
Abstract
Introduction
Lung cancer is the most common cancer worldwide and the lungs are frequent sites of metastasis. 1 Tissue diagnosis is often required because the imaging appearance of lung nodules is non-specific. 2 Computed tomography (CT) guidance modalities are the most common choice for transthoracic needle biopsies because of their ease of use, excellent temporal and spatial resolution, and lack of impediments in air and bone.3,4 Unlike the real-time guidance of ultrasound and fluoroscopy, the puncture accuracy of the conventional freehand technique mainly depends on the operator’s experience using a challenging visual spatial orientation. The freehand technique can sometimes be time consuming, and it usually requires several CT controlling scans to correct the needle trajectory, particularly for beginner or non-interventional clinical physicians, or when the target is small or deep in the tissue. As a result, the procedure is prolonged, the radiation exposure is increased, and there is increased potential for complications.
To facilitate puncture accuracy, numerous devices have been developed, from various low cost, simple devices to highly complex electromechanical systems that need to be integrated into a CT scan unit and that communicate with software such as CT fluoroscopy, electromagnetic navigation, or robotic puncture systems.5-7 Real-time CT fluoroscopy can successfully overcome patient movement, including respiratory movement; however, it also results in extra radiation exposure to operators. 5 Despite apparent advantages over the conventional CT-guided puncture technique, advanced navigation or robotic systems are rarely used by interventional radiologists. Specifically, in addition to the need for complex equipment in the CT room and specific software, required preoperative disinfection and registration also make the process time consuming.6-8 Another disadvantage of these systems is that they completely limit the needle path to within a planned trajectory. Therefore, it is difficult for the operator to make adjustments or re-plan to adopt changes in the target position caused by subtle body or breathing movements by the patient during the procedure.
With newly developed laser-supported systems, mechanical guidance is replaced by laser beams that do not contact the puncture area, allowing the needle to be moved freely, which overcomes the shortcomings of the previously mentioned robot-assisted method.9-13 The principles of a laser navigation system are relatively simple: the system requires no preoperative system disinfection or registration, and it preserves the operator’s accustomed haptic control of the puncture needle that caters to the radiologist’s preferences. 14 Compared with the freehand technique, commercially available laser navigation systems are a significant improvement to planning the puncture point and adjusting the needle angle. 11 However, in addition to cost, some of these devices require the installation of fixed rails or support equipment on the ceiling of a CT room.11-13 Because not all hospitals or clinics have a specialized CT room solely for interventions, the need to modify a CT scan room is not easily accepted by administrators. Laser-assisted positioning devices mounted on the CT scanning gantry faces the same problem.10,11
Thus, we designed a simple laser-assisted angle selection system (LASS) to facilitate conventional freehand CT-guided punctures, and a clinical study was conducted to determine whether this LASS was advantageous in terms of saving time and dosage compared with a conventional freehand method.
Materials and Methods
LASS Device Design
The developed LASS system was designed to mount at the foot of the CT table and emit a linear laser toward the CT gantry (Figure 1). The primary system component is a line laser (KYC650N5-X1240, Xinkunyang Technology Co., Ltd, Shenzhen, China) fixed in a rotatable bearing that rests on a horizontally moveable table installed on two parallel sliding rods. The angulation of the emitted fan-shaped light directed toward the CT gantry can be adjusted freely by rotating the bearing, and it can be precisely read from a dedicated 180° indexing dial. A built-in bubble level and four adjustable feet were installed on the platform for leveling the unit on any scan table. Illustrations of the principle of the LASS. (a) The main components of this system are a line laser projector, a rotatable bearing, a round indexing dial, and a sliding rod platform. The system can be placed on the bottom of any standard CT table. (b) The LASS projects a fan-shaped light toward the scanning gantry and the angle can be read from the indexing dial. Before each use, the LASS is first adjusted to the zero position, then the laser unit’s position is adjusted to allow the beam (curve arrow) to totally overlay the CT’s inner positioning laser along the longitudinal axis of the scanning table (arrow) to achieve system alignment. LASS: laser angle selection system; CT: Computed tomography.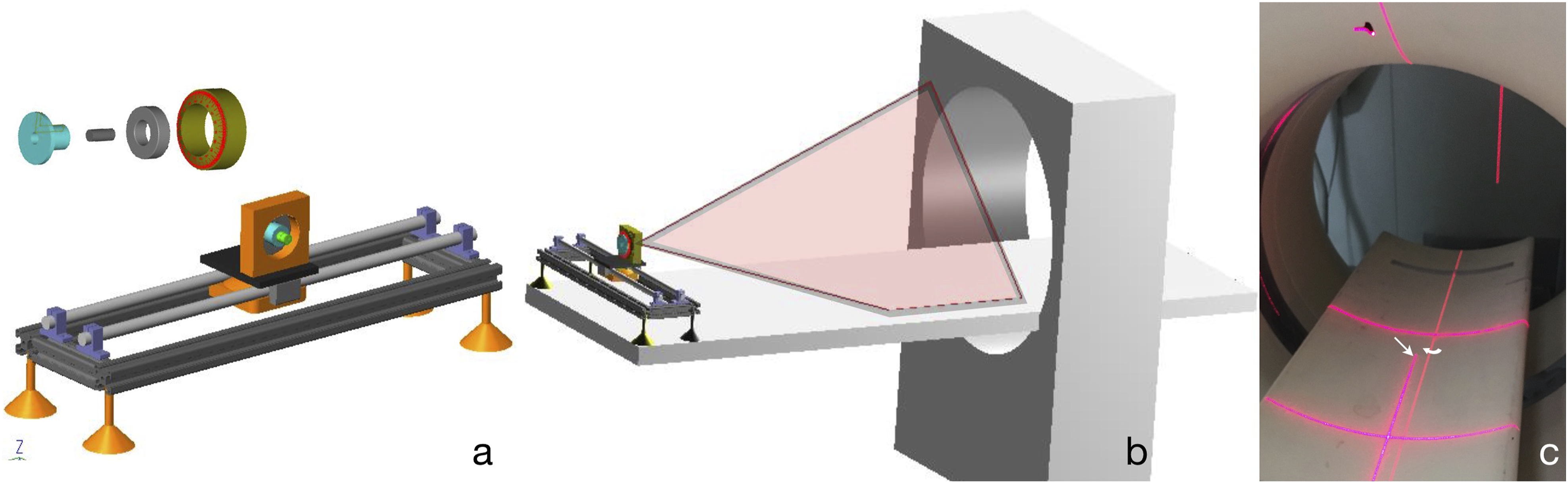
After mounting the device at the foot of the CT table, the correct positioning of the system relative to the table was obtained by aligning the generated laser line at position zero parallel to the CT centering laser positioning light (Figure 1(c)). The setup can be performed in less than two minutes by one person. The system is not physically connected to the CT unit and the dimension of the system was 18 cm (H) × 48 cm (W) × 48 cm (L), which allowed it to be stored when not in use such that the daily scanning work was not affected.
The preparations for a LASS-guided puncture are similar to those for a freehand puncture. The skin-entry point and target are conventionally chosen from the pre-biopsy CT, and the needle puncture angle (the angle of the planned route off the vertical) and depth (from the planned entry point to the target region) are calculated (Figure 2(a)). An assistant rotates the laser to the planned angle, then horizontally slides the table to make the laser beam pass through the marked skin-entry point (Figure 2(b)). The resulting laser beam is then projected over the patient corresponding to the planned needle puncture angle. Because the system does not affect the surgery area, the operator can perform skin disinfection and local anesthetization at the same time. (a) Laser angle selection system-assisted percutaneous transthoracic needle biopsy. Planning CT shows the planned entry point, lung lesion, and the planned puncture path. (b) Adjusting the table position to make the laser beam pass through the marked skin entry (arrow). (c) When the skin-entry point, needle shaft, and hub are totally aligned with the red light (arrow), the pre-planned punctured is correctly achieved. (d) Advance the needle to the planned depth and perform a control CT scan to confirm the needle tip position. This lesion was achieved by one pass. CT: Computed tomography.
For needle insertion, the needle tip is placed at the skin-entry point and the hub of the needle is adjusted to precisely match the laser projected angle. The needle should exactly match the planned puncture angle when the whole needle length is illuminated by the laser (Figure 2(c)). During needle insertion, the operator maintains laser light illumination of the entire needle length to prevent deviation from the planned path. CT is used to monitor the needle tip position until the target has been reached (Figure 2(d)). When the CT shows that the target site has been reached, the subsequent biopsy can be completed using standard techniques.
Study Design
This is a single institution, retrospective, observational study of patients who underwent a biopsy of lung lesions with and without LASS. Patients referred for CT-guided PTNB between September and November 2016 were included. All biopsies were performed using the same CT (Philips, Precedence 16, Netherlands) by two interventional radiologists with at least 6 years of experience in CT-guided biopsy. The exclusion criteria were lung lesions <10 mm at the maximum diameter, small lesions near or adhering to the heart, diaphragm, and large vessels, lesions suspicious for vascular origin, and patients who were not able to follow verbal or visual instructions. Emphysema was not an exclusion criterion for biopsy. The study was approved by the ethics committee, and all procedures were performed after informed consent of the patient had been obtained. The imaging parameters of the scanner were 120 kV, 100 mA, 0.75 s rotation time, 0.985 pitch, 5 mm collimation, 5 mm thickness, 5 mm increment, and 512 matrix. If small lesions were punctured, the slice thickness was adjusted accordingly. The coaxial biopsy technique was used in all patients with a 17-gauge coaxial introducer and an 18-gauge inner automated cutting needle (Angiotech, BioPince, Argon, Medical, Bloomington, IN, USA).
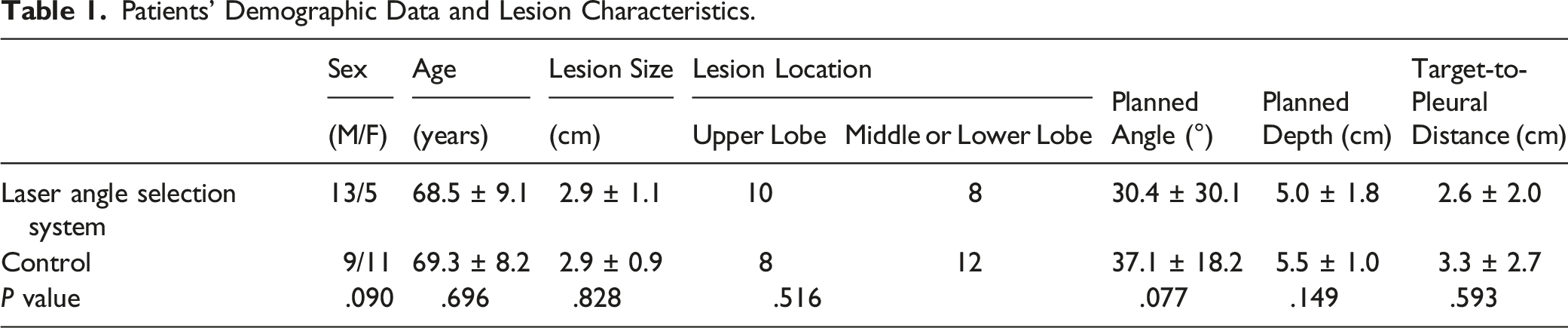
Patients’ Demographic Data and Lesion Characteristics.
Data Evaluation
Information collected for every patient included lesion size, target-to-pleural distance, puncture length and angle, the number of control scans, time of the procedure (including the operation time and room time), patient’s radiation dose, and post-biopsy complications. The operation time was defined as the time interval between the initial localizing scan and control scan showing the needle tip in the target. The room time was recorded from when the patient entered and left the CT room. The dose length product (DLP) in mGy × cm measured by the CT unit was used as the primary dosimetric quantity data. Separate DLPs of each scan were recorded, and the DLP of the control scans and whole procedure were calculated separately. The mean effective dose during the procedure was calculated using the European quality criteria (DLP × conversion factor k (chest; 0.017 mSv × mGy−1 × cm−1)). 15
All analyses were performed using SPSS16.0 for windows. Data are expressed as mean ± standard deviation (SD). Statistical significance was calculated according to the Mann–Whitney U test. A P < .05 was considered statistically significant.
Results
Puncture Results and Post-Biopsy Complications.
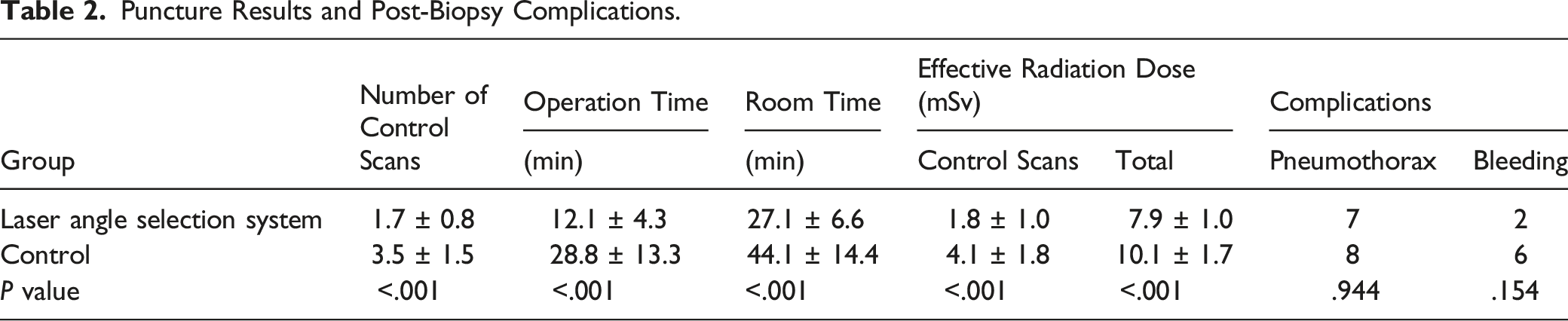
After the biopsy, asymptomatic pneumothorax conditions that did not require further treatment were detected in 15 patients (7 patients in the LASS group and 8 patients in the freehand method group, P = .944). Mild lung parenchyma hemorrhages were documented in 8 patients (2 patients (11%) in the LASS group, the remaining 6 patients (30%) were in the freehand method group, P = .154). No other major complications occurred.
Discussion
Various laser guidance systems that can be either handheld or permanently fixed to a CT gantry or the ceiling of a CT room have been introduced clinically.10,11 Various reports have also confirmed the value of these devices in improving puncture accuracy, reducing operating time, and reducing patients’ radiation.11-13 Our device uses a simple table and laser line projector that allows easy and accurate alignment of a biopsy needle on the X–Y plane, and the initial results demonstrate that this setup can achieve similar results as commercially available laser navigation systems in terms of time saving and dose reduction. The procedure time is reduced because of fewer needle corrections, and the patient’s exposure to radiation is reduced because fewer scans are needed to confirm the needle position. Numerous studies have shown the advantages of computer-assisted navigation systems; however, deficiencies, such as increased handling and setup times, have prohibited the spread of one navigation system.10-12,16 Without the need to change the CT room structure or complex software, the LASS can be installed and setup by one person in only two minutes, and the system can be moved to another room or scanner. Robotic devices have the disadvantage of restricting the needle path to the planned trajectory, preventing the operator from spontaneous adjustments when the position of the target changes during the operation (eg, breathing, movement, or a pneumothorax). Handheld laser devices require sterilization after each use, and gantry-mounted systems reduce the access to the patient because of their limited reach. Because the laser system is a contact-free guidance system and it does not affect normal routine imaging, the operator can easily adjust the needle or even re-plan a new path.
Our data shows that with the help of LASS, 56% of the operations hit the target without additional needle corrections compared with only 10% of the conventional method without LASS. Brabrand et al reported lesion hits 85% of the first needle passes with LASS. 11 Previous studies have shown similar results with needle guidance devices.17,18 Therefore, the high accuracy achieved when using the LASS system would allow even inexperienced radiologists to place the needle at the target without repositioning. Reaching a lesion on the first needle pass has great benefit to thin patients where the needle does not have sufficient support from the chest wall and lung tissue itself. Frequent repositioning of the needle results in higher radiation doses for such patients and has the potential to increase their risk of related complications. The incidence of lung parenchyma bleeding was less in the LASS-assisted group than in the freehand group; however, the differences was not significant and larger studies are necessary to confirm this benefit. Although successful biopsies were often achieved on the first pass, it is still better to use the step-by-step method for small deep lesions, or lesions around important structures to avoid injury to important structures because of subtle position changes during needle advancement.
The operation position typically has the extension line of the needle tip toward the hub aimed at the operator to allow for hand–eye coordination so the operator can make fine angle adjustments and maintain the puncture needle in the axial plane. A disadvantage of commercial laser guiding systems, as described by Gruber-Rouh et al, 11 is that the laser needs to enter along the puncture needle extension line, and the operator’s body may block the light, especially when the puncture angle is relatively large. 12 Therefore, the operator often needs to rotate their body to one side, resulting in a one-handed operation, or standing on the opposite side, which may impair the stability of needle advancement and affect the operator’s haptic sensations. Because this device is mounted at the foot of the CT table and the laser comes toward the CT gantry along the longitudinal plane, the operator does not need to change their position, which allows for a normal two-handed procedure. However, because the laser beam projects from the side parallel to the operator’s body, the operator may need to rotate their head to check the relationship between the laser beam and needle shaft, which may result in a deviation of the needle from the Z-axis. An assistant standing behind this laser device is recommended when puncturing small lesions to help the operator monitor the needle advancement process and provide real-time oral instructions when necessary.
This study had several limitations. For example, all manipulations were performed by two experienced interventional radiologists. Puncture is highly dependent on the experience of the operator and therefore, may vary considerably among inexperienced general radiologists or nonradiologists. Additionally, more patients are needed to assess the reproducibility of the results. Although the needle angulation accuracy is not included in these results, the requirements of positioning corrections were significantly reduced; therefore, on the basis of our clinical experience, the accuracy will be improved. The precision may be the main limitation of this device because the angle selection and needle advancement are still controlled by hand rather than more precise advanced electromechanical or electromagnetically systems. Even with a robotic system, many factors may deviate the needle away from its intended paths such as the inhomogeneity of the tissue and the beveled needle itself. Double oblique punctures are a challenge for every radiologist, and the presented device has only one angulation. Jeon et al used an additional Laser guidance system placed on the opposite side of the patient to the operator to provide additional angulation on the Z-plane. But this method has shortcoming, as the needle will not be maintained in the same slice and the laser beam may hurt the operator’s eyes. In our practice, the LASS is combined with gantry tilting. As the needle is aligned with the CT gantry laser beam and LASS at the same time, maintaining this alignment allows the entire needle trajectory to be seen on a single CT slice.
In conclusion, the present study demonstrated that the developed LASS can be used to reduce radiation dose exposure and reduce the procedure time of a CT-guided percutaneous transthoracic needle biopsy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Wuxi “Taihu Lake Talent Plan” medical and health high-end talents (2020).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
This study was approved by the local ethical board, and the informed consensus was obtained from all individual participants included in the study.