
Abstract
This study was done to determine if urine phenobarbital measurements provide a reliable indicator of presence of the drug in neonates. Urine was collected from neonates treated with phenobarbital for clinical indications within 4 to 6 hours of clinically indicated collection of serum phenobarbital levels. Urine samples were also collected from control neonates not treated with phenobarbital. One aliquot was assayed fresh, another frozen at -30°C and assayed 1 to 3 months later. Phenobarbital was assayed using the ONLINE TDM Roche/Hitachi automated clinical chemistry analyzer. Serum and urine concentrations were compared as were fresh and frozen urine measurements. Serum phenobarbital ranged from 5.6 to 52.7 μg/mL. Matched urine samples were 56.6 ± 12.5% of the serum level. Frozen samples were 98.3 ± 8.0% of the fresh samples. Urine phenobarbital concentrations, either fresh or frozen, can be used in neonates as a noninvasive estimate of drug levels.
Continuation of antiepileptic treatment after hospital discharge in neonates whose seizures resolve within 3 to 7 days of onset is highly variable. 1 Some physicians discharge most or all infants on no medications if they are seizure-free at the time of discharge; others discharge most or all infants on antiepileptic drugs usually phenobarbital, for 3 to 9 months, regardless of the presence or absence of seizures at the time of discharge. This decision is based on limited data from retrospective reviews, cohort studies of patients with neonatal seizures followed prospectively for outcome, with or without a standardized approach to outpatient care, and animal studies on the effect of chronic phenobarbital exposure on brain growth.
A multicenter randomized, placebo-controlled trial is underway to assess the benefits and risks of continued phenobarbital treatment after hospital discharge for prophylaxis of infants with neonatal seizures. For this study, 3 approaches will be used to determine compliance with study drug: (1) parents will be contacted monthly during the intervention period and asked if they have been administering study drug as instructed, (2) parents will be instructed to bring study drug bottles with them to each outpatient visit and the amount of study drug remaining in the bottle will be estimated, and (3) urine samples after 2 months and 4 months of participation will be collected for qualitative determination of phenobarbital presence or absence. Collection of urine is a less invasive means of determining the presence of drug than is collection of blood samples and, we believe, will be acceptable to families.
Before initiation of the clinical trial, we conducted a preliminary investigation to see if urine phenobarbital measurements, collected and stored under conditions similar to those in the proposed trial, would provide a reliable indicator of the presence of study drug. In addition, if urine screening proves reliable, providers can consider its use in the clinical context to monitor compliance with medication usage.
Methods
We conducted a single center observational study at a regional perinatal center. The study population consisted of infants at least 34 weeks’ gestation being treated with phenobarbital as part of their clinical care in the neonatal intensive care unit for whom serum phenobarbital levels were requested by the care team (“treated infants”). Control infants were at least 34 weeks’ gestation and not being treated with phenobarbital. These control samples were included to simulate patients not compliant with medication. The agreement of the treating physicians was obtained before approaching the families for informed consent. This study was approved by the University of Rochester Medical Center (URMC) Research Subjects Review Board.
Urine was collected within 4 to 6 hours of obtaining blood for serum phenobarbital levels ordered by the care team (in the case of treated infants) or within 4 to 6 hours of obtaining other routine blood tests (in the case of control infants). The urine sample was identified with a study number separate from the infant’s medical record number and sent to the URMC laboratory. Upon arrival in the laboratory, the specimen was aliquoted into 2 samples. One sample was assayed “fresh” and the other sample was frozen at −20°C and assayed 1 to 4 months later. The results of the urine testing were available only to study personnel and not to the care team as measurement of urine phenobarbital concentration is not standard of care.
Phenobarbital was assayed in urine using the ONLINE TDM Roche/Hitachi automated clinical chemistry analyzer, cobas. No modifications were made in the procedures for assay of phenobarbital in serum or plasma. For this assay, the measuring range is 2.4 to 60 μg/mL, the analytical sensitivity (lower detection limit) is 1.2 μg/mL, and the functional sensitivity is 2.4 μg/mL. There is no reported cross-reactivity with the following drugs commonly prescribed in the neonatal intensive care unit: caffeine, phenytoin, theophylline, and intralipid.
Additional clinical data were collected from the infants’ medical records including clinical diagnoses, urinary output and serum creatinine levels on the day the urine sample was obtained.
Linear regression (with zero intercept) was used to describe the relationship between phenobarbital concentrations in fresh urine samples and those in concomitant serum concentrations.
Results
Ten infants who were receiving phenobarbital and 4 control infants were recruited for this study. One to 4 urine samples were obtained from each treated infant for a total of 21 paired samples. Of the 10 treated infants, 9 were diagnosed with seizures (2 with intracranial hemorrhage; 4 with hypoxic-ischemic encephalopathy [HIE, 1 mild, 2 moderate, 1 severe]; 1 with HIE and a subdural hemorrhage; 1 with HIE and hydranencephaly; 1 with unknown etiology) and 1 was being treated with phenobarbital for sedation (congenital diaphragmatic hernia previously on ECMO). Samples were obtained at chronologic ages ranging from 1–20 days after birth. The 4 control infants did not have seizures and were not receiving any antiepileptic drugs or sedatives.
Serum phenobarbital concentrations in treated infants ranged from 5.6 to 52.7 μg/mL, with the majority of the levels 20 to 40 μg/mL. Matched urine samples were 56.6 ± 12.5% (mean ± standard deviation) of the serum levels. There was no detectable phenobarbital in any of the control infants’ urine. Individual data points are shown in Figure 1 with each paired sample displayed.
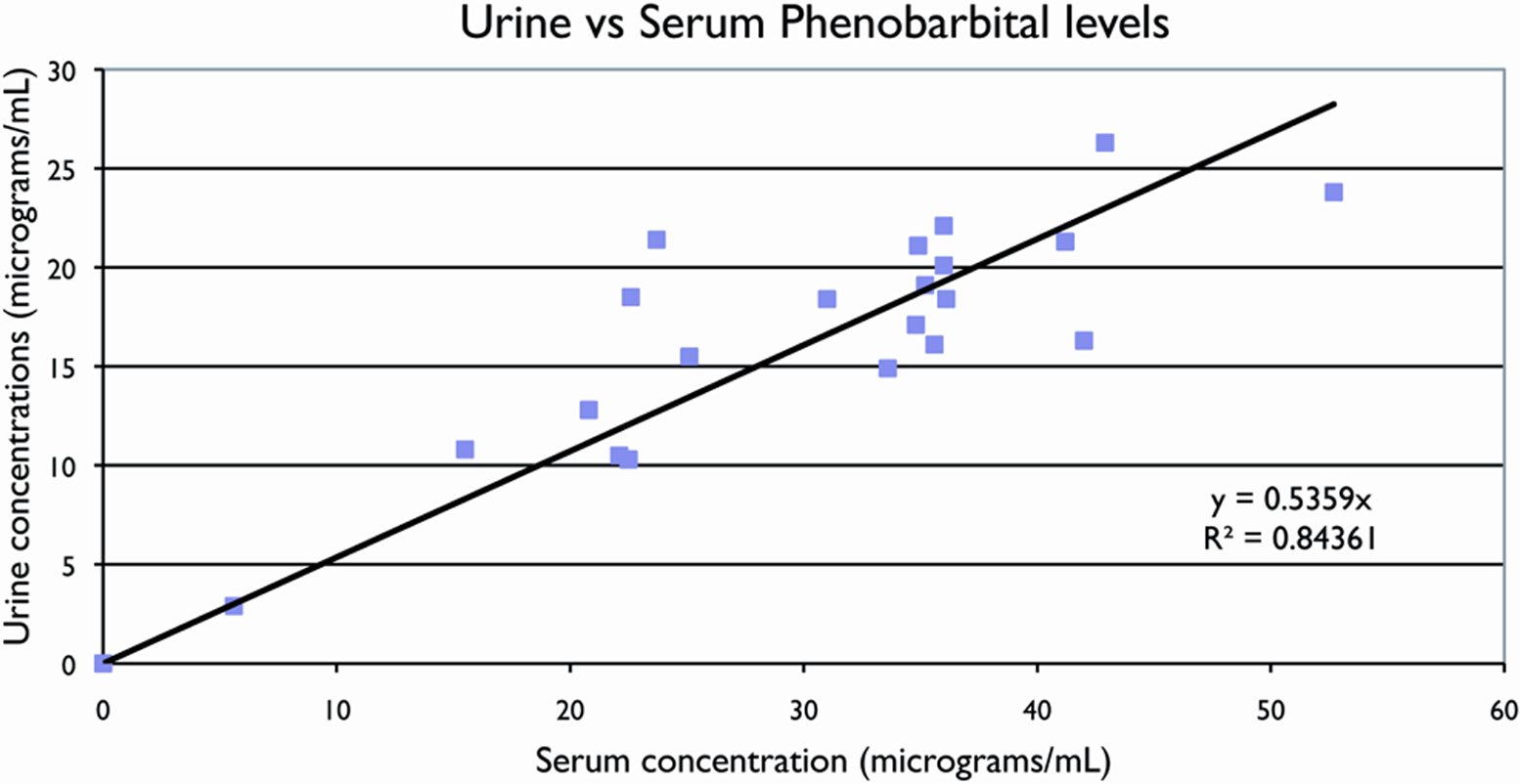
Urine versus serum phenobarbital levels. The relationship between serum and urine phenobarbital concentrations appears to be linear over a wide range of values. Depicted are 22 paired samples obtained from 10 infants treated with phenobarbital for clinical indications and 4 urine samples from infants not treated with phenobarbital (serum level assumed to be zero).
Serum creatinine levels and hourly urine output (indicators of renal dysfunction), when available, did not appear to explain the variance.
There was excellent agreement between the results of the urine specimens that were assayed upon receipt compared with those assayed after up to 3 months in the freezer. As shown in Figure 2 , with the exception of 1 sample, the values were nearly identical (98.3 ± 8.0%; 99.7 ± 5.6%, with and without the outlier, respectively).
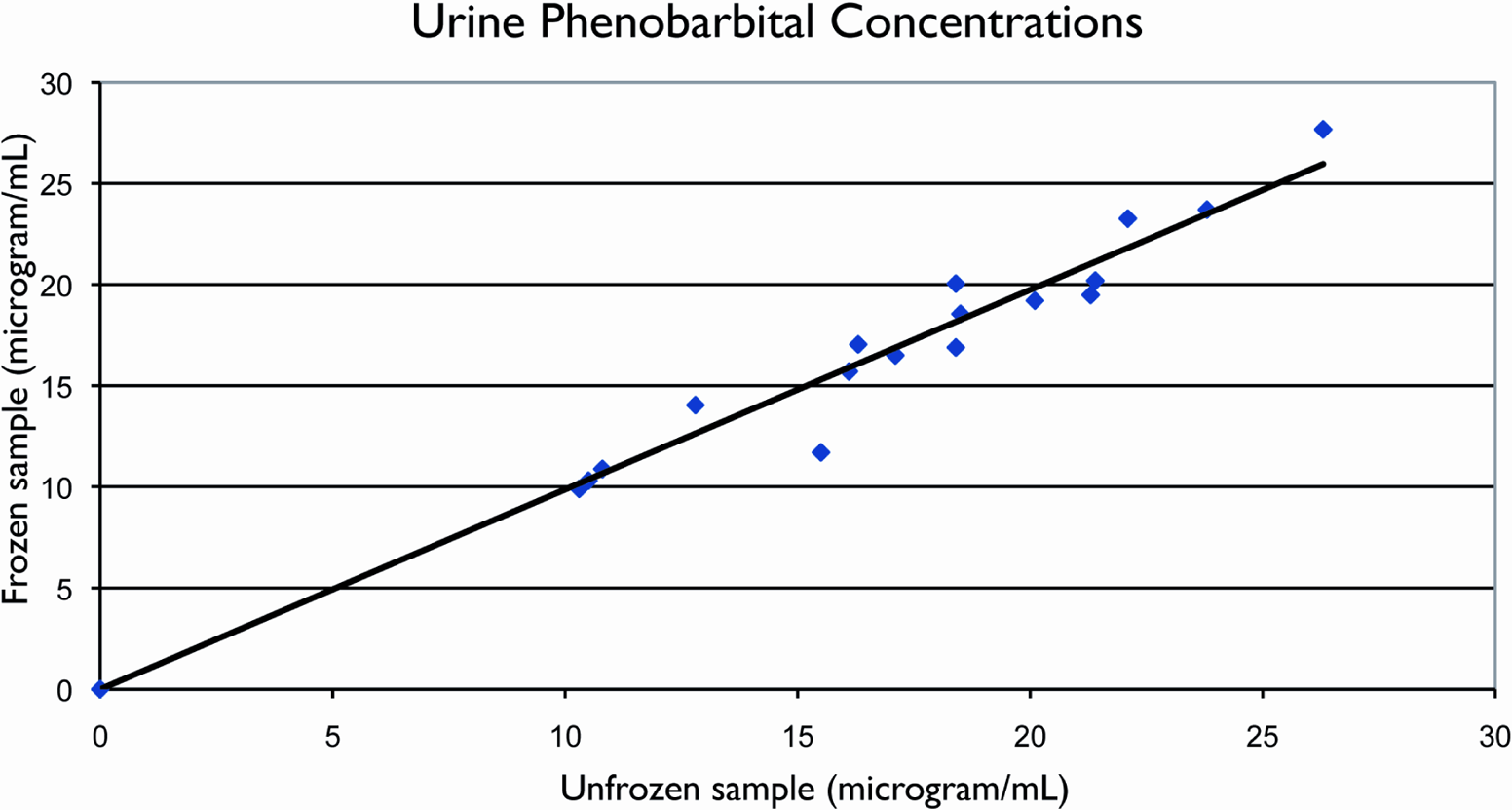
Urine phenobarbital levels in fresh versus frozen samples. The line depicted in the figure is the 45° line (line of agreement). There is excellent agreement between urine phenobarbital levels when measured soon after collection and when measured in aliquots that were frozen for up to 3 months.
Discussion
Phenobarbital is a commonly used antiepileptic drug, especially in the neonatal population. 1 To date, measurement of phenobarbital concentrations has been limited to serum, particularly in the acute clinical situation. However, both for longer term clinical monitoring and for monitoring of clinical trials using phenobarbital in 1 or more treatment arms, a less invasive means of assessing compliance can involve urinary assays. We demonstrated that measurement of urine phenobarbital concentrations, using the same method as with plasma or serum, in either fresh or frozen samples can be used in neonates for screening purposes.
Urine testing has been used in many different clinical scenarios. Chemical dependency screening is frequently performed using urine samples from individuals suspected of using illicit drugs. 2 MacDaniel et al 3 compared urine and serum testing for detection of acetaminophen overdose. In addition, urine samples can be collected to assess exposure to environmental agents such as tobacco smoke. 4 Couto et al 5 reported use of an algorithm applied to urine drug screening to assess compliance with an oxycontin regimen.
In infants, the ability to measure drug levels in urine, especially to assess compliance with experimental regimens, is particularly attractive. Large volumes of urine can be obtained, whereas the cumulative amount of blood that can be drawn without increased risk is limited to 3 mL/kg by most research subject review boards. Moreover, 1 of the factors many families take into consideration when approached for consent for a clinical trial involving their infant is the number and extent of invasive procedures. Frequent blood draws are often a disincentive to enrollment in clinical trials.
Although measurement of phenobarbital in the urine can be a relatively simple procedure, the results can be influenced by the infant’s renal function at the time of treatment. As many as 40%–60% of infants with seizures can have suffered hypoxic-ischemic encephalopathy. 6 Concomitant with brain injury, these infants can also have experienced compromised renal function (acute tubular necrosis) with decreased urine output. 7 Given the small number of infants in this “proof of concept” study, we were unable to assess the magnitude of any effect of perinatal asphyxia on the relationship between the serum and urine concentrations of phenobarbital. Thus, in the acute situation, the relationship between serum and urine concentrations cannot be as strong as it can be in more stable situations such as maintenance dosing or in the context of longer term use in a clinical trial.
Urinary measurement of phenobarbital either within a clinical trial or in a clinical context provides the researcher or clinician with a noninvasive screening tool for assessment of compliance. The strong association between blood and urine phenobarbital levels, the long half-life of phenobarbital, and the relatively wide therapeutic range combine to make urinary assessments a very attractive option. Given the long half-life of phenobarbital in the neonate, even serum determinations will not provide absolute confirmation of compliance with all recommended doses. Urine values obtained cannot be appropriate for adjustments in dosing, but may be used to determine if the infant’s phenobarbital levels are within the expected range—from which inferences can be made as to whether the infant is receiving the medication on a regular basis. Additional studies are warranted to more precisely determine the relationship between serum and urine phenobarbital levels and to determine if this relationship holds for older infants and children and in children with differing renal function.
Footnotes
RG: principal investigator responsible for the design and implementation of the study, oversight of data analysis, manuscript preparation. JMK: coinvestigator responsible for input on study design, data analysis and review of manuscript. SXC: summer research student responsible for data collection, preliminary data analysis, manuscript review. MPM: biostatistician responsible for final data analysis and manuscript review.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded in part by R34 HD050102 (R. Guillet PI). S. Chen was supported by the Strong Children’s Research Center Summer Student Program, 2010.
This study was approved by the Institutional Review Board of the University of Rochester Medical Center