
Abstract
Chiari malformation type 2 is characterized by hindbrain protrusion and a constellation of supratentorial malformations. Chiari malformation type 2 is thought to be causally related to myelomeningocele due to intrauterine cerebrospinal fluid overdrainage. This relationship is so strong that it has become a rule. A 14-year-old girl affected by mental retardation, spastic triparesis, and epilepsy is presented. Brain magnetic resonance imaging disclosed a severe Chiari malformation type 2, whereas spine magnetic resonance imaging was unremarkable. The authors discuss previous literature describing rare cases of Chiari malformation type 2 without open spinal dysraphism and the relevance of concomitant, sometimes overlooked, neuroimaging findings, underlying how exceptions might be hurdles but might also eventually strengthen the rules.
Chiari malformation type 2 is a complex congenital anomaly of the hindbrain characterized by protrusion of the cerebellar vermis, medulla, and fourth ventricle through the foramen magnum into the upper cervical spinal canal, variably associated with a wide constellation of supratentorial abnormalities. 1 –4 Chiari malformation type 2 has almost always been related to spinal dysraphism. 1,2 This relationship is very close and has led to the syllogism “If Chiari II, then myelomeningocele; if myelomeningocele, then Chiari II.” 1
We present a case of Chiari malformation type 2, occurring without any concomitant spinal dysraphism, that challenges the pathogenic hypotheses proposed to explain the spectrum of brain abnormalities associated with Chiari malformation type 2.
Case Report
A 14-year-old girl affected with left partial seizures, severe mental retardation, and paraparesis with left hemiparesis underwent brain magnetic resonance examination in our center. She was born at 36 weeks of gestational age and presented with macrocephaly (>97th percentile); a ventricular-peritoneal shunt was placed at 1 month of age because of hydrocephalus secondary to marked cerebral aqueduct stenosis. Her mother had a history of a previous miscarriage for fetal anencephaly. Genetic tests, including high-resolution karyotyping (550 bands) and array-comparative genomic hybridization (resolution 70 000 base pairs), were negative.
Brain magnetic resonance imaging showed a small posterior fossa with low-lying torcula and upward and downward hindbrain protrusion, corpus callosum agenesis, thalamic noncleavage, duplication of the cerebral falx and superior sagittal sinus, diffuse stenogyria of the parieto-occipital cortex, large areas of coarse polymicrogyria, periventricular heterotopias, marked atrophy of the chiasm, and abnormal shape of the third and lateral ventricles (Figure 1). The pituitary gland was small, and a persistent craniopharyngeal duct was noted. The latter finding was confirmed by a brain computed tomography that also revealed air along the duct to its intracranial tip, close to the neurohypophysis, seen on magnetic resonance imaging (Figure 2). Anterior pituitary hormones were normal. The hindbrain malformation and the constellation of the supratentorial abnormalities were consistent with Chiari malformation type 2; therefore, a total spine magnetic resonance imaging was performed, which excluded any form of spinal dysraphism.

Sagittal (a-c) and coronal (d) T1-weighted magnetic resonance images showing absence of corpus callosum, hindbrain downward (straight arrow) and upward herniation (curved arrow), coarse polymicrogyria (), subependymal heterotopias (⋆), low insertion of cerebellar tentorium (*), stenogyria (§), falx cerebri, and sagittal superior sinus duplication (å). All these findings feature a Chiari malformation type 2.
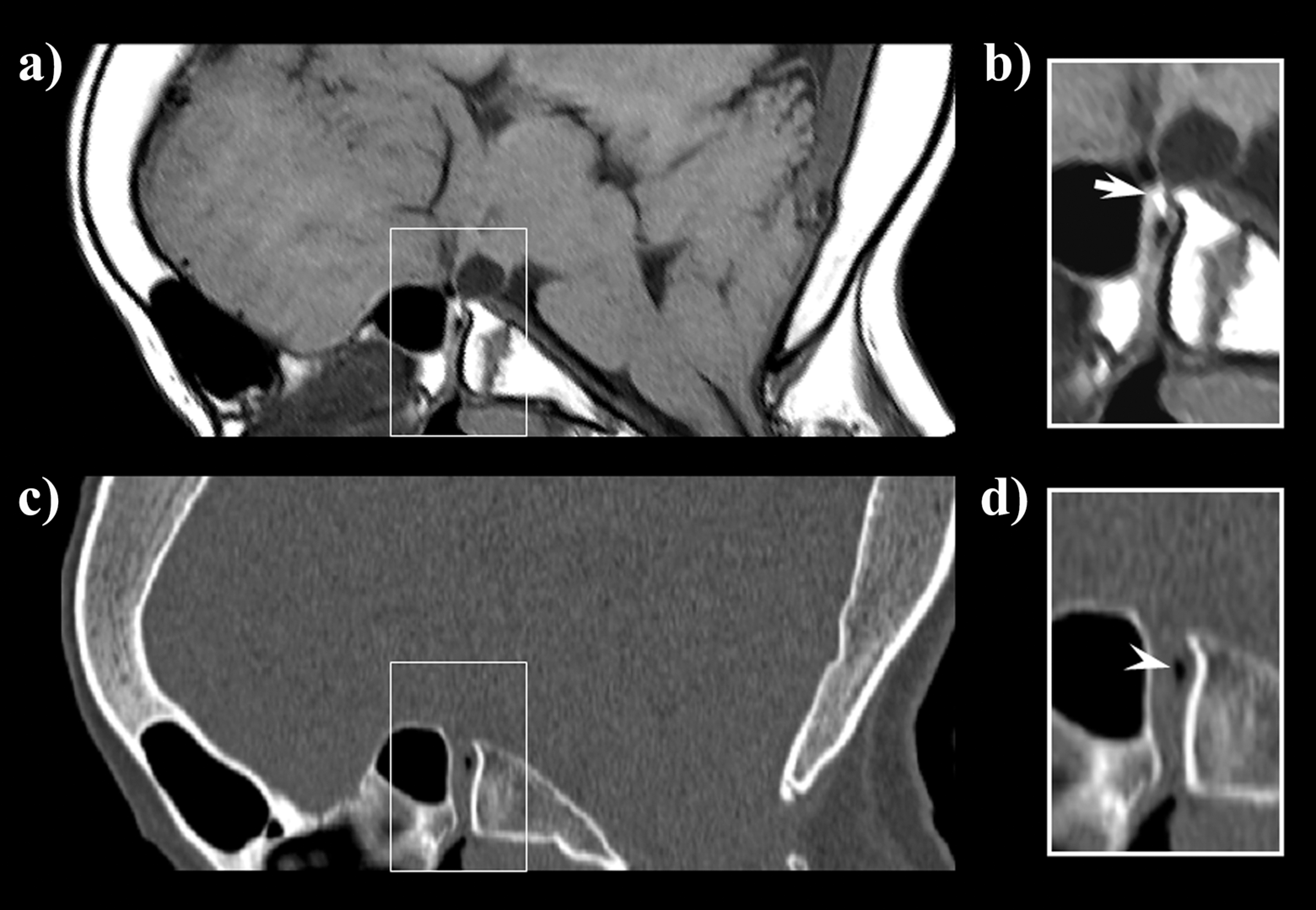
Midsagittal magnetic resonance (a, b) and computed tomography (c, d) scans revealing the presence of patent craniopharyngeal duct with air bubble (arrowhead) close to the neurohypophysis (arrow).
Patency of the craniopharyngeal duct was confirmed by endoscopic inspection (Figure 3), and surgical closure was performed.
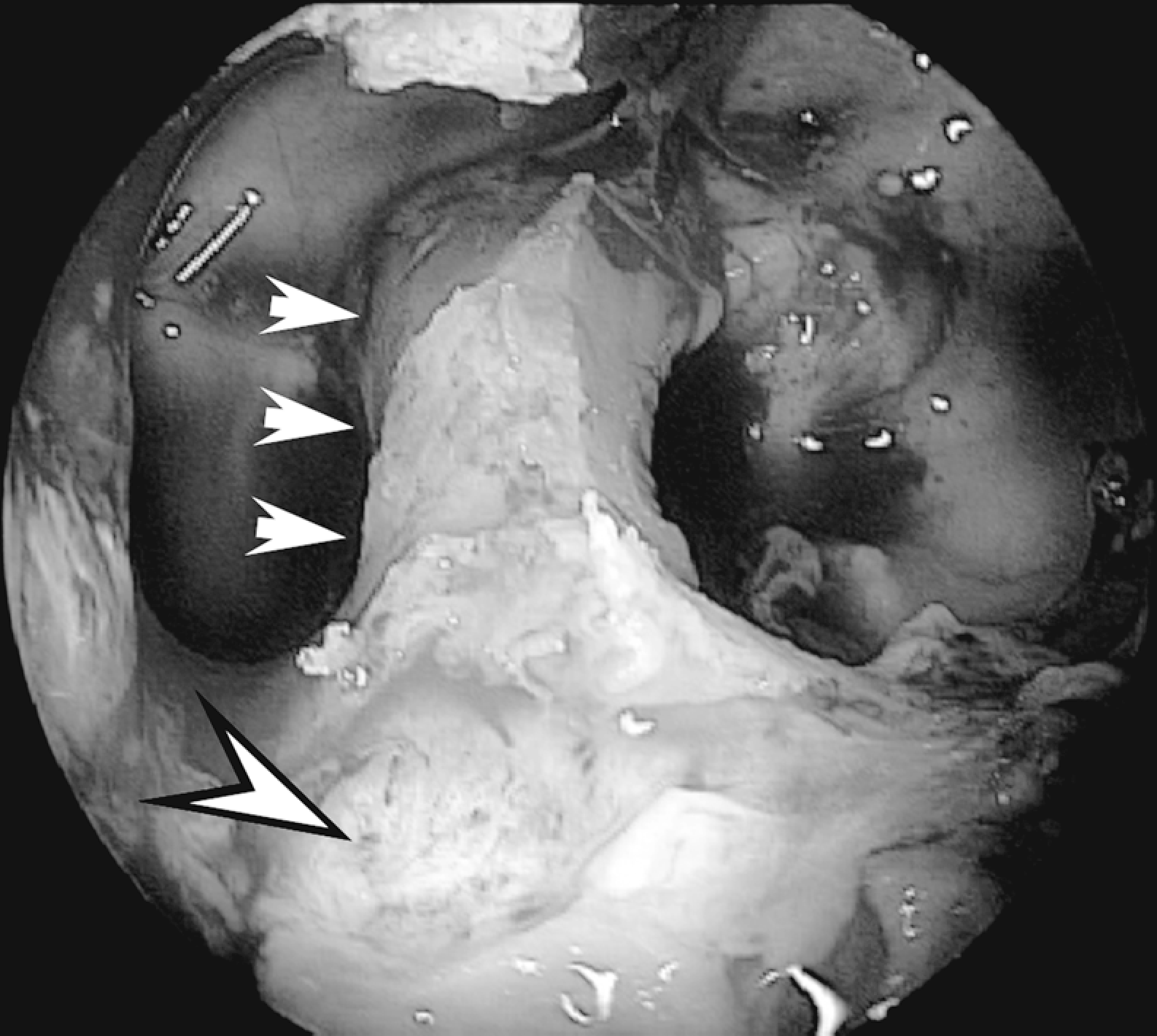
Endoscopic vision with 0° optic showing the craniopharyngeal duct and the inferior opening (arrowhead) after removal of the intersphenoid septum.
Discussion
Chiari malformation type 2 is a complex hindbrain malformation, variably associated with a rather large spectrum of supratentorial anomalies. 1 –4 The cause of Chiari malformation type 2 has been extensively debated and several hypotheses have been proposed to explain the almost constant association of Chiari malformation type 2 with spina bifida. 1,3,5
The most accepted theory, proposed by McLone and Knepper in 1989, 1,3,5 is based on this very close relationship. According to this theory, a faulty neural tube and spine closure allow cerebral spinal fluid to drain through the central canal, thus hindering the physiological brain ventricle distension. The latter seems to be required for a normal neuronal migration process, and its failure would account for most of the supratentorial abnormalities (eg, stenogyria, polymicrogyria, periventricular heterotopias, corpus callosum dysgenesia) associated with Chiari malformation type 2. Concurrently, cerebral spinal fluid hypotension would impair calvarian development determining a small posterior fossa. The subsequent hindbrain development in an underdeveloped posterior fossa resolves in downward (and sometimes also upward) displacement of cerebellar structures, the main feature of Chiari malformation type 2. Recently, it has been shown that defective or ectopic expression of homeotic genes might have a pathogenic role in hindbrain and spinal cord dysgenesis, thus relegating cerebral spinal fluid hypotension to a secondary potentiating role. 6 However, a pivotal pathogenic role of cerebral spinal fluid leakage has been demonstrated in experimental animal models where an incision in the central canal at lumbar level during fetal life led to Chiari malformation type 2. 7
A few cases of Chiari malformation type 2 have been described with no associated open spinal dysraphism. 4,8 –10 In 2 of them, Tubbs and colleagues reported a Chiari malformation type 2 solely associated with a lipoma of the filum terminale, a mild form of occult spinal dysraphism, which is not a site of cerebral spinal fluid leakage. This finding weakens McLone and Knepper’s pathogenic hypothesis of Chiari malformation type 2, whereby Chiari malformation type 2 might develop even in the absence of cerebral spinal fluid leakage and hypotension.
In our patient, a thorough spinal magnetic resonance imaging evaluation excluded any form of dysraphism, even a lipoma of the filum terminale, thus apparently supporting the criticism of Tubbs and colleagues. Nonetheless, in our case the presence of a patent craniopharyngeal duct with the detection of air bubbles in the pituitary region seems to identify an alternative site of cerebral spinal fluid leakage. During fetal life, this malformation might have acted as a surrogate of an open spinal dysraphism leading to chronic cerebral spinal fluid hypotension. Interestingly, one of the patients described by Tubbs et al 9 had a history of surgery for a dermal sinus tract at the nasion. The latter is a fistula between intra- and extracranial structures, 11 and it might have represented a site of chronic cerebral spinal fluid leakage during intrauterine life.
According to these observations, intrauterine cerebral spinal fluid hypotension seems to reemerge as a pathogenic mechanism of Chiari malformation type 2 even in those rare cases without a concomitant open spinal dysraphism. Consequently, cases of Chiari malformation type 2 without spina bifida should prompt a careful search for concealed sites of chronic cerebral spinal fluid leakage. Therefore, Chiari malformation type 2 might be present without spinal dysraphism, and the above mentioned syllogism should be modified to “If Chiari II, then intrauterine cerebral spinal fluid leakage; if intrauterine cerebral spinal fluid leakage, then Chiari II.”
Footnotes
Acknowledgments
The authors sincerely thank Dr. Chiara Briani, Dr. Arastoo Vossough and Dr. J Christopher Edgar for their detailed review, constructive criticism and excellent advice.
VC: study design, acquisition of data, drafting the manuscript, interpretation of data. IT: acquisition of data, analysis of data, drafting the manuscript for content. LB: acquisition of data, revising the manuscript for content. AP: acquisition of data, revising the manuscript for content. EE: acquisition of data, revising the manuscript for content. SS: acquisition of data, revising the manuscript for content. RM: study concept, acquisition of data, interpretation of data, drafting the manuscript, study supervision.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.
The study protocol was approved by our Institutional Review Board.