
Abstract
Pancreatic ductal carcinoma (PDAC) is one of the leading causes of cancer-related death worldwide. Computed tomography (CT) remains the primary imaging modality for diagnosis of PDAC. However, CT has limitations for early pancreatic tumor detection and tumor characterization so that it is currently challenged by magnetic resonance imaging. More recently, a particular attention has been given to radiomics for the characterization of pancreatic lesions using extraction and analysis of quantitative imaging features. In addition, radiomics has currently many applications that are developed in conjunction with artificial intelligence (AI) with the aim of better characterizing pancreatic lesions and providing a more precise assessment of tumor burden. This review article sums up recent advances in imaging of PDAC in the field of image/data acquisition, tumor detection, tumor characterization, treatment response evaluation, and preoperative planning. In addition, current applications of radiomics and AI in the field of PDAC are discussed.
Introduction
Pancreatic ductal carcinoma (PDAC) is the seventh leading cause of cancer-related death worldwide. 1 Despite substantial progress in the non-operative treatment of patients with PDAC, including knowledge of PDAC biology and advances in neoadjuvant therapies, complete surgical resection remains the only curative therapy for PDAC pending R0 resection. 2 Unfortunately, only 20% of patients with PDAC are candidates for surgical resection. 2 In addition, for patients deemed operable based on preoperative imaging, intraoperative findings often reveal unresectable disease or surgery does not always allow for R0 resection and especially for pancreatic head PDAC. 2 All these factors reinforce the need for more precise imaging techniques, and this applies to early detection, lesion characterization, preoperative assessment, risk stratification, and prediction of treatment outcome.
For many years, preoperative assessment of PDAC has been based on computed tomography (CT). In the mid 90s, the overall accuracy of helical CT for assessing resectability of PDAC was 70% 3 and rose to 90% more recently. 4 However, since CT has limitations for early pancreatic lesion detection and characterization, researchers have placed more hope on magnetic resonance imaging (MRI). 5 Recently, particular attention has been given to radiomics for the characterization of pancreatic lesions using extraction and analysis of quantitative imaging features that are beyond human visual perception.6-8 Radiomics is now considered as a useful tool for pancreatic lesion characterization and outcome prediction. 9 In addition, radiomics has currently many applications that are developed in conjunction with artificial intelligence (AI) with the aim of better characterizing pancreatic lesions and providing a more precise assessment of tumor burden. 9
The purpose of this article was to sum up recent advances in imaging of PDAC in the field of image/data acquisition, tumor detection, tumor characterization, treatment response evaluation, and preoperative planning.
Image and Data Acquisition
CT image quality has greatly benefited from advances in image reconstruction that were developed as a response to the use of low dose CT examination. 10 Iterative reconstruction algorithms such as hybrid or statistical iterative reconstruction algorithms, model-based iterative reconstruction algorithms, and deep-learning based algorithms are now commonly used to improve image quality. 10 Lyu et al have assessed both diagnostic performance and reader confidence for prediction of margin-negative resection (i.e., R0 margins) in PDAC with CT images reconstructed using a deep learning image reconstruction (DLIR) algorithm. 11 They compared CT images reconstructed using DLIR to those obtained with filtered back projection and hybrid model-based adaptive statistical iterative reconstruction (ASiR-V) 60%. 11 They found that DLIR at high strength levels allowed better prediction of margin-negative resections (i.e., R0 margins) with area under the curve (AUC) of 0.91, compared to filtered back projection (AUC = 0.75; P = .030) and ASiR-V (AUC = 0.81) (P = .023). 11 In addition, DLIR at high strength levels was associated with the highest interreader agreement and reader confidence. 11
Dual-energy CT allows calculation of iodine concentration in tissues, which represents the uptake of iodine in a region of interest and reflects blood supply in tissues. 12 Nagayama et al. reported that dual-layer spectral technology improves virtual monoenergetic image (VMI) quality in patients with PDAC. 13 They found that VMI at 40 keV resulted in lower image noise and better contrast-to noise ratio compared to conventional polyenergetic images along with equivalent or even better tumor conspicuity and peripancreatic vasculature assessment compared to conventional pancreatic parenchymal phase images. 13 Noda et al. found that greater PDAC conspicuity and better reproducibility of PDAC size measurement were obtained at lower energy levels (40 keV) using VMI with fast-voltage-switching dual-energy CT by comparison with those obtained at higher levels (45, 50, 55, 60, 65, 70, and 75 keV). 14 Moreover, data from dual-energy CT can be used for further radiomics analysis with encouraging results. 15
MRI has been subjected to major developments during recent years.
5
However, artifacts caused by physiologic motion in the abdomen, remain a major concern.
16
To overcome these limitations, the use of deep-learning based reconstruction with iterative denoising that provides abdominal MR images with increased sharpness, higher signal-to-noise ratio, and reduction of blurring artifacts shows great promise for the detection of small pancreatic lesions; but this would require further studies.16,17 It is admitted that MRI has major advantages over CT for the detection of hepatic metastases, pancreatic lesion characterization, and detection of isoattenuating PDAC (Figure 1).18,19 Diffusion-weighted MRI helps discriminate between PDAC and other conditions.
20
Intravoxel incoherent motion (IVIM) diffusion-weighted MRI is another research path for characterization of pancreatic tumors, with perfusion fraction (f) being a discriminating variable to differentiate PDAC from auto-immune pancreatitis (AIP) and from non-hypervascular pancreatic neuroendocrine tumors.21,22 IVIM can also be used to differentiate between poorly differentiated PDAC from well/moderately differentiated PDAC.
23
65-year-old woman with pancreatic ductal adenocarcinoma of the pancreatic head. (A) CT image obtained in the axial plane during the arterial phase of enhancement shows ill-defined lesion (arrow) of the pancreatic head. (B) CT obtained in the coronal plane during the arterial phase of enhancement shows ill-defined lesion of the pancreatic head (arrow). Of note, the main pancreatic duct (arrowhead) is seen, abutting pancreatic lesion. (C) Three-dimensional image obtained from CT data reveals right replaced hepatic artery (arrow). (D) T1-weighted MR image obtained in the axial plane during the arterial phase of enhancement shows well defined hypointense lesion (arrow) of the pancreatic head. (E) T1-weighted MR image obtained in the axial plane during the portal venous phase of enhancement shows less visible, hypointense lesion (arrow) of the pancreatic head. (F) Diffusion-weighted MR image obtained in the axial plane shows hyperintense lesion (arrow) of the pancreatic head, consistent with restricted diffusion. CT: computed tomography; MR: magnetic resonance.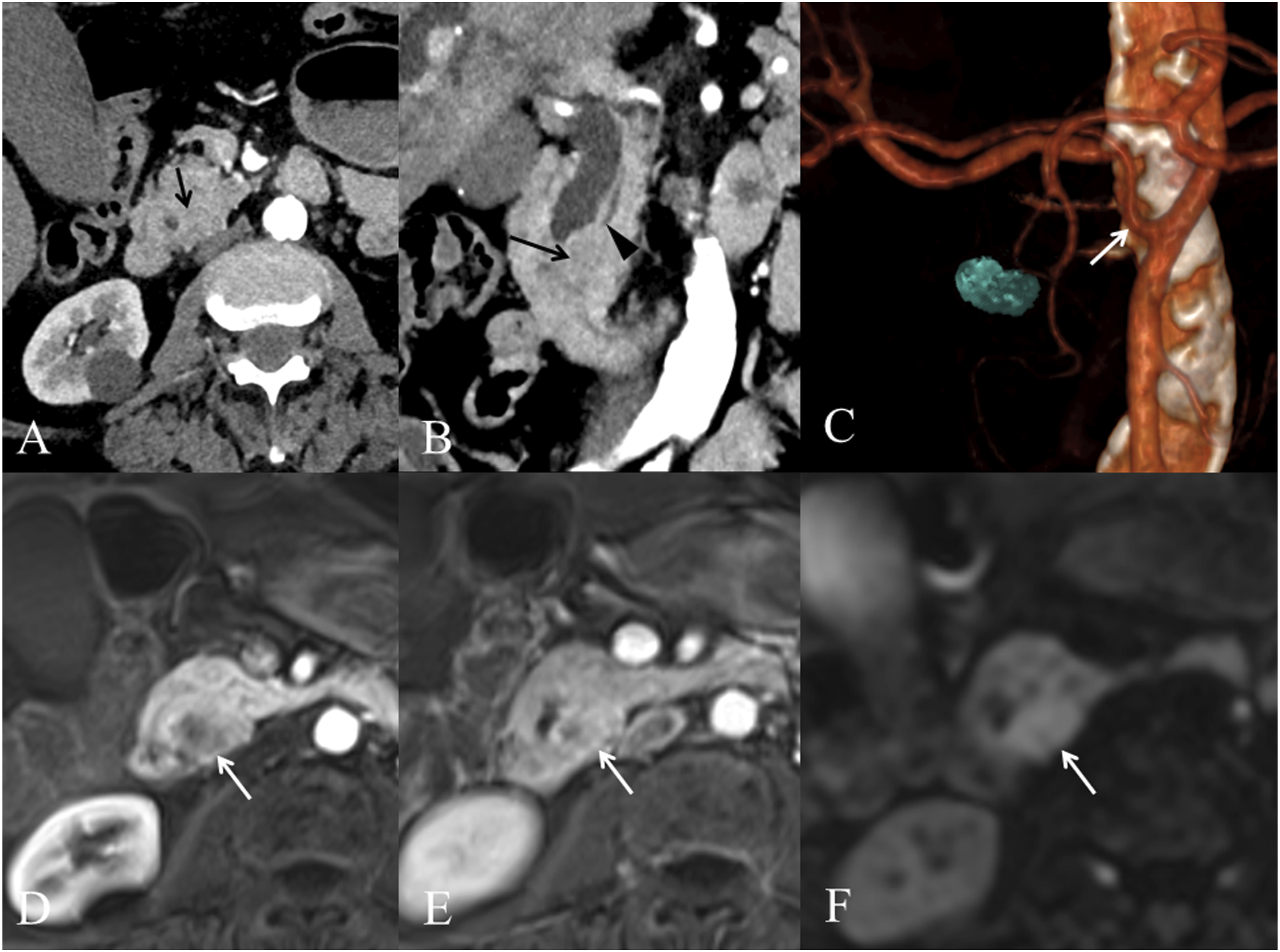
Radiomics often requires image segmentation as the initial post-processing step before radiomics feature extraction and model building can be performed. Image segmentation in the field of pancreas imaging remains a critical issue (Figure 2). Whereas major progress has been made for automatic segmentation of the whole pancreas,
24
fully automated and volumetric segmentation of pancreatic tumors is still challenging with insufficient similarity indexes or Dice scores.
25
Diagram shows the different steps of the process of building a radiomic or an artificial intelligence model to detect and/or classify a pancreatic lesion. In this example, computed tomography images obtained during the arterial phase of enhancement were used as the first step.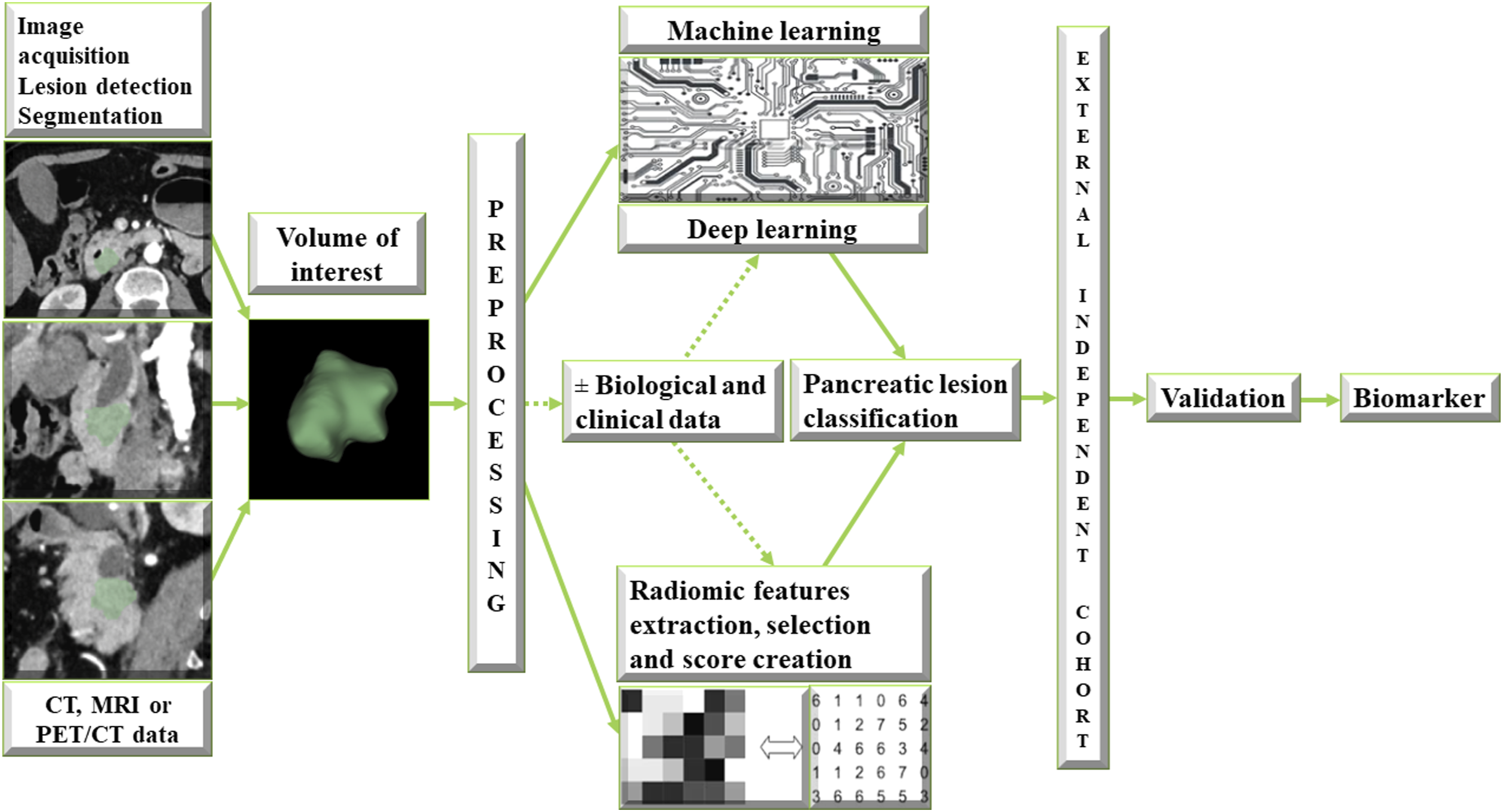
Lesion Detection
Early detection of PDAC in asymptomatic patient is of crucial importance because it is assumed that it could markedly increase survival. The sensitivity of CT for PDAC detection ranges between 78% and 96.8%, with an overall sensitivity of 90%, but drops to 63-77% for PDAC < 20 mm in size.4,19 Toshima et al. have identified morphological abnormalities on CT, including focal pancreatic parenchyma atrophy, faint focal enhancement, and focal ductal changes, which precede the diagnosis of stage 1 PDAC by one year. 26 Current studies suggest that AI would help detect small PDAC, 24 with deep-learning models yielding AUC of 0.9632 for the diagnosis of PDAC 27 or sensitivity reaching 98.3% compared to 92.9% for the radiologists (P = .014). 28 However, the latter deep-learning model achieved only 63.1% sensitivity (95% confidence interval [CI]: 50.2-74.7%) for PDAC < 20 mm using an external test set. 28 Another deep learning algorithm yielded 91.58% sensitivity with unenhanced images, 94.08% with arterial phase images, and 92.28% with portal phase images, with no differences with clinicians (P = .384) but as limitations, all PDACs were >20 mm with a median size of 35 mm. 29 A recent study, reported impressive early detection of PDAC (i.e., 3-36 months before clinical diagnosis) using radiomics-based ML model with 95.5% sensitivity (95% CI: 85.5-100%), 90.3% specificity (95% CI: 84.3-91.5%), and AUC of 0.98 (95% CI: 0.94-0.98). 30
Lesion Characterization
Pancreatic lesion characterization is also of paramount importance, because the pancreas can be involved by a wide spectrum of conditions, including benign and malignant primary lesions, lesions with intermediate malignant potential, and metastases from distant primaries.31-35 Although morphological imaging findings can be used to confidently discriminate between several pancreatic entities, researchers have tested the capabilities of radiomics in differentiating between PDAC and other pancreatic conditions, including normal pancreatic parenchyma.32,36,37 In this regard, one study showed that radiomics has the ability to differentiate PDAC from AIP, with an accuracy of 95.2% compared to 67% by the radiologists. 35 Another study reported AUCs of 0.96 and 0.93 for radiomic models for differentiating between PDAC and mass-forming pancreatitis. 38 Differentiating between PDAC and pancreatic neuroendocrine neoplasm (PNEN) can be difficult with conventional imaging when PNENs are not hypervascular. 34 Li et al. developed a CT-based radiomics model that yielded an AUC of 0.887 (95% CI: 0.793-0.948) for discriminating between PDAC and PNEN. 34 Radiomics can also discriminate between pancreatic adenosquamous carcinoma and PDAC, with an AUC of 0.80 using texture analysis from unenhanced CT data. 39 However, the incremental value of radiomics may be limited. Guo et al found that radiomics was not superior to arterial and portal enhancement ratios (AUC of 0.99 and 0.98, respectively) to discriminate between pancreatic neuroendocrine carcinoma (ie, poorly differentiated PNEN) and PDAC (AUC of 0.72 and 0.71, respectively). 40 Other researchers compared standard CT features and texture features to discriminate between PDAC and pancreatic lymphoma. 41 Interestingly, there were no differences in AUC value between tumor size on CT (0.821) and the best texture feature (0.704) (P = .306) for discriminating capabilities, thus questioning the actual utility of radiomics in some indications. 41
It is now well established that radiomics features may be limited to capturing low level representations of the input image whereas AI models can learn and extract more complex representations. One study suggested that deep features yielded greater discriminating capabilities than traditional first order radiomics features. 42 Ziegelmeyer et al have trained a machine learning (ML) model using deep features and first order radiomics features to discriminate between AIP and PDAC using CT data. 42 The AI model using deep features achieved an AUC of 0.90 compared to 0.80 using radiomics features and showed better sensitivity (89%) and specificity (83%) that the radiomics model (72% and 78%, respectively) for the diagnosis of AIP. 42 Recently, an AI model using radiomics has demonstrated utility for preoperative prediction of fibroblast activation protein expression in PDAC. 43
Survival Prediction After Curative Surgery
Studies showed that radiomic features can be used for risk stratification of PDAC and can predict survival after surgical resection.44,45 Hypoattenuating PDAC on CT images are associated with shorter overall survival (OS) and disease-free survival (DFS) after surgery.44,45 Similarly, radiomic features that are representative of tumor hypoattenuation are associated with poorer outcome.46-48 By contrast, the association between radiomic features representative of tumor homogeneity on CT and DFS is less clear.46,49 One study found that PDAC with homogenous texture features conveyed shorter DFS 46 whereas another reported that greater dissimilarity (heterogeneity) was associated with longer OS. 49
The capabilities of radiomics for predicting OS after neoadjuvant therapy have been evidenced in several studies that used CT data.47,50 Kim et al. found that high subtracted value of entropy and small subtracted value of GLCM entropy were associated with longer OS. 50 Another study identified a second-order feature (directional edge-based ACM) that provided AUCs of 0.80-0.90 and accuracies of 75-83% for identifying patients with OS less than two years after neoadjuvant chemotherapy (gemcitabine and oxaliplatin) and surgical resection. 47 Of interest, another study that used a hybrid model (radiomic features, CA 19-9 serum level and Brennan score) found a greater concordance index than radiomics alone to predict OS. 48 Park et al. have investigated the utility of preoperative CT radiomics features to predict postoperative survival of 153 patients with surgically resected PDAC. 51 The 10 most relevant radiomics features yielded 82.2% accuracy in the classification of high-risk (survival time <one year) vs low-risk (survival time >three years) patients. The C-index of survival prediction using clinical parameters alone was 0.6785, whereas the addition of radiomics features resulted in a greater C-index of 0.7414. In this study, addition of CT radiomics features to standard clinical factors improved survival prediction in patients with PDAC. 51 In general, the majority of radiomics studies that used CT data found that first-order entropy is significantly associated with OS. 52
The use of MRI for radiomics has been assessed in a few studies53,54 Choi et al. used data from T2-weighted turbo spin-echo MR images obtained at 3T to identify texture features associated with OS and DFS. 53 Although tumor size, skewness, and kurtosis were associated with DFS and tumor size and entropy with OS in univariable analysis, in multivariable analysis, tumor size was the most significant predictive variable for DFS and equivalent to entropy for OS, thus questioning the utility of radiomics. 53 However, another study used MRI for the prediction of early recurrence after surgical resection of pancreatic cancer at large. 54 The radiomics signature yielded AUC values of 0.802 in the training set, 0.807 in the internal validation set, and 0.781 in the external validation set to identify patients with early recurrence. 54 Of note, in the same study, a nomogram including radiomics signature, clinical stage, and preoperative CA 19-9 level, yielding greater AUCs of 0.871 (training cohort), 0.876 (internal validation cohort), and 0.846 (external validation cohort). 54
AI shows promises for predicting OS in patients with PDAC. One study reported a supervised ML model based on diffusion-weighted imaging (DWI)-derived radiomics features that yielded an AUC of 0.90 for the prediction of above- vs below-median OS in the validation cohort. 55
Prediction of Tumor Response to Therapy in Unresectable or Locally Advanced PDAC
Using dual-energy CT, Noda et al. found that kurtosis of iodine concentration allowed to identify responders (partial response and stable disease) with lower values in the response group, reflecting lower tumor heterogeneity in this group. 15 In addition, the difference in mean iodine concentration of PDAC between pancreatic and equilibrium phases (ΔIC) was lower in patients with poorer prognosis than in those with better prognosis. 15 Combining ΔIC and kurtosis, these researchers created an iodine concentration diagnosis factor yielding an AUC of 0.889 for identifying early response to first-line chemotherapy. 15
Neoadjuvant therapy is now highly recommended in patients with borderline or locally advanced PDAC. 56 However, neoadjuvant therapy induces morphological changes due to inflammation, necrosis, or fibrosis, which often result in overestimation of vascular involvement on CT. 57 Moreover, assessment of tumor response using tumor size only can overlook favorable response associated with no observable tumor size decrease. 58 Studies showed that radiomics can be an option to overcome limitations of conventional CT.58-60 Chen et al. reported that changes in radiomic metrics such as decrease in skewness and increase in kurtosis precede tumor dimension changes. 58 Ciaravino et al. observed significant differences in kurtosis values obtained before and after neoadjuvant treatment in PDAC that responded favorably to chemotherapy whereas differences were found in PDAC with progression. 60 Kim et al. found that subtracted texture features allowed identifying resectable PDAC after neoadjuvant chemotherapy. 59
Watson et al. created an AI model based on CT data that predicted favorable response of PDAC to neoadjuvant therapy prior to pancreatectomy with an AUC of 0.738 that markedly outperformed decrease in carbohydrate antigen 19-9 (AUC of 0.564). 61
Prediction of Survival to Therapy in Unresectable, Borderline or Locally Advanced PDAC
Researchers found that radiomics features obtained from CT data can be predictive of OS in patients with locally advanced or unresectable PDAC.62,63 Sandrasegaran et al. reported that in patients with unresectable PDAC, mean value of positive pixels > 31.625 and kurtosis > 0.565 using medium spatial filter were significantly associated with worse OS (P = .036 and .028, respectively) after either Gemcitabine-based chemotherapy and stereotactic body radiation therapy or FOLFIRINOX chemotherapy. 62 Cozi et al found a clinical-radiomics signature (age and homogeneity on unenhanced CT data) that allowed to identify patients with better OS in the validation set with an AUC of 0.73 after stereotactic body radiation therapy. 63 In general, several radiomics features have been identified as associated with DFS and OS. However, they vary across studies. One study reported association between skewness and progression-free survival and OS in patients with unresectable PDAC treated with chemotherapy 64 whereas other researchers found association between tumor response (OS and time to progression) and a specific radiomic feature (ie, cluster tendency with square-root filter) in patients with unresectable PDAC undergoing chemotherapy. 65
Prediction of Resectability
Evaluation of local resectability of PDAC at initial workup is paramount to select the most appropriate therapeutic option. CT, with arterial and portal phase images, remains a pivotal examination. One limitation of CT is that preoperative opinion regarding resectability, negative margins and R0 resection, is subject to marked interobserver variability, with experienced radiologists having higher degrees of agreement. 66 One study found moderate (κappa = 0.48) interobserver agreement for resectability classification. 66 Another study that used six observers reported a limited pooled agreement for tumor resectability of 0.64 (Gwet’s agreement coefficient) for differentiating between resectable, borderline resectable or unresectable PDAC using CT after neoadjuvant therapy for PDAC. 67 However, in the same study a high agreement for differentiating between resectable or borderline resectable vs. unresectable cancer was obtained (Gwet’s coefficient, 0.84). 67
One study assessed the capability of CT to identify superior mesenteric artery (SMA) and posterior and superior mesenteric vein/portal vein (SMV/PV) involvement in patients with resectable or borderline resectable PDAC of the pancreatic head. 68 The authors reported poor pooled sensitivity (15%) but high pooled specificity (99%), with no differences between SMA and SMV/PV. 68
Regarding the potential advantage of MRI over CT, Noda et al found no differences in the detection of vascular involvement as determined by two independent readers between CT (AUC = 0.50 and 0.89) and MRI (AUC = 0.51 and 0.75) 69 and no differences in classification as resectable, borderline resectable, and locally advanced PDAC.
A large number of studies have assessed how radiomics features can be used to predict vascular involvement, resection margin positivity, and lymph node metastases.45,70,71 To address the limitations of morphological imaging to predict complete margin resection (R0) in patients with PDAC, Rigiroli et al. have tested the capabilities of radiomics to identify SMA involvement in PDAC with CT. 70 They obtained a model with five features (maximum hugging angle, maximum diameter, logarithm robust mean absolute deviation, minimum distance, square gray level co-occurrence matrix correlation) that outperformed radiologist assessment (AUC = 0.71 vs. 0.54, respectively; P < .001). Of interest this model yielded 62% sensitivity and 77% specificity. 70 Radiomics can be used to predict SMV involvement as reported by Bian et al. who developed a CT rad-score that showed limited capabilities with an AUC of 0.565 only to predict R0 resection of SMV. 71
Regarding lymph node involvement in PDAC, Cassinoto et al found that hypoattenuating PDAC on portal phase CT images were associated with higher rate of nodal involvement greater lymph node invasion, and shorter DFS, with all-tumor average pixel attenuation at SSF2 yielding highest AUC (0.74 for the diagnosis of lymph node metastases. 45 Another study that used dual-energy CT data from patients with PDAC who underwent chemoradiation followed by surgical resection and lymph node dissection reported 96% sensitivity, 34% specificity, and an AUC of 0.61 using a radiomics model based on mean intensity of pancreatic parenchymal phase image and tumor volume. 72
Assessment of Distant Disease
Patients with PDAC often have distant metastases that mostly involve the liver, the lung, and the peritoneum. 73 In highly selected patients, surgical resection of synchronous hepatic metastases (median OS up to 34 months), metachronous lung metastasis (median OS, 51-121 months) or metachronous liver metastasis (median OS, 24-40 months) may show some benefits. 73 However, in general, presence of synchronous liver metastases from PDAC is considered as contra-indication for surgery. Data from the literature show that MRI significantly outperforms CT for the detection of liver metastases from pancreatic cancer, with sensitivities for CT and MRI of 45% and 83%, respectively, whereas the two techniques have similar specificities (94% and 96%, respectively. 74 Of interest, CT shows better sensitivity when triphasic and quadriphasic examinations are obtained. 74 As a consequence, MRI is now recommended when searching for liver metastases from PDAC, and especially when surgical resection is considered, because it may alter management in up to 10% of patients. 18 The added value of DWI in patients with no visible liver metastases on CT is not demonstrated. In this regard, one study found that all hepatic metastases from PDAC were visualized both with and without DWI. 18
The lung is the second most common location of metastases from PDAC. A recent study revealed that lung metastases from PDAC may present with an unusual pattern on CT that includes an alveolar presentation (22%) in association with nodules with halo sign (41%), air-space nodules (24%), pure ground glass nodules (18%) and consolidations (18%). 75 In this study, the “alveolar” pattern on CT was due to lepidic growth of the metastatic cells at histopathological analysis. 75 The role of CT for the detection of lung metastases is currently debated. 76 One study reported that OS of patients with PDAC is not affected by the presence of indeterminate lung nodule identified on staging chest CT. 76 In the same study, isolated lung metastases did not alter management of the primary tumor. 76 A systematic review confirmed that preoperative detection of indeterminate lung nodule is not associated with decreased OS after surgery and should not preclude curative resection in patients with otherwise resectable PDAC. 77 Finally, the results of one study suggested that in patients with locally advanced PDAC and either no pulmonary nodule or apparent benign pulmonary nodule on initial chest CT, routine follow-up chest CT is not recommended, because they do not develop lung metastases. On the opposite, patients with pulmonary nodules too small to characterize at initial chest CT are at risk to develop lung metastases during follow-up. 78
Preoperative Planning
Besides estimation of vascular involvement, preoperative planning of PDAC requires precise visualization of vascular structures in relation to the tumor and also identification of anatomical variations, such as celiac axis stenosis, that may make surgery difficult or increase the risk of intraoperative vascular complications.
79
This is also because in selected situations, resection of the celiac axis may be required, so that careful evaluation of potential spontaneous anastomoses that preserve liver vascularization is of paramount importance.80,81 To address this issue, three-dimensional imaging has a major role in identifying vascular variations such as arcuate ligament or celiomesenteric trunk.82,83 More recently, cinematic rendering, which is a recent form of three-dimensional volume rendering that generates photorealistic images, has demonstrated utility as it helps surgeon to better identify presence of arterial anatomic variants and vascular involvement (Figure 3).
81
Although beyond the scope of this article, recent evidence suggests a limited or even no role for 18F-fluorodeoxyglucose positron emission tomography/CT in the initial preoperative evaluation of PDAC.
84
45-year-old woman with pancreatic ductal adenocarcinoma of the pancreatic body. (A) Computed tomography image obtained in the axial plane during the arterial phase of enhancement shows large lesion (arrow) of the pancreatic body. (B) Cinematic rendering allows vascular mapping and reveals encasement of celiac axis (arrow). (C) Cinematic rendering with tissue mapping shows splenic vein involvement (arrow). (D) Cinematic rendering demonstrates enlargement of left gastroepiploic vein (arrow) indicating segmental portal hypertension due to splenic vein obstruction by pancreatic tumor.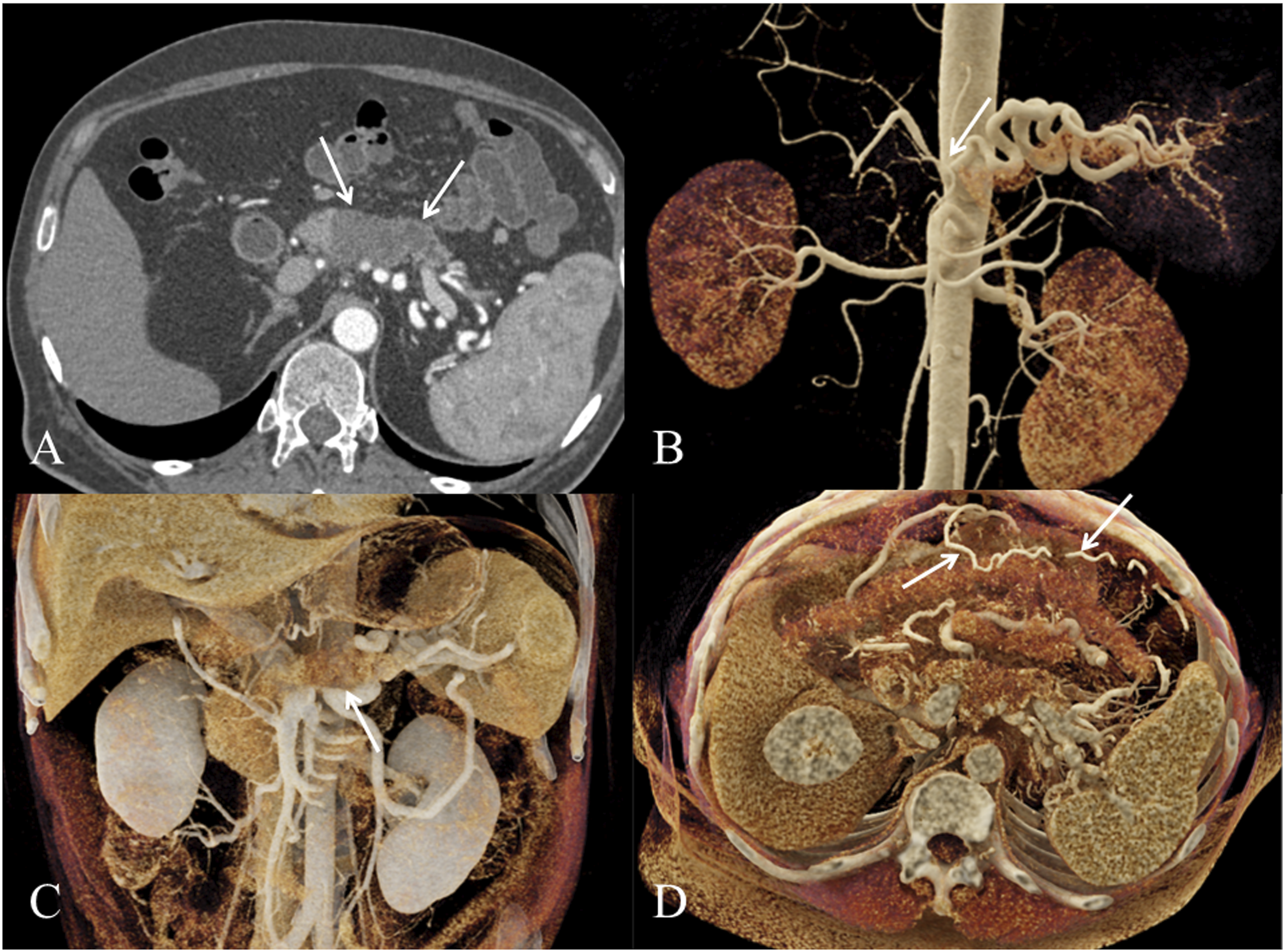
Conclusion and Future Developments
Despite major progress in imaging, PDAC remains a severe disease with limited OS. CT is still the front-line imaging modality for the detection and initial assessment of PDAC, with limited capabilities in terms of detection of small PDAC and preoperative assessment of resectability and prediction of R0 margins. Radiomics shows encouraging results in terms of tumor resectability prediction and discriminating between border line and locally advanced PDAC. AI is a field of major ongoing research but has major drawbacks, and for the majority of tasks it remains inferior to the radiologist and requires an important amount of work for radiologist for features extraction. One goal for AI could be the detection of small PDAC at an early stage, as a substantial proportion of these cancers remain not visible to the human eyes. Future studies should also include sophisticated models that associate imaging data with clinical and biological data. The recent introduction of new therapies should also stimulate further studies for a better evaluation of tumor response.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.