
Abstract
Background
Achieving culturally safe healthcare is a global priority, yet traditional immersion programs are often costly, inaccessible or short-term, limiting opportunities to examine positionality, power, and colonial accountability. Collaborative Online International Learning (COIL) offers a scalable alternative in nursing education. This study evaluated a COIL Indigenous Health module delivered through a virtual global classroom and immersive digital tools across two countries.
Methods
A mixed methods design included pre- and post-module surveys and focus group interviews. Of 165 enrolled nursing students, 162 consented to participate and 74 provided matched pre–post responses. Students engaged in synchronous virtual global classrooms, virtual reality (VR) simulations, and asynchronous Padlet discussions. Cultural capability was measured using a validated tool; paired-samples t-tests (α = 0.01; Cohen's dz) quantified pre-post change. Post-module surveys (students) and focus groups (students n = 12; faculty n = 10) assessed COIL perceptions.
Results
Advocacy for Indigenous health improved significantly (p < .001; dz ≈ 0.68), as did confidence in culturally safe communication (p = .001; dz ≈ 0.40). Students rated the Indigenous Health VR scenario highly (M = 4.50) reporting transformative learning. Faculty reported enhanced pedagogical skills, deepened research engagement and strengthened international partnerships.
Conclusions
The Indigenous Health COIL module improved cultural capability and facilitated deep reflection on equity and historical influences related to Indigenous health. Immersive VR and cross-national dialogue created emotionally resonant learning experiences. Faculty gained opportunities for professional growth and sustained collaboration. Embedding Indigenous-led COIL modules into core curricula offers a scalable, globally relevant approach to developing culturally safe health professionals.
Keywords
Background and Purpose
The Imperative for Indigenous Health Education
Globalisation, increased migration, and the enduring legacies of colonisation have intensified the need for culturally safe and responsive healthcare systems (Handtke et al., 2019; Te et al., 2019; Zak, 2021). In settler-colonial nations such as Australia and Canada, Indigenous Peoples continue to experience significant health inequities, shaped by both historical and ongoing impacts of colonisation, including intergenerational trauma, systemic racism, and unequal access to culturally appropriate services (Australian Institute of Health and Welfare, 2025; Hosking et al., 2023; Truth Reconciliation Commission of Canada, 2015).
These persistent disparities highlight the need for preparing nursing graduates to provide culturally safe care—an approach that involves recognising power imbalances, challenging institutional bias, and respecting Indigenous worldviews (Curtis et al., 2019; Te et al., 2019). Nursing professionals, as the largest group of healthcare providers globally, have both responsibility and opportunity to lead this transformation (Wakefield et al., 2021).
Evidence consistently demonstrates that healthcare provider attitudes and behaviours significantly affect Indigenous patients’ healthcare experiences and outcomes, with culturally unsafe care deterring access to services, whilst culturally safe interactions improve outcomes and strengthen patient-provider relationships (Bourassa et al., 2015; Curtis et al., 2019; Freeman et al., 2014; Milligan et al., 2021; Wylie & McConkey, 2019).
Transforming Nursing Education: Beyond Cultural Competence to Cultural Safety
Traditional approaches to educating students related to Indigenous culture in healthcare education have been critiqued for their focus on cultural characteristics rather than power relations, their tendency to essentialise cultural groups, and their failure to address systemic inequities (Browne et al., 2016; Ramsden, 2002). In contrast, cultural safety—a concept developed by Māori nurse Irihapeti Ramsden—places power dynamics, historical context, and Indigenous self-determination at the centre of healthcare education and practice.
Cultural safety requires healthcare providers to examine their own cultural assumptions, recognise the impact of colonisation on health outcomes, and work actively to address systemic barriers to equitable care (Bourassa et al., 2015, 2021; Ramsden, 2002). Importantly, cultural safety is defined not by the healthcare provider but by the recipient of care, emphasising Indigenous peoples’ right to determine what constitutes safe and appropriate care for themselves and their communities (Te et al., 2019).
In the Canadian healthcare landscape, cultural safety is explicitly defined as a patient-determined outcome based in respectful engagement that addresses power imbalances within healthcare systems (Aboriginal Nurses Association of Canada, 2009; Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025; First Nations Health Authority, 2016). Within this framework, cultural humility is understood as the ongoing practice required to achieve cultural safety. Cultural humility involves lifelong critical self-reflection on positionality, power and both personal and systemic biases, and is essential for fostering relationships based on trust and accountability (Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025; First Nations Health Authority, 2016).
The Canadian Nurses Association further identifies “Pursuing Truth and Reconciliation” as a foundational professional value, requiring nurses to acknowledge their role in addressing the historical and ongoing harms of colonisation and to actively respond to the Truth and Reconciliation Commission's Calls to Action. This includes recognising the profession's historical complicity in colonial systems and integrating First Nations, Inuit, and Métis knowledges into practice (Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025).
Preparing nursing students for culturally safe practice therefore requires more than knowledge of cultural practices. It demands pedagogical approaches that centre Indigenous voices, acknowledge historical and ongoing trauma, and support students to critically reflect on their positionality and the power they hold within healthcare systems (Aboriginal Nurses Association of Canada, 2009; Ball & Janyst, 2008; Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025; Wilson, 2023).
Barriers to Traditional Immersive Learning
In-country cultural immersion programs have traditionally offered transformative learning opportunities. However, these programs are often costly, logistically complex, and inaccessible to many students due to financial or safety constraints, including direct costs such as travel, accommodation, and visa fees, and indirect costs such as lost income and the additional burden on students with caring responsibilities (Rubin, 2017; Trapani & Cassar, 2020; Zak, 2021).
These approaches may also raise ethical concerns. When Indigenous communities are positioned primarily as sites of learning rather than as partners in co-creation, such programs risk becoming extractive, placing responsibility on communities to support students’ reflection or “unlearning” without ensuring reciprocity, shared authority, or sustained benefit. The COVID-19 pandemic further highlighted the vulnerability of travel-based models, reinforcing the need for accessible and sustainable alternatives.
Collaborative Online International Learning: An Innovative Approach
Collaborative Online International Learning (COIL), a model pioneered by the State University of New York (SUNY), offers an innovative and inclusive alternative. COIL brings together students and faculty from different countries in co-designed, co-taught, and co-assessed online learning experiences that promote intercultural engagement and global perspectives (SUNY COIL Centre, 2023).
In health professions education, COIL has been shown to enhance intercultural engagement, communication skills, and global health understanding, while supporting inclusive internationalisation (Hackett et al., 2023; Hua et al., 2023; Jager et al., 2019; Niitsu et al., 2023; Roqueta-Vall-llosera et al., 2024; Woodley et al., 2023). It is increasingly recognised as a scalable and cost-effective approach to embedding internationalisation at home (De Castro et al., 2019; Zak, 2021).
Despite this potential Indigenous health remains underrepresented in COIL initiatives. This is likely due to ethical and structural challenges, including the need to avoid tokenism, the importance of Indigenous-led co-design, and concerns about generalising place-based Indigenous knowledges across contexts (Hosking et al., 2023; Lindstrom, 2022). It may also reflect a broader tendency within international education to prioritise generic intercultural competencies over engagement with local Indigenous realities. As a result, there is limited research evaluating COIL initiatives focused on Indigenous health, representing an important gap in the literature (Shaw et al., 2025).
Theoretical Framework
This study draws on three complementary perspectives to understand intercultural learning in virtual environments. Bennett's Developmental Model of Intercultural Sensitivity provides a framework for understanding how students’ perspectives shift through intercultural engagement (Bennett & Bennett, 2004). Ramsden's concept of cultural safety foregrounds power, patient-defined safety, and systemic inequities (Ramsden, 2002). Mezirow's transformative learning theory
Cultural Capability Assessment
The Cultural Capability Measurement Scale (West et al., 2017, 2018) was used to assess students’ preparedness for culturally safe practice with Indigenous populations. The scale measures domains including cultural self-awareness, understanding of colonisation, Indigenous cultural knowledge, communication, advocacy, and equity.
Grounded in cultural safety principles, the tool emphasises power, systemic inequities, and Indigenous self-determination, capturing both knowledge and reflective capability (West et al., 2017). While cultural humility, as a lifelong practice of critical self-reflection (Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025; First Nations Health Authority, 2016), underpins the educational approach, it is not directly measured. Instead, the scale is interpreted as reflecting progression towards culturally safe practice, recognising that cultural safety is defined by the recipient of care (Aboriginal Nurses Association of Canada, 2009; Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025).
Study Context and Rationale
Informed by these theoretical perspectives and gaps in the literature, this study evaluated a Collaborative Online International Learning (COIL) Indigenous Health module co-developed through a partnership between nursing educators in Australia and Canada. This collaboration reflects shared challenges in Indigenous health education across both contexts, while recognising the importance of engaging with Indigenous knowledges in ways that are relational, context-specific, and ethically grounded.
At both institutions, Indigenous health content was already embedded within core nursing curricula, primarily through classroom-based teaching focused on historical context, cultural knowledge, and professional standards. However, faculty identified limited opportunities for students to translate this knowledge into practice, particularly in developing communication, advocacy, and critical self-reflection. The COIL module was therefore designed as a co-curricular extension to provide applied, experiential learning rather than duplicate existing content.
While previous COIL research has largely focused on student outcomes, there remains limited examination of faculty experiences, co-design processes, and the development of international research partnerships. Addressing this gap, the present study examines both the impact of the module on students’ cultural capability and the experiences of faculty involved in its design and delivery.
This evaluation builds on the COIL protocol published by our team (Kiegaldie et al., 2022), which provided the theoretical and operational framework for designing and delivering the module, including alignment with SUNY COIL standards and Indigenous-led co-design principles (Shay et al., 2024).
Aim: To evaluate the implementation and outcomes of a COIL Indigenous Health module delivered to nursing students in Australia and Canada. Specifically, the study aimed to examine changes in students’ cultural capability and explore their and faculty members’ experiences of the module.
Research Questions
What is the impact of the COIL Indigenous Health module on students’ self-reported cultural capability, as measured by the Cultural Capability Measurement Scale? How do students perceive the COIL learning experience, including VR simulations, virtual global classrooms, and asynchronous collaboration? What are faculty members’ experiences of co-designing and delivering the module, and what factors influence implementation and sustainability?
Methods and Procedures
Study Design
This study employed a mixed methods design consistent with a sequential explanatory approach (Creswell et al., 2003), allowing for a layered understanding of both measurable outcomes and experiential insights from participants. Reporting includes explicit description of the integration rationale, how phases informed each other, and how data were brought together at the interpretation stage. The design supported triangulation of data sources and provided a richer interpretation of the COIL module's impact on students and faculty.
Quantitative phase: Data were collected through a structured pre- and post-module survey to assess students’ self-rated cultural capability and identify patterns of change over the course of the intervention. A post program survey assessed students’ perceptions of the COIL learning experiences.
Qualitative phase: Subsequently, focus groups were conducted with students and faculty. The purpose of this phase was to expand upon and contextualise the quantitative findings, with particular attention to emotional engagement, perceived cultural impact, implementation experiences, and suggestions for program improvement.
Participants and Setting
Student participants were recruited by convenience sampling from Holmesglen Institute (Melbourne, Australia) and Northwestern Polytechnic (Alberta, Canada). Eligible students were enrolled in pre-registration nursing programs and self-selected into the COIL module as a voluntary co-curricular activity. Faculty members (n = 10) who co-designed and co-delivered the module were also invited to participate in the evaluation.
Focus Group Selection: The first 12 student volunteers who consented to focus group participation were recruited, with representation from both institutions (six per site). Faculty focus group participants (n = 10) were purposively recruited from module co-designers and co-deliverers, with five from each institution.
Setting: All activities were conducted online. Synchronous sessions were delivered via Zoom™, asynchronous collaboration occurred through Padlet™, and immersive VR simulations were accessed remotely using CenarioVR™. Focus groups were conducted via Zoom™, audio-recorded, and transcribed verbatim.
Intervention
The intervention in this study was the COIL Indigenous Health module which applied the COIL framework as the overarching design. This module was developed following the COIL protocol published by our team (Kiegaldie et al., 2022), which provided the theoretical and operational foundation for implementation and ensured alignment with SUNY COIL standards . COIL is a structured approach that integrates multiple components to enable intercultural, co-designed learning experiences. In this module, COIL was operationalised through four interconnected strategies:
Immersive Virtual Reality (VR) simulations using CenarioVR™ featuring Indigenous healthcare scenarios. Online Virtual Community (OVC) hosted on Padlet™ for asynchronous engagement, including introductions, preparatory resources and shared cross-cultural reflections. The OVC included structured discussion boards, resource libraries, and weekly faculty reflection prompts aligned with the VR modules. Virtual global classroom via ZoomTM for synchronous case discussions, storytelling, and faculty-led reflections. Collaborative group work between Australian and Canadian students to foster intercultural dialogue.
The module was delivered over six weeks as a co-curricular component within the broader nursing curriculum (see Supplementary Material 1). It was co-designed and co-delivered by faculty from both institutions with input from Indigenous educators and cultural advisors to ensure cultural integrity and relevance. Students participated in mixed-country sessions, jointly facilitated by instructors, creating a unique learning environment that highlighted both shared and distinct experiences of Indigenous health. Faculty also engaged in a
Data Collection
Quantitative Data
Pre- and post-module surveys were administered online via Qualtrics™ to assess students’ self-rated cultural capability. The pre-survey was completed prior to the first Virtual Global Classroom session, and the post-survey immediately following the final COIL learning activity. A separate post-program survey captured students’ perceptions of the COIL experience.
Qualitative Data
Qualitative data were collected through two post-program focus groups conducted via Zoom, one with students (n = 12), and another with international faculty (n = 6). Student discussions explored learning outcomes, emotional engagement, cultural awareness, participation dynamics, and the perceived relevance and professional impact of the module. The faculty focus group examined co-design experiences, pedagogical outcomes, professional development, institutional and operational challenges in COIL delivery, and recommendations for curriculum integration. Sessions were audio-recorded and transcribed verbatim using an external transcription service.
The student guide included prompts on experiences with COIL components (VR, Virtual Global Classroom, OVC), perceived cultural impact and emotional engagement, technology usability, implementation enablers and challenges, and suggestions for improvement. The faculty focus group examined co-design experiences, pedagogical outcomes, professional development, institutional and operational challenges in COIL delivery, and recommendations for curriculum integration.
Instruments
Cultural Capability Measurement Tool: We used a modified version of the First Peoples Cultural Capability Measurement Tool, developed to measure the effectiveness of cultural capability education and validated with undergraduate health students (West et al., 2017, 2018). The tool measures preparedness for culturally safe practice across five domains: cultural self-awareness, historical understanding, cultural knowledge, communication confidence, advocacy and equity understanding. It comprises 18 items rated on a 5-point Likert scale (1 = Strongly disagree to 5 = Strongly agree). For this study, minor wording adaptations were made to reflect both Australian and Canadian contexts. One item (“Improving First/Indigenous Peoples’ health is the responsibility of all health professionals”) was inadvertently omitted from the post-survey due to a programming error. Published reliability for the tool is strong (Cronbach's α ≈ 0.86); internal consistency for this sample will be reported in the results.
Post-program COIL Learning Experience Survey: The post-survey was adapted from the International Cross-Cultural Experiential Learning Toolkit (State University of New York, 2015). It included 17 Likert-scale items (1 = Strongly disagree to 5 = Strongly agree) and open-ended questions. Items explored the motivators for students participating in a COIL program, their expectations of the COIL program, and overall COIL experience. Content validity was established through review by faculty from both institutions and Indigenous advisors.
Ethical Considerations
Approval
The study was approved by Holmesglen Institute's Human Research Ethics Review Panel (HRERP #01/2020). Students were participants in this evaluation rather than co-researchers in the formal sense and therefore were not involved in evaluation design, analysis, or interpretation. Recruitment was managed through faculty offices, but consent was obtained independently of the teaching relationship; students were explicitly advised that participation was voluntary and would not affect their academic standing. No teachers who directly assessed participating students were involved in data collection or analysis. The Indigenous co-design partners for the VR scenario are acknowledged in this paper.
Prior to participation, students were provided with a Welfare Letter, and it was explained during the introductory session that should there be Indigenous students who are impacted to contact one of the facilitators who stayed in a breakout room to talk with anyone who needed it. Students were also provided with the number for Indigenous mental health support.
Data Analysis
Quantitative Data
Survey data were analysed using IBM SPSS Statistics (version 18)®. Descriptive statistics (means, standard deviations, frequencies) summarised demographic data and baseline characteristics. Paired-samples t-tests examined pre–post changes in cultural capability. We set α = 0.01 to reduce Type I error across multiple comparisons. Effect sizes were calculated using Cohen's dz for paired designs (computed as t/√n), providing an estimate of the magnitude of change. With n = 74 paired responses, the study had 80% power to detect a moderate effect size (Cohen's dz ≈ 0.34) at α = 0.01.
Qualitative Data
Qualitative data were analysed thematically using Braun and Clarke's six-step reflexive thematic analysis framework: (1) familiarisation, through repeated reading of all focus group transcripts; (2) generation of initial codes, applied independently by two researchers (LS and DK) in Excel; (3) collation of codes into candidate themes through discussion and consensus; (4) review of themes against the dataset to ensure coherence and distinctiveness; (5) refinement and naming of themes; and (6) production of the final thematic account. This approach was selected for its flexibility, reflexivity, and suitability for exploring experiential data in health education (Braun & Clarke, 2006). Both researchers (LS, DK) are based in Australia; Canadian co-author (TE) reviewed emerging themes for cultural resonance within the Canadian context to strengthen cross-national analytical rigour. Peer debriefing was used to manage interpretive differences, and reflexive notes were maintained throughout. Rigour was further supported through triangulation across data sources (student and faculty focus groups, open-ended survey responses) and an audit trail of coding decisions. Data saturation was considered achieved when no new themes emerged across focus group transcripts during iterative coding, consistent with reflexive thematic analysis practice.
Results
Participant Characteristics (Students)
A total of 165 students participated in the Indigenous Health module. Of these, 162 consented to the study (participation rate = 98.2%), and 74 provided matched pre–post survey responses (paired completion rate = 45.7%). Sixty-four were from Holmesglen Institute (Australia) and 98 from Northwestern Polytechnic (Canada). The majority (94%) were enrolled in Bachelor of Nursing programs, with a smaller proportion from diploma-level programs. The cohort reflected considerable cultural diversity: 49% of students spoke a language other than English at home, and 25% were international students (Table 1).
Student Demographics.
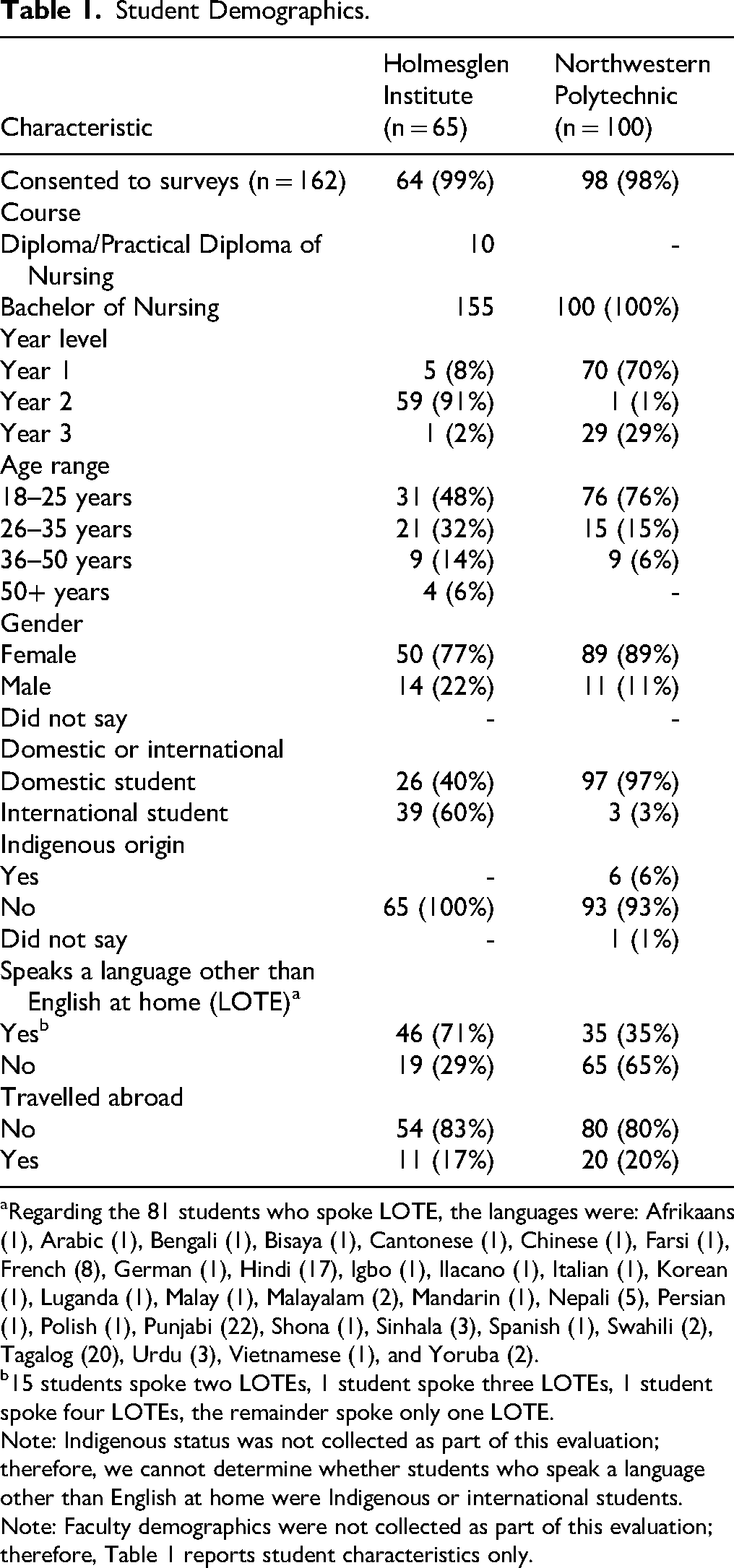
Regarding the 81 students who spoke LOTE, the languages were: Afrikaans (1), Arabic (1), Bengali (1), Bisaya (1), Cantonese (1), Chinese (1), Farsi (1), French (8), German (1), Hindi (17), Igbo (1), Ilacano (1), Italian (1), Korean (1), Luganda (1), Malay (1), Malayalam (2), Mandarin (1), Nepali (5), Persian (1), Polish (1), Punjabi (22), Shona (1), Sinhala (3), Spanish (1), Swahili (2), Tagalog (20), Urdu (3), Vietnamese (1), and Yoruba (2).
15 students spoke two LOTEs, 1 student spoke three LOTEs, 1 student spoke four LOTEs, the remainder spoke only one LOTE.
Note: Indigenous status was not collected as part of this evaluation; therefore, we cannot determine whether students who speak a language other than English at home were Indigenous or international students.
Note: Faculty demographics were not collected as part of this evaluation; therefore, Table 1 reports student characteristics only.
Although Table 1 presents characteristics for all participants, only 74 students provided matched pre–post survey responses (effective response rate = 45.7%; attrition rate = 54.3%). This high attrition rate suggests potential participation bias, as completers may differ in motivation or demographics from non-completers. Detailed comparison was not possible due to missing data for non-completers.
This section integrates quantitative findings from Tables 2 and 3 with thematic findings from Supplementary Materials 2 and 3, tracing the mechanisms through which specific module components produced measurable and experiential change.
Self-Reported Change in Cultural Capability (Pre–Post, n = 74 Paired Responses).
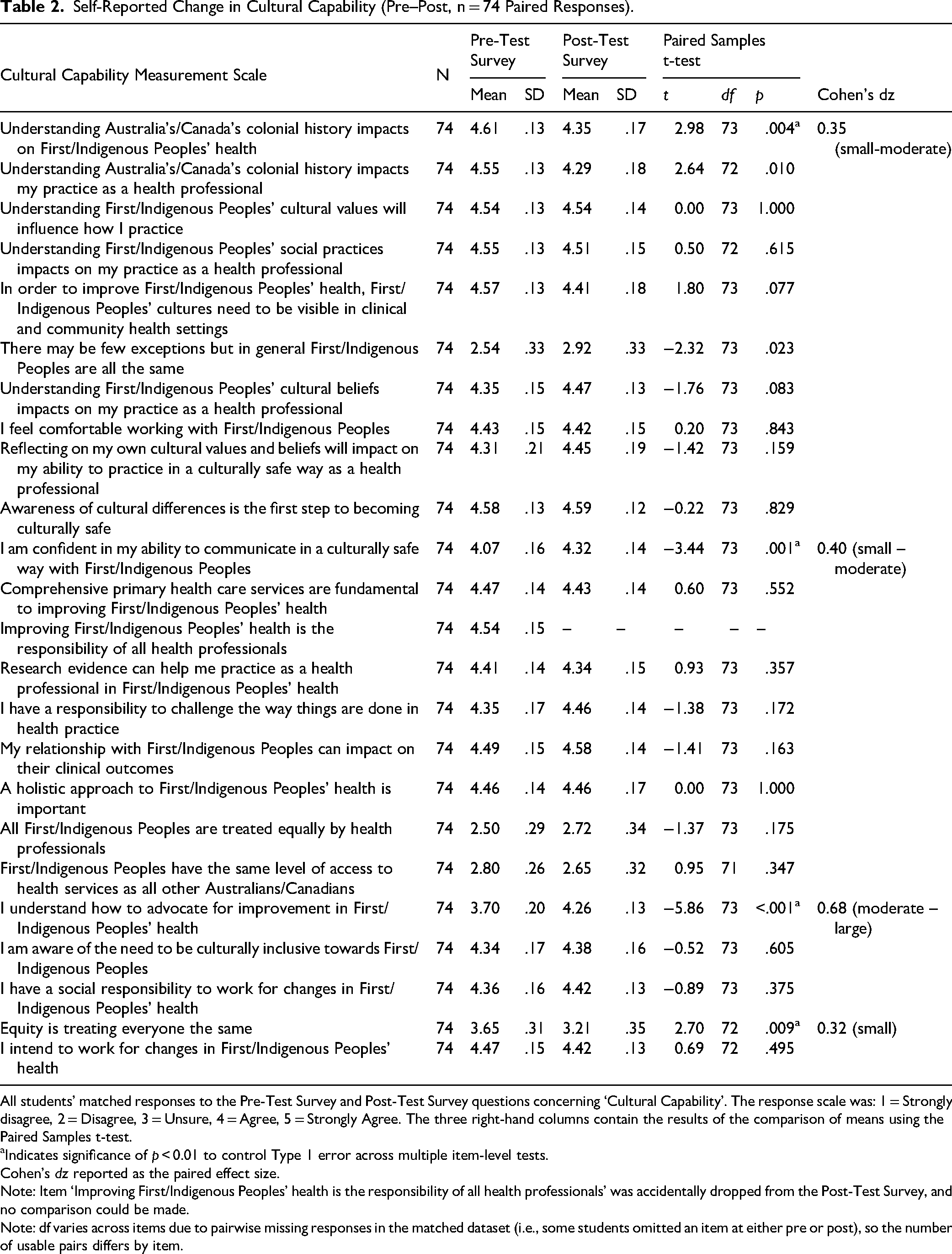
All students’ matched responses to the Pre-Test Survey and Post-Test Survey questions concerning ‘Cultural Capability’. The response scale was: 1 = Strongly disagree, 2 = Disagree, 3 = Unsure, 4 = Agree, 5 = Strongly Agree. The three right-hand columns contain the results of the comparison of means using the Paired Samples t-test.
Indicates significance of p < 0.01 to control Type 1 error across multiple item-level tests.
Cohen's dz reported as the paired effect size.
Note: Item ‘Improving First/Indigenous Peoples’ health is the responsibility of all health professionals’ was accidentally dropped from the Post-Test Survey, and no comparison could be made.
Note: df varies across items due to pairwise missing responses in the matched dataset (i.e., some students omitted an item at either pre or post), so the number of usable pairs differs by item.
Views on the COIL Learning Experiences and the Indigenous Health Module.
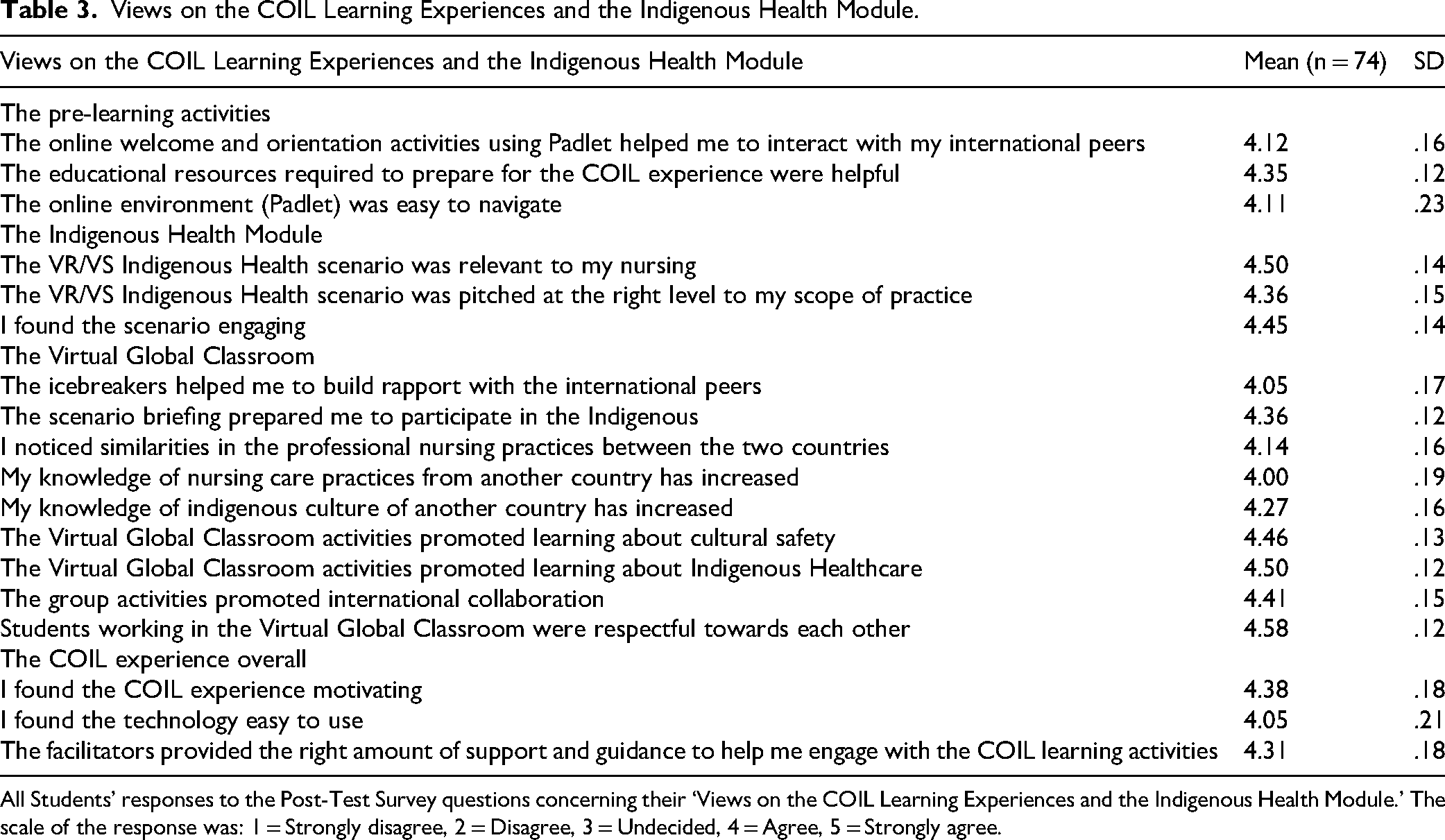
All Students’ responses to the Post-Test Survey questions concerning their ‘Views on the COIL Learning Experiences and the Indigenous Health Module.’ The scale of the response was: 1 = Strongly disagree, 2 = Disagree, 3 = Undecided, 4 = Agree, 5 = Strongly agree.
Change in Cultural Capability
Advocacy for Indigenous health showed the largest pre-post shift (3.70 to 4.26; p < .001; dz ≈ 0.68, moderate–large) and the qualitative data provide a clear explanatory account. Students reported that confronting the VR scenario made systemic inequities tangible in a way that abstract knowledge had not: “To really highlight that I probably have to be a better advocate for Indigenous people because I am so educated on the issue” (Student P2, Supplementary Material 3).
Faculty independently observed this shift: “I really enjoyed watching the empathy grow” (Faculty P1, Supplementary Material 2).
This convergence across data sources strengthens the interpretation that the VR scenario, rather than the COIL format itself, was the active ingredient driving advocacy gains.
Confidence in culturally safe communication also improved significantly (4.07 to 4.32; p = .001; dz ≈ 0.40, small–moderate). Qualitatively, this aligns with students’ accounts of the Virtual Global Classroom as a site of practiced cross-cultural interaction: “It probably will empower me to advocate more and not assume that everybody has the same motivation” (Student P2, Supplementary Material 3).
Faculty observed the same process from the facilitation side, describing, “so many goosebump moments … to see the empathy that came through with the students” (Faculty P8, Supplementary Material 2).
Students rated the Virtual Global Classroom's promotion of cultural safety learning at M = 4.46 (Table 3), and the respectful collaborative environment at M = 4.58 — the highest-rated item in the survey — suggesting these conditions actively supported communication confidence.
Two further items met the significance threshold. The decrease in colonial history scores (4.61 → 4.35; p = .004; dz ≈ 0.35) was initially counterintuitive. The qualitative data offer an explanatory frame: students described being, “quite taken back by the lack of knowledge … there's a real need for programs like this” (Student, Supplementary Material 3),
Several high-scoring items showed no significant change (e.g., holistic care, cultural inclusion, social responsibility), all remaining above 4.3. This pattern is meaningful: it suggests these foundational values were already established in this nursing cohort and were sustained rather than eroded by the module. The items that did shift were those requiring more active, applied capability: knowing how to advocate, communicating confidently, and holding a nuanced view of equity, which were the competencies targeted by the VR scenario and the Virtual Global Classroom format.
Views on the COIL Learning Experiences and Indigenous Health Module
Overall, students reported highly positive perceptions of the COIL learning experience and the Indigenous Health Module (Table 3). Students rated the Indigenous Health VR/VS scenario as the highest rated item for relevance to nursing practice (M = 4.50) and rated Indigenous healthcare learning in the Virtual Global classroom equally highly (M = 4.50). Faculty corroborated the scenario's impact: “I really loved having a virtual simulation to bring in the clinical piece right into the lecture component” (Faculty P7, Supplementary Material 2),
and students reported the experience prompted direct professional reflection: “I realised … there are actually services that you can recommend for [Indigenous patients] as a post care” (Student P1, Supplementary Material 3).
Taken together, the integrated findings suggest two distinct mechanisms of change. First, the VR scenario operated as a disorienting dilemma — producing emotional engagement, recalibrated confidence, and heightened advocacy motivation. Second, the Virtual Global Classroom provided a structured space for practising culturally safe communication across national contexts, producing the confidence gains observed. These mechanisms align with Mezirow's transformative learning theory and Ramsden's cultural safety framework respectively, demonstrating that the multi-component COIL design addressed different dimensions of cultural capability through complementary pedagogical pathways.
Qualitative Findings
Thematic analysis of focus group data revealed complementary insights from faculty and students across cultural, pedagogical, emotional, and technological domains. Representative quotes from Supplementary Materials 2 (faculty) and 3 (student) are embedded within each theme to anchor the interpretive claims in participant voices. Both datasets showed a high degree of alignment.
Faculty Perspectives (Supplementary Material 2)
Faculty participants (n = 10) identified eight themes across their experience of the COIL module, described below with illustrative quotes from Supplementary Material 2.
Theme 1: Professional growth through collaboration. Faculty described significant professional development through international partnership and collaborative teaching. Exposure to diverse healthcare systems broadened perspectives and supported pedagogical innovation. As one faculty member noted: “I think the differences but similarities between the two healthcare systems” (P8), while another described the value of cross-institutional student interaction: “I myself, loved seeing the students collaborate internationally with each other but also within the same departments” (P7).
Theme 2: Research collaboration opportunities. For faculty new to research, the COIL program offered a meaningful entry point: “I haven’t conducted or been part of much research, so I just loved being able to collaborate with people that have done research” (P7). Others described sustained intellectual engagement beyond the module: “I’ve found myself going down rabbit holes and looking at different journal articles … finding it really interesting” (P8).
Theme 3: Pedagogical innovation. Co-teaching in a virtual setting encouraged integration of emerging tools, particularly VR. Faculty valued the multifaceted learning design: “I really loved having a virtual simulation to bring in the clinical piece right into the lecture component” (P7). The layered structure — pre-reading, VR, video, and live classroom discussion — was experienced as coherent and engaging (P4).
Theme 4: Cultural humility development. Faculty engaged in meaningful self-reflection on their own cultural assumptions and unconscious biases, deepening their practice of cultural humility alongside their students. One faculty member described being prompted to examine their own biases: “The two videos … looking at unconscious bias and your culture have really stuck with me” (P1). Another described intentional reorientation: “Making sure that we’re coming from a space of curiosity rather than … judgement” (P6). Notably, even faculty with prior Indigenous community experience found new practical learning (P3).
Theme 5: Virtual Community of Practice benefits. The program fostered lasting relationships among faculty across countries, with one describing the value of students “being collaborative together all around the world. East and west and learning from each other” (P10).
Theme 6: Student engagement observations. Faculty consistently observed profound emotional and empathetic engagement among students, particularly in response to Indigenous content. These moments were described as transformative: “So many goosebump moments … to see the empathy that came through with the students” (P8); “I really enjoyed watching the empathy grow … probably more so for the Indigenous module” (P1); “Watching those a-ha moments, those moments in their faces” (P4). One faculty member described witnessing a student's empathic response to a peer: “Having another student be able to say, ‘I’m sorry that happened to you’ … I didn’t realise” (P1).
Theme 7: Implementation challenges. Faculty identified practical barriers including large group sizes that limited intimate interaction: “The 200 people is a lot to have when you’re trying to get people to interact on a more intimate basis” (P2). Variable student engagement in voluntary sessions was also noted: “It was a totally voluntary project, yet students would come on and wouldn’t say a word” (P1). Platform complexity posed challenges for some educators (P5).
Theme 8: Sustainability considerations. Faculty strongly advocated for formal curriculum integration to maximise participation and impact: “We should embed it into the curriculum as a [core] course” (P1). There were also calls for institutional recognition of the time and labour involved in delivery, and interest in longitudinal follow-up: “I would really like to see how the learnings from VR have translated into clinical practice” (P5).
Student Perspectives (Supplementary Material 3) Student participants (n = 12) identified six themes across their experience of the COIL Indigenous Health module, described below with illustrative quotes from Supplementary Material 3.
Theme 1: Enhanced cultural awareness and empathy. Students described profound emotional engagement with Indigenous narratives that challenged assumptions and expanded cultural understanding. One student reflected on the global reach of colonial histories: “I always, because I’m not from here … This class made me realise that it's other countries too, especially Australia” (P1). Another described genuine surprise at gaps in their prior knowledge: “I was quite taken back by the lack of knowledge … there's a real need for programs like this and for education like this.”
Theme 2: Professional identity development. Students reported increased awareness of cultural considerations in clinical practice and a stronger commitment to culturally safe care. One student described a shift in clinical thinking: “I realised … there are actually services that you can recommend for [Indigenous patients] as a post care” (P1). Another described a reorientation in their approach to patient assumptions: “A reminder to be culturally aware … helped me understand that First Nations people … need more special care” (P4).
Theme 3: Advocacy motivation. Students described a markedly strengthened desire to advocate for Indigenous peoples and address systemic inequities. This was the theme most directly reflected in the quantitative advocacy gain (dz ≈ 0.68): “To really highlight that I probably have to be a better advocate for Indigenous people because I am so educated on the issue” (P2). Another student described the VR scenario as generating the confidence to act: “It probably will empower me to advocate more and not assume that everybody has the same motivation” (P2).
Theme 4: International collaboration benefits. Cross-border peer learning enriched student perspectives and motivated future international practice. Students described the module as broadening their professional horizons: “My plan is to be a travel nurse … That's why this is important … I get to learn about diversity” (P1); “When we did this COIL program it motivates me more … I want to see the other part of the world” (P3).
Theme 5: Curriculum integration support. Students identified the module's national specificity as a limitation and called for comparative content: “The scenario … is just a Canadian way. Where's the Australian way of doing things?” (P3); “If there were two scenarios … that would probably serve the purpose … much better” (P2). Students also raised practical concerns about cohort size: “There was 280-something people at the same time … Some computers can’t handle that many people” (P2). These observations directly informed the Canadian-specific co-design limitation described in this paper.
Theme 6: Technology integration challenges. VR and platform difficulties hindered engagement for some students, particularly with VR hardware reliability: “We were given a VR glass and it didn’t work … This is ridiculous” (P3); “It worked for me but it was lagging really hard … it's slow basically” (P4). Navigation of the Padlet platform was unfamiliar for some: “There were a lot of people that didn’t even know what [Padlet] was” (P2). These experiences point to the need for pre-module technical orientation and hardware testing, particularly for large cohorts.
Discussion
This study evaluated the implementation and impact of a COIL module focused on Indigenous health, delivered to undergraduate nursing students in Australia and Canada. Framed by Bennett's Developmental Model of Intercultural Sensitivity (DMIS) (Bennett & Hammer, 2017), Ramsden's cultural safety framework (Ramsden, 2002), and Mezirow's transformative learning theory (Mezirow, 2000), the findings demonstrate the capacity of well-designed virtual learning environments to promote culturally safe practice, critical reflection, and international collaboration.
The integration of quantitative and qualitative findings strengthens interpretation of the module's impact. Significant gains in advocacy (dz ≈ 0.68) and communication confidence (dz ≈ 0.40) can be traced to specific module components: the VR scenarios generated the disorienting dilemma and emotional resonance that drove advocacy gains, while the Virtual Global Classroom rated highly for promoting cultural safety learning (M = 4.46) and sustaining respectful collaboration (M = 4.58) — built the conditions for communication confidence to grow. The counterintuitive decrease in colonial history scores is interpreted, in light of qualitative accounts of surprise and recalibration, as evidence of deeper critical awareness rather than knowledge loss — a pattern consistent with transformative learning. These mechanisms align with Mezirow's transformative learning theory and Ramsden's cultural safety framework, highlighting how the multicomponent COIL design addressed different dimensions of cultural capability through complementary pedagogical pathways.
Developing Cultural Empathy and Transformative Learning
These findings align with broader research on COIL's ability to foster openness to diversity and global health awareness among nursing students. Niitsu et al. (2023) found that COIL experiences enhanced students’ cultural sensitivity and global engagement (Niitsu et al., 2023), which was mirrored in our findings. Importantly, this reinforces the value of COIL as a low-barrier, scalable alternative to in-country immersion programs, with the added benefit of centring Indigenous voices in ways traditional placements may not.
Students’ engagement with Indigenous narratives, virtual simulations, and intercultural dialogue contributed to the development of cultural empathy and self-awareness, which are key markers of transformative learning. In line with Mezirow's theory, students frequently described discomfort, emotional resonance, or critical questioning triggered by confronting colonial histories and contemporary inequities (Mezirow, 2000). These disorienting experiences catalysed reflection and reframing of prior assumptions, reinforcing the theory's emphasis on perspective transformation as a pathway to deeper understanding.
Advancing Cultural Capability Through Culturally Safe Pedagogy
The COIL module was deliberately structured around Ramsden's principles of cultural safety (Ramsden, 2002), with Indigenous educators’ local Indigenous community members shaping the curriculum and guiding learning activities. As cultural safety is defined by the recipient of care, it was important to acknowledge their perspectives when they did not feel safe in the healthcare setting and how healthcare professionals can show cultural humility. It is important to acknowledge that the Indigenous knowledges, narratives, and cultural markers embedded in this module (including Cree language elements) are specific to particular Nations and communities and are not interchangeable with the knowledges of Australian First Nations Peoples. The module is therefore best understood as an introduction to principles of Indigenous-centred care, prompting students to engage with the communities local to their own future practice, rather than as a culturally universal curriculum. Through immersive simulations, critical reflection exercises, and culturally grounded case studies, students were supported to interrogate their own cultural positioning and recognise their responsibility in fostering equitable healthcare environments.
Student narratives revealed increased confidence in cross-cultural communication, greater awareness of unconscious bias, and strengthened advocacy motivation, reflecting a shift from cultural competence toward cultural humility, where learners actively challenge structural inequity. Importantly, several students identified that cultural safety is defined by the recipient of care, aligning with Ramsden's foundational principle and Hosking et al.'s (2023) finding that Indigenous-led modules were described as “the most culturally safe training I’ve ever had” (Hosking et al., 2023).
Student Experience of the COIL Learning Environment
The virtual learning environment was generally perceived as engaging, inclusive, and intellectually stimulating. The immersive VR simulations were consistently described as impactful, offering emotionally resonant scenarios that helped bridge cognitive and affective learning.
However, some students encountered barriers including technological limitations, variable internet access, and discomfort with speaking in cross-national groups. These challenges reflect the complexity of virtual intercultural education and underscore the importance of providing adequate scaffolding, trauma-informed facilitation, and flexible participation options. Despite these limitations, the module appeared to support the psychological safety necessary for sharing, reflection, and vulnerability, which are core conditions for intercultural and transformative learning (Zak, 2021).
Faculty Development and the Virtual Community of Practice
These findings mirror recent COIL literature that increasingly highlights benefits for faculty, particularly in developing digital capability, co-teaching skills, and pedagogical adaptability (Shaw et al., 2025). These benefits reflect not only professional development but also broader shifts in teaching identity and global engagement.
Beyond student learning, the COIL module offered significant professional development opportunities for faculty. Participation in the design and facilitation of the module fostered cross-cultural dialogue, pedagogical innovation, and reflective practice among educators from both institutions. Faculty reported gaining new insights into Indigenous health, trauma-informed pedagogy, and virtual teaching strategies. These outcomes are consistent with Gerrard et al. (2025), who emphasised the importance of Indigenous governance and co-design in building sustained institutional partnerships and culturally safe curricula, including embedding Indigenous-led decision-making in collaborative curriculum development (Gerrard et al., 2025).
A key legacy of the project was the establishment of a transnational Virtual Community of Practice (VCoP), which extended beyond the formal module into ongoing collaboration. Faculty participants reported increased engagement in research and academic writing with several describing this as their first experience with collaborative research. Some pursued conference presentations and future publications, aligning with COIL's broader goal of fostering international research networks and building educator capacity. These outcomes respond to a critical gap in the COIL literature, which has largely overlooked the role of faculty development and international academic partnership in sustaining global learning outcomes (De Castro et al., 2019).
Curriculum Integration and Sustainability
Both students and faculty strongly advocated for integrating the COIL module into core curricula. Embedding the program, rather than offering it as an optional enrichment activity, was viewed as essential to ensuring equitable access and lasting impact. Several students noted that cultural safety education should not be optional given its centrality to ethical nursing practice. This view aligns with formal professional and accreditation mandates: in Canada, the Canadian Association of Schools of Nursing and provincial nursing regulatory colleges’ Entry to Practice Competency frameworks require programs to address Indigenous health and the Calls to Action of the Truth and Reconciliation Commission (Canadian Indigenous Nurses Association & Canadian Association of Schools of Nursing, 2025); in Australia, the Australian Nursing and Midwifery Board, (ANMAC) accreditation standards (Australian Nursing and Midwifery Accreditation Council, 2025) and the Australian Health Practitioner Regulation Agency (AHPRA) (Australian Health Practitioner Regulation Agency, 2025) codes of conduct require cultural safety for First Nations peoples as a professional expectation for all registered nurses.
To sustain and scale such programs, institutional support is essential. Faculty highlighted the need for recognition of time and labour, protected space for collaboration, and continued investment in digital infrastructure. Crucially, Indigenous leadership must remain central to the design and delivery of future iterations. Formal curriculum integration should not occur without adequate safeguards: sustained Indigenous governance over the content; resourcing of Indigenous faculty and cultural advisors; trauma-informed facilitation training for all educators; and proactive support structures for any Indigenous students in the cohort, who should not be expected to bear the emotional labour of educating their settler peers. Embedding Indigenous ways of knowing and pedagogical sovereignty is not only ethically necessary but enhances the authenticity and relevance of learning experiences(West et al., 2018). As Pitama (2013) argues, Indigenous health curricula must be structurally embedded, not added as optional content, to foster transformative, socially accountable education (Pitama, 2013).
Limitations
This study has several limitations. The effective response rate was 45.7%, with attrition of 54.3%, introducing potential participation bias. Indigenous status was not recorded, which constitutes a significant limitation beyond interpretation alone. The study cannot confirm whether Indigenous students were present in sessions, nor address the potential harm to any Indigenous students who may have experienced content framing Indigenous health and intergenerational trauma as “other” within a predominantly settler peer group. Future iterations must address this by collecting Indigenous status data sensitively and with consent; providing alternative engagement pathways for Indigenous students who wish to opt out of specific content; and involving Indigenous students in program design and governance if they choose to participate. Site-specific analyses were not possible due to data constraints, and one Cultural Capability item was omitted from the post-survey. A further limitation is that the Indigenous co-design partners were all affiliated with Northwestern Polytechnic in Canada; no equivalent Indigenous co-design partner from an Australian First Nations context was involved in scenario development. This means the module's Indigenous content reflects specific Canadian Nations and communities, and its cultural validity for Australian First Nations students and contexts has not been formally established. Outcomes relied on self-report at short follow-up; future research should include longitudinal and behavioural measures.
Implications and Future Directions
Virtual, culturally safe, COIL programs can promote meaningful shifts in students’ cultural capability, empathy, and professional identity, and offer a replicable model for faculty collaboration and curriculum innovation. Future research should explore longitudinal impacts on clinical behaviour, advocacy, and refine trauma-informed approaches for virtual delivery of emotionally complex content.
Conclusion
By embedding cultural safety within nursing education and fostering international collaboration, COIL can serve as a powerful tool in preparing globally competent, equity-oriented health professionals. Sustaining and scaling such initiatives requires institutional commitment, Indigenous leadership and core curricula integration to ensure equitable access and lasting impact.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621261466749 - Supplemental material for Fostering Cultural Safety Through COIL: Evaluating an Indigenous Health Module for Nursing Students in Australia and Canada
Supplemental material, sj-docx-1-cjn-10.1177_08445621261466749 for Fostering Cultural Safety Through COIL: Evaluating an Indigenous Health Module for Nursing Students in Australia and Canada by Louise Shaw, Teresa Evans, Melissa Ciardulli and Debra Kiegaldie in Canadian Journal of Nursing Research
Supplemental Material
sj-docx-2-cjn-10.1177_08445621261466749 - Supplemental material for Fostering Cultural Safety Through COIL: Evaluating an Indigenous Health Module for Nursing Students in Australia and Canada
Supplemental material, sj-docx-2-cjn-10.1177_08445621261466749 for Fostering Cultural Safety Through COIL: Evaluating an Indigenous Health Module for Nursing Students in Australia and Canada by Louise Shaw, Teresa Evans, Melissa Ciardulli and Debra Kiegaldie in Canadian Journal of Nursing Research
Supplemental Material
sj-docx-3-cjn-10.1177_08445621261466749 - Supplemental material for Fostering Cultural Safety Through COIL: Evaluating an Indigenous Health Module for Nursing Students in Australia and Canada
Supplemental material, sj-docx-3-cjn-10.1177_08445621261466749 for Fostering Cultural Safety Through COIL: Evaluating an Indigenous Health Module for Nursing Students in Australia and Canada by Louise Shaw, Teresa Evans, Melissa Ciardulli and Debra Kiegaldie in Canadian Journal of Nursing Research
Footnotes
Acknowledgements
The authors wish to acknowledge the valuable contributions of the staff and students from Holmesglen Institute and Northwestern Polytechnic who participated in the COIL experience. We are especially grateful to the Indigenous co-creators of the Indigenous Health module, Desiree Mearon, Bernadette Laboucan, and Darlene Horseman, whose knowledge, insights, and cultural guidance enriched the learning experience and deepened the impact of this initiative.
Holmesglen acknowledges the local Aboriginal people of the land on which its many sites are located. Holmesglen acknowledges Aboriginal people as the Traditional Owners/Custodians of the land. We are committed to improving the health and wellbeing of Aboriginal and Torres Strait Islander people and their communities.
Northwestern Polytechnic acknowledges that our campuses are located on Treaty 8 territory, the ancestral and present-day home to many diverse First Nations, Metis, and Inuit people. We are grateful to work, live and learn on the traditional territory of Duncan's First Nation, Horse Lake First Nation and Sturgeon Lake Cree Nation, who are the original caretakers of this land.
Ethical Approval and Informed Consent Statements
The study was approved by Holmesglen Human Research Ethics Review Panel (HRERP # 01/2020). Participation was voluntary. Students and faculty provided informed consent via an online checkbox in Qualtrics before completing surveys and could withdraw at any time without penalty. Pre–post survey matching used student IDs, which were anonymized by an independent researcher before analysis. Focus group transcripts were de-identified. Data were stored securely in password-protected institutional systems.
Funding
The trial was funded by a Study Melbourne Research Partnership grant from the Victorian Endowment for Science Knowledge and Innovation (VESKI) organisation. The funding body have no role in research design, data collection or data analysis. All evaluation was independent from the funding body.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.