
Abstract
Hypoxic–ischemic encephalopathy is an important cause of neuropsychological deficits. Little is known about brain diffusivity in these infants following cooling and its potential in predicting outcome. Diffusion tensor imaging was applied to 3 groups: (1) three infants with hypoxic–ischemic encephalopathy: cooled; (2) three infants with hypoxic–ischemic encephalopathy: noncooled; and (3) four controls. Diffusivity values at the corticospinal tract, thalamus, and putamen were correlated with Apgar scores and early neurodevelopmental outcome. While cooled infants exhibited lower Apgar scores than noncooled infants, their developmental scores at a mean age of 8 months were higher. All groups differed in their diffusivity values with the cooled infants showing better values compared with the noncooled, correlating with early neurodevelopmental outcome. These preliminary results indicate that diffusion tensor imaging performed at an early age in infants with hypoxic–ischemic encephalopathy may forecast clinical outcome and support the neuroprotective effect of hypothermia treatment.
Hypoxic–ischemic encephalopathy is a severe neurological complication in live-born, term infants with an incidence of 2 to 4 in every 1000.1,2 Several patterns of hypoxic–ischemic brain injury have been described involving the basal ganglia, brainstem, corticospinal tracts, sensorimotor cortex, and white matter in various overlapping combinations. The pervasiveness of brain damage depends on brain maturation and the severity and duration of reduced oxygenation and blood flow to the infant’s brain. Between 10% to 15% of infants with hypoxic–ischemic encephalopathy die during the neonatal period, 3 while in 25% to 45% of those who survive, permanent neuropsychological deficits, such as cerebral palsy, mental retardation, learning disability, and epilepsy may be present.1,2,4
Recently, therapeutic hypothermia has been adopted as the standard of care in some parts of the world for the treatment of infants with hypoxic–ischemic encephalopathy 5 who fulfill specific inclusion and exclusion criteria. 6 Whole-body cooling or selective head cooling are induced by maintaining the infant rectal temperature between 32°C and 34°C for 72 hours. Such treatments have been shown to improve neurological outcome in survivors with reduced risk of cerebral palsy and improved scores on mental and motor development functions.6–8 However, few studies have used advanced magnetic resonance imaging (MRI) to demonstrate the impact of this neuroprotective strategy on the brain of these infants and its potential in predicting outcome.1,6,7,9
Abnormal magnetic resonance (MR) signal intensity in several brain regions, including the posterior limb of the internal capsule, periventricular white matter, cortex, basal ganglia, and thalami, were documented in infants with hypoxic–ischemic encephalopathy using conventional MR methods (T1 and T2 weighted images).10,11 Following hypothermia therapy, a significant reduction in lesions in the basal ganglia or thalamus, white matter, and posterior limb of the internal capsule, was reported. 7
Diffusion tensor imaging provides additional information regarding white matter integrity, tissue organization, maturation, and pathology. 12 The various diffusivity indices provide deeper insight into the brain’s microstructural changes. The most common diffusivity indices are: (1) axial diffusivity—indicating the direction in which water diffusion is highest, typically parallel to white matter fiber fascicles and considered to reflect axonal growth; (2) radial diffusivity—the diffusion perpendicular to the axis 13 considered to reflect axonal width and myelination14,15; (3) apparent diffusion coefficient—the average values of the radial and axial diffusivity, providing information regarding brain maturation; and (4) fractional anisotropy—that describes the water diffusion anisotropy (directional dependence), considered to reflect tissue integrity and development.12,16,17
Abnormal fractional anisotropy (lower values) and mean diffusivity (higher values) found in various brain regions were suggested to predict unfavorable functional outcome in infants with hypoxic–ischemic encephalopathy.18,19 In a recent study, abnormal fractional anisotropy values were detected in the anterior and posterior limbs of the internal capsule, the corpus callosum, and optic radiations in noncooled infants with this complication but only in the internal capsule in the cooled group. 9
Another study suggested the use of MRI, including diffusion tensor imaging, as a predictive tool for neurodevelopmental outcome of infants with hypoxic–ischemic encephalopathy. 20 Yet, the correlation between diffusion tensor imaging findings and neurodevelopmental outcome following cooling is still limited.
The aim of our study was to investigate the effect of hypothermia in infants with hypoxic–ischemic encephalopathy using diffusion tensor imaging, and to determine the correlation of these findings with both Apgar scores and with early neurodevelopmental outcome.
Methods
In this study, we analyzed MRI data of the first infants with hypoxic–ischemic encephalopathy to be treated with hypothermia in Tel Aviv Sourasky Medical Center 21 and in Laniado hospital, and compared these findings with MRI data of asphyxiated infants who were not cooled, and with nonasphyxiated neonate controls. MRI scans were acquired at ages 1 to 7 weeks, while neurodevelopmental assessments were performed at the age of 6 to 10 months.
Subjects
The following 3 groups of subjects were studied, comprising a total of 10 infants: (1) three infants with hypoxic–ischemic encephalopathy underwent hypothermia therapy (cooled); (2) three infants with hypoxic–ischemic encephalopathy underwent standard therapy (noncooled); and (3) four were healthy controls. Subjects' details are presented in Table 1 .
Subject Details
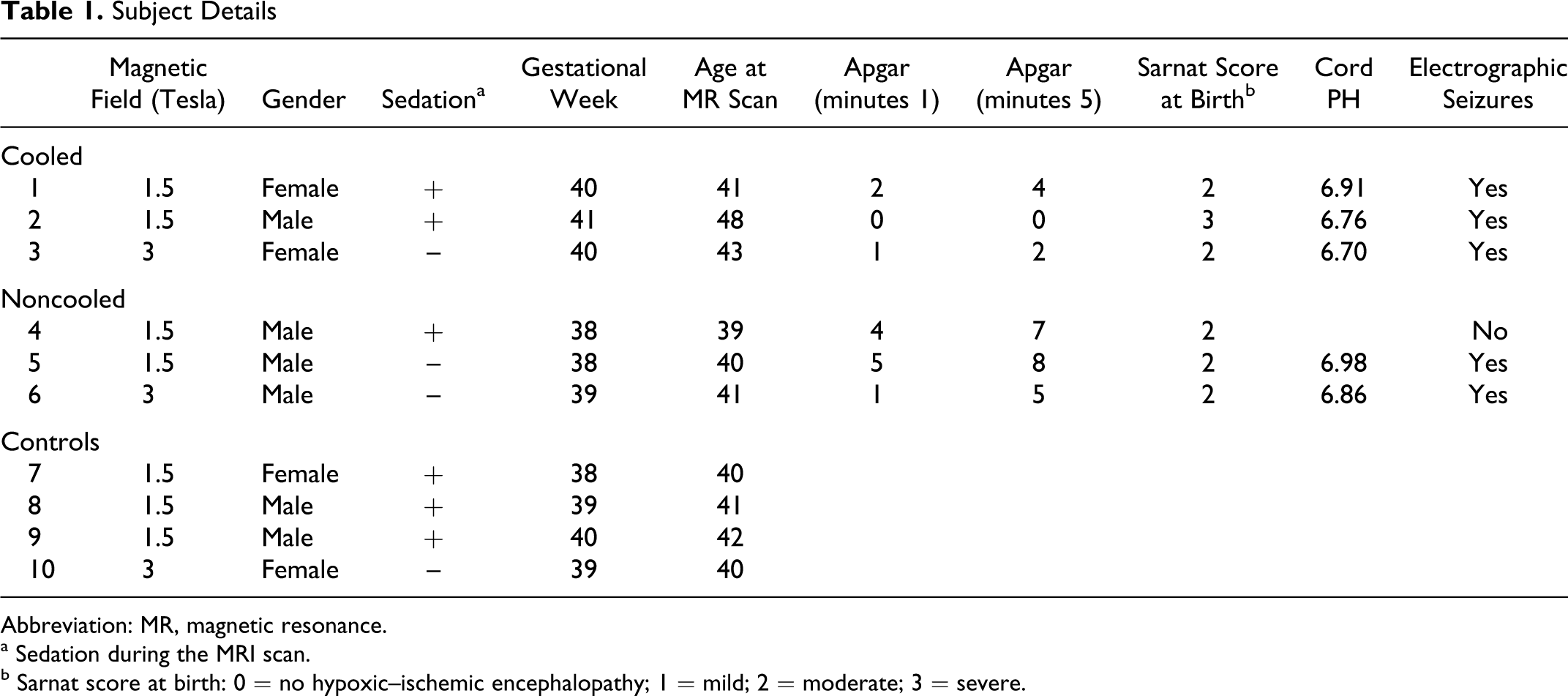
Abbreviation: MR, magnetic resonance.
a Sedation during the MRI scan.
b Sarnat score at birth: 0 = no hypoxic–ischemic encephalopathy; 1 = mild; 2 = moderate; 3 = severe.
Study Groups
Cooled infants with hypoxic–ischemic encephalopathy
Three asphyxiated term infants that fulfilled all criteria for hypothermia treatment underwent cooling based on clinical criteria as published by large trials.22,23
Noncooled infants hypoxic–ischemic encephalopathy
Three asphyxiated term infants were not cooled. One infant (subject number 6) was born in another hospital, where a cooling facility was not available. The other 2 infants (subjects number 4 and 5) had perinatal asphyxia but were not cooled because they did not fulfill all clinical inclusion criteria for hypothermia therapy.
Whole body therapeutic hypothermia was initiated within 6 hours of birth. Infants were placed on the hypothermia blanket (CritiCool unit, MTRE advanced technologies, Israel) and set to an automatic control mode at 33.5°C for the rectal and skin probe. All noncooled infants underwent standard treatment with temperature control to maintain the rectal temperature at 37°C (normothermia).
All infants demonstrated clinical and MRI findings consistent with hypoxic–ischemic injury, reconfirming the diagnosis
Healthy controls
Four term infants were referred to MR examination for various clinical indications (Table 1). All subjects demonstrated no brain anomalies on conventional MRI.
Neurodevelopmental Follow-up
All infants with hypoxic–ischemic encephalopathy were followed up at the neonatal neurology outpatient clinic at Tel Aviv Sourasky Medical Center by the same pediatric neurologists and a physical therapist. A detailed neurological examination was performed for each infant, including assessments of head circumference, neuromotor function (deep tendon reflexes, muscle tone, muscle strength), cranial nerves, and sensation. In addition, the Battelle Developmental Inventory screening test was administered, assessing personal, social, adaptive, motor, communication, and cognitive domains. A total screening score was then derived, from which developmental age was recorded. The child’s developmental age, divided by the chronological age, and multiplied by 100, yielded the developmental quotient score. Battelle’s developmental quotient has a mean of 100 and a standard deviation of 15.
MRI Protocol
MRI scans were performed either on a 3 Tesla Signa HDXT or on a 1.5 Tesla Signa HD General Electric scanner (Milwaukee, Wisconsin). Six MR scans were performed under sedation, while the remaining 4 scans were performed without sedation (Table 1). For nonsedated infants, the MR setup was performed according to Mathur et al. 24 Briefly, infants were fed approximately half an hour before the procedure. During the scan, infants were warmed and wrapped in a special cover and mattress. Noise was reduced by using adapted neonatal noise guards and a special microphone, with a noise cancellation system (Optoacoustics, Or Yehuda, Israel), was used to monitor any distress of the infant. For all subjects, blood oxygen saturation and pulse were monitored during the entire scan. MRI scans included conventional imaging: T1 weighted, T2 weighted, fluid attenuation inversion recovery, and gradient echo T2-weighted imaging. In addition, diffusion tensor imaging was performed with the following parameters: a set of axial gradient echo-echo planar images covering the entire brain; a slice thickness of 2.5 mm; no gap; and 33 diffusion gradient directions (b values = 0, 700 sec/mm2).
Data Analysis
Preprocessing of the diffusion data was performed using FSL 4.1 (FMRIB Software Library; University of Oxford, Oxford, UK). After applying eddy current and motion corrections, fractional anisotropy, mean diffusivity, axial diffusivity, and radial diffusivity, maps were calculated using FMRIB’s diffusion toolbox. The following 3 volumes of interest were defined based on adult brain atlases: (1) right and left corticospinal tract (obtained from the Juelich histological atlas); (2) right and left thalamus, and (3) right and left putamen (obtained from the Harvard-Oxford structural atlas). The defined volumes of interest were aligned to each subject’s images using an FMRIB linear image registration tool (Figure.1 ). All volumes of interest were carefully inspected in each subject.
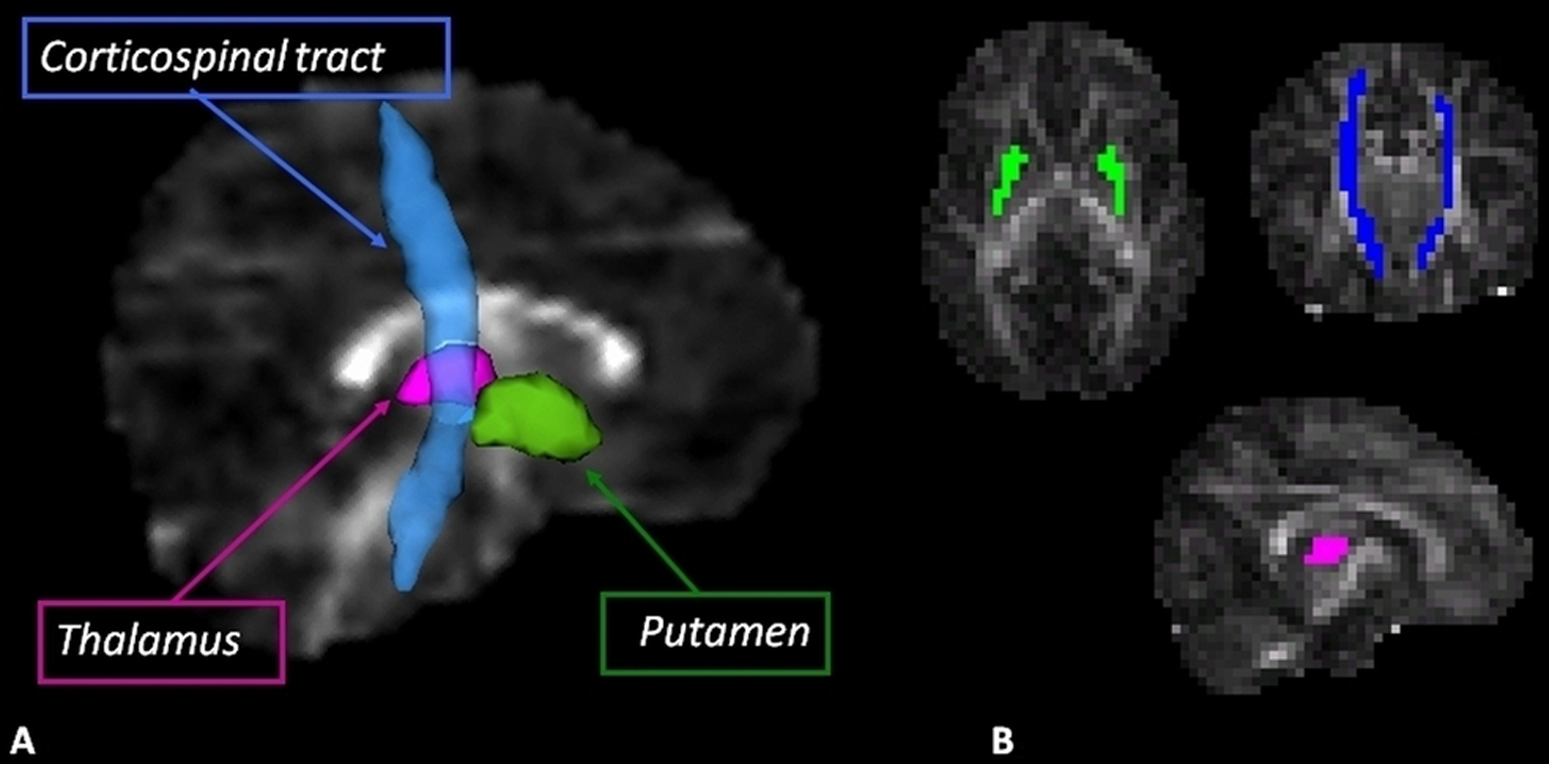
The defined volumes of interest, superimposed on a fractional anisotropy image of a 7-day-old healthy infant, 3D visualization (A), and axial, coronal, and sagital orientations (B).
Mean diffusivity value was calculated in all volumes of interest and mean fractional anisotropy, axial, and radial diffusivities were additionally calculated in the white matter areas. The diffusivity values of the 2 hypoxic–ischemic encephalopathy groups (cooled and noncooled) were compared with the healthy subjects and to normal reference values.25–28 This study was approved by the Institutional Review Board of Tel-Aviv Sourasky Medical Center.
Results
Clinical Results
Apgar scores at 1 and 5 minutes in cooled infants were much lower than those of the noncooled group (Table 1). The hypoxic–ischemic encephalopathy Sarnat scores of the 2 groups were similar. Apgar scores were normal for the control group.
Results of neurodevelopmental outcome at a median age of 8 months (range, 6.6-10.4 months) are shown in Table 2 . The neuromotor examination was normal in all 3 cooled infants and abnormal in 2 out of 3 infants in the noncooled group. Developmental quotients were abnormal (<2 standard deviations) in the 2 hypoxic–ischemic encephalopathy groups, yet the median developmental quotient of the noncooled group (38.5; range, 9.8-67.3) was much lower than that of the cooled group (66.6; range, 60.6-69.4).
Neurodevelopmental Outcomes
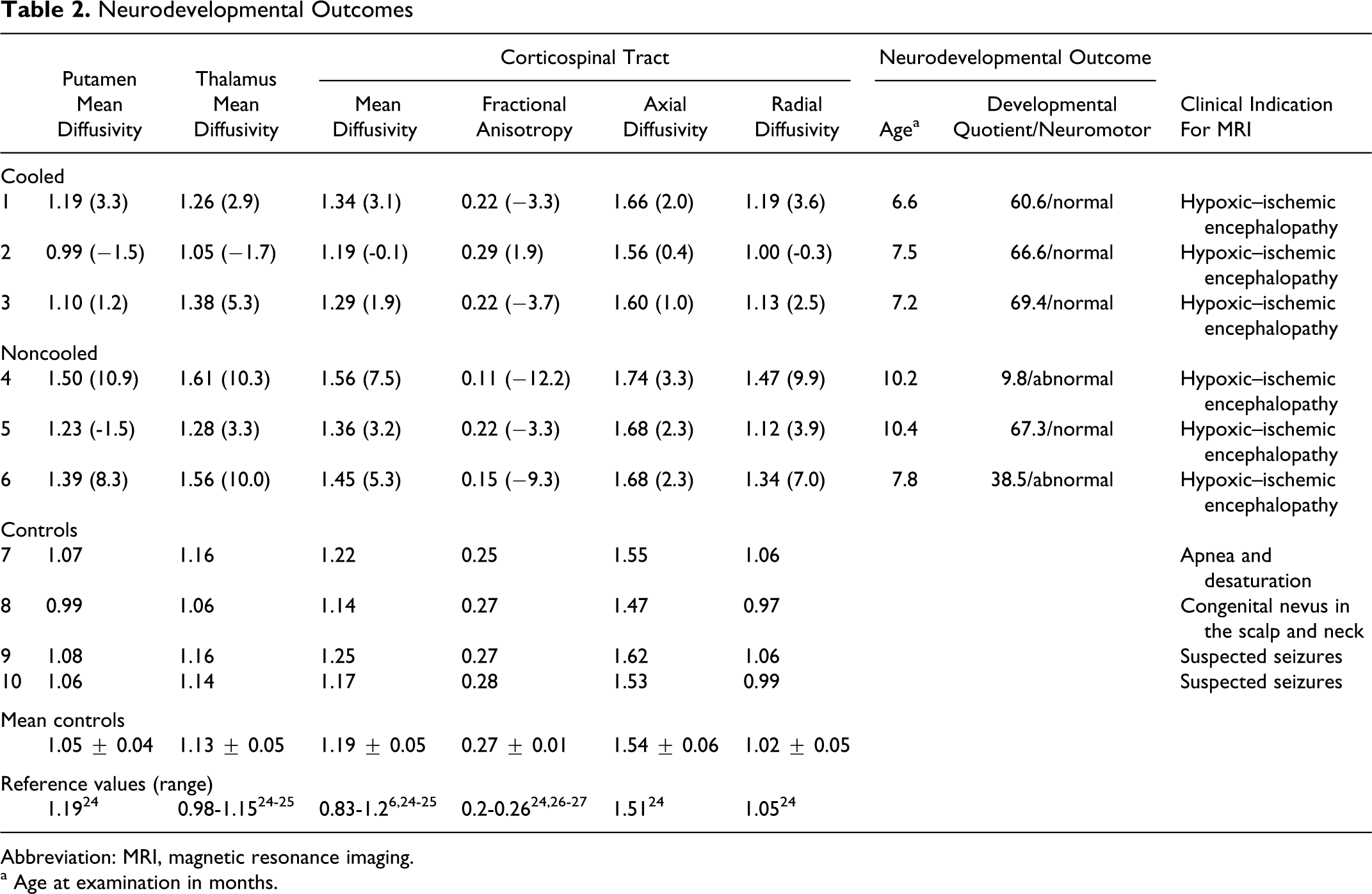
Abbreviation: MRI, magnetic resonance imaging.
a Age at examination in months.
Imaging Results
Diffusivity values of all subjects obtained in the 3 volumes of interest (averaged values of the right and the left hemispheres) are presented in Table 2. The distance in standard deviations from the normal values are given in brackets. Diffusivity values obtained from the control infants were in agreement with previously reported normal values.25–28 Figure 2 shows mean diffusivity values of the 3 groups obtained in the corticospinal tract, thalamus, and putamen, versus age.
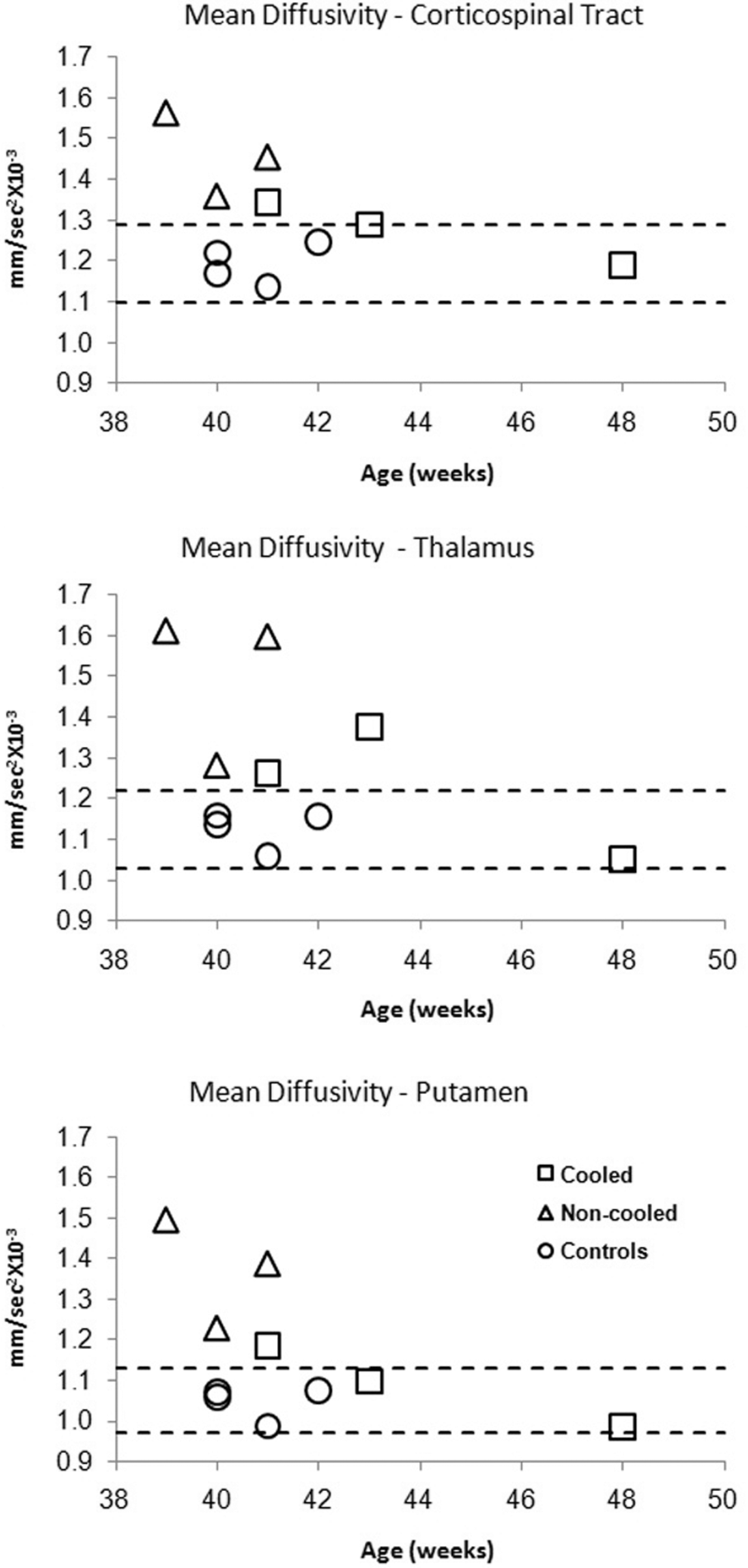
Mean diffusivity values of all subjects detected at the corticospinal tract (A), thalamus (B), and putamen tract (C). Dashed lines indicate 2 standard deviations confidence intervals.
Diffusivity values in the cooled infants were more similar to those of the control group and to values found in the literature (Table 2, Figure 2) in all measured volumes of interest, compared with those of the noncooled group (smaller distance from the normal values). In the noncooled infants, all diffusivity values were abnormal, differing by more than 3 standard deviations from normal values except for axial diffusivity in the corticospinal tract. Two infants in this group (infants number 4 and 6) demonstrated more abnormal diffusivity values, indicating a higher degree of tissue impairment in all measured brain areas (manifested by higher mean diffusivity values in the thalamus, putamen, and corticospinal tract; reduced fractional anisotropy values and increased radial diffusivity in the corticospinal tract). Abnormal values were also detected for the axial diffusivity, but were less remarkable (Table 2). The third noncooled infant (infant number 5) demonstrated diffusivity values similar to those of the cooled infants. Figure 3 shows a scatter plot of developmental quotient scores of the hypoxic–ischemic encephalopathy infants and mean diffusivity values detected in the putamen. Because of the small number of subjects, statistical analysis was not performed; however, a trend of correlation between developmental quotient and mean diffusivity in the putamen can be seen.
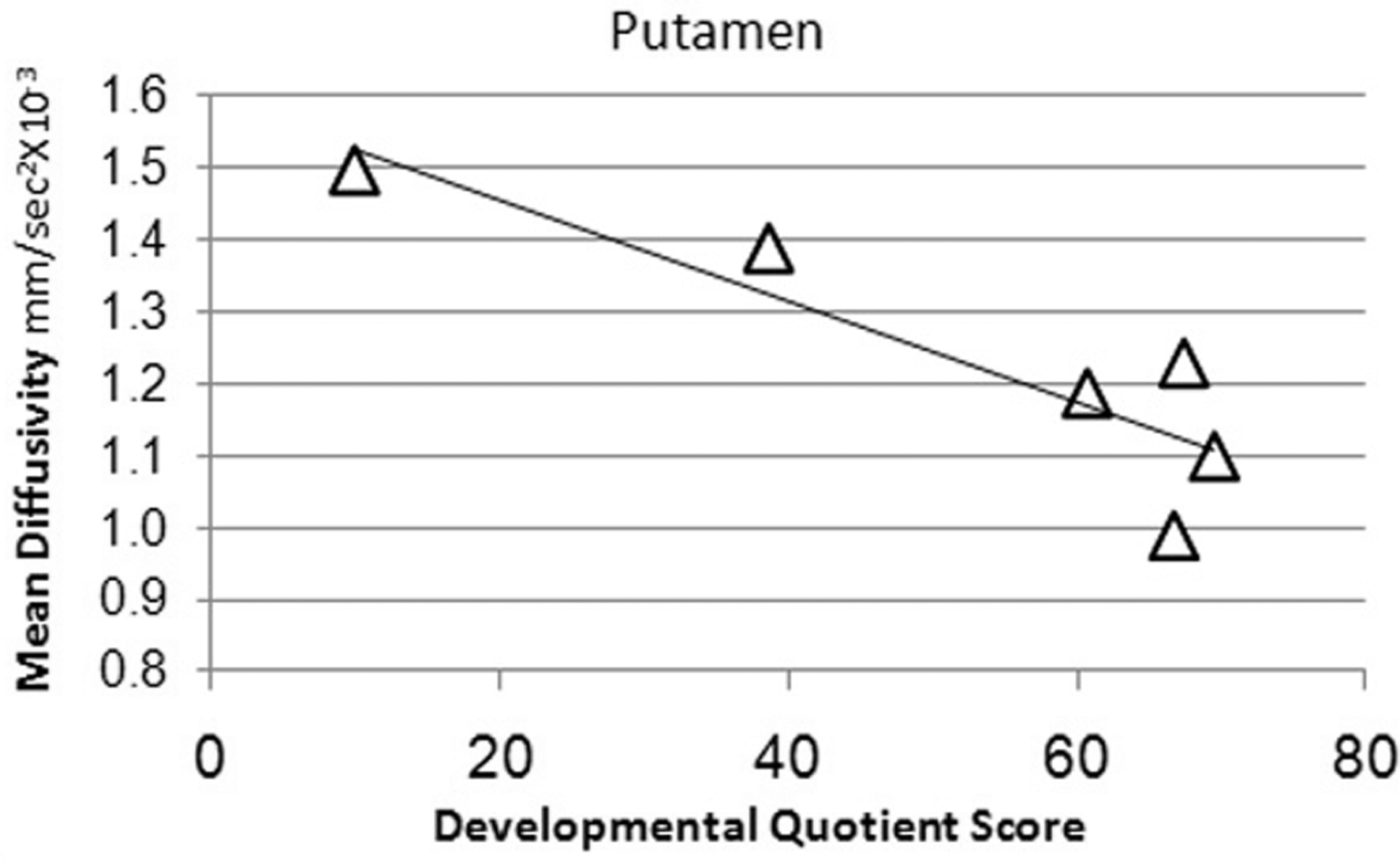
Mean diffusivity and developmental quotient score in infants with hypoxic–ischemic encephalopathy.
Discussion
This study evaluated the effect of hypothermia therapy in infants with hypoxic–ischemic encephalopathy using diffusion tensor imaging and correlated imaging findings with Apgar scores and with early neurodevelopmental outcome. Preliminary results showed that infants with hypoxic–ischemic encephalopathy treated with hypothermia had less abnormal diffusivity values compared with infants who were not treated with hypothermia, which may indicate less damage to their brain. In addition, the cooled infants demonstrated better early neurodevelopmental outcome in spite of lower Apgar scores at birth compared with the noncooled infants.
In the present study, diffusivity values were in line with developmental quotient scores. These results confirm previous research that support diffusion tensor imaging as a good predictor of early neurodevelopmental outcome in infants with hypoxic–ischemic encephalopathy.28,29 In this study, Apgar scores were taken into account, enabling evaluation of the effects of hypothermia. The effect of hypothermia therapy on the asphyxiated brain could have been assessed more accurately using repeated MRI examinations before and after cooling. However, because hypothermia must be applied as soon as possible (within 6 hours of birth) such dual scanning may not be feasible. To evaluate the efficacy of hypothermia therapy, a methodology based on reference values, which can be correlated to clinical and neurodevelopmental assessments, as was performed in this study, is most appropriate.
The results of this study may corroborate the neuroprotective effect of hypothermia on brain tissue. Hypothermia therapy has already shown promising results in various pathologies30,31 and has been associated with reduced lesions in infants with hypoxic–ischemic encephalopathy in brain areas related with abnormal neurodevelopmental outcome, 32 and a differential protection of the cortex was suggested. 33 Yet, quantitative advanced MRI studies demonstrating the effect of this therapy and its correlations with clinical outcomes are limited.
The diffusion tensor imaging analysis in this study used automatic volume of interest definition on each subject image, providing quantitative measurements of the diffusivity values. Previous studies of infants with hypoxic–ischemic encephalopathy used either manually defined volumes of interest, visual assessment of the diffusion images, or voxel-based whole brain analysis.8,9,32,33 Manually defined volumes of interest less accurate, time consuming, and have significant intersubject variability. Other automatic methods usually require data normalization, which may cause image distortion. The analysis methodology used in this study enables automatic definition of several volumes of interest and can be easily applied to studying several brain regions in a large number of subjects.
Our results showed abnormal (increased) mean diffusivity values in all measured brain regions in all infants with hypoxic–ischemic encephalopathy compared with healthy controls. Diffusivity values are very sensitive indices that change rapidly following ischemic injury, indicating tissue destruction before it can be detected on conventional imaging.14,34 These changes include a reduction in mean diffusivity values during the first week, pseudo-normalization during the second week, followed by an increase in mean diffusivity values.35 Thus, diffusivity values are highly dependent on the time of scanning relative to the onset of the ischemic event. In this study, all infants were scanned at least 5 days after the ischemic event, and all showed increased mean diffusivity. Future longitudinal studies may help to better understand and define the time course of changes in diffusivity values at this age and in this pathology.
In this study, various diffusivity indices were studied and abnormal radial diffusivity values were detected in the corticospinal tract, while changes in axial diffusivity values, although noted, were less remarkable. Most studies in infants with hypoxic–ischemic encephalopathy using diffusion tensor imaging based their results solely on fractional anisotropy and mean diffusivity values. Axial and radial diffusivity can provide additional information regarding the pathomechanism underlying tissue destruction. Abnormal radial diffusivity values, as found in this study, might suggest abnormal myelination in the corticospinal tract. 16 The small number of subjects in this study prevents us from drawing a firm conclusion, yet the results do highlight the importance of studying the various diffusivity indices in this pathology.
Limitations to be considered are the use of 2 different magnetic fields for infant scanning and referral of infants to the control group based on various clinical indications. However, identical acquisition parameters were maintained in both systems and similar normal diffusivity values were obtained in both magnetic fields, matching literature values. Moreover, even when controlling for the magnetic fields, similar differences between the groups were obtained for all diffusivity values. It is important to note that the initial promising results may reflect not only the cooling effect, but also prenatal processes that were not fully evaluated in our study. This study presents preliminary results from a small group of infants. Our results must be confirmed on a large scale before a reliable conclusion can be drawn on the neuroprotective effect of hypothermia treatment following hypoxic–ischemic encephalopathy.
In conclusion, our preliminary study demonstrated that infants with hypoxic–ischemic encephalopathy treated with hypothermia had less abnormal diffusivity values compared with infants who were not treated with hypothermia. This may indicate less damage to the studied brain areas in the cooled infants that correlated with better early neurodevelopmental outcome compared with the noncooled infants. Diffusion tensor imaging quantification may provide an imaging biomarker to measure the efficacy of hypothermia treatment in asphyxiated infants and to predict their future developmental outcomes.
Footnotes
Acknowledgments
The authors are grateful to the infants and their families who so willingly participated in this study. The authors thank Vicki Myers for editorial assistance.
MA and LBS are both first authors who contributed equally to this work. MA contributed to the data analysis and manuscript preparation. LBS was the pediatric neuroradiologist in charge of MRI scanning, who also contributed to MRI interpretation and manuscript preparation. HB was the pediatric neurologist in charge of data collection, who also contributed to neurological and developmental outcome examinations and assisted in patient recruitment and in manuscript preparation. VG-T, YL, and RG were the pediatric neurologists/pediatric psychologists who contributed to clinical outcome assessment and manuscript preparation. IB, RM, YB, and YS were the neonatologists responsible for infant care, including hypothermia therapy and clinical monitoring during MR scanning. They also assisted in manuscript preparation. MW assisted in data analysis and research coordination. DBB was the senior researcher, contributing to project management, data analysis supervision, and manuscript preparation.
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.
Approval was received from the Tel Aviv Sourasky Medical Center Ethics Board.