
Abstract
It is rare for both limb ischemia and arterial ischemic stroke to occur in the same child during the perinatal period. Two children who appear to have had perinatal emboli to both an arm and a middle cerebral artery territory are presented here. One child required amputation of the ischemic limb below the shoulder, and the other required skin grafts to the distal ischemic fingers. Each of these children later received cerebral magnetic resonance imaging for evaluation of developmental delay and was found to have what appeared to be old perinatal arterial ischemic stroke. Both children were homozygous for the methylenetetrahydrofolate reductase C677T gene variant. Eight other children with perinatal limb ischemia and stroke were found on literature review; several also had delayed diagnosis of perinatal stroke. This report examines the approach to diagnosis and treatment in each of these and makes suggestions for the similar cases in the future.
Perinatal ischemic events are rare. Perinatal limb ischemia occurs in approximately 1 in 4500 births per year, 1 whereas perinatal arterial ischemic stroke occurs in approximately 1 in 4000 full-term infants per year. 2 The occurrence of both perinatal limb ischemia and perinatal stroke in the same child is an even rarer event. This article presents 2 children who appear to have had both perinatal limb ischemia and perinatal stroke and reviews the diagnosis, possible contributing causes, treatment, and outcome of this phenomenon in these and previously reported cases.
Case Reports
Case 1
A 6.1-lb boy was born full-term via a scheduled repeat cesarean section after a pregnancy complicated by preeclampsia 1 week before delivery. Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. The placenta was not described. At birth, the neonate’s right arm was described as “gray and cool” below the elbow, with decreased movement below the elbow. The physical examination was otherwise unremarkable. He received ampicillin and gentamicin for the first 10 days of life. These were discontinued on day 10 after blood cultures were found to be negative. Coagulation studies suggested disseminated intravascular coagulopathy (prothrombin time, 15.9 seconds; normal, 11.3-13.2 seconds; activated partial thromboplastin time, 49.3seconds; normal, 24.7-33.4 seconds), and he was given oral vitamin K for 3 days. Tests for protein C and S activity, fibrinogen, homocysteine, and prothrombin G20210A and factor V Leiden gene mutations were unremarkable. His neurologic examination was normal at discharge at 2 weeks of life. Family history was positive for a maternal grandmother who took warfarin for several deep vein thromboses and a maternal great uncle who took warfarin for a pulmonary embolism at the age of 55 years.
From 2 weeks to 2 months of age, the infant underwent multiple operations and received a multistage amputation of the right arm below the shoulder. At 3 months of age, a physical therapist noticed he had decreased right kick. His parents became concerned when he was 1 year old because he was not crawling or pulling to stand. Since that time, he has continued to have intact cranial nerves; full strength, and range of motion in his left arm and leg; increased tone in his right leg; normal sensation; a slightly spastic gait; and slightly hyperactive reflexes in his right leg.
At 2 years of age, the patient received cranial magnetic resonance imaging for evaluation of delayed speech and walking. This revealed remote left middle cerebral artery infarction assumed to have occurred during the perinatal period (Figure 1 ). The right arm would have been the limb most affected by the stroke, but it had been amputated because of perinatal limb ischemia.
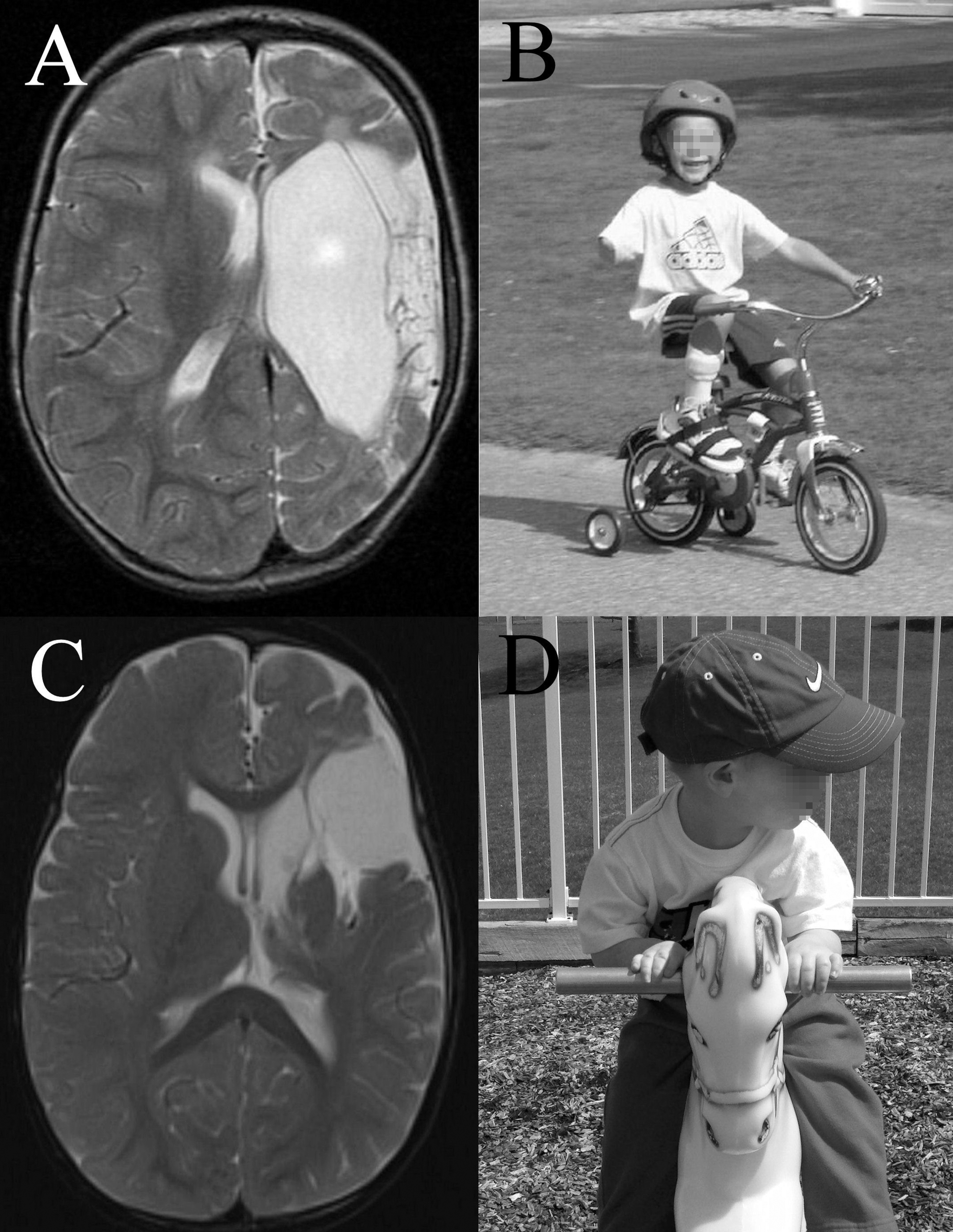
Cranial magnetic resonance imaging (MRI) and photo of cases 1 and 2. A, T2-weighted brain MRI of case 1 at 2 years of age showing remote infarction in the distribution of the left middle cerebral artery. B, case 1 riding a bicycle at 4.5 years of age. Note amputated right arm. C, T2-weighted brain MRI of case 2 at 1 year of age showing remote infarction in the distribution of the left middle cerebral artery. D, case 2 playing on the playground at 2 years of age.
The child received further investigation for stroke risk factors. Both the child and his mother were found to be homozygous for the methylenetetrahydrofolate reductase C677T gene variant, and both began taking a folate supplement. He was also found to be homozygous for the plasminogen activator inhibitor-1 4G gene variant. He had decreased high-density lipoprotein on lipid panel (28 mg/dL; normal, >40 mg/dL). Echocardiography and evaluations for activated protein C resistance, lupus anticoagulant, antiphospholipid antibody, and levels of protein C, protein S, antithrombin III, factor VIIIC, lipoprotein (a), and homocysteine were unremarkable.
At birth, the child weighed 6.1 lb (10th percentile), was 18.5 in long (13th percentile), and had a head circumference of 12.2 in (below the 3rd percentile). At the latest follow-up at 8 1/2 years of age, he weighed 47 lb (4th percentile), was 50 in tall (15th percentile) and had a head circumference of 19.6 in (4th percentile).
The child has received speech, occupational, and physical therapies. He was eventually diagnosed with attention-deficit hyperactivity disorder. At 4 years of age, he began having seizures; electroencephalography revealed multifocal sharp discharges over the left hemisphere. He was tried on oxcarbazepine but suffered fatigue and was switched to lamotrigine. He repeated kindergarten because of hyperactivity and inattention. Now at age 8 1/2 years, he attends a regular school. He wears a right leg brace but is active in sports.
Case 2
A 5.3-lb boy was born at 35 weeks' gestation via induced vaginal delivery due to fetal cardiac dysrhythmia. Apgar scores were 2, 6, and 7 at 1, 5, and 10 minutes, respectively. Examination of the placenta was not noted. The neonate had sloughing of skin, edema, and blistering of both forearms at birth, which was worse on the right. On neurologic examination, he was noted to have asymmetric motor activity, hypotonia, and a diminished Moro reflex. He was sent to the neonatal intensive care unit for respiratory distress syndrome.
He was initially treated with ampicillin and gentamicin for possible sepsis, but these were discontinued when blood cultures were negative. Radiographs of his upper extremities were normal. A complete blood count and newborn screen were unremarkable. Family history was negative for thromboembolic disease. His right arm was treated with daily dressing changes. When he was discharged at 4 days of life, he was noted to have full range of motion of his extremities. The patient underwent a skin graft to his right forearm at 4 months of age.
At 12 months of age, the child was evaluated for speech and motor delay. His parents noted that he had decreased right arm movement since birth, which had been thought to be due to his arm ischemia. His physical therapist noted that he had truncal hypotonia and right hemiparesis with increased tone in the right arm and both legs. Electromyography revealed old medial and ulnar neuropathies in the right arm. Magnetic resonance imaging of the cervical spine and right shoulder were normal. Magnetic resonance imaging of the right forearm showed decreased muscle mass. Magnetic resonance imaging of the head showed remote infarction in the distribution of the left middle cerebral artery and right periventricular gliosis (Figure 1). This was assumed to have occurred during the perinatal period. Since this time, he continued to have intact cranial nerves, increased tone in both arms and legs (right greater than left), normal sensation, and hyperactive reflexes in his right arm and leg. He is able to move all 4 extremities. He favors his left side and reaches for objects with his right hand only when the left is constrained.
On further evaluation, an echocardiogram was normal, but electrocardiogram and Holter monitoring showed occasional premature atrial contractions. The cardiologist believed that these were not concerning and were unrelated to emboli. Electroencephalography demonstrated left fronto-polar spike-and-slow wave complexes; he was started on oxcarbazepine. He was homozygous for the methylenetetrahydrofolate C677T gene variant and began folic acid supplements. Lipid panels at 16 and 23 months of age found elevated low density lipoprotein (LDL) cholesterol (107 and 155 mg/dL, respectively; normal, 0-100 mg/dL) and elevated lipoprotein (a) (40 and 52 mg/dL, respectively; normal, <30 mg/dL). Evaluations for prothrombin G20210A, factor V Leiden mutation, plasminogen activator inhibitor–1 gene variant, and levels of protein C, protein S, and antithrombin III were unremarkable. The parents were counseled about dietary changes, and the mother was referred to her obstetrician to discuss evaluation for thrombophilia and other pregnancy risk factors. The child also underwent physical, occupational, and speech therapies.
At birth, the child weighed 5.3 lb (3rd percentile), was 19 in long (25th percentile), and had a head circumference of 12.25 in (less than 3rd percentile). At the latest follow-up at 2 years old, he weighed 25.8 lb (19th percentile), he was 33 in tall (9th percentile), and his head circumference was 18.7 in (17th percentile).
At 25 months of age, the patient continued to have speech delay and communicated mostly through sign language and 1-word phrases; however, he was able to follow complex commands. He could not crawl and walked only with a reverse walker. He has good seizure control on oxcarbazepine.
Discussion
A review of the literature revealed reports of 8 other children who appeared to have had emboli to both an extremity and the brain during the perinatal period 3–9 (Table 1 ). Each of these children presented with limb ischemia within 10 minutes of birth but was not diagnosed with stroke until 1 day to 7 months later. There were similarities in the presentation of limb ischemia in these cases, but imaging evaluations, risk factor evaluations, treatments, and outcomes varied widely. Most of these cases had risk factors that may have contributed to both limb ischemia and perinatal stroke. The 2 new cases described here have some similarities to previously presented cases.
Clinical Features of Previously and Currently Reported Cases
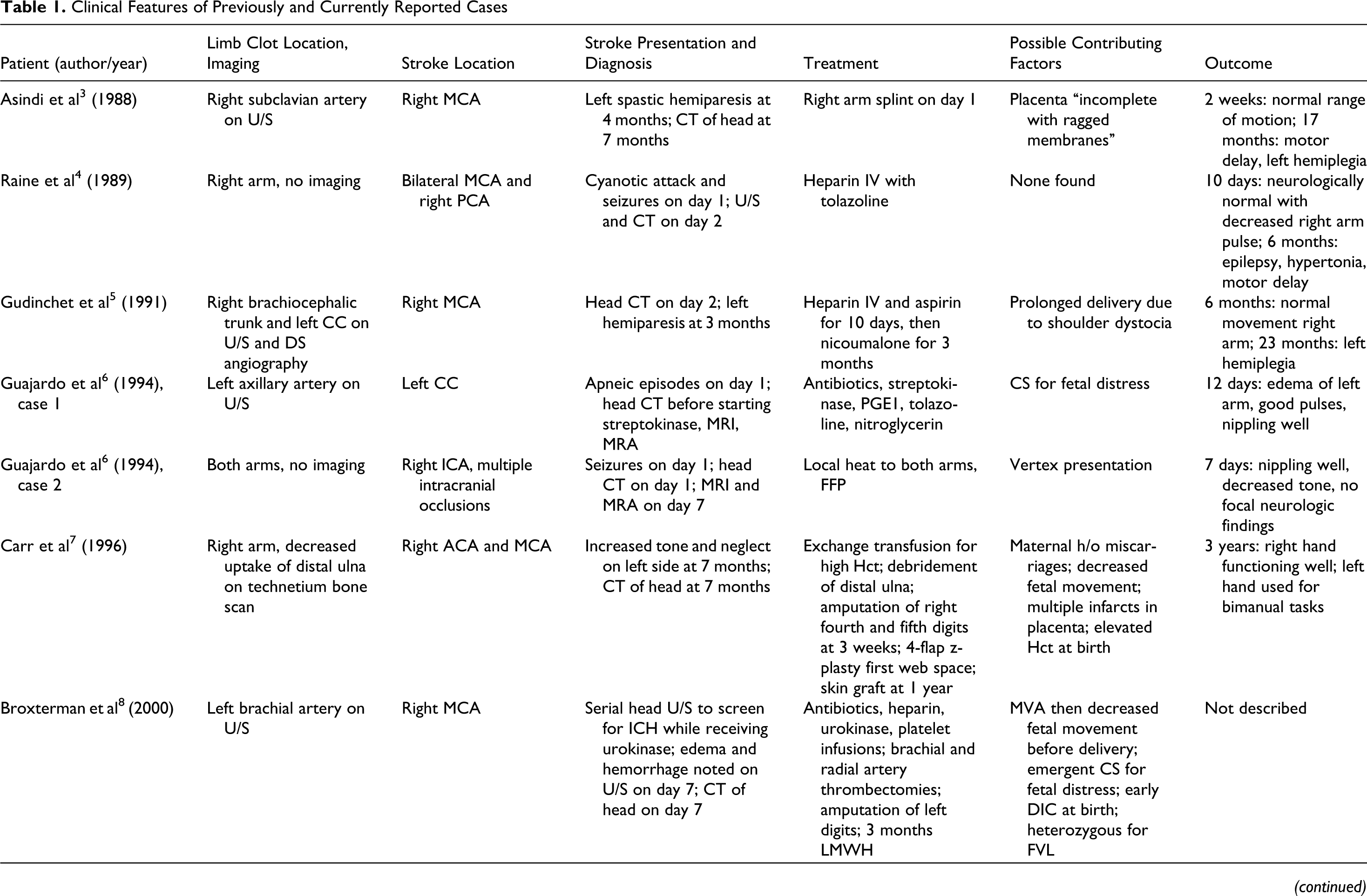
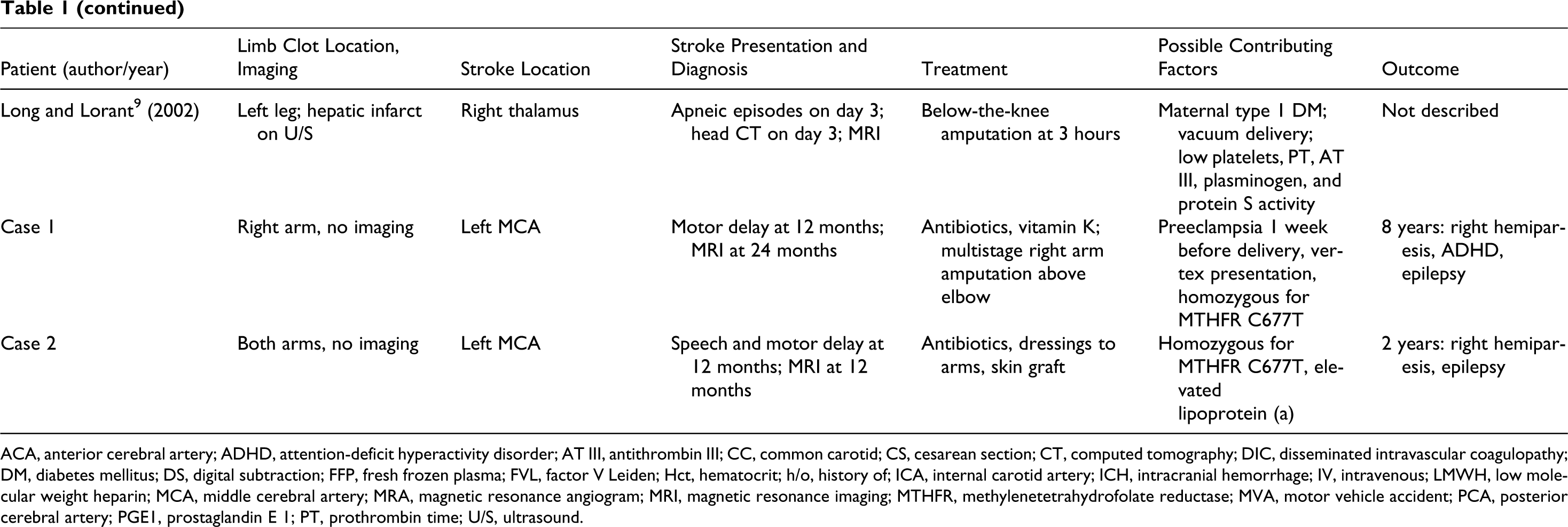
ACA, anterior cerebral artery; ADHD, attention-deficit hyperactivity disorder; AT III, antithrombin III; CC, common carotid; CS, cesarean section; CT, computed tomography; DIC, disseminated intravascular coagulopathy; DM, diabetes mellitus; DS, digital subtraction; FFP, fresh frozen plasma; FVL, factor V Leiden; Hct, hematocrit; h/o, history of; ICA, internal carotid artery; ICH, intracranial hemorrhage; IV, intravenous; LMWH, low molecular weight heparin; MCA, middle cerebral artery; MRA, magnetic resonance angiogram; MRI, magnetic resonance imaging; MTHFR, methylenetetrahydrofolate reductase; MVA, motor vehicle accident; PCA, posterior cerebral artery; PGE1, prostaglandin E 1; PT, prothrombin time; U/S, ultrasound.
The appearance of limb ischemia progresses from pallor to mottled, then a line of demarcation forms, and finally gangrene develops. This pattern may aid in estimating the time of occlusion. 1 Most of the 8 previously described children had limb discoloration and absent pulses at birth. Two had malformation and decreased muscle mass in the affected ischemic limbs, suggesting the occlusion took place in utero. 3,9 Both of the 2 newly presented cases also had abnormal limb appearance at birth.
Diagnosis of stroke was made after the diagnosis of limb ischemia in all children with both, probably because perinatal stroke can have subtle presentations during the perinatal period. Seizure is the most common presenting sign of perinatal stroke, 10 but neonates may also present with lethargy, hypotonia, or apnea. 2 Some children with perinatal stroke appear normal as neonates but later develop asymmetric use of extremities, seizures, or developmental delay. 2,11 Several of the children with both perinatal limb and brain ischemia had perinatal seizures 4,6 or apneic episodes, 6,9 but several had no clear perinatal signs of stroke. 5,7,8 Several were first diagnosed when screening cranial imaging was performed before starting thrombolytics for limb ischemia 6,8 or to further evaluate carotid occlusions seen on color Doppler sonography. 5
Cerebral ischemia was not always ipsilateral to limb ischemia; some children had stroke contralateral to limb ischemia, 8,9 bilateral infarcts, 4,6 and/or bilateral limb ischemia. 6 Only 1 child had an ischemic leg 9 ; this was also the only child with organ involvement (liver ischemia and adrenal hemorrhage). However, most children were not screened with abdominal imaging.
Color duplex ultrasound is the recommended imaging test for identifying occluded vessels in ischemic limbs, 1 and 5 of the cases were evaluated with ultrasound. 3,5,6,8,9 Radiographs were performed in 5 cases, 3,4,6,7 including case 2, and were all normal, suggesting that radiography may not contribute much to these evaluations.
Emboli may originate from an intracranial vessel, the heart, or the placenta and may travel through the foramen ovale or ductus arteriosus into the arterial system. 1,2 In most of the 10 cases reviewed, it was not clear where emboli originated. Placentas were examined in only 4 cases; 2 were normal, 4,8 and 2 were believed to be possible sources of emboli. 3,7
Almost all of the previously and currently described cases had at least 1 possible risk factor identified. The 1 exception was from 1989, when less was known about perinatal thromboembolism, and fewer tests for thrombophilia were available. 4 Possible risk factors that have been associated with perinatal thromboembolism and were identified in the previously and currently reported cases include gestational hypertension and/or diabetes in the mother, 9 vertex presentation, 6 vacuum assistance, 9 emergency cesarean section, 6,8 intolerance of labor, 6,8 decreased fetal movements, 7 shoulder dystocia, 5 prenatal motor trauma, 8 high perinatal hematocrit, 7 early disseminated intravascular coagulopathy, and other prothrombotic risk factors 8,9 (Table 1). 2,10-14 Both of the new cases presented in this article were homozygous for the methylenetetrahydrofolate reductase C677T variant; in addition, case 1 was homozygous for the plasminogen activator inhibitor–1 4G gene variant, and case 2 had elevated lipoprotein (a). Surprisingly, no cardiac abnormalities were found in the 5 children who received echocardiography. 6,8
Therapy in all 10 cases varied dramatically, in part due to medical developments since the earlier cases were reported. Five children received intravenous antibiotics for suspected sepsis. 6,8 Three children received conservative management of limb ischemia, such as splinting, local heat, and frequent dressing changes, and had spontaneous restoration of blood flow. 3,6 One child underwent thrombectomy, 8 and 4 children required debridement, skin grafting, and/or amputation. 7,9 Some physicians prefer conservative management of limb ischemia if the limb is viable, but thrombolytics may be considered. 1 Salvageability depends on time since occlusion, which is sometimes difficult to assess in prenatal clots. 1 Two of the 10 children did receive thrombolytics. One child received urokinase for the ischemic limb before stroke was diagnosed. He was screened with serial cranial ultrasounds, but cerebral edema was not noted until 7 days of life, suggesting the stroke may have occurred days after the limb ischemia. 8 The other child received streptokinase after stroke was discovered. 6 Three children received heparin, 4,5,8 and the child treated with thrombectomy received low molecular weight heparin for the following 3 months. 8
Optimal acute and long-term treatment for perinatal stroke remains undecided. 11 Few studies have been conducted in children. 2,14 Anticoagulation may be considered in neonates with stroke who have severe thrombophilia or multiple sites of thromboembolism. 11 Currently, thrombolytics are not recommended in the treatment of perinatal stroke. 11
It is difficult to correlate treatment with outcome in these cases because of small numbers, and variability in treatment, and length of follow-up. None of the 10 cases had reported recurrence of thromboembolism. Six children who had longer follow-up, including cases 1 and 2, developed some hemiparesis and motor delay. 3–5,7 Several children developed seizures. 4,6 Cases 1 (now 8 years old) and 2 (now 2 years old) both have hemiplegia and are being treated for epilepsy, which is well controlled on medication.
It is not clear why some children develop multiple emboli to multiple sites; there are not enough cases reported with complete workups to determine if these children have risk factors that place them at higher risk than other children with only limb ischemia or only perinatal ischemic stroke. Further work is needed to determine how best to detect and treat multiple perinatal emboli. The authors suggest that cranial imaging be considered in all children with perinatal limb ischemia regardless of neurologic status, especially in the setting of concomitant known risk factors for thromboembolism.
Footnotes
MJM reviewed the charts and literature and generated all drafts of the paper as part of a pediatric neurology clinical research elective. MRG provided the cases, mentored the first author through research and writing, and provided feedback and editing on each draft.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: The senior author received support from the Department of Neurology at the Indiana University School of Medicine.
This study was approved by the Indiana University Institutional Review Board (study 0207-55).