
Abstract
The SEN virus (SENV), a DNA virus that has been linked to blood transfusion, is a major cause of post-transfusion hepatitis. SENV-D and SENV-H are non-A to E hepatitis viruses. The present study was conducted to investigate the prevalence of SENV-D/H among dialysis patients and blood donors as control group in Diyala province/Iraq. This study includes 120 participants: 80 dialysis patients who have been attending the Ibn-Sina Dialysis Center-Diyala Directorate of Health were previously diagnosed with the disease, and 40 individuals as controls were selected at random from blood donors at the Central Blood Bank during the period from 1/5/2025 to 30/11/2025. Full information had been taken directly from the patients, and the information had been arranged in an informative formula sheet, which includes age and gender. All study subjects were screened for nested polymerase chain reaction. The SENV-D prevalence was 10 (12.50%) and 0.00% for dialysis patients and controls, respectively, and SENV-H was 5 (6.25%) and 1 (2.50%) for dialysis patients and controls, respectively. The SENV co-infection rate of genotypes D and H was 3 (7.50%) in the dialysis group, and no cases in the control group were found. A very strong association was found between the distinct SENV genotypes and Hepatitis B virus (HBV) or Hepatitis C virus (HCV) status. Positivity for SENV was also correlated with high serum Aspartate Aminotransferase (AST) and Alanine aminotransferase (ALT). SENV-D and SENV-H were more prevalent among hemodialysis patients than in normal blood donors. The presence of SEN-V in both groups indicates its categorization as a blood-borne virus and suggests risk for transmission by blood exposure.
Introduction
SEN virus (SENV) is a recently discovered blood-borne DNA virus described in Italy in 1999 (Matsumoto et al., 1999). It was suggested to be etiologically associated with non-A–G (NAG) hepatitis and, at the beginning, implicated in post-transfusion hepatitis. Viral hepatitis continues to be a major global health concern, especially in the tropics, where it accounts significantly for morbidity and mortality. At least six distinct viruses are responsible for this condition; although their molecular structures and replication mechanisms differ, they share an attraction to hepatic tissue and give rise to similar clinical presentations (Al-Ouqaili et al., 2020). Although the classical hepatitis viruses remain the most frequent blood-borne pathogens causing chronic liver disease, other agents have been associated with cases of NAG hepatitis. The latest agent to have been suggested in these cases is the SENV (Chethan and Valliyamma, 2017).
Based on molecular and genetic studies, SENV shows that it belongs to the Anelloviridae family and is characterized as a small, circular, non-enveloped single-stranded DNA virus. Its diameter is approximately 26 nm, and its genome is nearly 3,800 nucleotides in length. The viral genome contains at least three open reading frames (ORFs). SENV is now recognized as a globally distributed virus, although its prevalence varies considerably among different regions (Al-Shuwaikh, 2020). Genetic characterization has identified nine genotypes of SENV, designated A through I, which differ from one another by roughly 25% at the nucleotide level. Among these, the D and H genotypes are the most commonly detected worldwide (Elaskary et al., 2023).
As SENV can be transfusion-transmitted, its DNA is detected more often under clinical settings in which transfusions are commonly administered, such as surgeries, hemophilia injection drug use, HIV infection, and hemodialysis(Al-Ani et al., 2019). The prevalence of the SENV among Hemodialysis (HD) patients is described between 13% and 68%. Conversely, the frequencies of SENV and its D/H genotypes differ greatly from one healthy population to another, being reported between 2% and 25% according to geographic area. Coinfection of SEN-V with chronic hepatitis C had also been reported, thereby suggesting a certain association of SENV and HCV. Given that patients on hemodialysis or PPCD require multiple transfusions, their risk for contracting blood-borne infections is increased. Therefore, analysis of the prevalence of SENV-D and SENV-H is important to provide insight into the clinical relevance of SENV infection in this population and the risk regarding non-A–E hepatitis. Country-based information is especially valuable for the distribution of SENV-D and SENV-H, since the prevalence of the virus is significantly linked to geographical aspects (Elnagi et al., 2021; Umemura et al., 2003).
Previous studies showed a possible association between SENV infection and NAG hepatitis in patients with dialysis. Several studies from various parts of the world have reported a surprisingly high frequency of this virus in hepatitis found among dialysis patients. SENV-D and SENV-H genotypes have both been linked to transfusion-transmitted hepatitis (AL-Maqati et al., 2022; Kobayashi et al., 2003). The D and H genotypes of SENV were most frequently detected in A–G hepatitis patients whom undergoing hemodialysis, indicating potential clinical relevance and higher prevalence (Naseri et al., 2025). In one study, Rizvi et al. found that 38% of cases of hepatitis were due to SENV-D genotype and noted the presence of SENV-H in 58% (Al-Kanaan et al., 2019; Aranda et al., 2025; Rizvi et al., 2013). Similarly to Mohamed et al., they′ve noticed that these two genotypes (D and H) were detected most often in blood unit recipients as well as the renal dialysis patients, which makes these groups potentially vulnerable to SENV infection (Ismail et al., 2011). Also, another study in Iran showed that blood-borne viral pathogens, such as SENV, pose a greater risk in patients under regular periodic hemodialysis. Through the Polymerase chain reaction (PCR) analysis, SENV-D and SENV-H were detected in 28.63% and 14.53% of patients, respectively; simultaneous detection of both genotypes was found in 9.69% of the examined population (227 individuals). Although SENV has been clearly associated with NAG transfusion-related hepatitis, most of the infected recipients did not show clinical signs of hepatitis (AL-Maqati et al., 2022; Tang et al., 2008). To the best of our knowledge, this is among the few studies in Iraq to evaluate the distribution of SENV genotypes D and H and their association with liver function markers in hemodialysis patients.
Methods
Study groups
This cross-sectional study was conducted in Diyala province from May 1 to November 30, 2025. Two groups were included: a case group consisting of (n = 80) hemodialysis patients attending Ibn-Sina Dialysis Center, Diyala Directorate of Health, and a group of healthy individuals (n = 40) who donated blood at the Blood Bank, Diyala Directorate. Of the dialysis patients, 57 were male, and 23 were female, and for healthy persons (39 male and 1 female), their ages ranged from less than 10 to >70 years. Through a standardized questionnaire, demographic factors including age and gender were collected. All patients signed an informed written consent before enrolment.
Inclusion and exclusion criteria
The inclusion criteria for hemodialysis patients included those who had been receiving regular hemodialysis for at least six months. Patients receiving antiviral therapy, those with known immunological or neoplastic disorders, and those with documented chronic liver disease unrelated to viral hepatitis were not included. Medical records provided the clinical data.
Those in the healthy control group had no prior history of chronic illness, liver disease, or blood transfusions. Before being enrolled, all controls underwent screening and had negative hepatitis B and C test results.
Blood samples collection
Ten milliliters of venous blood were obtained from all subjects by a sterile gel tube, without any anticoagulant. After centrifugation of the samples at 3000 rpm, the serum was aliquoted into three separates. The latter aliquot was employed to analyze ALT and AST levels in accordance with the manufacturer’s guidelines by an AU 680 automated chemistry analyzer (Beckman, USA). The second aliquot was used to detect anti-HBs antigen and anti-HCV antibodies according to the manufacturer’s instructions (Dia. PRO, Italy). The third aliquot was frozen at –20°C until PCR-based detection of SENV-D/H was performed.
SENV DNA extraction
Each serum sample was treated to extract genomic DNA with the ReliaPrep™ Blood gDNA Miniprep System (Promega, USA) according to the manufacturer’s instructions.
Detection of SENV DNA by nested PCR
Primers
For the nested PCR method, primer sets specific for part of the ORF-1 gene of SENV-D and SENV-H were used as described previously (5, 14). The primers were purchased from Macrogen (South Korea) as lyophilized, reconstituted in nuclease-free water to make their stock concentration of 100 pmol/μL. Ten microliters of each primer was suspended in nuclease-free water, mixed, and serially diluted by 90 μL nuclease-free water for the working dilution (10 pmol/μL), which is mentioned in Table 1.
Primers Used for Detection of ORF-1 Gene
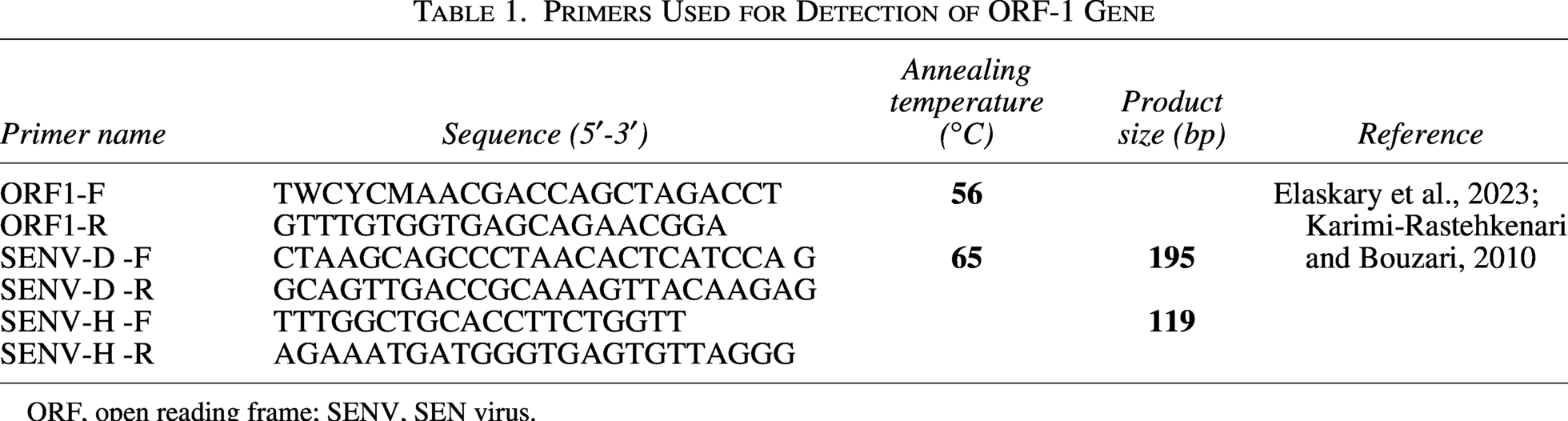
ORF, open reading frame; SENV, SEN virus.
SENV-D and SENV-H detection by PCR
Nested PCR was utilized to amplify a portion of the ORF-1 sequence, which is unique for SENV-D and SENV-H. The first round of amplification was performed in a reaction mix containing the primer pair, master mix, nuclease-free water, and extracted DNA. Cycling conditions comprised three steps: denaturation-annealing-extension plus a final extension step. For the second round, a small amount of the first PCR product was used, and genotype-specific primers for SENV-D or SENV-H were applied with comparable but shorter cycles. PCR products were then analyzed by agarose gel electrophoresis, and product sizes were determined based on a 1500-bp DNA ladder.
Statistical analysis
Statistical analysis was performed using SPSS version 29. Continuous variables were compared using an independent t-test. Categorical variables were analyzed using the chi-square test; however, Fisher’s exact test was applied when the expected number of cells was less than five. A p value ≤ 0.05 was considered statistically significant (George and Mallery, 2024).
Ethical approval
The inquiry was governed by the ethical standards outlined in the Declaration of Helsinki. Prior to the collection of the sample, the patient provided verbal and written consent. The study protocol, subject information, and permission form were reviewed and approved by a local ethics committee under document number 37,085 (dated 7/10/2025).
Results
Population studied
The present study was conducted on 80 dialysis patients (57 [71.25%] males and 23 [28.75%] females with a mean age of 52.60 ± 1.64) and 40 healthy blood donors as controls (39 [97.50%] males and 1 [2.50%] females with a mean age of 31.67 ± 0.99). Dialysis patients revealed significantly higher percentage of HCV, and AST liver enzymes, and no significantly in ALT enzyme, while the control group had significantly higher HBS percentage compared with patients, as found in Table 2.
Distribution of Demographic Factors and Clinical Data Among the Studied Population
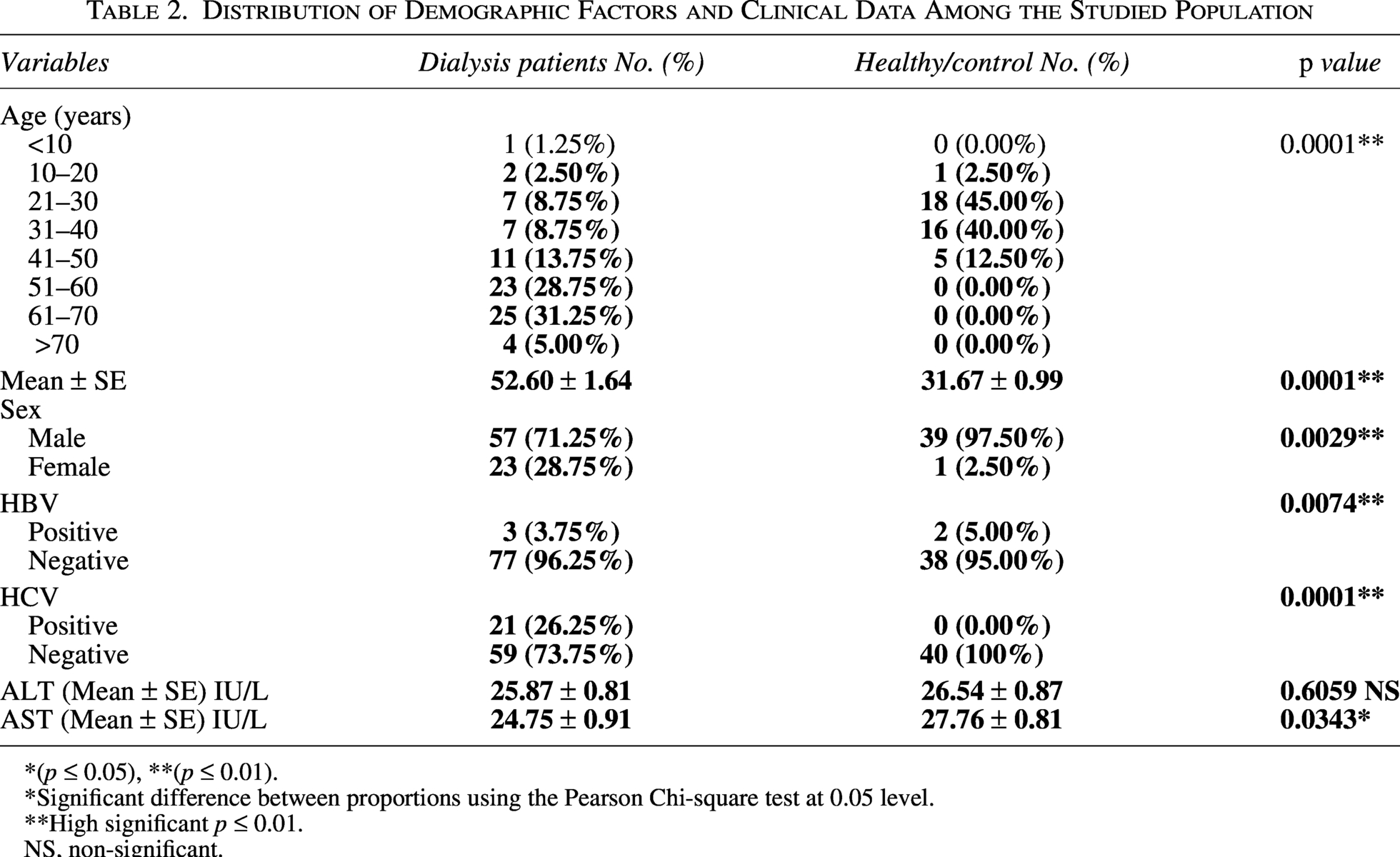
*(p ≤ 0.05), **(p ≤ 0.01).
Significant difference between proportions using the Pearson Chi-square test at 0.05 level.
High significant p ≤ 0.01.
NS, non-significant.
SENV detection by nested PCR
Among the studied population, the prevalence of SENV-D, SENV-H, and SENV-D/H was 10 (12.50%), 5 (6.25%), and 3 (7.50%), respectively, among dialysis patients. The results of nested PCR found that only 1 (2.50%) of blood donors as controls were positive for SENV-H (Table 3 and Figs. 1 and 2).
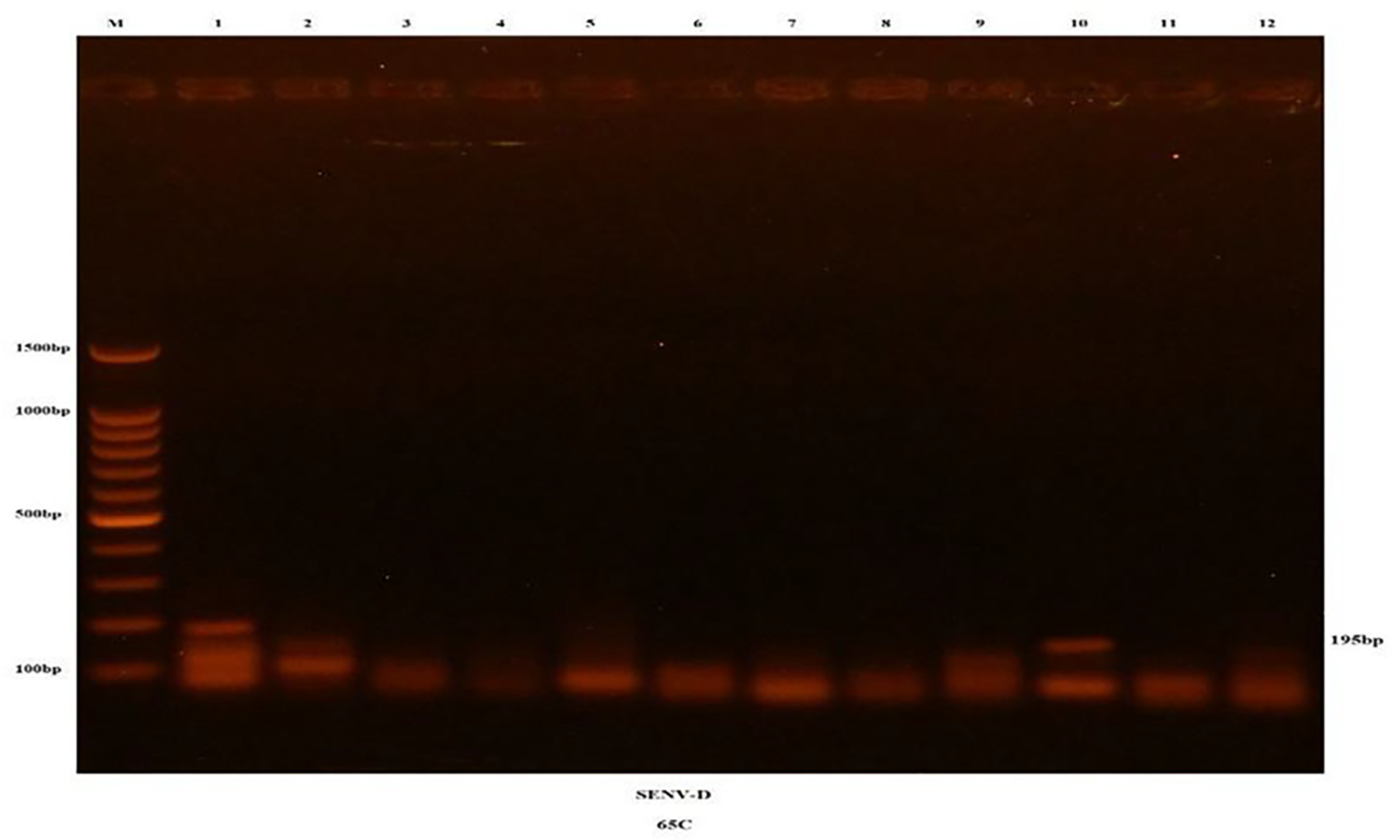
The amplified SENV-D-specific region from SENV samples was separated on a 1.5% agarose gel stained with ethidium bromide. M represents the 100-bp DNA ladder. Lanes 1–12 show PCR amplicons of approximately 195 bp. SENV, SEN virus.
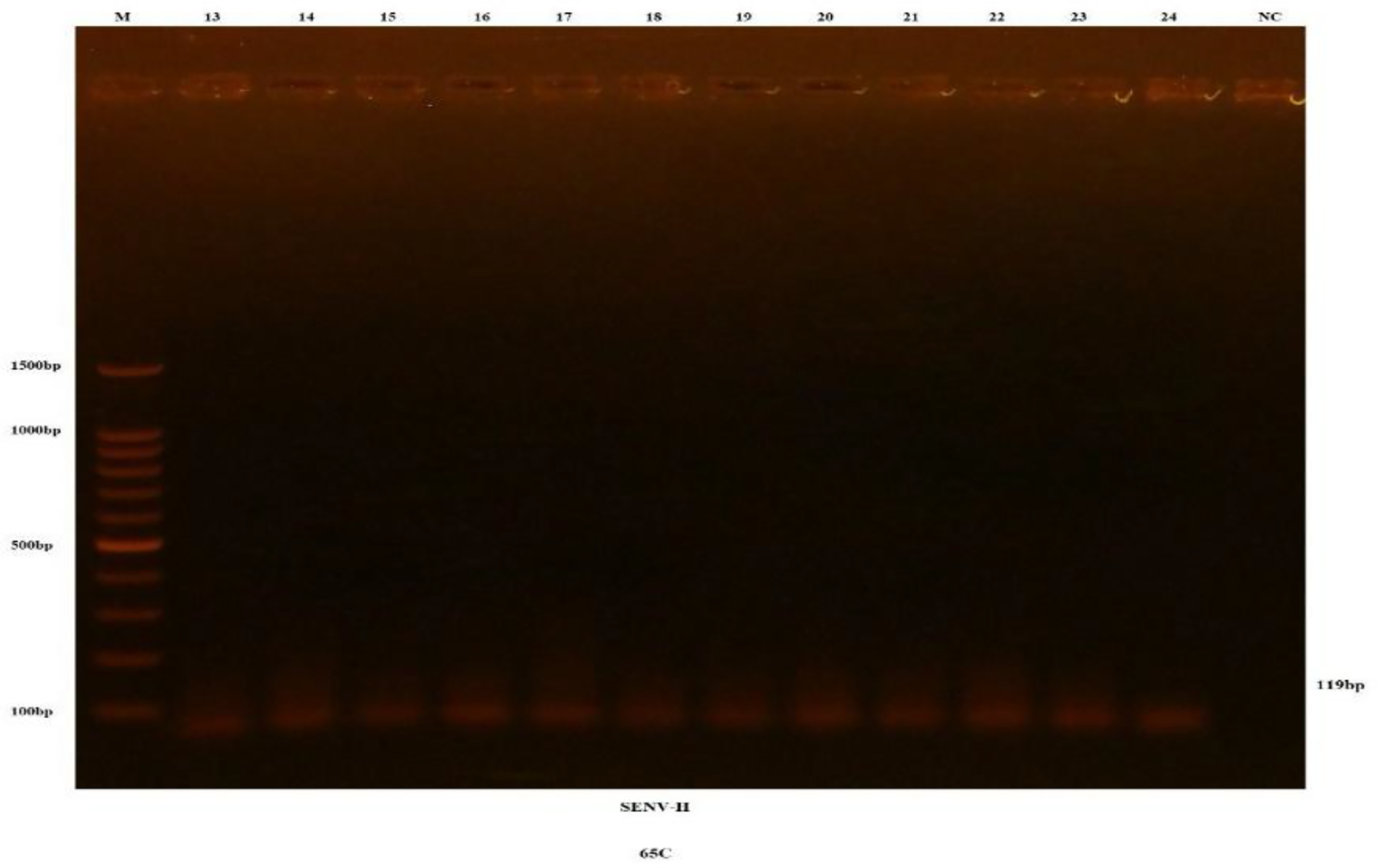
The amplified SENV-H-specific region from SENV samples was resolved on a 1.5% agarose gel stained with ethidium bromide. M denotes the 100-bp DNA ladder. Lanes 13–24 display PCR products of approximately 119 bp.
SENV-D, SENV-H, and SENV-D/H Prevalence Among the Studied Population
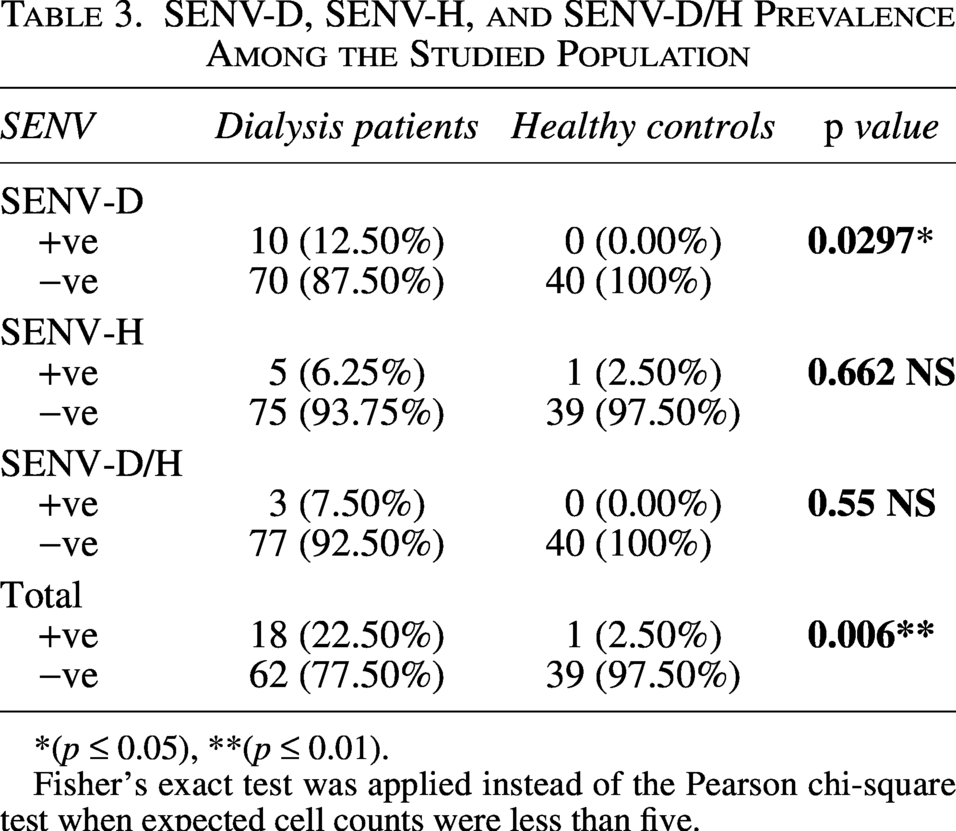
*(p ≤ 0.05), **(p ≤ 0.01).
Fisher’s exact test was applied instead of the Pearson chi-square test when expected cell counts were less than five.
Relationship between SENV genotypes and demographic factors and clinical data
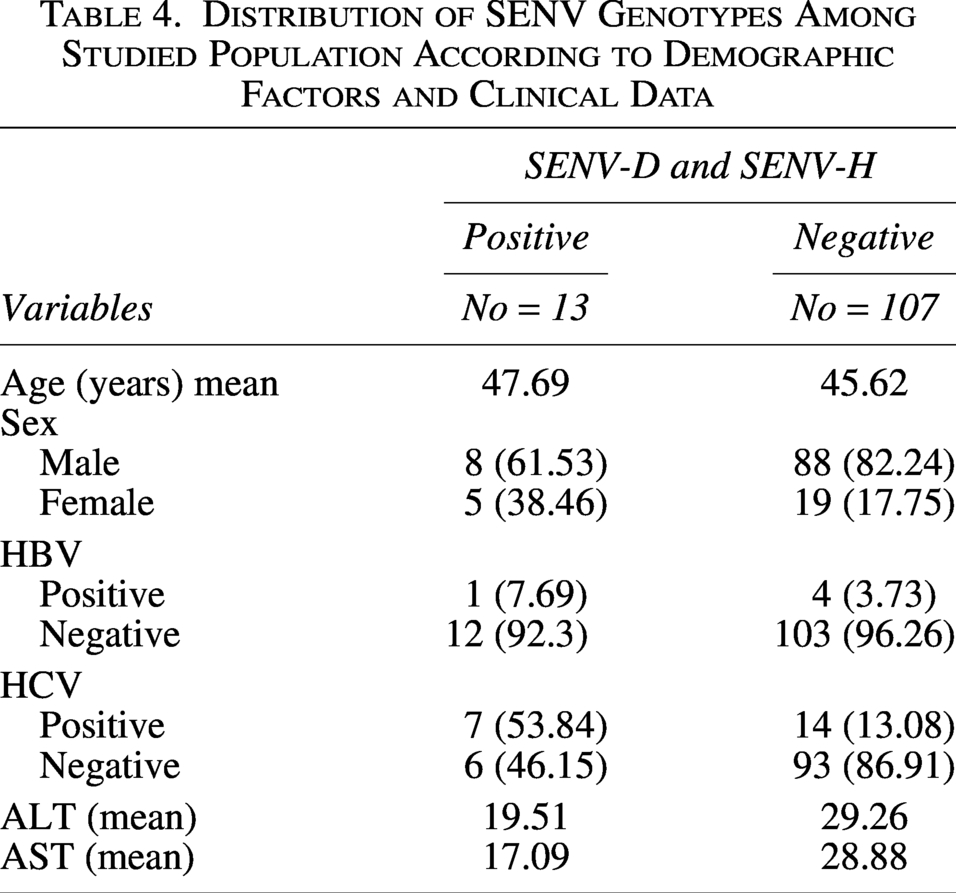
Table 4 revealed the association between SENV-D and SENV-H genotypes; age, sex, HBV, HCV, ALT, and AST in the population studied were 47.69, 8 (61.53) for males and 5 (38.46) for females, 1 (7.69), 7 (53.84), 19.51 and 17.09, respectively.
Distribution of SENV Genotypes Among Studied Population According to Demographic Factors and Clinical Data
Discussion
The current study showed the prevalence of SENV-D, SENV-H, and SENV-D/H was 10 (12.50%), 5 (6.25%), and 3 (7.50%), respectively, in dialysis patients, and only 1 (2.50%) of blood donors as controls were positive for SENV-H. This result is consistent with previous reports of SENV-D (5.4%) and SENV-H detection rates (17.4%, 1.1%) in Ahvaz, Iran (Abbasi et al., 2016). These values are also consistent with the frequency rates described by Elaskary et al. (2023), who reported SENV DNA in 67.5% of HD patients and 9.6% among matched control subjects. Moreover, the incidence of SENV has been found in Saudi Arabia with 9.3% prevalence (AL-Maqati et al., 2022). A higher prevalence of SENV infection was observed among dialysis patients, which may be associated with repeated blood transfusions and potential exposure to blood products. The low prevalence in the control group of healthy blood donors indicates that while the virus is present in the general population, dialysis patients are a particularly vulnerable group (Afkari et al., 2012; AL-Maqati et al., 2022; Kobayashi et al., 2003). The present study found the association between SENV-D and SENV-H genotypes, and HBV and HCV infection in the population studied were 7.69% and 53.84%, respectively, and these results are consistent with the findings of other researchers who had recorded similar results (Abbasi et al., 2016; AL-Maqati et al., 2022; Awad, 2018; Elaskary et al., 2023; Hosseini and Bouzari, 2016). Also in the current study, the relationship between SENV-D and SENV-H genotypes with age and gender was examined, and the results were found to be consistent with the results of other researchers (e.g., Elaskary et al., 2023; Ali et al., 2022; and Pirouzi et al., 2014) who showed a non-significant relation of SENV with age and sex. However, the current study found a relationship between SENV-D and SENV-H with ALT and AST, and these results were inconsistent with other studies (Abd El-Hady et al., 2006; AL-Maqati et al., 2022; Al-Shuwaikh, 2020; Elaskary et al., 2023; Javanmard et al., 2024). The effect of SEN virus on ALT and AST levels is varied, with some studies finding no significant difference, while others show increased levels in SENV-positive individuals, particularly in co-infections with other viruses. Previous research has suggested that SENV infection may not significantly alter liver enzyme levels or may be linked with normal ALT/AST readings; however, our data showed a favorable correlation between certain SENV genotypes and raised liver enzymes. This variation may be due to study demographic characteristics, sample size, dialysis duration, and co-infections such as HBV or HCV. Age and sex distribution may have also affected biochemical results. We cannot exclude residual confounding due to the cross-sectional design (Al-Shuwaikh, 2020; Javanmard et al., 2024). SENV and liver enzymes may be confused by HCV co-infection. SENV subtypes A and B do not affect HCV chronic infection, and patients coinfected with SENV and HCV had similar ALT levels to those infected with HCV alone. However, more research is needed to determine if HCV infection affects plasma SENV replication. The study found no significant effect of SENV infection on liver enzyme levels in chronic HCV patients. Despite the study’s important findings, numerous limitations should be noted. First, the control group was not adequately matched with the dialysis group in age and sex distribution, which may have affected the results and should be noted when interpreting them. Second, the PCR results were not sequenced to establish genetic specificity, which may reduce genotype identification accuracy. HCV co-infection may also complicate the link between SEN virus infection and liver enzyme levels. Therefore, interpret the reported relationships with caution. More research with bigger sample sizes, well-matched control groups, and PCR product sequencing is needed to corroborate these findings.
Conclusion
Hemodialysis patients had higher SENV genotypes than healthy controls, which may be connected to liver enzyme levels. The prevalence of SENV in dialysis patients and healthy blood donors emphasizes the need for comprehensive blood screening for all viral agents, including HIV, HBV, and HCV. SENV is a blood-borne infection that can cause non-A to non-E hepatitis when transferred from donor to recipient. SENV-D and SENV-H are discovered in dialysis patients and blood donors. Further research is needed to understand the epidemiology and pathogenesis of SENV, particularly its impact on the liver and kidney. Large-scale long-term studies are needed to clarify SENV’s pathogenic role, co-infections, dialysis duration, and long-term treatment implications.
Authors’ Contributions
Conceptualization was carried out by A.D.S., I.H.M., and L.G.A.; Methodology was developed by A.D.S.; Validation was performed by I.H.M.; and formal analysis was conducted by L.G.A. The investigation was undertaken by all three authors, while data curation were managed by A.D.S. and L.G.A. Writing original draft preparation was completed by A.D.S., with review and editing by. Visualization was contributed by I.H.M. and L.G.A. All the authors have read and agreed to the published version of the article.
Footnotes
Acknowledgments
The authors thank the Department of Biology, College of Sciences, Diyala University, Diyala, Iraq, and the Department of Microbiology, College of Sciences, Mustansiriyah University, Baghdad, Iraq, for providing materials and instruments for necessary technical support.
Data Availability Statement
The authors declare that all the data supporting the findings of this study are available within the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.