
Abstract
The aim of the study is to assess mandibular function in young patients with spinal muscular atrophy type II. A total of 12 children and young adults with spinal muscular atrophy type II and 12 healthy matched controls participated. The mandibular function impairment was moderate to severe in 50% of patients. A limited mouth opening (≤30 mm) was observed in 75% of the patients. In patients with a severe reduction of the mandibular range of motion the temporomandibular joint mainly rotated during mouth opening instead of the usual combination of rotation and sliding. The severity of the limited active mouth opening correlated with the severity of the disease (motor function measure scores). This study shows that mandibular dysfunction is common among young patients with spinal muscular atrophy type II. Early recognition of mandibular dysfunction may help to prevent complications such as aspiration as a result of chewing problems.
Spinal muscular atrophy is a severe neuromuscular disease characterized by degeneration of α motor neurons in the spinal cord, causing weakness and muscular atrophy. 1 With an incidence of about 1:6000 to 10 000 it is one of the most common autosomal recessive diseases and an important hereditary cause of childhood morbidity.2,3 Spinal muscular atrophy is caused by the homozygous deletion of the survival motor neuron 1 gene that has been mapped to chromosome 5q11.2–13.3. 4 Spinal muscular atrophy severity varies considerably, and age at onset and the extent of motor impairment are used to distinguish 4 subgroups.5–9
Problems with biting and chewing are often reported by patients with spinal muscular atrophy but there are few studies that have systemically addressed this issue. These studies mentioned feeding related problems, weaker bite force of the masticatory muscles, reduced range of mandibular motion, and craniofacial and dental malocclusions, which might cause chewing difficulties in children and young adults with spinal muscular atrophy type II.10–13 Rehabilitation and modern management of complications have improved the quality of life and life expectancy of children with spinal muscular atrophy. 14 Management of nonfatal complications of the disease, such as strong limitations in the mandibular function that compromise feeding, chewing, oral hygiene, and dental care becomes increasingly important. The mechanisms that cause mandibular dysfunction are not well known. Dysfunction of the temporomandibular joint, weakness of the masticatory muscles (mouth openers and closers), and reduced head balance may all be involved. Management of the mandibular dysfunction depends on insight in these mechanisms. The aim of the present study was to systemically investigate mandibular function by a combination of questionnaires and comprehensive clinical examination in young patients with spinal muscular atrophy type II.
Materials and Methods
A cross-sectional study was performed from June 2008 to June 2009. The studied population consisted of 12 patients with a genetically confirmed diagnosis of spinal muscular atrophy type II. Age limits were set from 5 to 19 years, to ensure patient cooperation. Patients with spinal muscular atrophy type II were recruited in the Netherlands from the following: the Department of Rehabilitation, Children’s Hospital, Radboud University Nijmegen Medical Centre; the Division of Surgical Sciences, Department of Oral-Maxillofacial Surgery, Prosthodontics, and Special Dental Care, and the Department of Temporomandibular Disorders and Orofacial Pain, University Medical Centre Utrecht; and the Multidisciplinary Neuromuscular Outpatient Clinic of the Wilhelmina Children Hospital (Spieren voor spieren Centre for pediatric neuromuscular disorders), University Medical Centre Utrecht. All patients were wheelchair bound and had weakness of the neck muscles and scoliosis of the spine. A total of 10 patients had been treated surgically for scoliosis.
A group of 12 healthy children and young adults matched for age and gender acted as a control group and gave their informed consent. They underwent the same clinical examination as the patients with spinal muscular atrophy.
The study was approved by the Committee on Research Involving Human Subjects of Arnhem, Nijmegen and Utrecht, the Netherlands, and informed consent of the parents and children was obtained.
Questionnaires
The patients completed 3 questionnaires. The first (Screen) was developed to assess pain characteristics in the head and neck region, and temporomandibular function.15,16 The second questionnaire (Mandibular Function Impairment Questionnaire) consists of 17 questions, which can be answered on a 5-point Likert scale to assess to what extent the patient has difficulties in performing particular mandibular functions such as chewing and yawning. The raw score of the scale (ranging from 0 to 1) can be converted to a qualitative level of impairment; no/low (I), moderate (II), and high (III). 17 Previous studies have considered the Mandibular Function Impairment Questionnaire to be a reliable and valid tool. 18 The third questionnaire (Patient Specific Approach) identifies complaints of mandibular function through the selection of activities from a list of 27 that cause discomfort. 19
Physical Motor Skills
Motor skills were assessed in 6 patients from the Department of Rehabilitation, Children’s Hospital, Radboud University Nijmegen Medical Centre, by using the motor function measure, performed by 1 physiotherapist. 20 Items 13 to 23 of the motor function measure test were designed to collect information about posture, arm and neck function, and head control.
Clinical Examination
Patients in this study were clinically examined following the validated procedure as described by Lobbezoo-Scholte et al.21,22 Clinical examination consisted of the following parts: history taking of the main complaints; the current and experienced limitations of mandibular function; the dental, medical, and personal history of the patient; an extraoral inspection of the head and neck; and an intra-oral inspection of the dentition and the soft tissues.
Mandibular function was assessed by examining the range of motion of the mandible, including active opening measured at the mesioincisal angle of the upper and lower front teeth (Figure 1), left and right lateral movement and protrusion, and passive mouth opening. The overbite and overjet were measured (Figure 1).
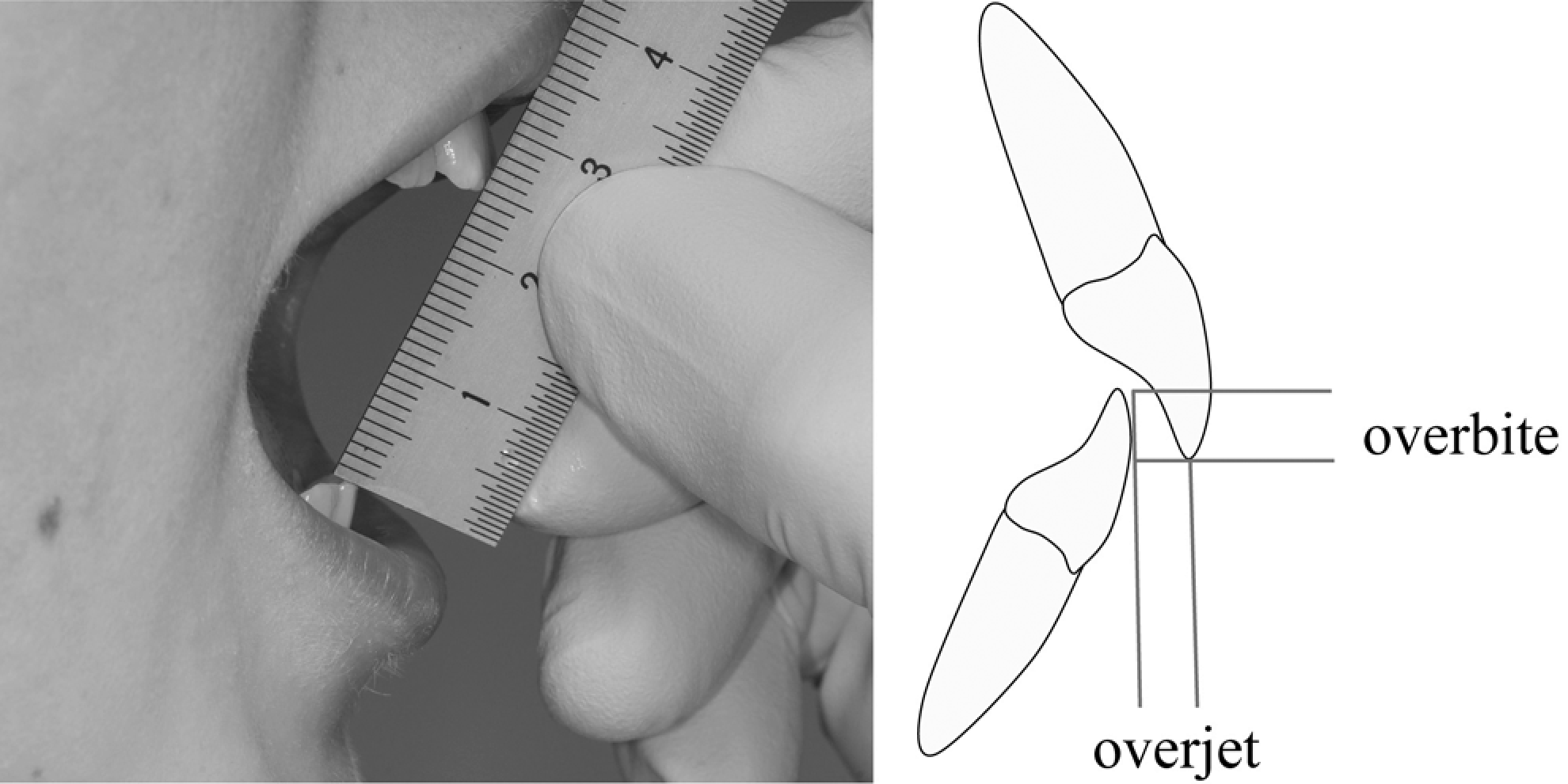
Measurement of the maximum voluntary mouth opening: the distance between the mesioincisal angle of the right upper and lower front teeth plus the overbite. Overbite refers to the vertical overlap of the front teeth and overjet to the horizontal overlap.
The patients' pain report during mandibular movements was recorded on a 5-point scale: 0 = no pain, 1 = mild, 2 = moderate, 3 = severe, 4 = very severe. The masticatory muscles (masseter, temporales, sternocleidomastoid, and occipital muscles) were palpated to assess painfulness. The temporomandibular joints were palpated on the left and right side with the mouth closed and open (lateral pole and posterior via the external acoustical meatus). Pain provocation and the extent of condylar movements were assessed. The mobility of the temporomandibular joint was assessed by traction and translation.
Statistical Analysis
SPSS 15.0 was used to analyze the collected data. The correlation between motor function measure scores and level of mouth opening was tested using the nonparametric Kendall rank correlation. The level of significance was set at P = .05.
Results
Patients with spinal muscular atrophy type II had a mean age of 11.8 years (range, 6 years and 4 months to 19 years); controls had a mean age of 12.3 years (range, 6 years and 4 months to 19 years and 3 months). Characteristics of the patients are summarized in Table 1.
Characteristics of the Spinal Muscular Atrophy Type II Group (n = 12) to Investigate Manbibular Function
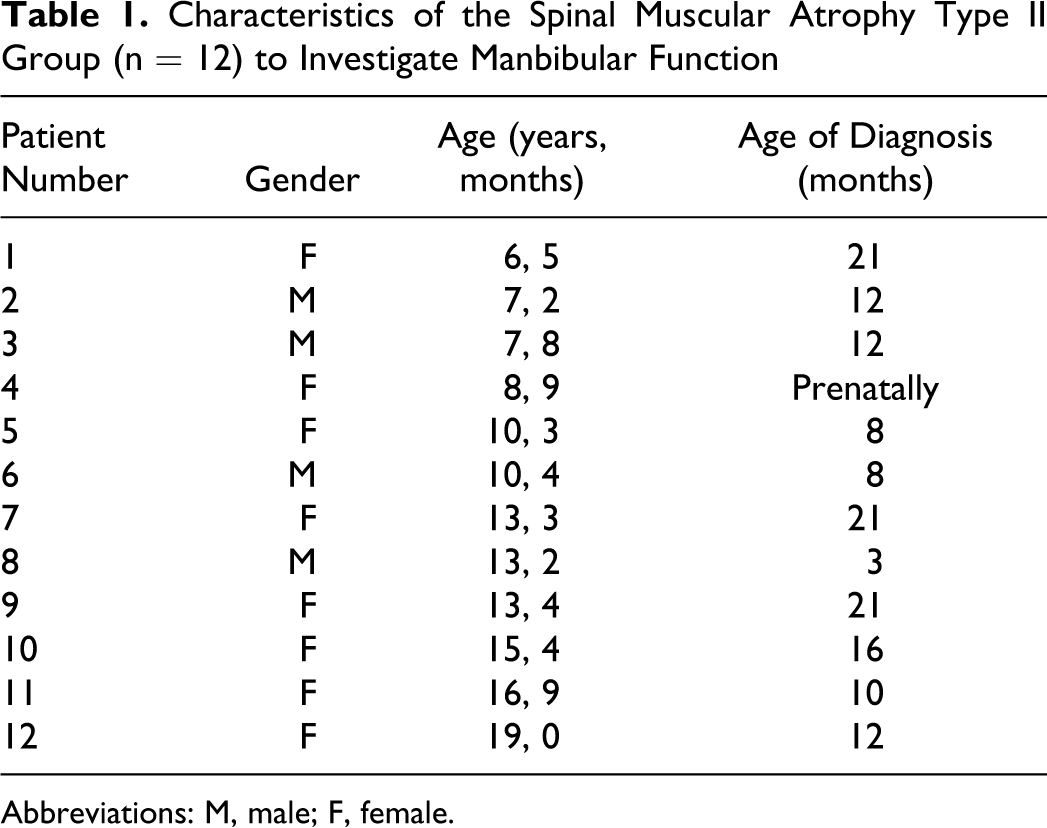
Abbreviations: M, male; F, female.
Questionnaires
Screen
One of the patients did not complete the questionnaires. The patients with spinal muscular atrophy type II did not spontaneously report pain in rest or when using the masticatory system. Three patients did not have chewing difficulties and did not report any limitation of mandibular function. Seven were aware of mouth opening limitations; however, they were not able to recall the time of onset of these limitations. They all experienced the limitations of mandibular function as a part of their disease.
Mandibular Function Impairment Questionnaire
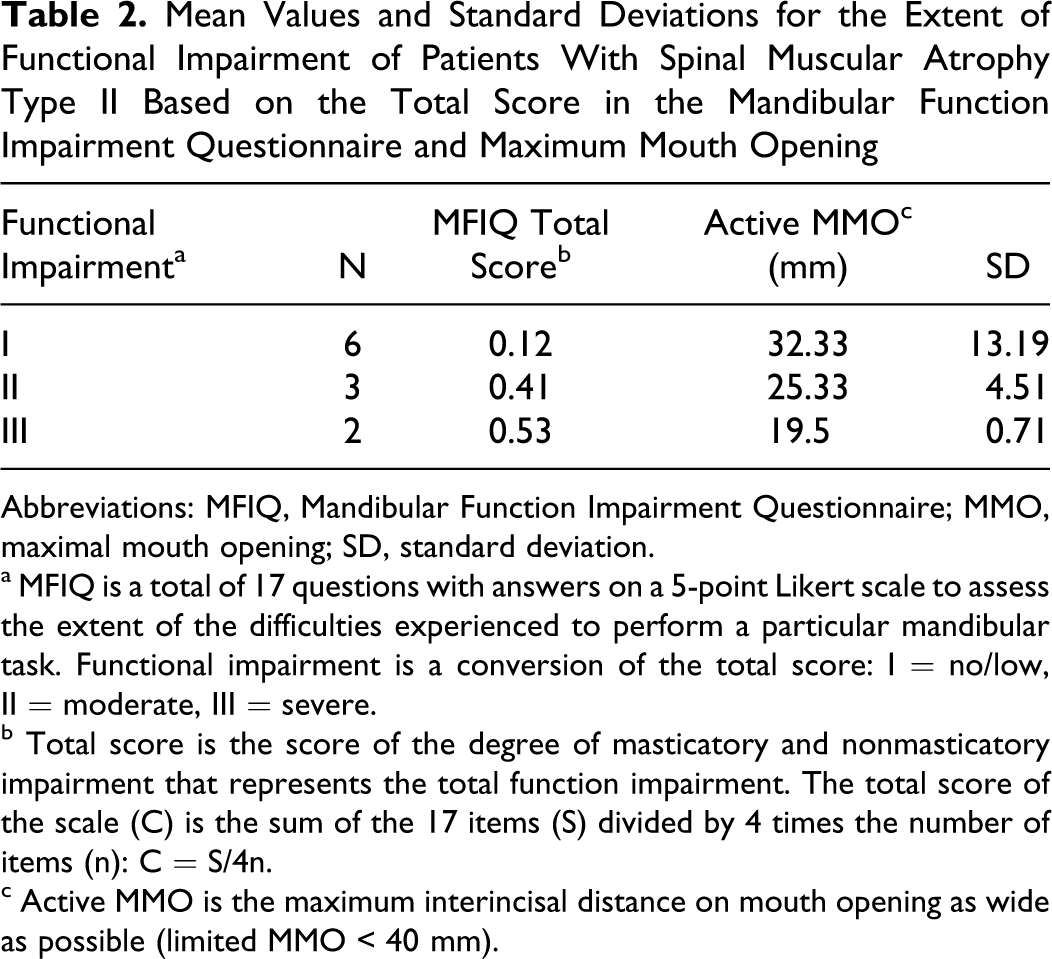
Functional impairment, expressed as the total score of the degree of masticatory and nonmasticatory impairment, ranged from 0 to 0.6 (Table 2). Two patients had a severe impairment, 3 had a moderate impairment, and 6 had no/low impairment.
Mean Values and Standard Deviations for the Extent of Functional Impairment of Patients With Spinal Muscular Atrophy Type II Based on the Total Score in the Mandibular Function Impairment Questionnaire and Maximum Mouth Opening
Abbreviations: MFIQ, Mandibular Function Impairment Questionnaire; MMO, maximal mouth opening; SD, standard deviation.
a MFIQ is a total of 17 questions with answers on a 5-point Likert scale to assess the extent of the difficulties experienced to perform a particular mandibular task. Functional impairment is a conversion of the total score: I = no/low, II = moderate, III = severe.
b Total score is the score of the degree of masticatory and nonmasticatory impairment that represents the total function impairment. The total score of the scale (C) is the sum of the 17 items (S) divided by 4 times the number of items (n): C = S/4n.
c Active MMO is the maximum interincisal distance on mouth opening as wide as possible (limited MMO < 40 mm).
Patient Specific Approach
The main complaints of the 9 patients with limitation of mandibular function assessed through Screen and the Mandibular Function Impairment Questionnaire were problems when chewing food, eating sticky and hard food, and brushing the teeth.
Physical Abilities
A total of 3 out of 6 patients from the Department of Rehabilitation, Children’s Hospital, Radboud University Nijmegen Medical Centre, had a low score on the motor function measure indicating problems with head balance. One out of 6 patients could keep head balance but had to compensate during item 14 of the motor function measure. Two out of 6 patients had no difficulty keeping head balance (Table 3).
Maximal Mouth Opening and Motor Function Measure in Patients With Spinal Muscular Atrophy Type II (n = 6)
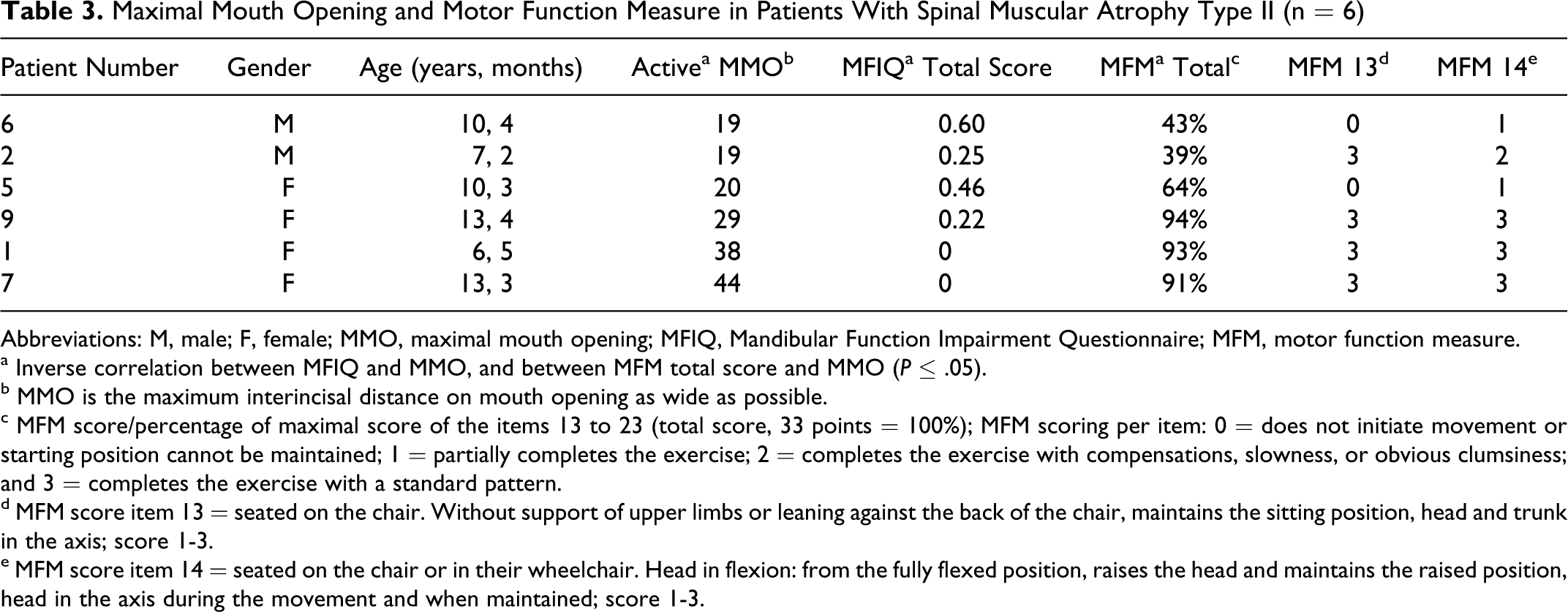
Abbreviations: M, male; F, female; MMO, maximal mouth opening; MFIQ, Mandibular Function Impairment Questionnaire; MFM, motor function measure.
a Inverse correlation between MFIQ and MMO, and between MFM total score and MMO (P ≤ .05).
b MMO is the maximum interincisal distance on mouth opening as wide as possible.
c MFM score/percentage of maximal score of the items 13 to 23 (total score, 33 points = 100%); MFM scoring per item: 0 = does not initiate movement or starting position cannot be maintained; 1 = partially completes the exercise; 2 = completes the exercise with compensations, slowness, or obvious clumsiness; and 3 = completes the exercise with a standard pattern.
d MFM score item 13 = seated on the chair. Without support of upper limbs or leaning against the back of the chair, maintains the sitting position, head and trunk in the axis; score 1-3.
e MFM score item 14 = seated on the chair or in their wheelchair. Head in flexion: from the fully flexed position, raises the head and maintains the raised position, head in the axis during the movement and when maintained; score 1-3.
Examination of the Masticatory System
Ranges of motion during active mandibular movements and passive openings were significantly less in the patient group than in the control group (Table 4).
Group Comparison and Descriptive Statistics of the Mandibular Range of Motion of the Mandible During Clinical Examination in the Patient Group (n = 12) and in the Control Group (n = 12)
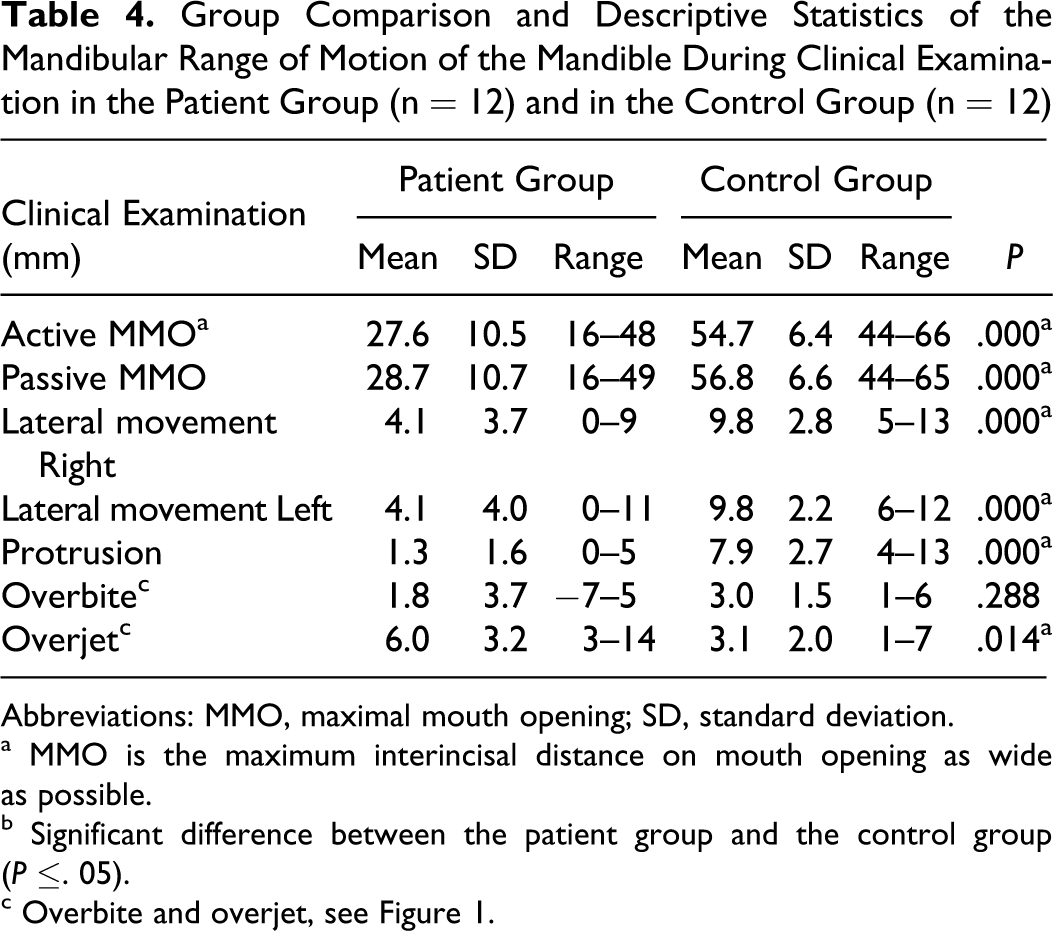
Abbreviations: MMO, maximal mouth opening; SD, standard deviation.
a MMO is the maximum interincisal distance on mouth opening as wide as possible.
b Significant difference between the patient group and the control group (P ≤. 05).
c Overbite and overjet, see Figure 1.
In patients with a severe reduced mandibular range of motion (≤30 mm), active and passive mouth opening were equally wide. The temporomandibular joints mainly rotated in the mouth opening, instead of the usual combination of rotation and sliding of the mandibular condyle. Pain could be provoked in 2 out of 12 patients during traction and translation, compression, and resistance tests. Pain was reported in the masseter muscle region in 8 out of 12 patients during assisted maximal mouth opening. In the control group, none of the patients reported pain during clinical examination. The severity of the limited active mouth opening correlated with the severity of the disease assessed by the motor function measure total scores (Table 3, P ≤ .05).
Discussion
The aim of our study was to systematically investigate mandibular function by using questionnaires and detailed clinical examination in young patients with spinal muscular atrophy type II. We found a striking difference in the mandibular range of motion between the patient group and control group, both statistically significant and clinically relevant.
Four out of 9 children with a severe limitation of active maximal mouth opening (≤30 mm) scored a low function impairment on the Mandibular Function Impairment Questionnaire (Table 2), which indicates a discrepancy between these limitations and the awareness of the patients and parents. This lack of awareness may result in limitations of mandibular function that are more extensive than if they were observed earlier. In the 9 patients with a severe reduced range of motion (≤30 mm), the stiff end feel in assisted mouth opening and mainly rotation of the mandibular condyles in the mouth opening indicates changes in the morphology of the temporomandibular joints. These changes might be initiated by inadequate movement of the lower jaw caused by the progressive weakening of the chewing muscles and the neck muscles leading to contracture of the temporomandibular joints. Some of our patients had a limited mouth opening at a very young age, ie, 7 years. It is therefore important to investigate whether early physiotherapy, starting when mandibular movements are still within the normal range, might be more efficacious than late intervention. This requires early recognition of the reduced mouth opening. Physicians may not be aware of mandibular dysfunction as a complication of spinal muscular atrophy, despite the fact that it may reduce the quality of chewing of solid food and compromise swallowing. A recent study showed that swallowing of solid food by patients with spinal muscular atrophy type II resulted in more postswallow residue, especially in the vallecula and above the upper esophageal sphincter than with liquid. 23 Hampered chewing because of malocclusion, reduced bite force, and fatigue caused by the involvement of the chewing muscles (cranial nerve V3, VII, IX, and XII), results in a hampered food comminution, inadequate food bolus formation, and oral transport. Thus, the already impaired swallowing process may be further hampered by the compromised chewing capability. Impaired chewing may be a clinically relevant impairment in children with spinal muscular atrophy type II. Moreover, the limited mandibular range of motion has an impact on oral hygiene and dental care.
Weakness of neck muscles may further contribute to impaired mandibular function. Head retraction by the neck muscle in an attempt to stabilize the balance of the head may increase reduction of the opening capacity of the mouth. 23 This is supported by the finding that motor function measure scores, which reflect motor disability in patients with neuromuscular disorders, were associated with mandibular dysfunction (Table 3, P ≤ .05). 20
Limitations of mouth opening can be easily accessed by means of a ruler. Interincisal distances (including the overbite; Figure 1) of less than 35 mm in children younger than the age of 12 years, and less than 40 mm in children older than 12 years, suggest limited mouth opening and warrants referral to a specialized dental team.
More research is needed to further assess the causative factors of reduced mandibular function and to establish the additional value of early physiotherapeutic intervention.
Conclusion
This study shows that mandibular dysfunction is common among young patients with spinal muscular atrophy type II. This reduces the quality of chewing and swallowing. Early recognition of mandibular dysfunction may help to prevent complications such as aspiration as a result of chewing problems.
Footnotes
Acknowledgments
The study was carried out at the Department of Rehabilitation, Children’s Hospital, Radboud University Nijmegen Medical Centre; the Division of Surgical Sciences, Department of Oral-Maxillofacial Surgery, Prosthodontics, and Special Dental Care, Temporomandibular Disorders, and Orofacial Pain Unit, University Medical Centre Utrecht; and the multidisciplinary outpatient clinic of the Children’s Hospital, University Medical Centre Utrecht, the Netherlands.
We thank the participating parents and children, whose cooperation made this study possible. We also thank C. F. van den Brink and R. H. Dirks for carrying out the pilot study.
All authors contributed substantially to the design of the study, drafting the article, and revising it, and gave final approval of the version to be published.
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
The study was approved by the Committee on Research Involving Human Subjects of Arnhem, Nijmegen, and Utrecht, the Netherlands, and written informed consent of the parents and children was obtained.