
Abstract
The investigation of acute pulmonary embolism is a common task for radiologists in Canada. Technical image quality and reporting quality must be excellent; pulmonary embolism is a life-threatening disease that should not be missed but overdiagnosis and unnecessary treatment should be avoided. The most frequently performed imaging investigation, computed tomography pulmonary angiogram (CTPA), can be limited by poor pulmonary arterial opacification, technical artifacts and interpretative errors. Image quality can be affected by patient factors (such as body habitus, motion artifact and cardiac output), intravenous (IV) contrast protocols (including the timing, rate and volume of IV contrast administration) and common physics artifacts (including beam hardening). Mimics of acute pulmonary embolism can be seen in normal anatomic structures, disease in non-vascular structures and pulmonary artery filling defects not related to acute pulmonary emboli. Understanding these pitfalls can help mitigate error, improve diagnostic quality and optimize patient outcomes. Dual energy computed tomography holds promise to improve imaging diagnosis, particularly in clinical scenarios where routine CTPA may be problematic, including patients with impaired renal function and patients with altered cardiac anatomy.
Introduction
Acute pulmonary embolism (PE) is an important cause of cardiovascular morbidity and mortality in Canada.1-4 It is a difficult clinical diagnosis to make and thus leads to thousands of computed tomography pulmonary angiogram (CTPA) studies being performed every year in patients in emergency departments and on inpatient wards. 1 CTPA plays a vital role in the diagnosis of acute PE while also helping to guide management due to its ability to identify imaging features that confer worse outcomes such as right heart enlargement and strain and central distribution of pulmonary emboli.2-9 Additional benefits of accessibility, accuracy, identification of alternate diagnoses and rapid reporting turn-around time have helped establish CTPA as the current standard of care imaging for acute PE.
Part 1 of our guidance document covered the essentials of optimal CTPA acquisition techniques including radiation dose reduction strategies and intravenous contrast considerations. Population based guidance relating to imaging pregnant and early post-partum patients suspected of having acute PE was also discussed.
Part 2 describes the common technical and image interpretation pitfalls that range from contrast timing and bolus interruption issues, motion and beam hardening artifact, interpretation pitfalls secondary to a post-surgical state or acute PE mimics such as chronic PE, neoplasms, tumor emboli and vasculitis. Part 2 also highlights emerging technologies such as dual energy CT and its potential future role in the imaging of acute PE. In the supplement, we provide a CTPA reporting template to draw attention to the key elements that should be included in the radiology report. Accurate description of the location of single or multiple filling defects within the pulmonary artery tree (segmental versus subsegmental etc.) is emphasized due to the potential impact on management.
Technical Issues and Pitfalls
Poor Contrast Opacification
Inadequate intravenous contrast concentration in the pulmonary arteries is a common technical problem. Ideally, density measurements in the main pulmonary artery and peripheral pulmonary arteries should be at least 300 HU. Poor opacification can be the result of 3 main errors: scanning the patient too early (before the contrast has adequately opacified the arteries); scanning too late (“missing” the bolus); or may result from an interruption of the IV contrast bolus. These errors can occur regardless of whether bolus tracking or test bolus protocols are used. Understanding why these errors occur can help radiologists adjust imaging protocols to pre-emptively mitigate these errors in patients at increased risk (Figure 1).
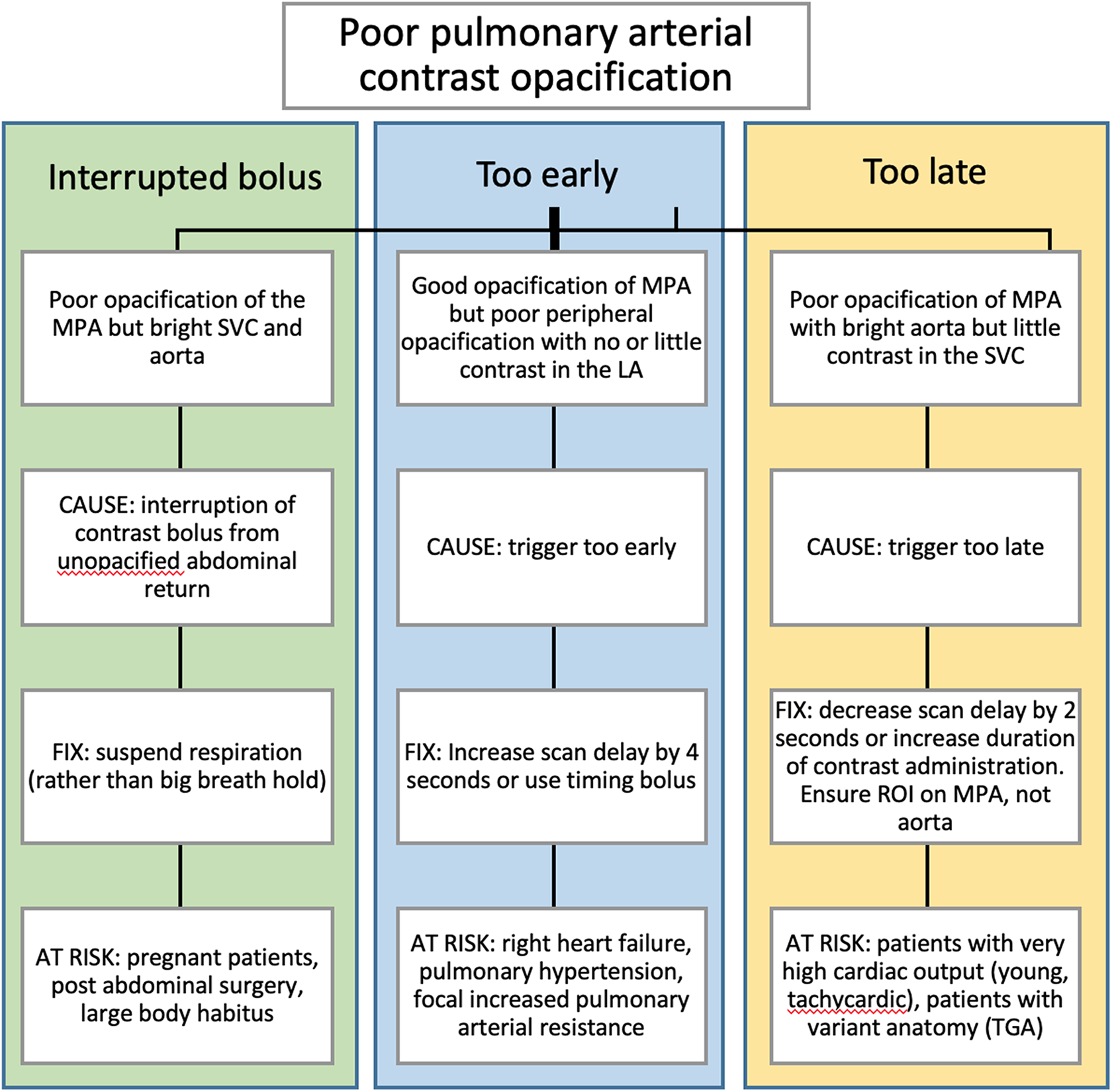
Flow chart for identifying causes of poor pulmonary contrast opacification.
If an exam has already been performed and IV contrast concentration is suboptimal, radiologists must decide whether the exam requires repeating or if the acquired images are diagnostic. In some cases, particularly for patients with renal failure or normal underlying lungs, an alternative exam can be performed with VQ imaging rather than a repeat CT. In other non-diagnostic CT exams, a careful search for alternate causes of symptoms should be done before deciding to repeat the test. Finally, when CTPA is non-diagnostic in the distal segmental or subsegmental arteries and repeating the scan is unlikely to result in a better quality study, bilateral lower limb duplex ultrasound can be considered as the next imaging modality to evaluate for deep venous thrombosis (DVT).
Interruption of Contrast Bolus
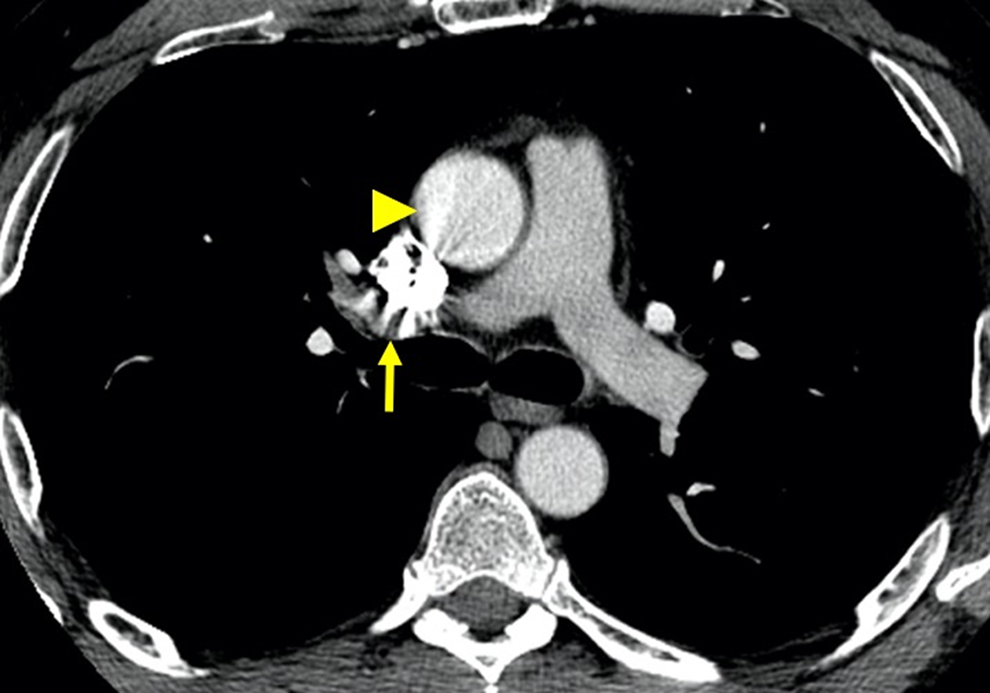
The most likely explanation for poor contrast in the main pulmonary artery but bright contrast in the aorta is transient interruption of contrast from IVC flow (Figure 2). This is most likely to occur in patients with increased abdominal pressure and is often a concern in pregnancy, in patients with recent abdominal surgery and in obese patients.1-3 Patients at risk should be instructed in breath suspension and should not be asked to “take a big breath in and hold it.”4,5 On fast scanners, it may be possible to obtain adequate imaging without any interruption of breathing.
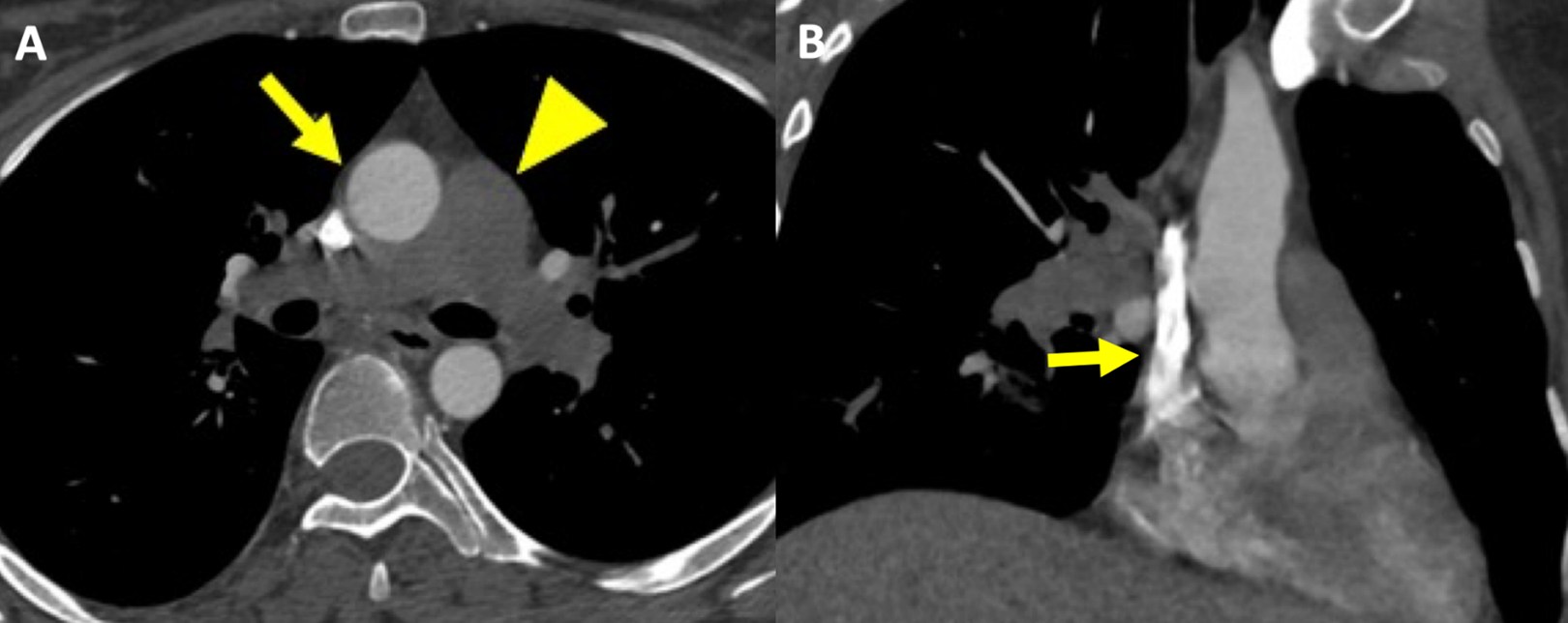
32-year-old woman 3-days post-partum with shortness of breath and chest pain and transient interruption of contrast. A, Axial CTPA image, mediastinal reconstruction, reveals dense contrast in the ascending aorta (arrow) and absence of contrast in the main, right and left pulmonary arteries (arrowhead). B, Coronal oblique reformat shows contrast in the SVC.
Scanning Too Early
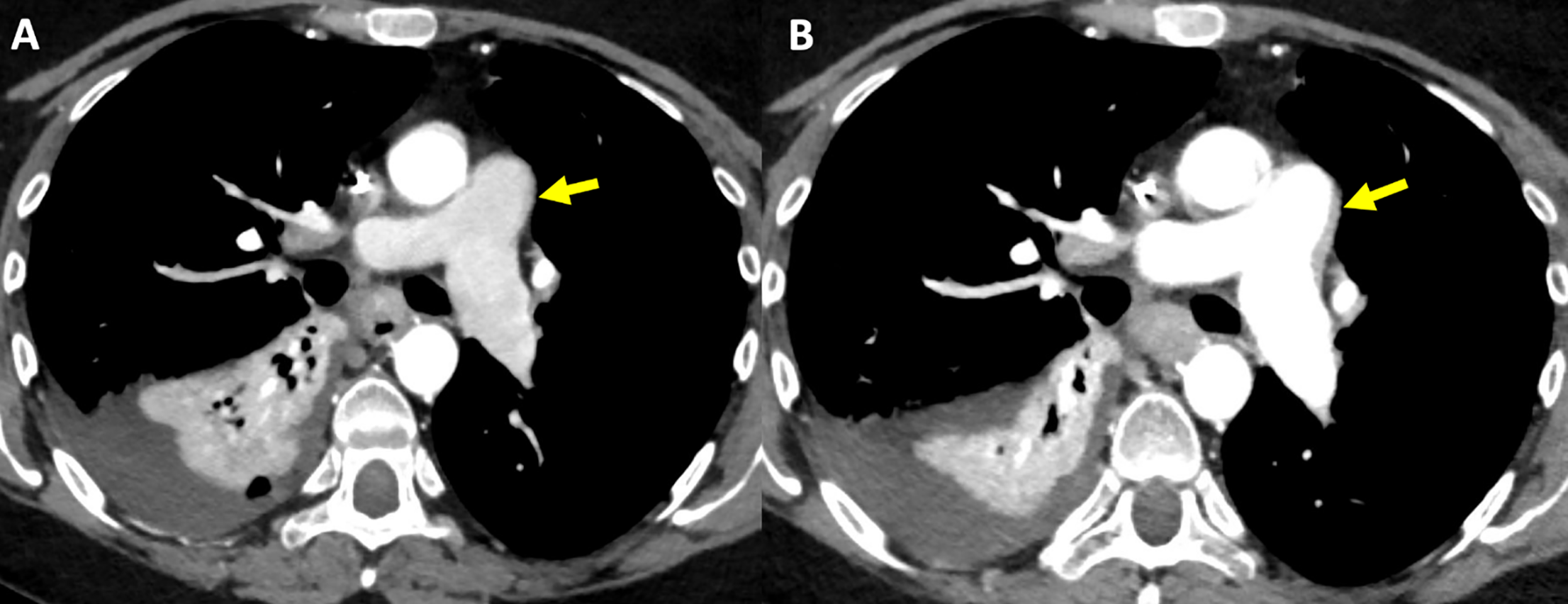
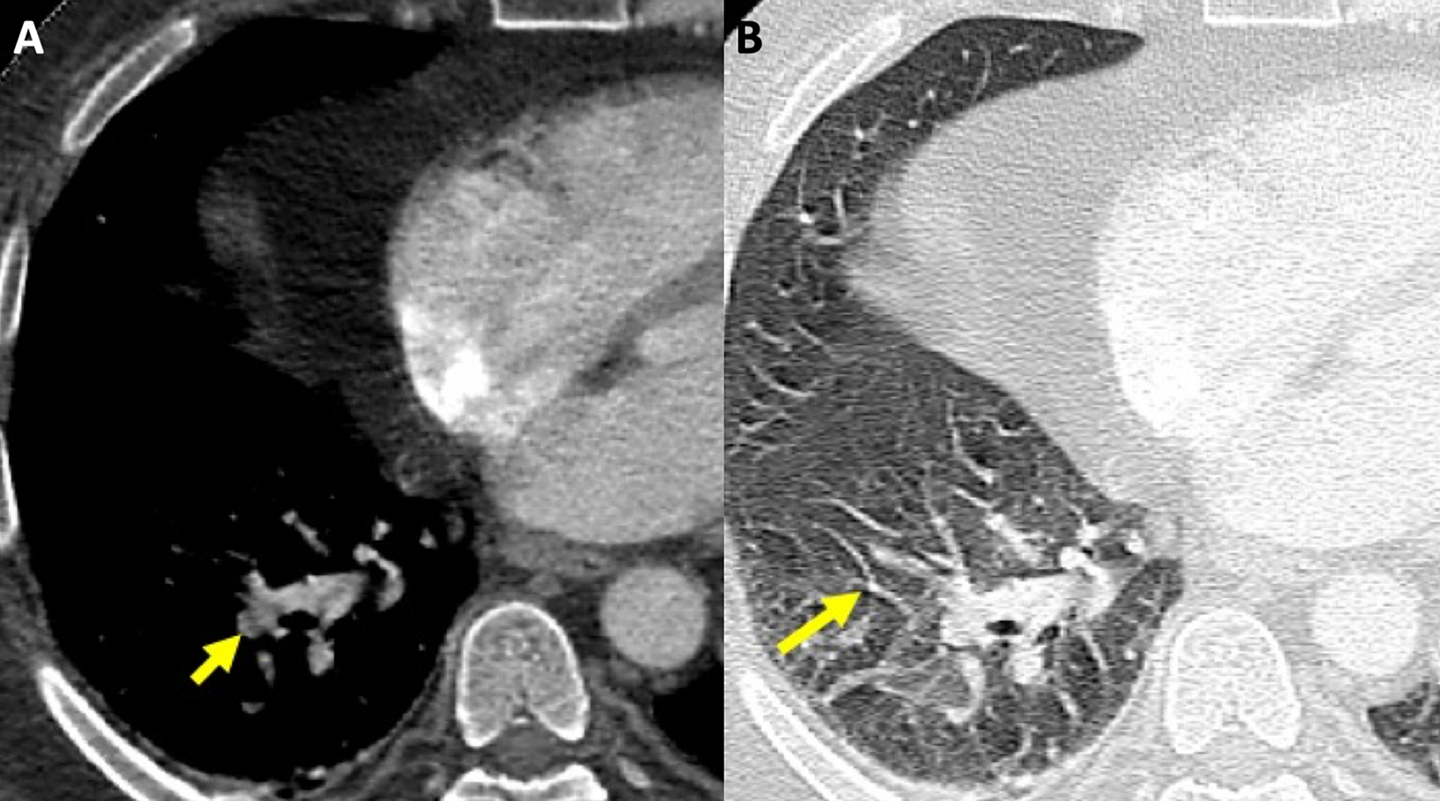
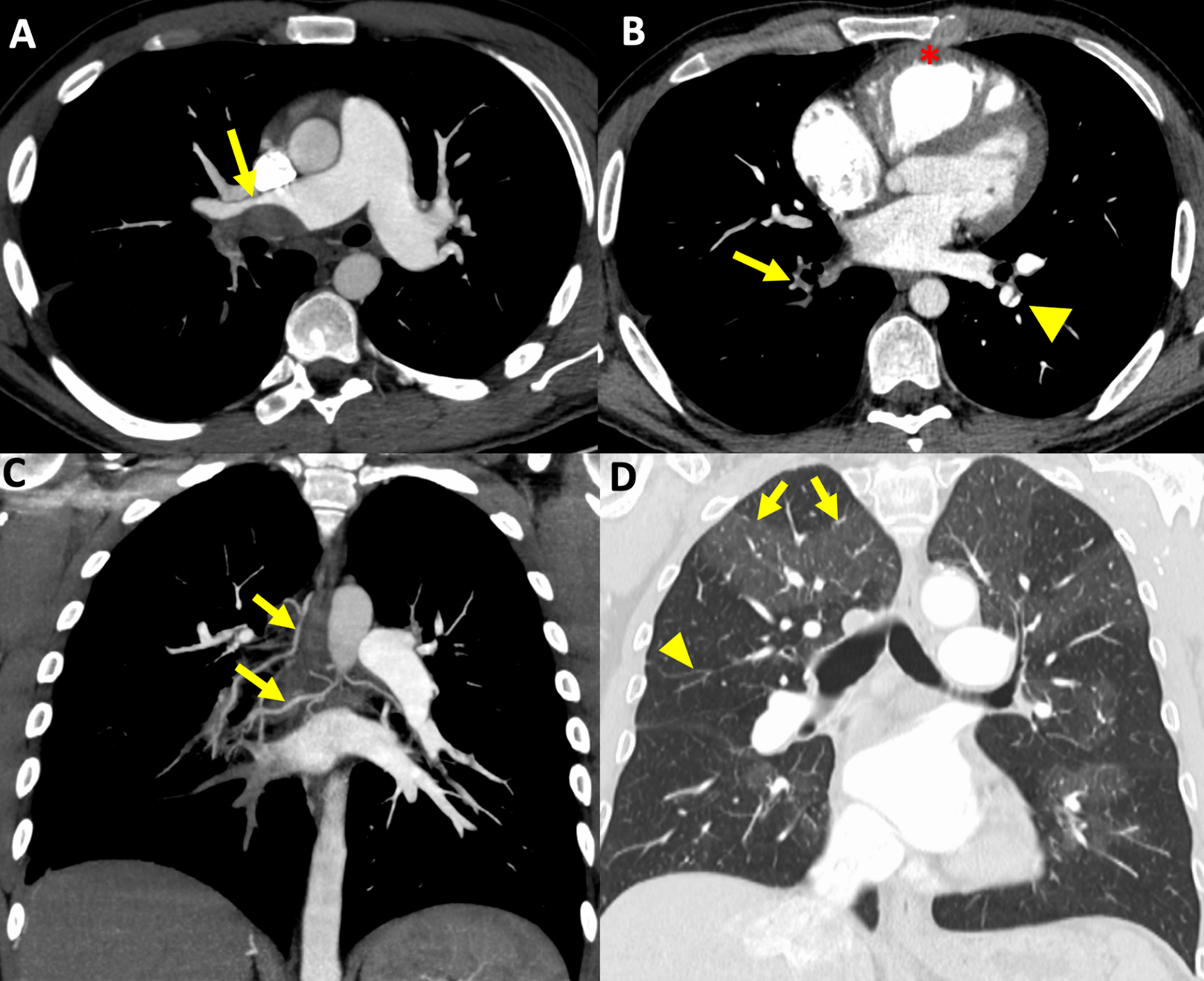
Patients with poor cardiac output, right heart failure and/or increased pulmonary arterial resistance are unable to pump IV contrast through the heart and lungs at a normal rate. 6 In these patients, even if contrast in the main pulmonary artery reaches a concentration above 300 HU, the peripheral pulmonary arteries may be poorly opacified mimicking acute pulmonary emboli (Figure 3). This can result in relatively symmetric unopacified vessels, or, when there is underlying lung disease or atelectasis, focal poor opacification due to delayed and reduced perfusion to involved segments (Figure 4). 7 Radiologists can inspect the pulmonary veins for clues. If there is no contrast in the pulmonary veins, it is possible that apparent filling defects reflect poor right heart output (Figure 3C). Asymmetric delayed enhancement in one pulmonary vein raises the possibility of local hypoxic vasoconstriction secondary to underlying lung disease, for example, in fibrosis. In these situations, the pulmonary arteries cannot be adequately assessed. Ideally, scan parameters are adjusted prior to imaging patients with known right heart disease or pulmonary hypertension. By delaying the scan start time by 2 to 4 seconds, the peripheral pulmonary arteries will be better opacified, and occasionally longer scan delays may be required to achieve optimal contrast opacification of small subsegmental arteries (Figure 3D-F). Some authors suggest using the test bolus technique for a patient with known poor right heart function. 8
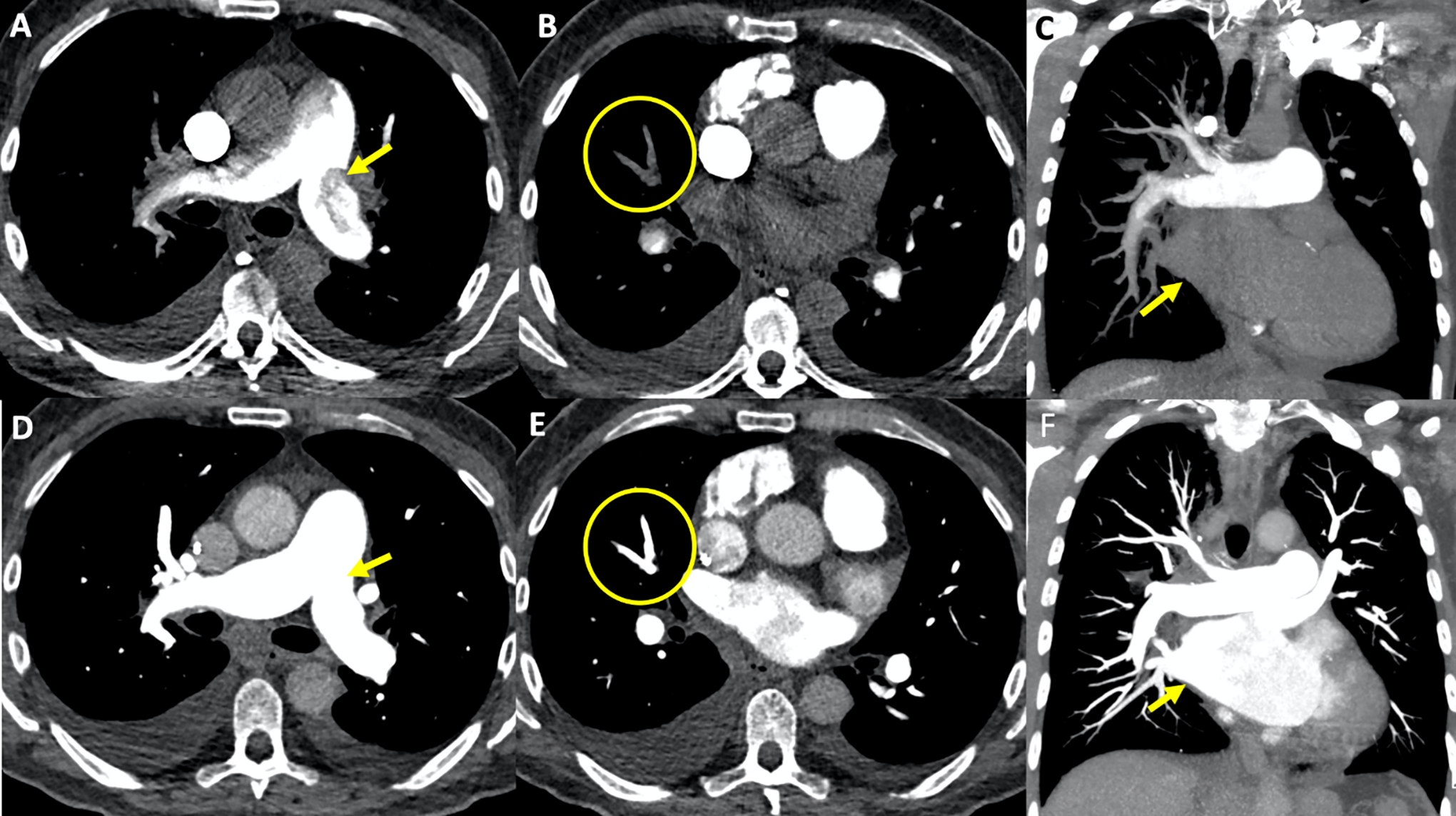
CTPA performed “too early” in a patient with severe pulmonary hypertension. A, Axial image, mediastinal window, demonstrates excellent contrast opacification in the main pulmonary artery (density over 600 HU) but this is inhomogeneous due to slow flow and mixing artifact with unopacified blood (arrow) concerning for acute pulmonary emboli. B, Axial image, mediastinal window, reveals poor opacification of the segmental arteries in the right middle lobe (circle). C, Note the absence of contrast in the left atrium/pulmonary veins, on the coronal reformat (arrow) confirming image acquisition was obtained too early after contrast injection. D, Repeat examination with increased trigger delay by 4 seconds shows excellent opacification of the pulmonary arterial tree (arrow). E, Note the absence of pulmonary emboli in the right middle lobe (circle). F, The coronal reformat depicts opacified left atrium/pulmonary veins confirming adequate timing of image acquisition (arrow).
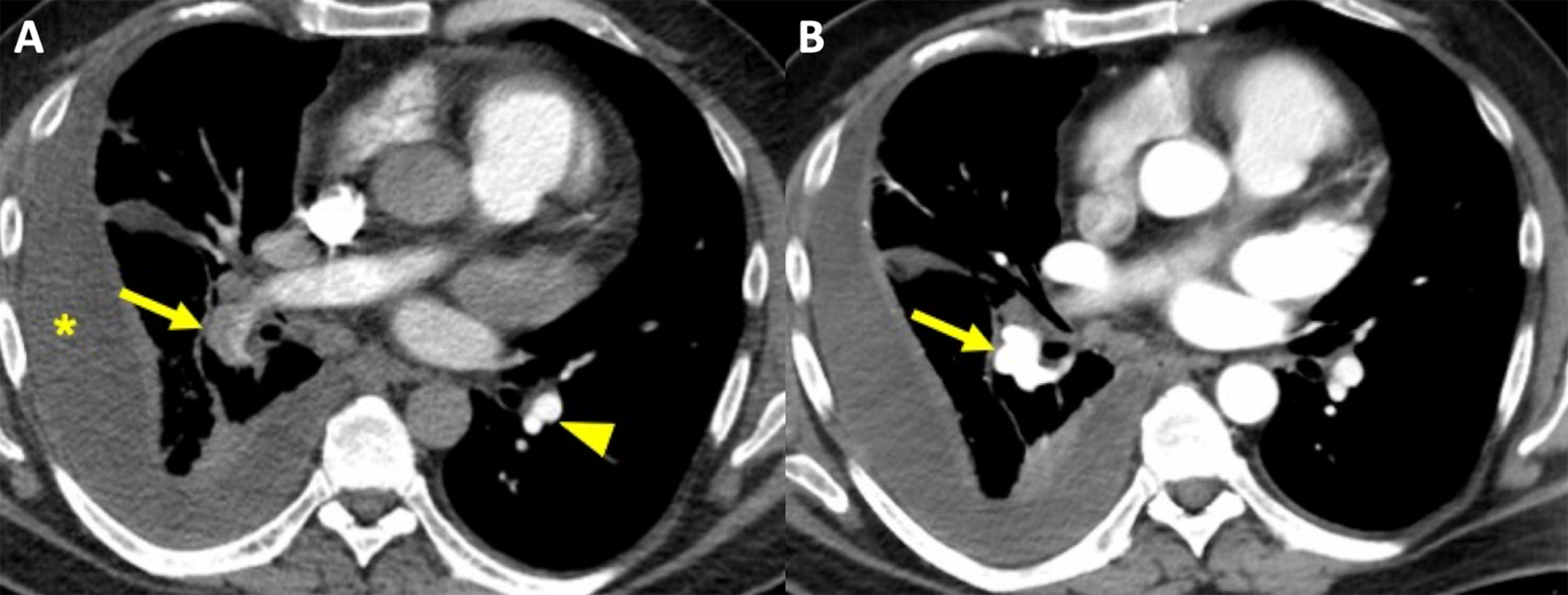
52-year-old man with a right empyema and unilateral increased pulmonary vascular resistance. A, Axial CTPA image, mediastinal reconstruction demonstrates an apparent filling defect in the right lower lobe pulmonary artery (arrow). Note the excellent opacification of the left lower lobe segmental pulmonary arteries (arrowhead). There is a loculated right pleural effusion (*). B, Repeat CTPA with a 4-second longer delay before the start of imaging acquisition reveals excellent opacification of the right lower lobe pulmonary artery and the absence of an embolus (arrow).
Scanning Too Late
Scanning after the contrast bolus has passed completely through the pulmonary arteries is uncommon. In some patients with extremely high cardiac output, it is possible for contrast to move through the pulmonary arteries prior to the scan start (Figure 5). In this situation, there will be no or little IV contrast in the SVC. “Missing the bolus” is more likely to occur when IV contrast is administered at a high volume per second but for a short duration. An alternate explanation is that the CT has been mistakenly performed to optimize contrast in the aorta rather than the pulmonary arteries. Always ensure the technologist has correctly identified the main pulmonary artery and not confused it with the aorta. In CTPAs performed with bolus tracking, placing the region of interest at the aorta, rather than the main pulmonary artery, will result in a suboptimal exam.
CTPA performed late, “missed bolus” in a 44-year-old woman with post-operative tachycardia. Contrast was injected through a right internal jugular central line. A, Axial image, mediastinal window, demonstrates poor contrast in the main pulmonary artery (<200 HU) (arrow) but high-density contrast in the aorta. The right atrium and right ventricle (not shown) also demonstrated very little contrast enhancement. Poor contrast opacification in this case is secondary to high cardiac output and injection through the central line. B, Axial image, mediastinal window, after a second injection with a 2-second shorter trigger delay shows much better pulmonary arterial contrast opacification (arrow).
Motion, Signal to Noise, Beam Hardening
Causes of false positive PE examinations can include partial volume averaging effects due to motion (breathing and cardiac), beam-hardening attenuation artifact from high density adjacent structures, poor image quality due to decreased signal to noise, and confusion of the pulmonary artery with venous structures and mucus filled bronchi.
Motion Artifact
The most common cause of misdiagnosis of pulmonary embolism, and the most common cause of equivocal studies, is motion artifact due to breathing, accounting for 42.2-50% of cases.9,10 Respiratory motion during a scan results in partial volume averaging between the opacified vessel and the lung which can simulate a filling defect.
Breathing artifact can be identified on lung windows by the presence of composite images of the vessels, known as the “seagull” artifact (Figure 6). On soft tissue windows, stair step artifact and rapid changes in the position of the vessels on contiguous slices can be seen. 11 To reduce breathing artifact, supplemental oxygen can be administered in patients with dyspnea. 12
85-year-old woman presents with acute shortness of breath and tachycardia. A, Axial CTPA image, mediastinal reconstruction depicts an apparent filling defect in a segmental right lower lobe pulmonary artery (arrow). B, Note the blurred appearance of the small vessels on the lung reconstruction at the same level with the typical “seagull” sign of breathing artifact (arrow).
Another cause of motion artifact which can result in misdiagnosis is cardiac pulsatility motion artifact, which can be seen in areas of the lung adjacent to the heart, most commonly in the lingula and paracardiac lower lobes.
Beam-Hardening Artifact
Beam hardening attenuation artifact from high density structures is the second most common cause of misdiagnosis of pulmonary embolism. 9 This is most commonly caused by pooled contrast agent in the SVC or adjacent vessels, metallic structures such as pacemakers, or by the patient’s arms if they are placed down by the patient’s side.
This artifact can be identified by its proximity to a high-density structure, its radial pattern from the source of the artifact and the identification of the artifact in other adjacent structures.9,11 In addition, regions of low attenuation due to streak artifact will form indistinct borders with the contrast in the vessel and have much higher densities (>78 HU) than true thrombus (Figure 7). 11
Axial CTPA image, mediastinal window, in a 51-year-old man reveals apparent filling defects at the take-off of the right upper lobe pulmonary artery (arrow) due to dense contrast in the SVC. Note the radial pattern of the artifact from its source in the adjacent ascending aorta (arrowhead).
Streak artifact from high-density contrast material in the superior vena and right sided cardiac chambers can be reduced by using a saline bolus immediately after the contrast material injection. 12 Streak artifact due to metallic implants may require additional imaging with V/Q scintigraphy.
Decreased Signal to Noise
Images obtained in large patients have more quantum mottle with increased image noise, which can limit the evaluation of segmental and subsegmental vessels, resulting in indeterminate studies or misdiagnosis of pulmonary embolism,2,11 Small pulmonary emboli can be obscured in scans with a large amount of noise. Apparent filling defects, which could result in misdiagnosis of PE, will appear ill-defined in comparison to a true embolus (Figure 8).
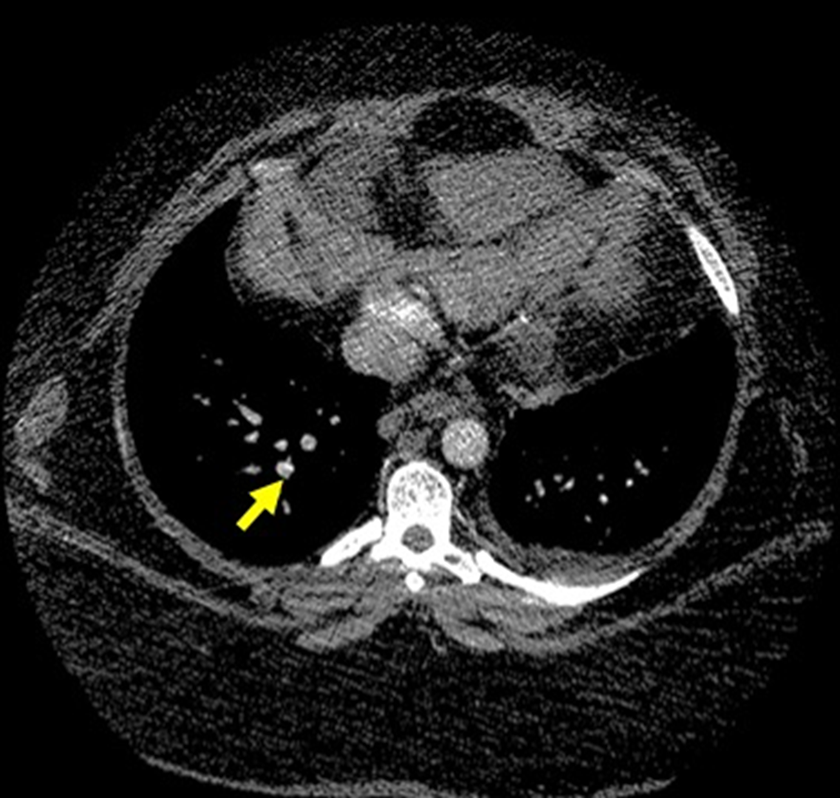
Axial CTPA image, mediastinal window, in a 41-year-old woman with a body mass index of 55. The study is indeterminate for acute pulmonary emboli due to excessive image noise in the subsegmental arteries in the right lower lobe (arrow).
Obesity has been noted to be a cause of non-diagnostic CTPA examinations in several studies, 2 with higher weight shown to be a predictor of indeterminate studies.
Increasing the dose can help to compensate for the increased noise from patients with a large body habitus. Although kVp can be increased as high as 140, multiple studies have shown that 120 kVp is adequate for most obese patients. 13 Increasing the mAs will also decrease noise, but at the cost of increasing radiation dose to the patient. The use of automatic tube current modulation software permits automatic adjustment of the tube current according to patient size and can help to optimize image quality without excess radiation exposure. Slowing gantry rotation and lowering the pitch can also be helpful in reducing image noise, however these modifications come at a cost of increasing risk of motion artifact and increased radiation dose. 13
The use of iterative reconstruction in this patient population can be useful to improve image quality while minimizing radiation dose. 14
Diagnostic Pitfalls
Normal Anatomical Pitfalls
Unopacified pulmonary veins and mucus-filled bronchi can potentially be a source of misdiagnosis. If image acquisition is performed too soon after the start of contrast injection, unopacified pulmonary veins can be mistaken for arteries containing filling defects. 11 It is important to follow these vessels back to the hilum to differentiate arteries from veins. The veins will terminate in the left atrium. Another mimicker of PE is a mucus plug within a bronchus (Figure 9). Careful review of contiguous images and adjacent anatomical structures can easily prevent this diagnostic pitfall. 9
72-year-old woman with acute shortness of breath and tachycardia, 3-days post knee replacement with mucoid impaction/aspiration. A, Axial CTPA image, mediastinal window, shows filling defects in the right lower lobe (arrow). B, Axial CTPA image, lung reconstruction at the same level depicts patent bronchi in the left lower lobe (arrowheads) and the absence of aerated bronchi in the right lower lobe (arrows). Note that bronchi are internal to pulmonary arteries (*) in the lower lobes. C, Axial CTPA image, mediastinal reconstruction at the level of the bronchus intermedius shows a low-density filling defect (arrow) in the bronchus. D, Axial CTPA image, lung reconstruction, demonstrates gas in the non-dependent subtotally occluded bronchus intermedius (arrow) confirming mucoid impaction/aspiration as the cause of the patient’s symptoms.
Post-surgical Pitfalls
The Fontan procedure is performed in patients with complex congenital heart disease and directs the flow of systemic blood to the pulmonary arterial system without traversing a ventricle. There are many variations of the procedure but many involve an end-to-side anastomosis between the superior vena cava (SVC) and the right pulmonary artery (RPA). Directing blood flow from the inferior vena cava (IVC) to the lungs is achieved either by connecting the right atrium to the RPA, or by constructing an intra-atrial or extracardiac conduit from the IVC to the RPA. 15
Patients with a Fontan circulation are at increased risk of venous thromboembolism. In fact, this is the most common cause of out-of-hospital death. 15
CTPA contrast injection and the timing of image acquisition must be altered in these patients in order to avoid a false diagnosis of massive pulmonary embolism (Figure 10) or a non-diagnostic study. Some authors have advocated a dual-injection technique into a right arm vein and a lower extremity vein with early and late imaging acquisition. However, scanning at a fixed delay of 90 seconds after a single arm-vein injection of 150 ml iodinated contrast (370 mg/ml) at 3 ml/sec avoids mixing artifact and allows homogeneous opacification to evaluate for acute pulmonary embolism as well as thrombi in the Fontan circuit (Figure 11). 16
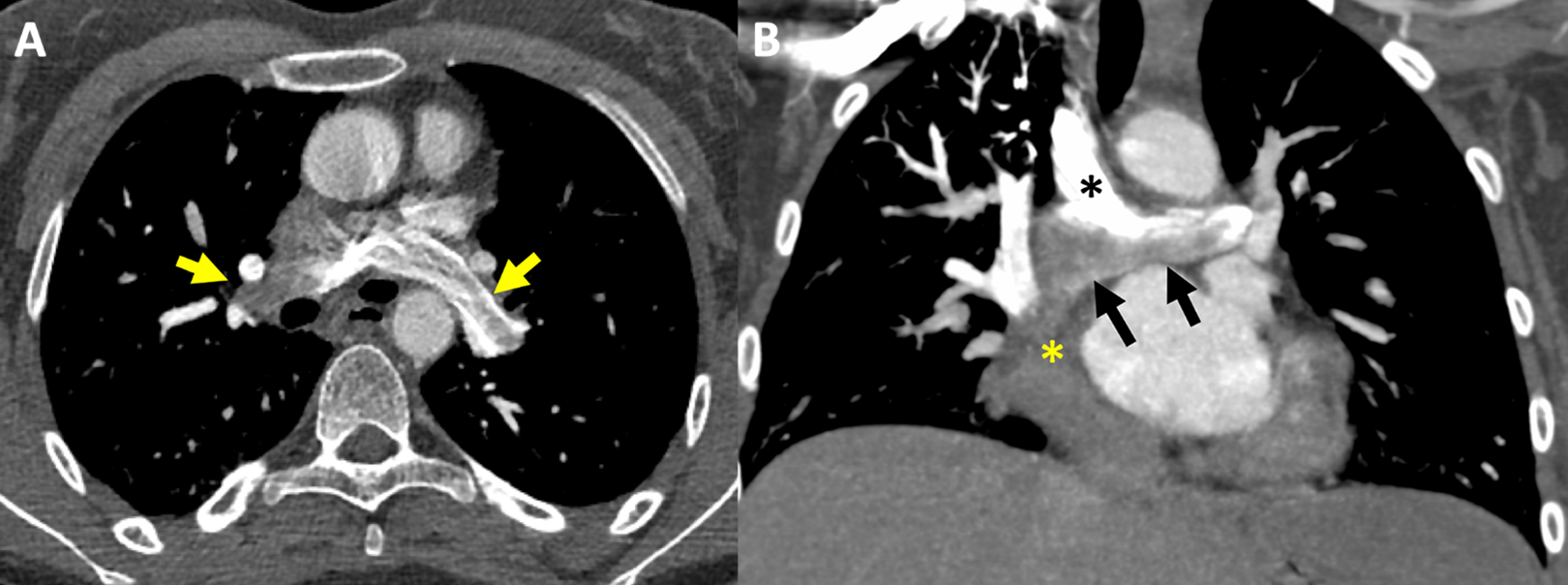
21-year-old woman with prior classical Fontan procedure and suspected acute PE. A, Axial CTPA image, mediastinal window, shows apparent filling defects in the right and left pulmonary arteries (arrows). B, 3 mm coronal MIP in the same patient depicts dense contrast in the SVC (black *) opacifying the right and left pulmonary arteries, mixing with unopacified blood (arrows) entering the inferior aspect of the RPA from the right atrium (yellow *).
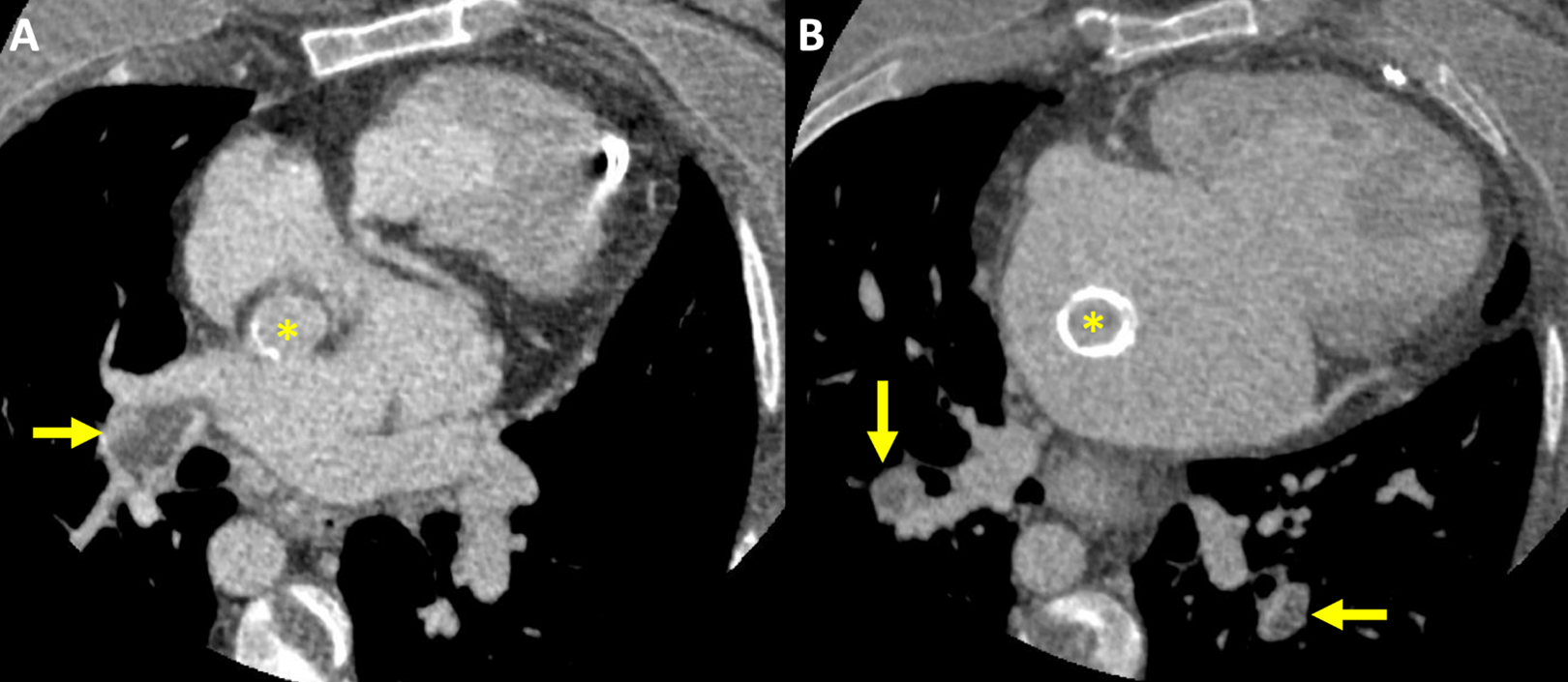
34-year-old woman, 1-week post-partum with a history of lateral Fontan connection. A, Axial CTPA, mediastinal window post-injection of 150 ml iodinated contrast and a fixed 90 second delay before image acquisition reveals a filling defect in the right lower lobe pulmonary artery. Note the homogenous opacification of the intra-atrial conduit (*) from the IVC to the pulmonary circulation. B, Axial CTPA image in the same patient shows calcification of the conduit (*) and pulmonary emboli in the segmental lower lobe pulmonary arteries.
Differential Diagnosis
Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
For unclear reasons, 1-4% of patients with acute PE do not recover completely. The emboli are incorporated into the wall of the pulmonary arteries leading to vessel stenosis and occlusion with the subsequent development of pulmonary hypertension. It is important for imagers to differentiate acute from chronic thromboembolic disease as the latter is generally treated with surgical thromboendarterectomy rather than anticoagulation alone. The prognosis without appropriate therapy is extremely poor. There is often a significant delay in diagnosis in these patients due to lack of awareness in the imaging community.
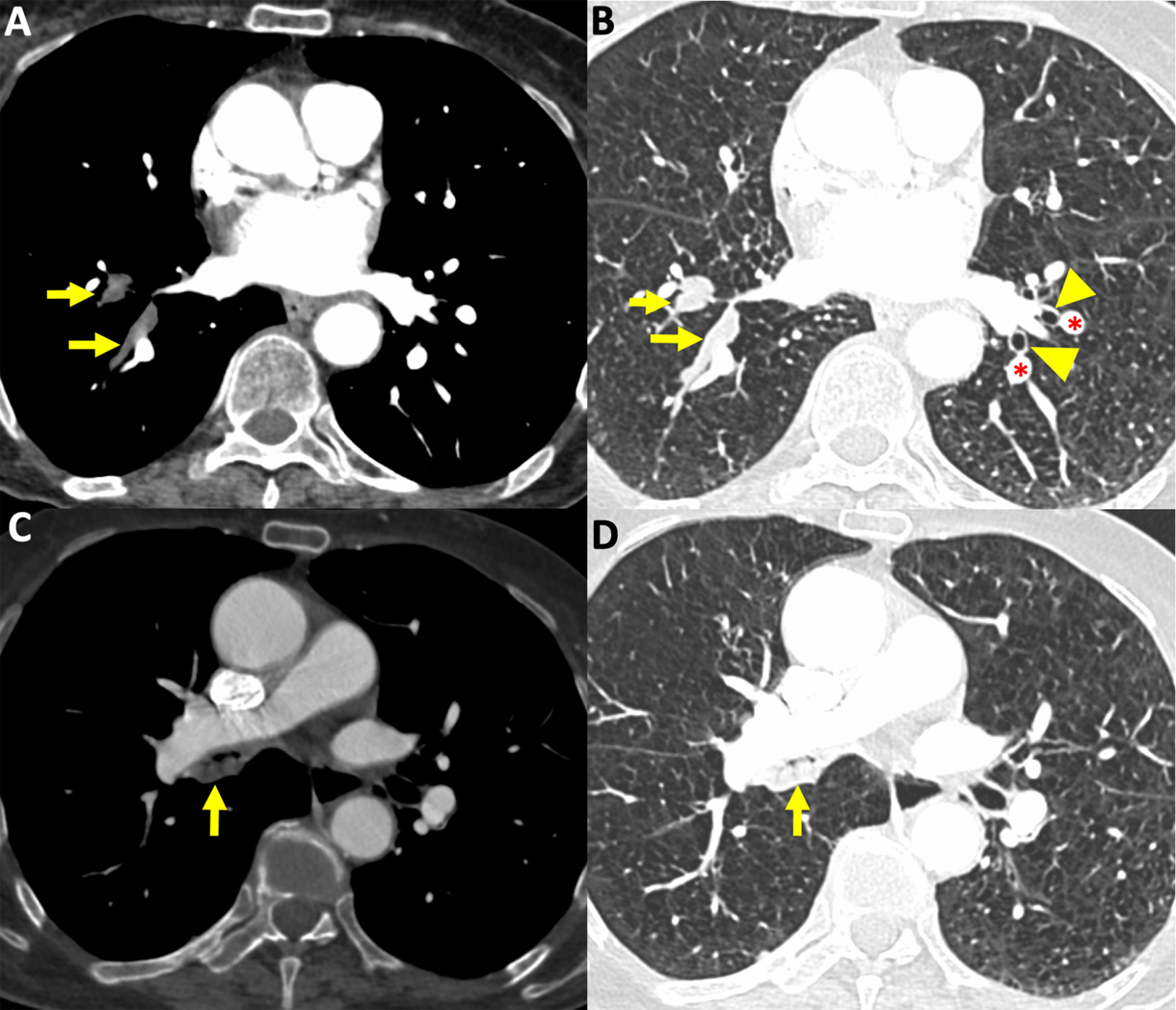
CTPA findings of CTEPH include the generic findings of pulmonary hypertension such as dilatation of the main pulmonary artery, right chamber dilatation and right ventricular hypertrophy. The pulmonary arterial findings are more specific and include eccentric mural filling defects (Figure 12A) that may be calcified. These differ from the central filling defects within a distended lumen seen in acute PE. Other findings include abrupt vascular occlusion with rapid tapering of the occluded artery distal to the occlusion as well as intraluminal webs (Figure 12B), bands and focal stenosis. Other suggestive findings include dilated bronchial artery collaterals (Figure 12C) and a mosaic pattern of attenuation on lung reconstructions (Figure 12D). It is especially important to raise the possibility of chronic PE in this setting to ensure prompt diagnosis and treatment. Note that some patients with well-established CTEPH may present with superimposed acute PE. 17
25-year-old-man with increasing shortness of breath. A, 5-mm axial MIP image, mediastinal window, depicts a mural filling defect (arrow) in the distal right pulmonary artery forming obtuse angles with the vessel wall. B, Axial image, mediastinal window, demonstrates a diminutive, completely occluded right lower lobe pulmonary artery (arrow) as well as a web in a segmental artery in the left lower lobe (arrowhead). Note the right ventricular hypertrophy (*) and dilatation as a sign of chronic pulmonary hypertension. C, 5-mm coronal MIP reconstruction, mediastinal window, reveals bronchial artery collaterals. D, Coronal reformat, lung reconstruction, in a different patient with CTEPH shows a mosaic attenuation pattern. Note the larger vessels within the areas of higher lung attenuation (arrows) and the smaller vessels (arrowhead) in areas of low attenuation due to vascular obstruction.
Primary Pulmonary Artery Sarcoma
Pulmonary artery sarcoma is a rare tumor that arises from the vascular endothelium. It results in an intraluminal filling defect that expands the vessel and eventually invades surrounding structures. Patients often present with advanced disease as they remain asymptomatic until vessel occlusion occurs. Presenting symptoms may mimic acute pulmonary emboli with dyspnea and chest pain being the most common. However, in contrast to acute PE, the duration of symptoms is longer than 100 days. Prognosis is poor with a median survival of 17 months. 18
Pulmonary artery sarcoma is often diagnosed in retrospect after “massive PE” fails to resolve or increases in size and extent despite appropriate anticoagulation (Figure 13). Suggestive CT findings include a filling defect occupying an entire central pulmonary artery and one of its branches (Figure 13A and B), heterogeneous and delayed enhancement of the lesion, a globular appearance, and the presence of lung metastases (Figure 13B). 18F-FDG-PET/CT (Figure 13C) or MRI with delayed gadolinium sequences can be diagnostic. 19
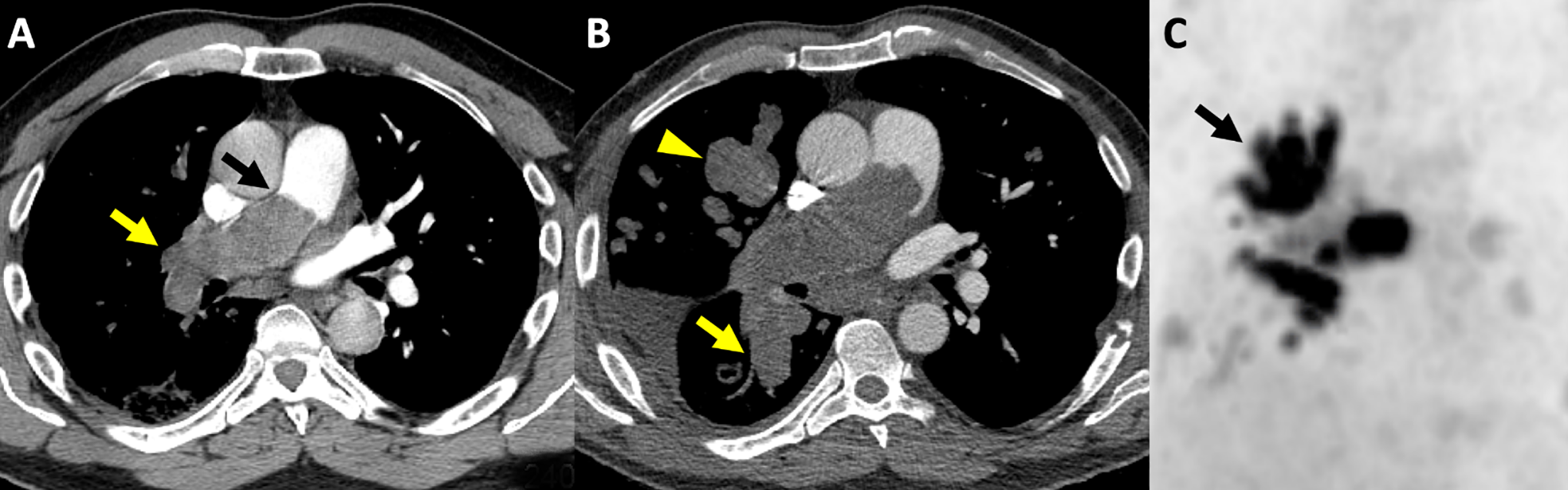
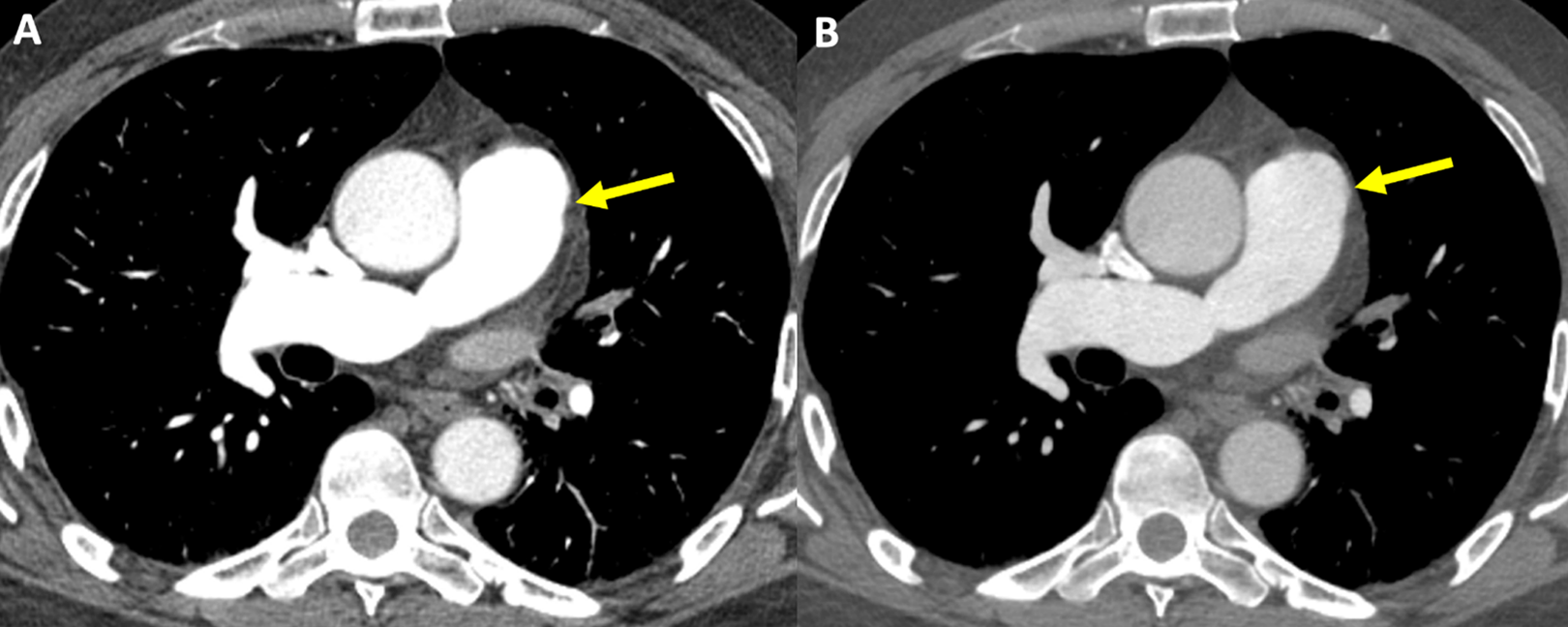
48-year-old man with increasing shortness of breath and chest pain. A, Axial CTPA image, mediastinal window, at presentation shows a large filling defect occluding and distending the right pulmonary artery and extending into the right interlobar artery. B, Axial CTPA image, mediastinal window, 2 months later reveals interval growth of the occlusive filling defect (yellow arrow) with a globular mass-like appearance extending into the main pulmonary artery (black arrow). Pulmonary metastases have also developed (arrowhead). C, 18F-FDG PET shows increase uptake in the tumor with a branching pattern extending into the right upper lobe. (arrow).
Peripheral Tumor Emboli
Tumor emboli are usually located in small and medium-sized arteries. Suggestive CT findings include multifocal dilatation or beading of subsegmental pulmonary arteries (Figure 14) that may be associated with peripheral wedge-shaped areas of consolidation and ground-glass due to hemorrhage or infarction. Rarely, they involve more proximal vessels. They are most commonly seen in patients with hepatoma, renal, gastric, breast, prostate and choriocarcinoma. PET/CT may be helpful to differentiate these from bland emboli. 20
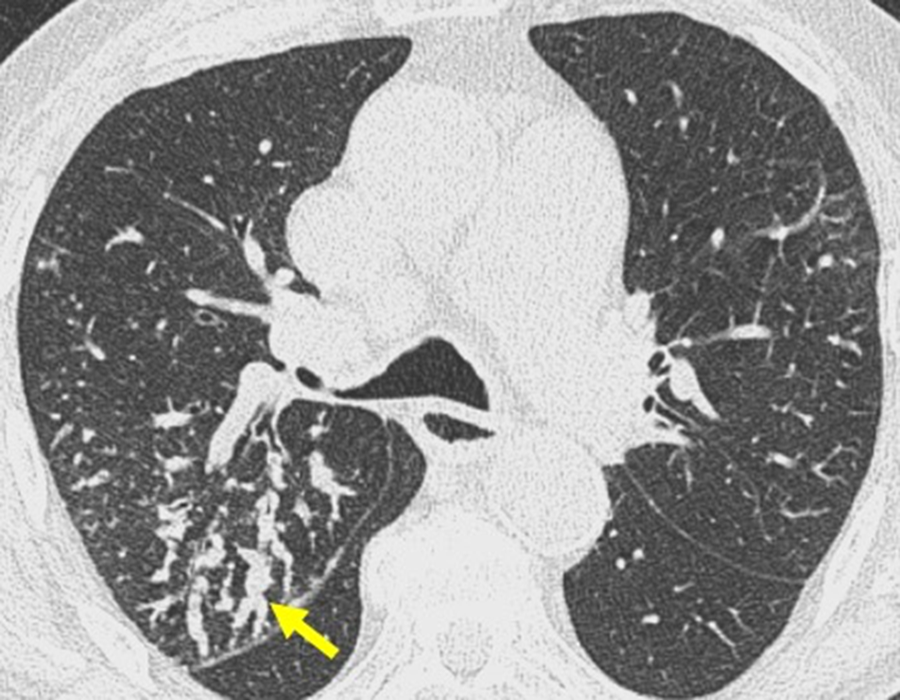
82-year-old man with advanced bladder cancer. Axial CT, lung reconstruction shows extensive beading of the subsegmental pulmonary arteries (arrow) in the posterior segment of the right upper lobe indicating endovascular metastases.
Pulmonary Artery Vasculitis
Reports of pulmonary artery involvement in Takayasu arteritis range between 14.3 to 86% in the literature. Involvement is often subclinical. It has also been seen in patients with giant cell arteritis and Behçet’s disease, although Behçet’s usually causes pulmonary artery aneurysms rather than stenosis. On imaging, the main differential for vasculitis is chronic rather than acute PE. CTPA reveals thickening of the pulmonary arterial wall and contrast enhancement in the acute inflammatory phase followed by luminal stenosis ± mural calcification in the chronic phase. As compared with chronic PE and acute PE abutting the arterial wall, the mural thickening is circumferential (Figure 15) as opposed to eccentric. It is important to carefully inspect the systemic arteries in these cases to correctly identify systemic vasculitis as the cause of the imaging abnormalities. PET/CT and MRI with gadolinium enhancement can confirm the diagnosis.
23-year-old woman with shortness of breath and fever. Axial contrast-enhanced CT, mediastinal window depicts mural thickening of the left interlobar artery (arrow). Note the thickening of the wall of the ascending and descending aorta (arrowheads) as a sign of systemic large vessel vasculitis. She was subsequently diagnosed with Takayasu arteritis and responded to steroid treatment.
In Situ Pulmonary Artery Thrombosis
In situ thrombosis has been reported in chronic obstructive pulmonary disease and asthma exacerbations, post-trauma, especially gunshot wounds, during a sickle cell crisis and secondary to a severe viral infection, most recently COVID-19. It should be suspected in these clinical settings when there are pulmonary arterial filling defects on CTPA, in the absence of deep venous thrombosis. 21
In situ pulmonary artery thrombosis can also develop in patients with severe pulmonary arterial hypertension (Figure 16), especially in those with unrepaired left-to-right shunt. Anticoagulation is not indicated in these patients as it is unhelpful in reducing the size of the thrombus.
42-year-old man with unrepaired atrial septal defect and Eisenmenger syndrome presents with hemoptysis and in situ thrombosis. Axial CTPA image, mediastinal window, demonstrates dilated central pulmonary arteries and mural calcification (arrowhead) and thrombus (arrow) along the right interlobar artery. Peripheral pulmonary arteries were dilated and all patent.
Pulmonary Artery Stump Thrombosis
Venous thromboembolism (VTE) after oncologic lung surgery has been reported in 5.3-7.4% of patients. Vascular stump thrombosis has a different etiology. It has been postulated to occur due to hypercoagulability, endothelial injury during surgery or because of stagnant blood flow at the end of a vascular stump.
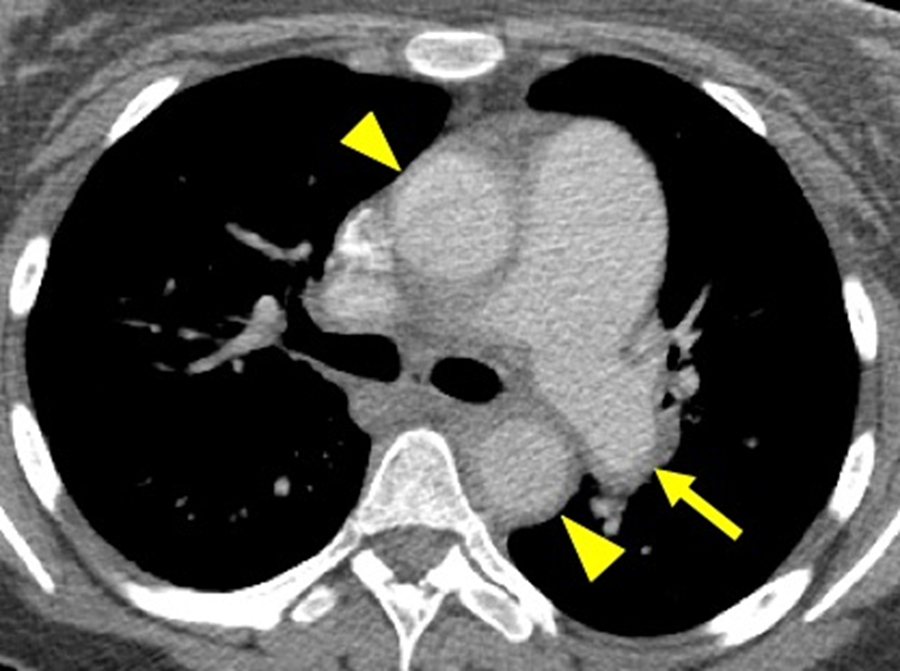
The incidence of vascular stump thrombosis has been reported in 3-4% of patients post-lobectomy and 12% after pneumonectomy. There is no consensus concerning stump thrombosis management. Some have recommended systemic anticoagulation if the thrombus has a convex margin and, observation if the shape is concave as this is felt to have a more benign behavior with a low risk of embolization. Regardless, the finding of a stump thrombus on CTPA (Figure 17) should be communicated to the referring physician when detected, keeping in mind that it generally has a different etiology than VTE. 22
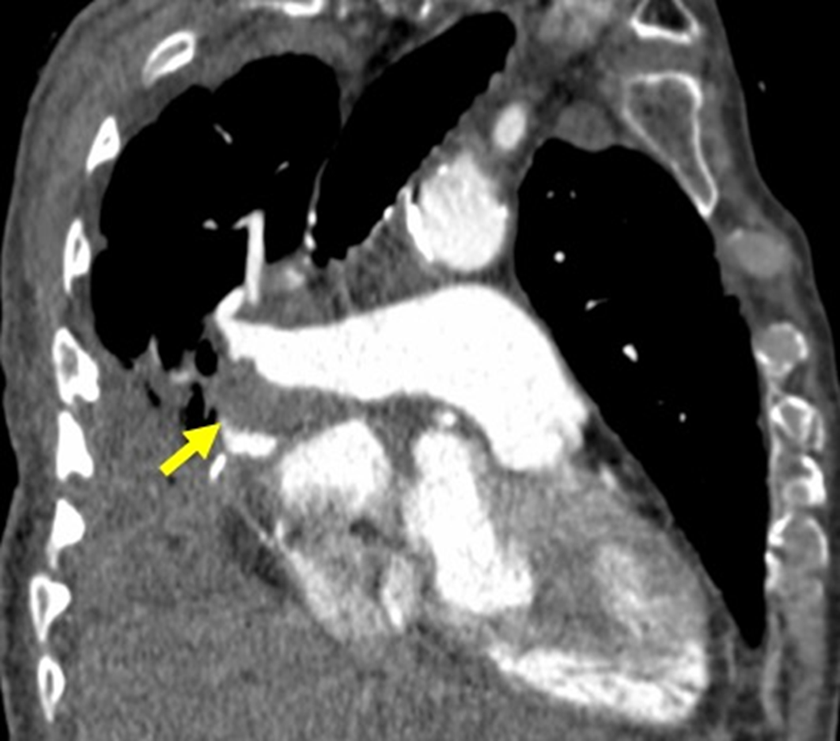
81-year-old man post right middle and lower lobectomy followed by radiation for non-small cell lung cancer. 5-mm coronal oblique MIP image, mediastinal window, reveals a mural filling defect (arrow) with concave upper margin lining the inferior aspect of the right and interlobar pulmonary artery stump.
Dual Energy CT for Acute Pulmonary Embolism Assessment
Dual energy CT (DECT) applications have been developed over the last decade and are now utilized for detection and characterization of many disease processes, including pulmonary embolism.23,24
The basic principles of DECT are focused on the ability to image a patient with photons derived from 2 different applied tube potentials. There are vendor specific differences with regard to how this is achieved, but the result is the same—the ability to create virtual monochromatic images and to perform material decomposition (i.e., creation of water, calcium, or iodine only images). 25
Virtual monochromatic image formation is performed from DECT datasets allowing the creation of either high or low kilovoltage images. The higher kilovoltage images (i.e., 90 keV) emulate imaging with a high tube potential, and provide images with lower noise, but also less contrast resolution. The lower kilovoltage images (i.e., 50 keV) emulate imaging with a lower tube potential, closer to the k-edge of iodine. For post contrast studies, this is beneficial as photoelectric absorption is optimized and iodine containing structures have increased attenuation, 26 improving contrast resolution.
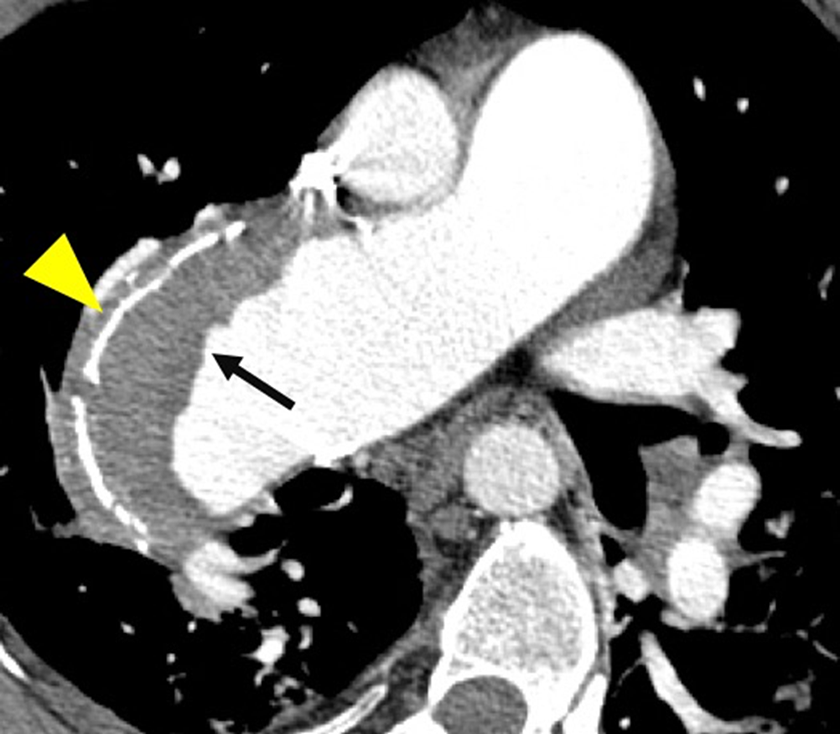
Low keV virtual monochromatic images for detection of pulmonary emboli have the benefit of increased contrast resolution (the iodinated blood pool becomes disproportionally bright based on the assumption of Compton scatter alone) between clot and contrast-enhanced blood pool. This technique can be useful in situations in which limiting contrast volume is warranted, such as in patients with diminished renal function (Figure 18). Low keV monochromatic images can also be of use in patients with Fontan circulation. 27 The differences in blood volume attenuation and clot are lessened in such patients, but creation of a low keV monochromatic datasets can help in this setting. The use of low volumes of IV contrast for pulmonary emboli detection has shown promise. 28 However, caution when using this application needs to be undertaken as low keV virtual monochromatic images can have higher image noise than standard 120 kVp CT studies.
Dual energy CTPA in a 45-year-old man with reduced renal function. A, Axial image performed with low contrast volume (40cc) viewed at window width 800 and window level of 50. Note the relative increased attenuation of the main pulmonary artery on the 50 keV monochromatic energy image (arrow). B, Compare this to the relative decreased attenuation of the main pulmonary artery on the 70 keV axial image (arrow).
The ability to perform material decomposition is the other major capability of dual energy imaging. The 2 different applied tube potentials allow decomposition of images into 2 base tissues/materials, provided the atomic number (Z) of these tissues is different. Material decomposition in the human body allows decomposition of soft tissue from bone and other calcium (Z = 20) containing structures (such as gout crystals). 29 In the setting of assessment for pulmonary emboli, the creation of iodine (Z = 53) only images are the focus of this technique. These “iodine maps” correspond to lung blood volume seen with planar scintigraphy and single photon emission CT.30,31 The iodine maps are viewed in conjunction with the anatomic images. This is done to help differentiate wedge-shaped iodine map defects secondary to pulmonary emboli (by assessment for pulmonary artery filling defects) versus other reasons for diminished iodine content such as consolidation, atelectasis, mass or pleural fluid to name a few (Figure 19). 32
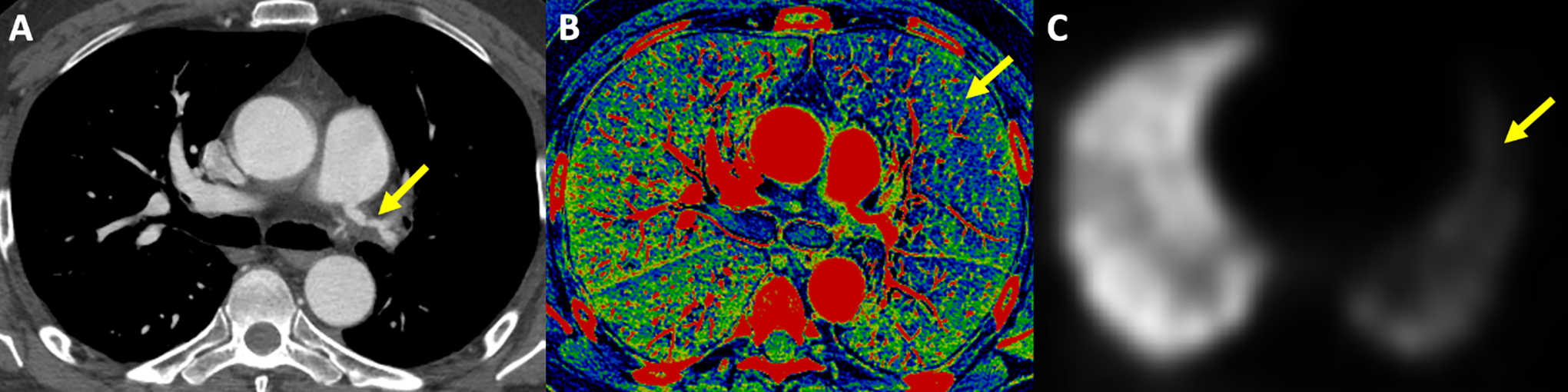
49-year-old man with Takayasu arteritis and involvement of the left pulmonary artery. A, CTPA axial image demonstrates marked narrowing and irregular mural thickening of the left pulmonary artery (arrow). B, An iodine map/iodine only image shows diminished perfusion/iodine content (more blue) throughout the left lung (arrow). C, This is confirmed on a perfusion SPECT nuclear medicine image (arrow).
Studies assessing the performance and incremental benefit of iodine maps for detection of pulmonary emboli are often inherently limited by the lack of an accepted gold standard, different from the CT pulmonary angiogram itself and variable prevalence of acute PE in the study populations. 33
A recent meta-analysis based upon 7 studies did indicate that DECT for detection of pulmonary emboli had a high pooled positive likelihood ratio (PLR) suggesting the importance of DECT as a prevalence independent rule-in test. 33 Although the outcome benefit on a patient and population level given the already excellent sensitivity of CTPA for PE detection, and the controversies surrounding management of asymptomatic subsegmental emboli remains unclear. 34
In summary, dual energy CT can be a useful tool in the evaluation of acute pulmonary emboli. The use of low kilovoltage monochromatic energy images can help to accentuate contrast attenuation and is potentially useful with low contrast volume scans, and in patients with altered hemodynamics. The role of material decomposition and iodine maps in this setting remains unclear but may help to increase sensitivity and specificity for detection of pulmonary emboli.
Conclusion
The objective of this guidance document is to provide current and practical recommendations on how to achieve high quality diagnostic CTPA studies while avoiding the most common technical and interpretation pitfalls. It is intended to remain relevant to radiologists and radiology departments nationwide and across a wide spectrum of health care practice settings. As new data emerges from ongoing and future research studies, we will revise the document accordingly.
Key Points
Understanding and avoiding the technical and image interpretation pitfalls is important to decrease mis- and overdiagnosis of acute PE and decrease the number of unnecessary repeat CTPAs that lead to increased patient radiation exposure.
Dual energy CT is an emerging technology that has a promising role in imaging of acute PE.
Footnotes
Appendix
Acknowledgment
We would like to thank Casey Hurrell for her valuable contributions in coordinating our work and preparing this guidance document.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EN—Nothing to declare. CH—Dr. Hague has received speaker fees from Boehringer Ingelheim. DM—Nothing to declare. BM—Nothing to declare. CS—Dr. Souza sits on an advisory board with AstraZeneca and Boehringer-Ingelheim. She has received consultant fees and honoraria from Pfizer, Boehringer-Ingelheim, AstraZeneca, and Hoffmann-La Roche. She has received an Educational Grant from Boehringer-Ingelheim. JT—Nothing to declare. CD-Nothing to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.