form, with dates and times for the Zoom meetings (Zoom, 2023). Potential participants were limited by their availability for date and time of the focus groups.
Focus Groups Data Collection
One-hour focus groups were conducted from November 15-21, 2023, over Zoom communications (Zoom, 2023) using record and transcribe functions. A semi-structured interview format (Supplemental file) guided the discussions led by first author.
Focus Groups Data Analysis
Interpretive description was used to interpret and discuss the findings in the qualitative phase of this study because of its applied approach to expanding knowledge (Thorne, 2016). The organization of the data used thematic analysis following the 6-step process established by Braun and Clarke's (2006), with Naeem et al. (2023) used as part of the iterative process to reconsider or verify the process by identifying keywords and potential themes. The familiarization process and ongoing coding was initiated by the first author with reviewing, correcting the audio to text transcriptions and using both Excel spread sheets (Naeem et al., 2023) and NVivo (Version 14) to help visualize and delve into the conversations. The iterative process continued reviewing the experiences of the focus groups, coding their experiences to reflect their perceptions which were grouped into themes and subthemes.
Focus Groups Rigour
All authors directed and guided the research process promoting rigor throughout the research process (Lorenzini et al., 2024) beginning with choosing the method to best address the research. There was constant awareness of researcher bias. The first author as coder recognized that her community nursing experience could affect beliefs, and impose bias, and values that could affect interpretation of the data of the focus groups (Polit & Beck, 2017; Renjith et al., 2021) to mitigate this, journaling and reflective notes (Polit & Beck, 2017) were used throughout the analysis of the transcripts and meetings with all authors. A member check (N = 5) was completed following McKim's (2023) process to gain insights from the participants to ensure their perceptions and experiences had been captured accurately. The integration of the data were jointly displayed to allow readers to evaluate the meta-inferences (Creswell & Plano Clark, 2018; Younas et al., 2023).
Integration Phase
Integration Matrix for Data Display
Integration connected the quantitative results with the qualitative findings, displaying the results and findings in a matrix to provide a visual link to further explaining the survey results (Creswell & Plano Clark, 2018; Guetterman et al., 2015; Younas & Durante, 2023). The quantitative findings formed the basis for examining the qualitative data with four main areas of focus: Attitudes toward AI, Utility of AI, Effects on professional practice, and Professional accountability. Based on these areas, the qualitative data were analysed for themes and sub-themes to capture CHNs’ perspectives related to these broader areas. The meta-inferences were developed by reviewing the integration of the quantitative and qualitative data and rethinking the nuances to gain plausible insights (Creswell & Plano Clark, 2018; Younas et al., 2023).
Results
There were 228 useable surveys (five blank surveys removed), and eight focus groups included 27 participants, five of whom also participated in the member check. The overarching concept of integration was implicit in the decision to use an explanatory sequential mixed method research design to answer the research questions. The sample characteristics provided an obvious integration point to describe both samples. The quantitative results followed by the qualitative results are reported separately. The integration of the results is jointly displayed with the meta-inferences.
Sample Characteristics of the Quantitative and Qualitative Research
The focus group sample created from the survey respondents, was a younger cohort (15/27, 55.6%) under 40 years compared to the survey group (68/178, 38.2%) sample (Table 1). The main differences were seen in the age categories of 30–39 years and 50–59 years. The focus group participants had a larger representation of younger CHNs 30–39 years (13/27, 48.1%) and a smaller representation for the 50–59 years category (2/27, 7.4%). Both groups of CHNs had similar levels of experience. Most had greater than five years RN experience, survey respondents (161/179, 89.9%) and focus group participants (24/27, 88.9%) and CHN experience for the survey respondents was (129/176, 73.3%) and the focus group participants (19/27, 70.4%). The focus group sample represented most regions of Canada except Northern Canada which had a low representation in the survey sample.
Survey and Focus Group Comparison of Age Category, Sex, and Region of Canada.
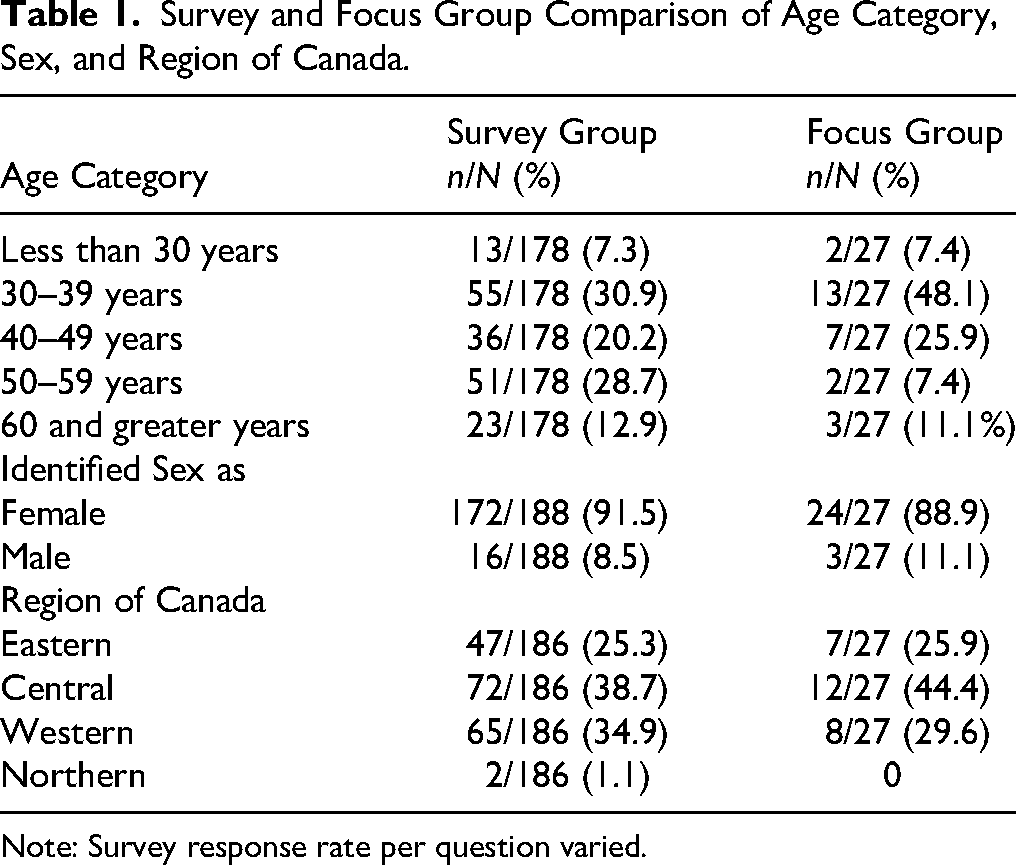
Note: Survey response rate per question varied.
Quantitative Phase
Quantitative Results
The 228 useable surveys had varying response rates per question. AI content questions had higher response rates compared to the demographic questions that were situated at the end of the survey.
Attitudes and Perceptions Towards Technology, Their Skills and Knowledge
Most CHNs described themselves as welcoming technology into their practice (205/228, 89.9%) and most identified themselves as either competent users of the internet and standard applications (129/227, 56.8%) or users of specialist applications (83/227, 36.6%). The predominant sources of knowledge (Figure 1) for common forms of AI (i.e., speech text, spam, recommendation algorithms) were informal sources such as media or social media and family and friends. A few CHNs were unaware that these applications were AI driven ranging from 12.7% (28/221) for recommendation algorithms to 14% (31/221) for speech text.
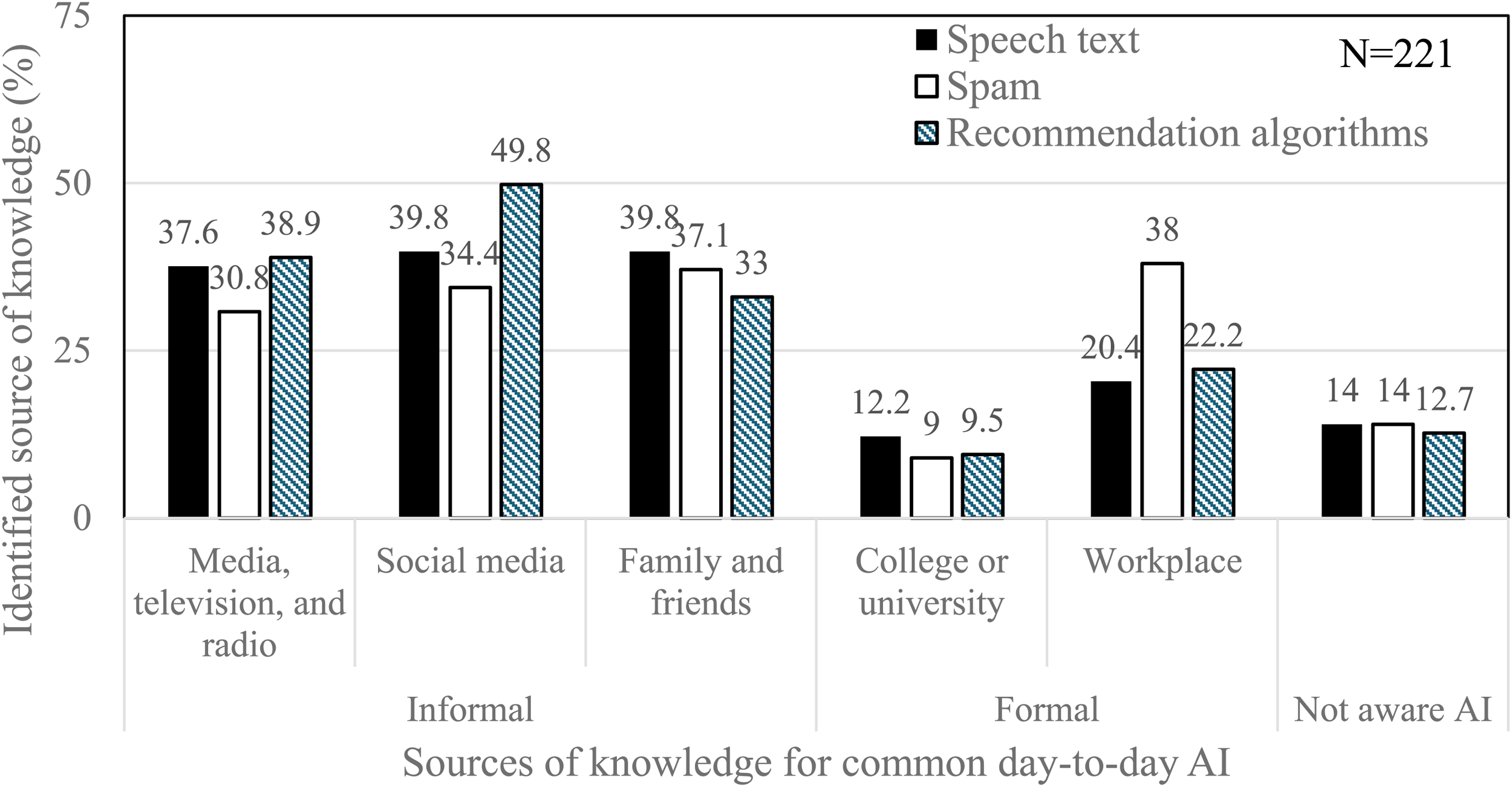
Survey group identification of knowledge sources of common artificial intelligence.
The CHNs rated their knowledge of AI from none to excellent; ‘none’ (42/220, 19.1%), ‘fair’ (83/220, 37.7%), ‘good’ (67/220, 30.5%), ‘very good’ (23/220, 10.5%), ‘excellent’ (5/220. 2.3%). This was presented as ‘good’ AI knowledge by grouping together ‘good’ to ‘excellent’ (95/220, 43.2%) and ‘not good’ AI knowledge by grouping ‘fair’ and ‘none’ (125/220, 56.8%). These two groups were used to determine if there was an association between the CHNs’ reported level of AI knowledge and their perceptions and attitudes.
Perception About the Effects of Artificial Intelligence on Practice with Level of Artificial Intelligence Knowledge
Chi-squared test for independence indicated a significant association between CHNs with ‘not good’ AI knowledge and feeling uncomfortable with AI development (χ2(1) = 4.2, P = .04, α = .05, small effect φ = .15). These CHNs were almost twice as likely (Odds Ratio [OR] 1.84, 95% CI 1.03–3.3) to indicate that AI development made them feel uncomfortable. CHNs with ‘good’ AI knowledge where more than twice as likely to consider that AI is part of nursing (χ2(1) =6.6, P = .01, α = .05, Φ= .18, OR 2.1, 95% CI 1.19–3.68), feel AI will revolutionize nursing (χ2(1) =7.3, P = .007, α = .05, Φ = .19, OR 2.28, 95% CI 1.25–4.18), and were excited about the future of AI in nursing (χ2(1) = 10.1, P = .001, α = .05, Φ = .22, OR 2.52, 95% CI 1.42–4.47) and healthcare (χ2(1) = 8.3, P = .004, α = .05, Φ = .20, OR 2.3, 95% CI 1.30–4.06).
Regardless of their AI knowledge, very few CHNs had concerns that they would be replaced (21/205, 10.2%) by an AI nurse. However, they agreed that AI should be part of nursing education (143/203, 70.4%) and professional development (152/202, 75.2%). They expressed their interest in being involved by being consulted (195/203, 96.1%) and raising nurse relevant questions (189/202, 93.6%).
Perception About the Utility of Artificial Intelligence Applications and Level of Artificial Intelligence Knowledge
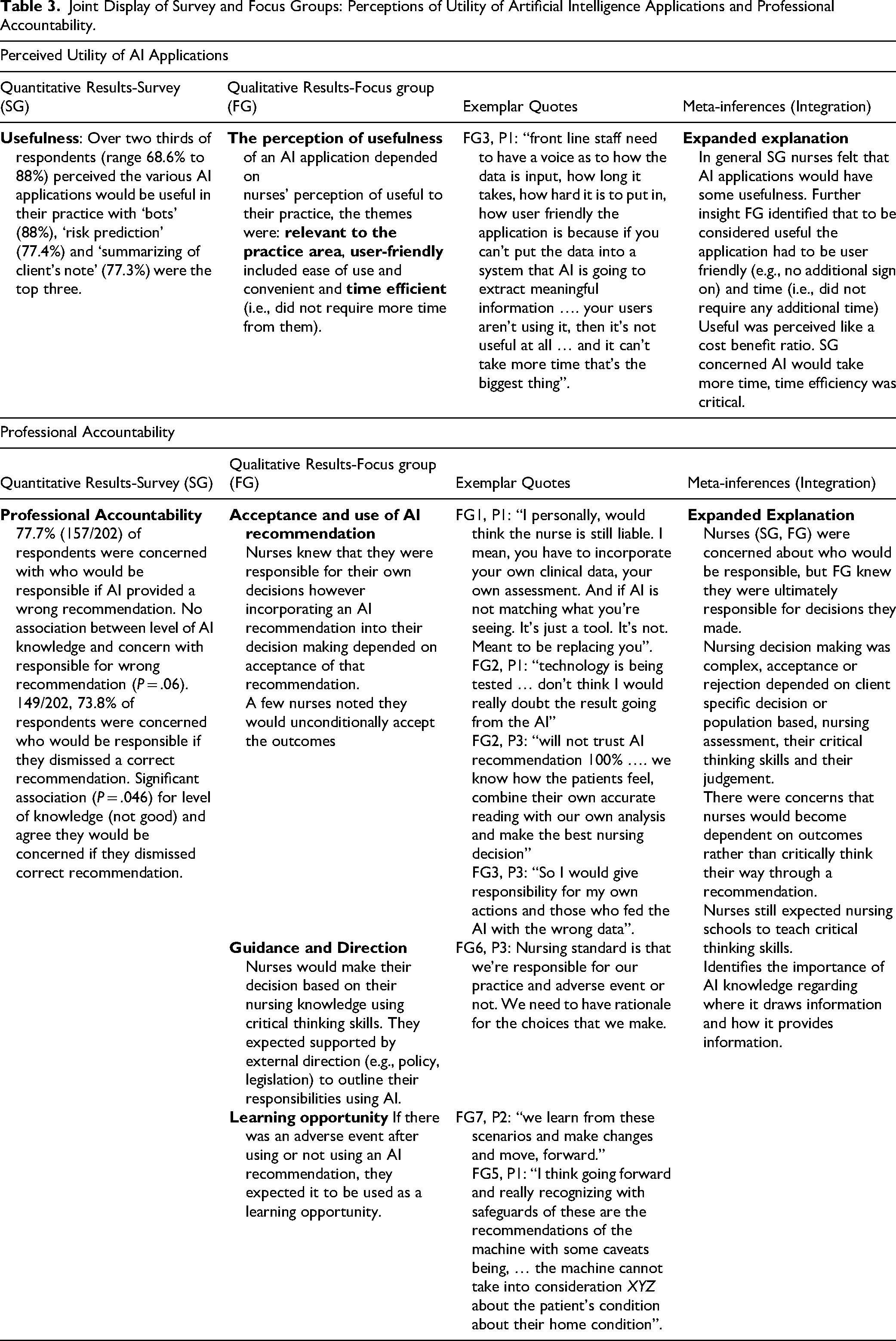
One application, transition management, had a significant association (χ2(1) = 7.9, P = .005, α = .05, Φ = .20, OR 2.45, 95% CI 1.30–4.63) between perceived usefulness and good AI knowledge. For the remaining AI applications there was no association between perceived usefulness and level of AI knowledge. In general, the CHNs perceived each AI application would be useful with their agreement ranging from 68.6% (142/207) to 88.0% (183/208). The most frequently selected as useful were ‘Bots’ (183/208, 88%), risk prediction (161/208, 77.4%), and summarizing of client's notes (160/207, 77.3%) (Figure 2).
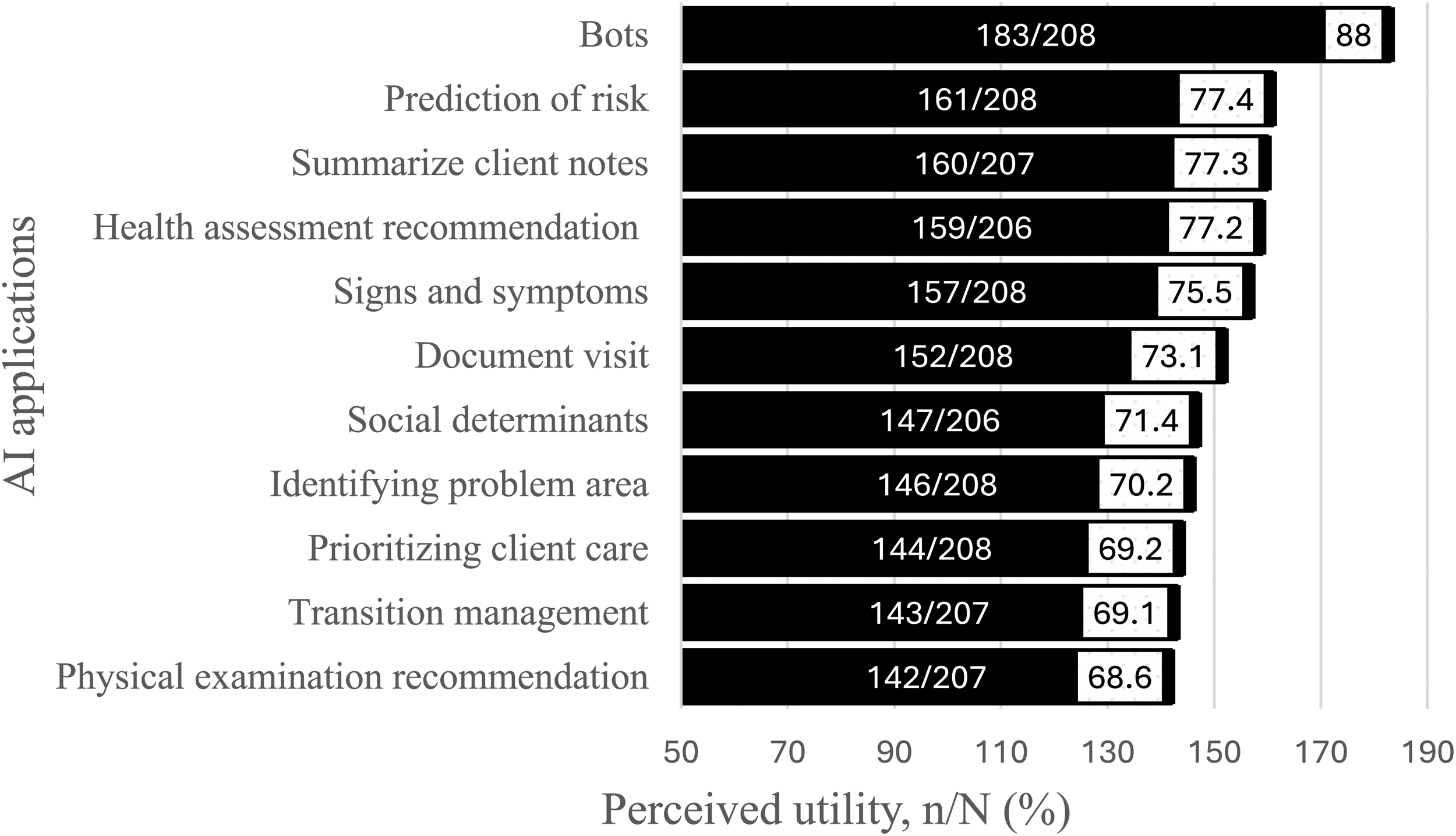
Survey group agreement of usefulness of artificial intelligence applications.
Perception of Their Professional Accountability and Level of Artificial Intelligence Knowledge
Professional accountability had varied results. Many CHNs were concerned about their accountability if AI provided a wrong recommendation (157/202, 77.7%) or if they dismissed a correct recommendation (149/202, 73.8%). There was no significant association (P = .06) between level of AI knowledge and concern for AI offering a wrong recommendation. However, there was a significant association (P = .046) between not good AI knowledge and concern if correct recommendation was dismissed (χ2(1) = 3.98, α = .05, Φ = .14, OR 1.9, 95% CI 1.01–3.57).
Qualitative Phase
Perceptions of Effects of Artificial Intelligence on Community Nursing Practice
Comfort with Artificial Intelligence Development
The CHNs provided insights on their comfort with AI development and potential use in their practice. The focus group participants exhibited guarded optimism of AI in their practice. None of the participants were resistive to the idea of AI in their practice. Their concerns were practical and appropriate which included client's privacy and the importance of safeguards against “cyber invasion [and] is AI going to open the door to that a bit more” (FG 6, P3). One participant admitted that hearing online “about deep fakes and things like that … make you a little bit concerned” (FG 1, P1). Another admitted “we just hear about technologies … we don’t even know …how we should use [them]” (FG 3, P2). One nurse indicated that “nurses will be receptive to it [AI]” (FG2, P2). Others identified strategies on how nurses would become more comfortable by “staying updated on the AI application … [and] enhance my own AI literacy” (FG1, P2), and knowing more about how AI works, pulls it data and “having some reasoning behind it” (FG1, P1).
Replace Human Nurse
Few references were made about human nurses being replaced by AI. Focus group conversations were more about extending nurses’ care and services rather than replace the human nurse. Nurses could envision how AI-driven technologies could support or improve care. Nurses felt that AI could be useful in orientation education for inexperienced nurses (e.g., walk nurses through practice scenarios) as “less shadowing and mentorship opportunities [exist]” (FG5, P1). Chatbots were identified as a method to support nursing service. One nurse described the use of chatbots to extend their service and care by answering clients’ health questions with the option of speaking to a human nurse. Another nurse shared they were exploring chatbots as a method to manage administrative tasks, e.g., using chatbots to automate online booking systems (FG4, P1). However, they also observed this had the potential to reduce positions due to funding and cutbacks “if government [can] find a way to use AI to eliminate positions they will” (FG4, P1).
More Exciting
Excitement or interest in AI was tempered with practical reservation. One nurse “my initial thoughts, were kind of a mix of curiosity and excitement …and the need then for responsible developments and the usage.” (FG1, P2). Another admitted to looking forward to AI perceiving the benefits but had concerns with “reliability of it and, the security …[and] implementation of it … a lot of considerations … when bringing something like AI in. But I do think there would be benefit too” (FG2, P2). Another stated “we’re excited about the possibilities of serving our clients better, serving our community better … new ways of doing things and that would be more effective and efficient” (FG4, P3). One acknowledged excitement for QR scanners being introduced for scanning vaccine vials at clinics but was not excited “about how that might look like on offsite programs … may or may not have to lug all this stuff” (FG7, P2).
Artificial Intelligence is Part of Nursing
Generally, direct experience with AI in their practice was minimal but could vary. There was acknowledgement that AI driven applications were being introduced or had been introduced into their practice (e.g., chatbots, QR scanners). The discussions revealed that devices or applications which are AI driven (e.g., email to fax, interpreter systems) were being used although the nurses did not identify them as AI. One nurse described how they would distinguish between the credibility of AI applications considering ones in the EMR would be more clinical because it had access to client information versus using ChatGPT to write a letter or asking Siri how much Tylenol. CHNs wanted guidance. One nurse had raised questions about “publicly available Chat GPTs … [but] … not getting many answers” (FG4, P3). However, member check (16 months after focus groups) revealed more AI driven applications had become part of their practice (e.g., co-pilot, Grammarly, Claude) some sanctioned by their worksites but not authorized by regulatory bodies. It was recognized that for publicly accessible AI applications CHNs needed the knowledge to identify inaccuracies in the information produced. One nurse described using AI to develop a client letter and concluded that was the “only time that I've used AI that I know of in practice” (FG8, P5). This was suggestive that CHNs may not be aware whether devices and applications are AI driven.
Education and Training
CHNs felt that AI education should be included in the nursing curriculum and ongoing professional development. A common perception was that nursing assessment skills, critical thinking and AI technologies should be taught together. This was further explained there will be a need for “fostering critical thinking skills to evaluate the AI generated information” (FG1, P2). Another stated, “your clinical skills are going to be overall what's most important and just incorporating the machine data or the AI data into your own clinical skills” (FG1, P1). Yet another nurse identified the importance of depending on nursing skills, knowledge and judgement because of the downtime that can occur with technology emphasizing [paper] “forms aren’t going to have pop ups or prompt for a lot of these things” (FG6, P1). CHNs expected to have dedicated time for ongoing AI education and training and recognized this support would have to come from management and or executive directors.
Involvement
CHNs felt strongly about being involved in AI that had some impact on their practice. CHNs had relevant issues that they thought AI could address, some were client specific (i.e., best interventions based on client's data, or predictions of health risks), others were system related (i.e., prioritizing caseload). One nurse identified the concern that CHNs would not “be given much choice in terms of what type of AI would be used” (FG2, P2). Another identified the negative impact when CHNs were not involved, i.e., “there's lots of tools out there that are just not user friendly because they haven’t asked the people who are going to be using them” (FG8, P5). CHNs felt that there needed to be recognition that CHNs had to be involved which started at high level leadership. One expressed “our nursing bodies that do … advocacy need to be at that high level table to be able to influence the nursing position and involved in these decision making … moments” (FG6, P3).
Usefulness of Artificial Intelligence Applications
CHNs perceived that AI applications would be useful to them. Further discussion by the groups revealed there were more tangible aspects that influenced whether a nurse felt an AI application would be useful or not. The practical aspects CHNs considered were the relevancy to their practice area, whether it was easy to use and efficient timewise, i.e., it could not take any more time. User friendly features were no “additional sign on” (FG8, P1), all “levels of computer experience” (FG8, P5) could use it, and it facilitated ease of inputting data. Time is considered separately even though it could be considered another user-friendly trait, but CHNs were adamant about the AI application not taking any more of their nursing time, therefore it was identified as stand-alone criteria. One participant described that you could think of a feature that might be “useful but once you actually get it in the real world … [it] just slows you down or trips you up in your assessment” (FG6, P1) suggestive that AI may not be time efficient.
Professional Accountability
The CHNs revealed their perceptions on acceptance and use of AI recommendations in their clinical decision making. They addressed their expectations on the guidance and direction they felt they would need to incorporate AI into practice, specifically in decision making. They voiced they wanted any untoward event associated with AI to be treated like a learning opportunity.
Acceptance and use of Artificial Intelligence Recommendations
The focus group participants’ perceptions of AI affected how they thought about their professional accountability. CHNs knew that they were responsible for their own decisions. However, the concept of concern about who would be held responsible for following or not following a correct recommendation or inadvertently accepting an incorrect AI recommendation was complex. Their discussions revealed the various aspects they would consider if they were incorporating an AI recommendation into their decision making. These aspects were different depending on whether they considered it a client specific recommendation or a more general population-based recommendation. One nurse felt that AI developed for trending would be reliable to follow recommendations. Whereas, when considering a client specific recommendations, several CHNs felt they would need to use their basic nursing assessment skills, critical thinking and nursing knowledge. One stated “… there might be things that we can’t put into that program … more subjective … not data points that make the picture different than what the AI can see”. (FG3, P1). CHNs perceived AI as a tool like a decision support tool with the belief that AI recommendations should be “developed to the same standard” (FG6, P1) of accuracy as decision support tools. Most CHNs felt it was important for CHNs to be able to justify their clinical rationale. One participant had concerns about is it “just gonna take my autonomy in decision making away” (FG6, P3) or becoming reliant on AI recommendations “concerned … that I would use AI as a bit of a crutch” (FG6, P3).
Some held different perceptions. A few CHNs were willing to accept the AI recommendations because they believed the AI application and its outcomes would have been tested before it was introduced into their practice. One said they would feel guilty if they did not follow the recommendations and suggested that perhaps a nurse would ignore a recommendation if “they [had] no information, or they lack[ed] the knowledge about what it entails” (FG3, P2). Another felt that an incorrect recommendation may occur because of competing AI developers or data needing to be updated. Yet another nurse felt the responsibility would be shared between the nurse and the AI developer.
Guidance and Direction
Focus group participants expected they would have formal direction to guide them in how they would go about incorporated AI recommendations into their practice in the form of decision support tools (DST), practice policies or guidelines as well as, direction from formal entities (e.g., licensing colleges and associations, unions, Canadian Nurses Protective Society, legislation). This returned to the assumption that CHNs would make their decision based on their nursing knowledge using their critical thinking skills. The CHNs concluded that AI should be recognized “as part of a decision-making framework … that it's going to become another part of the suite of tools that we go to make decisions” (FG7, P1) and the importance of charting “about why I did or did not do those things” (FG6, P1). Ultimately, CHNs would have to know whether following AI recommendations were procedure or policy recognizing “there's must do's and then there's gray areas … that's open to discretion and interpretation” (FG7, P2).
Learning Opportunity
Focus group participants indicated that if there was an adverse event after using or not using an AI recommendation, they expected it to be handled as a learning opportunity. CHNs were familiar with procedures that existed to follow up on adverse events, “we always have to go back and investigate it”. (FG5, P2). This included looking at extraneous factors and why a “nurse [made] a decision that was different than what was offered by AI. We want to look at what was the client's presentation” (FG5, P2). There was recognition that the adverse event may not be related to following or not following the AI recommendations, “maybe the situation wouldn’t have been better if we had followed the advice of AI.” (FG5, P2) and “it may or may not have happened in the absence or presence of AI” (FG7, P1). Participants agreed that these events should be used as learning opportunities “… we learn from these scenarios and make changes and move, forward” (FG7, P2). In discussing adverse events one participant acknowledged the importance of “… more training and inclusion of nurses in … developing those AIs that we should be included”. (FG5, P3). Finally, accepting that AI may not consider all factors: “I think going forward and really recognizing with safeguards of these are the recommendations of the machine with some caveats being, you know, the machine cannot take into consideration XYZ about the patient's condition about their home condition.” (FG5, P1)
Integration Phase–Quantitative and Qualitative Results: Meta-Inferences
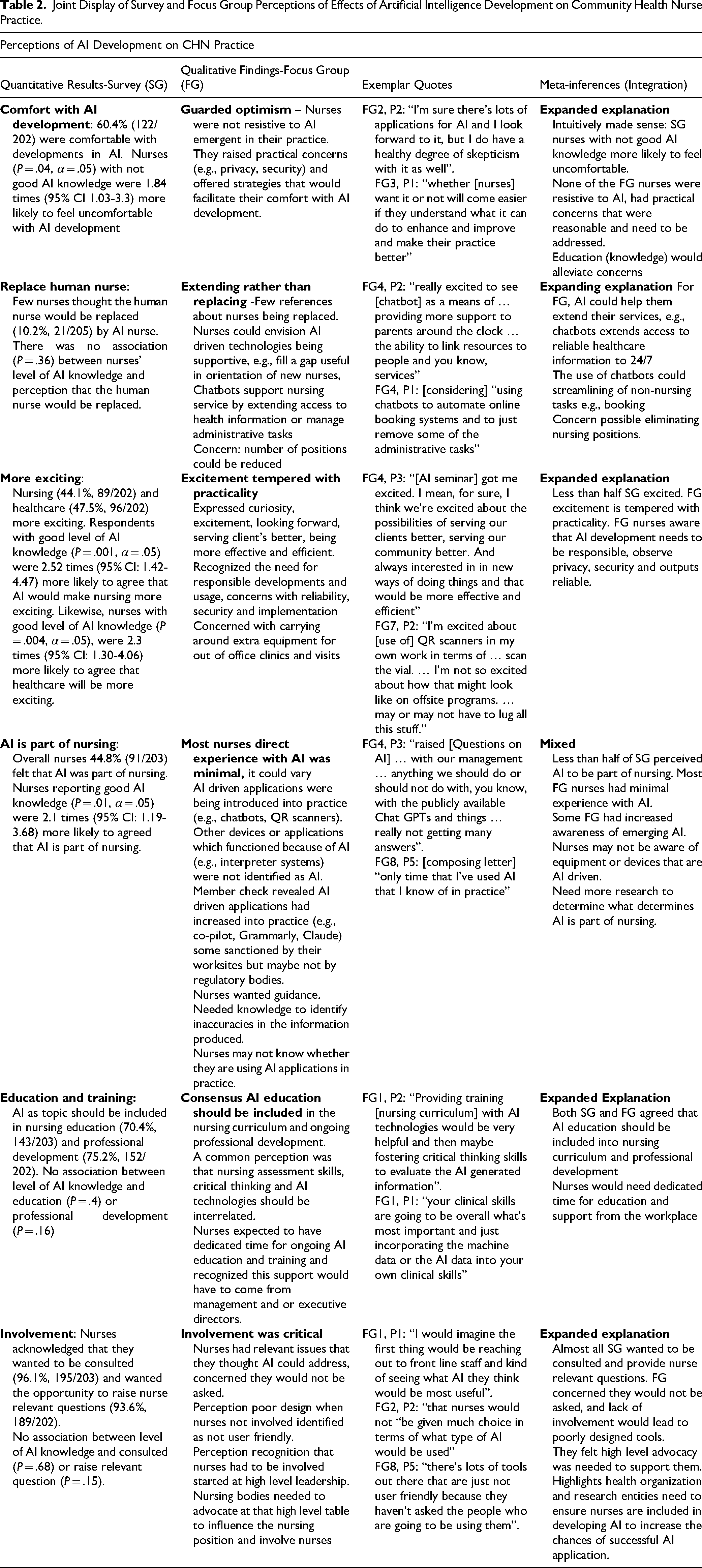
The joint display assisted in determining the meta-inferences by expanding the explanation of the survey results in most cases. The survey item that AI is part of nursing provided mixed information. (Tables 2 and 3).
Joint Display of Survey and Focus Group Perceptions of Effects of Artificial Intelligence Development on Community Health Nurse Practice.
Joint Display of Survey and Focus Groups: Perceptions of Utility of Artificial Intelligence Applications and Professional Accountability.
Discussion
The sample characteristics of the CHNs in the focus group and the survey group mirrored each other except for age. The CHNs were younger in the focus group with the potential to be continuing in the CHN workforce for another 20 years or more. It is possible that the younger age group benefited this study because nurses who are in their 40s likely grew up with computers and appear to be highly motivated. This factor underscores the importance of learning from their perspectives on AI and how they can be better involved.
Perceptions of Effects of Artificial Intelligence on Community Nursing Practice
Both comfort with AI development and feeling excited about AI delved into the nurses’ emotions. CHNs in the survey group who reported ‘good’ AI knowledge tended to feel more favourable with aspects of AI. Examining comfort with AI development from the survey provided two perspectives 1) regardless of their AI knowledge almost two thirds of the survey respondents were comfortable with the development of AI into their practice 2) respondents reporting ‘not good’ AI knowledge were almost twice as likely to feel uncomfortable about the development of AI in their practice. Clinically, not having a good understanding of AI, could raise your concerns making a person uncomfortable (Schiavo et al., 2024). The focus group participants revealed they had a guarded optimism towards AI as no one voiced resistance to the idea of AI emerging into their practice, aligning with Rony et al. (2024). Even though focus group participants felt that CHNs would be receptive, they identified a need to better understand AI (e.g., know more about how AI works, where it pulls its data) which would address both issues, knowledge and comfort (Huo et al., 2023).
Likewise, the survey responses to ‘nursing and healthcare will be more exciting’ produced two overarching results. Irrespective of AI knowledge, under half of the survey respondents perceived that nursing and healthcare will be more exciting. Again, it was the survey respondents with ‘good’ AI knowledge who were twice as likely to agree that nursing and healthcare would be more exciting. The focus group participants described excitement tempered with practicality. Focus group participants perceived that there would be benefits with AI but were aware that there were practical concerns that needed to be addressed such as privacy and security for clients and reliable outcomes for care decisions (ICN, 2023). They recognized devices that could help them (e.g., QR scanners) but the extra equipment they would have to carry might be problematic (ICN, 2023). The focus group participants’ results expanded our understanding of what practical issues may limit nurses’ excitement and the practical information nurses want, e.g., reliability of outputs, how to ensure privacy and security of their client.
Replacement of human nurse for an AI nurse was not top of mind for either group. Regardless of level of AI knowledge few (10%) survey respondents felt the human nurse would be replaced by an AI nurse similar to findings by Castagno & Khalifa, 2020; Mehta et al., 2021; Swan, 2021. The focus group participants described AI as extending rather than replacing the human nurse (Buch et al., 2018; Mohanasundari et al., 2023). Focus group participants also recognized some benefits that AI could help them extend their services, e.g., chatbots providing 24/7 access to reliable healthcare information or chatbots reducing or managing some non-nursing tasks which might free up nursing time. As well, focus group participants suggested that AI could fill a gap, e.g., lack of nurse mentors in orientation of inexperienced nurses by providing examples and guiding them through learning scenarios. This aligned with other opinions that AI complements (Booth et al., 2021; Mohanasundari et al., 2023), or redefines positions (Jha & Topol, 2016), or supports (Buch et al., 2018) rather than replaces experts. One focus group participant voiced concern that maybe AI could be used to reduce nursing positions if funding became an issue. However, AI cannot provide emotional qualities of nursing (e.g., empathy) (Buch et al., 2018; Mohanasundari et al., 2023). The focus groups corroborated the survey that few nurses were concerned with being replaced by AI.
The survey respondents’ perceptions that ‘AI is part of nursing’ revealed regardless of AI knowledge less than half agreed that AI was part of nursing practice. However, survey respondents with ‘good’ AI knowledge were twice as likely to agree that AI was part of nursing practice. The focus group participants revealed that most nurses had minimal experience with AI in their practice, but a few had more experience. Even though nurse leadership has been promoting the use of digital health technology inclusive of AI driven applications and advocating for end-users to be involved in AI (Booth et al., 2021; Canadian Nurses Association (CNA, 2024); ICN, 2023; Ronquillo et al., 2021) our findings were mixed, suggesting that nurses may be unaware of whether some of the devices or applications within their practice are AI driven (Canada Health Infoway, 2024; Coakley et al., 2022). Further research will be needed to better understand how nurses interpret AI is considered part of nursing.
Ongoing education and involving nurses in AI development have been recommended by professional organizations (Ronquillo et al., 2021; CNA, 2024; ICN, 2023). The survey results supported that most nurses felt AI education should be included in nursing. The focus groups confirmed that AI should be included in the nursing curriculum and ongoing professional development. The focus group participants further provided support that nursing assessment skills and critical thinking will always be needed in nursing along with the introduction of AI technologies. This logic was supported by the practical observation that with technology downtime paper forms did not have pop up prompts. Focus group participants were also in agreement that they would need dedicated time and support from their managers and executive directors to participate in AI education (Booth et al., 2021; Ronquillo et al., 2021; Rony et al., 2024; Rony et al., 2024).
Involvement in AI that could influence their practice was important to the CHNs. The survey results indicated that most CHNs wanted to be consulted and to raise nurse relevant questions. The focus group participants confirmed that nurses felt strongly about being involved if the AI would influence their practice. CHNs were aware of negative impacts when nurses were not involved (e.g., poorly designed tools). However, focus group participants felt they would not be asked to participate unless there was advocacy at a high level supporting them to be involved. Many benefits are suggested when including nurses (e.g., end-user) in AI development such as identifying and explaining user needs (Cooper, 2024; van Houwelingen et al., 2024), ensuring AI fits into their workflow (Ronquillo et al., 2021; van Houwelingen et al., 2024) and increased acceptance of AI (Huo et al., 2023), all factors key to improving the chance of a successful AI product (Cooper, 2024).
Perceptions of Usefulness
Many survey respondents perceived that AI applications would be useful in their practice aligning with perceptions of usefulness found by other AI researchers (Castagno & Khalifa, 2020; Oh et al., 2019). The focus groups expanded on criteria to determine usefulness identifying AI needed to be relevant to their practice area, user-friendly (ease of use and convenient) and time efficient (i.e., did not require more time from them). User-friendly was a commonly documented criterion (Sharma et al., 2021; Westenberger et al., 2022). However, our study revealed CHNs were concerned AI would add a burden (i.e., time) to their workload. CHNs wanted AI in their practice to be time efficient, not add to their workload. A general reason for AI applications to fail was broadly termed, lack of understanding what the user needs because end-users are usually not involved in AI development (Cooper, 2024). Therefore, time efficiency would be an important criterion for AI researchers and developers to know and have a broader understanding of why CHNs perceived AI could add time to community practice and nursing workflow.
Perceptions of Professional Accountability
Some results varied in relationship to level of AI knowledge and professional accountability. CHNs with ‘not good’ AI knowledge had concerns if they dismissed a correct recommendation (P = .046). No other association existed. However, when considering clinical importance, the majority of CHNs expressed concerns for both scenarios: if they dismissed a correct recommendation and if AI provided a wrong recommendation. Similarly, physicians (Oh et al., 2019) felt that they would be held accountable if they followed an AI recommendation that caused harm. The CHNs in the focus group knew they were responsible for the clinical decisions they made (Almost, 2021; CNA, 2015; Roberts, 2019). The qualitative results provided three themes that added to our understanding: acceptance and use of AI recommendations, guidance and direction, and learning opportunity, which helped to understand how CHNs worked through these scenarios and their expectations of how they should be supported.
CHN decision making was complex. Acceptance or rejection of a recommendation depended on whether the CHN was considering a client specific or population-based decision, what their nursing assessment was indicating, and whether their critical thinking skills combined with their judgement of the situation aligned with the recommendation. A few focus group participants felt that AI recommendations should be followed unconditionally because of their belief that testing prior to implementing AI would be sufficient. These descriptions suggested that focus group participants were not sure what level of AI autonomy (i.e., total acceptance to assistive only) they should assign to AI applications (Island Health, 2024; Morelli, 2025; National Academy of Medicine (NAM, 2025)). Related to this was the fear of losing their autonomy and the fear of becoming reliant on AI (e.g., using it as a crutch) or reliance bias (Morelli, 2025). Focus group participants were familiar with the process for adverse events used as a learning opportunity for the organization and for the CHN (Provincial Patient Safety, 2024). They expected the same format to be continued for any issues arising from AI recommendations aligning with the ‘learning health care system’ (Forcier et al., 2019).
Combining the survey group and the focus group results confirmed that CHNs have concerns about their professional accountability. Various methods could be used to alleviate their professional concerns which would also address their comfort with AI. First, including CHNs in AI development would improve their understanding of how AI recommendations are generated, what data are used, building confidence and rationale for accepting or not accepting AI recommendations (Guthrie et al., 2021; Huo et al., 2023; ICN, 2023; Sinn et al., 2017). CHNs in both the survey and focus groups in this research expressed willingness to participate in advising and consulting for practice related AI. Second, establishing ongoing AI education would address knowledge gaps, i.e., types and functions of AI, bias, ethical concerns and limits to AI autonomy would help to lessen nurses’ concerns (ICN, 2023; Morelli, 2025; Ronquillo et al., 2021: Rony et al., 2023). Third, a planned comprehensive implementation of AI into nursing practice should examine regulations governing AI, ethics, and develop clear policies and guidelines providing a framework to help nurses assimilate AI into practice (Booth et al., 2021; Forcier et al., 2019; Van Der et al., 2023; Island Health, 2024). Policy and guidelines need to discuss the concepts of level of AI autonomy and related professional responsibility (Botwe et al., 2021), including the process to follow to protect the client and the CHNs if human and AI decisions differ (WHO, 2024). These pertinent concepts could be incorporated into nursing education and professional development to support professional accountability.
Strengths and Limitations
Both strengths and limitations are acknowledged. The use of a mixed methods design provided a comprehensive understanding of CHNs’ perceptions of AI emerging into their practice. As far as we know this is the first Canadian study using an explanatory sequential mixed method research design to examine the perceptions of CHNs and AI. National coverage was achieved from a regional perspective. Some factors would caution generalizability: lack of identified representation from Prince Edward Island, Saskatchewan, and Northwest Territories; the survey was in English which limited participation of Francophone nurses; and even with practising reflexivity there was potential for bias in interpreted the findings. Overall, the research provides a foundation for subsequent studies to support CHNs with emerging AI.
Conclusion
CHNs with good AI knowledge, had more favourable views of the implications of AI on practice. They perceived that AI would make nursing and healthcare more exciting, revolutionize nursing practice and were more likely to be comfortable with AI development. CHNs provided further understanding of their practical concerns (e.g., the need for privacy, security, reliability) as well as what would make them excited about AI (e.g., new ways to do things, better serve clients). In general, they perceived AI applications would be useful, but an AI application could not add more time to their busy schedules. They had concerns about their professional responsibility and the use of AI in their decision making regarding the level of autonomy to give AI and whether they might become reliant on AI recommendations. CHNs voiced practical concerns regarding the implications of AI on their practice.
The CHNs’ concerns highlighted the importance of future directions to address solutions that support them in their practice. Solutions identified by the CHNs focused on including them in the development of AI application for their practice, appropriate AI education that addressed their concerns, and development of clear policy and guidelines on using AI in nursing that can support them in their practice. Nurses recognized nursing institutions and workplaces should ensure that AI as a topic is included in nursing curriculum and ongoing professional development. The inclusion of CHNs, specifically end-users would not only support clinical relevance it would improve the chances that AI applications developed for use in the community sector would succeed.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621261463882 - Supplemental material for Community Health Nurses’ Perceptions of Emerging Artificial Intelligence and its Impact on Nursing Practice: An Explanatory Sequential Mixed Methods Study
Supplemental material, sj-docx-1-cjn-10.1177_08445621261463882 for Community Health Nurses’ Perceptions of Emerging Artificial Intelligence and its Impact on Nursing Practice: An Explanatory Sequential Mixed Methods Study by Mary Henderson Betkus, Davina Banner, Leanne M. Currie, Piper Jackson and Shannon Freeman in Canadian Journal of Nursing Research
Footnotes
Acknowledgements
We would like to thank the nurse participants who contributed to this study by sharing their time and experiences.
Ethical Considerations
Research approval (#6009080, #6009311) was received from the University of Northern British Columbia (UNBC) research ethics board (REB) April 2023 for Quantitative phase and November 2023 for qualitative phase.
Informed consent was provided by the participant electronically prior to access to the on-line survey.
Written informed consent was provided by each focus group participant prior to participating in the focus group activity.
Written or verbal informed consent was given by each participant in the member check interview.
Author Contributions
Conceptualization: All, Methodology: All, Formal Analysis: All, Investigation: MHB, Data curation: MHB, Original Draft: MHB, Review and editing: All, Validation: All, Visualization: All, Supervision: SF, LC, DB, PJ
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The research ethic approval does not include sharing of data other than what is presented in the paper.
No generative AI was used to produce the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.